Embed Size (px)
Citation preview

Psychiatry Research, 13,295-304 Elsevier
295
Effect of Clonidine on the Secretion of Anterior Pituitary Hormones in Heroin Addicts and Normal Volunteers
Francesca Brambilla, Mario Lampertico, Albert0 E. Panerai, Laura Sali, Francesco Salerno, and Eugenio E. Miiller
Received July 13. 1983; revised version received February 13, 1984; accepted April 5, 1984.
Abstract. Neuroendocrine effects of intravenous injections of clonidine, 0.15 mg, were investigated in 13 heroin addicts and 14 normal control subjects. The study was designed to determine whether continuous opiate administration leads to the development of hypersensitive a,-adrenergic receptors. The peak increments in levels of plasma growth hormone (GH) and P-endorphin induced by clonidine did not differ between heroin addicts and normal control subjects. At no time interval could the clonidine-induced rise in GH levels in addicts be differentiated from that induced by placebo. Clonidine failed to alter plasma prolactin, gonadotropin, or thyrotropin levels in either heroin addicts or controls. Since clonidine’s neuro-
endocrine effects are reportedly due to the activation of postsynaptic o,-adreno- ceptors, it appears that (1) continuous opiate use does not lead to the development of hypersensitive cu,-adrenergic receptors involved in neuroendocrine mechanisms and (2) brain norepinephrine does not play a role in the regulation of tonic prolactin, gonadotropin, and thyrotropin secretion in man.
Key Words. Heroin addicts, clonidine, growth hormone, /3-endorphin.
Because the behavioral and biochemical effects of opiates seem to involve interactions with catecholamine (CA) neurotransmitter systems (Lal, 1975), clinicians have attempted to modify opiate euphoria and withdrawal through the administration of drugs that modify these neurotransmitters. One such drug is clonidine, an cY,-adreno- ceptor agonist (Anden et al., 1976) which appears useful in both inpatients and outpatients and for both heroin and methadone detoxification (La1 and Fielding, 1983). The rationale for using clonidine is that of switching off noradrenergic neuro- transmission and thus impeding norepinephrine (NE) release onto postsynaptic NE receptors that have become hypersensitive as a result of continuous opiate administra- tion (Gold et al., 1978). Among the properties of clonidine is the stimulation of anterior pituitary (AP) hormone release; it provokes growth hormone release in a
Francesca Brambilla, M.D., is Professor, Ospedale Psichiatrico Pini, Milan. Mario Lampertico. M.D.. is Head, and Laura Sali, M.D., is Resident, Second Medical Division. General Hospital of Saronno. Francesco Salerno, M.D., is Assistant Professor, Clinica Medica III, University of Milan. Albert0 E. Panerai. M.D.. is Associate Professor, and Eugenio E. Mtiller, M.D., is Professor, Department of Pharma- cology, Chemotherapy, and Toxicology, University of Milan. (Reprint requests to Dr. E.E. Mtiller. Department of Pharmacology. Chemotherapy, and Toxicology. University of Milan, 20129 Milan, Italy.)
01651781/84/$03.00 0 1984 Elsevier Science Publishers B.V.

296
variety of species, including man (see Miiller et al., 1978) and stimulates luteinizing hormone (Estes et al., 1982) and /3-endorphin (Pettibone and Mueller, 198 1) release in rats. Since these neuroendocrine effects of clonidine reportedly result from the activa- tion of postsynaptic NE sites (Estes et al., 1982; Krulich et al., 1982; McWilliam and Meldrum, 1983), it seemed worthwhile to evaluate clonidine’s effects on the secretion
of some AP hormones in heroin addicts and to compare these effects to those occurring in normal volunteers.
Methods
Subjects were 14 heroin addicts, 12 men and 2 women, aged 17-30 years, who had histories of addiction to heroin alone that had lasted between 18 months and 9 years. (See Table 1 for clinical characteristics of the sample.) All the patients had previous histories of intake of other drugs of abuse (amphetamine, LSD, cannabis, morphine) but had been totally off them since starting to use heroin. Eleven addicts were outpatients and three were inpatients in our Institutes. Daily heroin, always taken intravenously, ranged from I50 to 1500 mg of the street preparation (-18% pure heroin). The last heroin intake before the hormonal study began was from 2 to I6 hours earlier. All patients had a normal body build and were within their ideal body weight range. Three of the subjects had previously had viral hepatitis.
Fourteen healthy volunteers, I2 men and 2 women, aged 20-36 years, with no metabolic or endocrine disorders were selected as control subjects. They had never used drugs of abuse.
After an overnight fast and rest for I2 hours (inpatients) or I hour (outpatients), heroin subjects were studied on two occasions. Thirteen of the I4 addicts were given I50 pg clonidine (Catapres, Boehringer Ingelheim, Ltd., Florence) diluted in IO ml of 0.9% saline over 3-4 minutes. Three days later, four of these patients and one additional addict were given 0.9c/c saline alone intravenously over 3-4 minutes. The two tests were administered in random order and under single-blind conditions. Control subjects received only the clonidine injection after an overnight fast and I hour at bed rest. Blood was taken through an indwelling butterfly needle at 30 minutes before treatment and at 0, 15, 30,45,60,90, and 120 minutes from the time of treatment. All subjects were supine, comfortable, and free of stress during the test.
Growth hormone (GH), prolactin (PRL), luteinizing hormone (LH), follicle-stimulating hormone (FSH), and thyrotropin (thyroid-stimulating hormone; TSH) were assayed by double antibody radioimmunoassay(RIA) methods, as previously described (Brambilla et al., 1978). In IO heroin addicts (Nos. 2,513) and 7 control subjects, P-endorphin was determined in plasma after clonidine administration as previously described (Panerai et al., 1983). It was also determined in five addicts after saline administration. In brief, blood samples collected in ethylenediaminetetraacetate (EDTA) and the enzyme inhibitor aprotinin were extracted and concentrated on octadodecanylic silica columns and applied on high performance liquid chromatography (HPLC). Fractions corresponding to the elution time of P-endorphin were evaluated by RIA. In heroin addicts, signs of abstinence from heroin were monitored by the use of the Blackly (1966) procedure, and urine was analyzed for the presence of the drug according to Spector and Parker (1970).
Results are expressed as mean (*SD) of absolute values (see Table 2) or as absolute changes (+SEM) from baseline following clonidine or saline administration (see Figs. I and 2) and also as area under the response curve (AUC).
Differences between groups were evaluated by both Student’s I test for paired and unpaired data and analysis of variance (ANOVA) and considered statistically significant when ap<0.05 was obtained. The frequency of inadequate hormonal responses to clonidine in addicts was evaluated in comparison to those occurring in control subjects using the ~2 test. Since few addicts and controls showed inadequate GH responses to clonidine (see below), a GH response to clonidine was arbitrarily considered within normal limits when the peak GH value at least doubled baseline level. with an increment of at least 4 ngiml.

Tab
le
1. C
linic
al
char
acte
rist
ics
of
her
oin
ad
dic
ts
Tim
e si
nce
D
ura
tio
n
of
last
her
oin
D
aily
C
ase
Ag
e W
eig
ht
Hei
gh
t ad
dic
tio
n
inje
ctio
n
her
oin
P
revi
ou
s N
o.
(yea
rs)
Sex
(k
g)
(cm
) (y
ears
) (h
ou
rs)
do
se
(mg
) h
epat
itis
1 20
M
62
17
3 18
mo
s.
16
150
No
2 23
M
72
18
0 2
16
500
No
3 22
M
55
16
8 1
12
1,00
0 Y
es
4 18
M
60
17
5 1
8 1,
500
No
5 30
M
70
17
2 4
6 25
0 Y
es
6 23
F
72
17
2 7
2 70
0 N
o
7 20
M
75
16
9 3
12
1,50
0 N
o
8 18
M
78
17
1 18
mo
s.
2 1,
500
No
9 17
M
74
17
5 18
mo
s.
12
1,50
0 N
o
10
18
M
74
173
2.5
16
500
No
11
23
M
67
175
18 m
os.
15
25
0 N
o
12
23
M
77
178
9 12
50
0 N
o
13
22
M
71
176
5 12
1,
000
Yes
14
22
F
69
169
3 2
1,50
0 N
o
M =
mal
e;
F =
fem
ale;
m
os.
= m
onth
s

298
Results
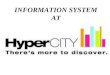
Mean basal plasma GH levels were 2.1 f 1.7 and 1.5 + 1 .O ng/ml in addicts and controls, respectively (p = NS). Three addicts (Table 1, Nos. 4, 6, and 14) had mildly elevated GH levels (5.3, 5.4, and 5.1 ng/ ml, respectively; range of normal values, O-3.0 ng/ ml). In addicts, administration of clonidine induced peak GH rises that occurred between 15 and 120 minutes, while in controls GH peaked between 30 and 90 minutes. Mean GH peak increments were 5.7 f 1.45 ng/ ml in addicts and 8.8 f 5.2 ng/ml in controls (p q NS) (Fig. 1). The mean AUC was 3 1.9 f 6.4 ng/ ml in addicts and 45.1 f 8.4 ng/ml in controls @ = NS). Evaluation of the results with ANOVA revealed that the difference between the two groups was not statistically significant (F= 0.322 1). Six addicts (Nos. 1, 2, 5, 6,9, and 11) and three controls showed reduced or absent GH responses to the clonidine stimulus (x2 = 1.87, p = NS). Administration of saline induced no significant changes in addicts’ plasma GH levels (basal, 2.7 f 0.7 ng/ ml; peak at 30 minutes, 3.0 + 1.7 ng/ ml). GH levels after saline and after clonidine did not differ significantly at any time interval (Table 2). The pattern of GH response to clonidine also did not correlate with basal GH levels, duration of addiction, dose of heroin intake, interval since the last heroin intake, previous history of viral hepatitis, or patient’s weight level.
Fig. 1. Growth hormone (GH) response to i.v. administration of clonidine (150 pg) in 13 addicts and 14 controls
20.
18. .
.
.
14. .
,a. .
. IO. :* . 8. ---I . . . 0. . t- .
. 4. .
. . .
2. . . .
. l
. 0
addicts Conlrols
Data are reported as peak GH mcrements from baseline 111 ln mdwldual subfects, and also as mean + SEM. In addition to data for addicts and controls receiving clonldine, data are also shown for 5 addicts receiving saline.

Tab
le
2. E
ffec
t o
f cl
on
idin
e (1
50 p
g i
.v.)
on
GH
, /?
-en
do
rph
in,
PR
L,
FS
H,
LH
, an
d T
SH
re
leas
e in
her
oin
ad
dic
ts
and
co
ntr
ols
0 15
30
Tim
e (m
inu
tes)
45
60
90
12
0
GH
in
g/m
li A
ddic
ts,
clon
idin
e A
ddic
ts,
salin
e
Con
trol
s,
clon
idin
e
p-E
ndor
phin
ifm
ole/
mll
Add
icts
, cl
onid
ine
Add
icts
, sa
line
Con
trol
s,
clon
idin
e
PR
L (n
g/m
l I
Add
icts
, cl
onid
ine
Add
icts
, sa
line
Con
trol
s,
clon
idin
e
FS
H j m
u/m
l j
Add
icts
, cl
onid
ine
Add
icts
, sa
line
Con
trol
s,
clon
idin
e
LH I m
u/m
l )
Add
icts
, cl
onid
ine
Add
icts
, sa
line
Con
trol
s,
clon
idin
e
TS
H
(pLJ
/mli
Add
icts
, cl
onid
ine
Add
icts
, sa
line
Con
trol
s,
clon
idin
e
2.1
t 1.
7
2.7
t 1.
7
1.5
+
1.0
38.7
f
17.0
41 .a
+_ 5
0.7
45.9
It
22.2
6.8
f 5.
3
12.5
t
9.2
6.6
2 2.
5
10.1
k
7.1
6.6
+
6.6
12.4
+
7.4
9.1
2 4.
0
4.6i
1.
2 7.
1 +
2.
5
1.6
+
0.7
2.3
+
1.3
1.32
1.
0
2.9
k 2.
6 2.
8 2
2.1
3.8
i 4.
3
30.8
f
16.0
37
.8
+ 4
3.4
47.2
k
22.1
6.1
+
5.3
14.1
f
10.4
6.6
+
2.8
10.5
+
6.8
6.7
+
6.6
13.3
t
7.9
a.5
2 4.
0 4.
4 +
0.
9 7:
6 t
2.3
1.6
k 0.
8
2.3
+
1.2
1.7
k 1.
4
4.3
1 4.
0 3.
0 +
1.
7
6.7
?I
5.5
32.2
i
15.4
21.9
i
20.1
57.3
+
23.
0
5.1
i 3.
4
13.9
i
13.8
5.
9 +
2.
8
10.1
I!I
5.
3 5.
9 ?
4.5
12.8
+
a.2
a.0
i 3.
0 3.
9%
1.1
7.5
+
2.8
1.8
-t
0.7
2.4
f 1.
5
1.52
1.
1 1.
4 k
1.2
1.4
k 0.
8 1.
1 i-
0.
7
5.3
k 5.
4 2.
5 i-
1.
2
9.1
2 6.
2
43.6
f
24.8
20.2
f
16.3
70.0
k
30.0
4.6
? 3.
0 14
.8 k
12
.3
5.2
k 2.
2
9.6
t 5.
5 6.
6 +
5.
0 12
.1 k
a.
8
a.5
+
2.6
4.5
f 1.
2 7.
8 i
2.3
1.8
2 0.
6 1.
8 f
0.9
5.1
+
5.5
2.6
+
1.5
a.2
2 4.
9
48.8
i
34.0
21.1
I
15.4
77.4
z?
z 66.
8
4.7
i 3.
1
12.6
k
10.8
5.
9 f
1.9
9.2
f 5.
9 5.
8 i:
4.8
10.5
i
5.8
a.3
+
3.1
4.7
i 1.
4 a.
1 i
1.1
1.5
f 0.
6 1.
9 k
0.7
4.0
k 3.
2 2.
2 k
1.3
4.6
t 3.
6
35.0
2
20.3
24.8
f
16.7
70.5
+
25.
9
4.7
f 3.
1
11.0
k
9.8
6.1
+_
2.2
a.8
i 5.
9 6.
3 I
4.4
13.5
+
10
.4
9.5
k 3.
0
5.0
i 2.
5 9.
5 i
2.8
1.6
+
0.6
2.2
f 2.
0
2.8
k 2.
7 2.
1 1
1.6
3.2
+-
4.0
47.1
_t
4.
9
la.3
+
_ 12
.3
48.9
k
25.9
4.5
i 2.
9 7.
8 k
5.3
6.1
k 2.
3
a.5
t 6.
5 6.
5 F
4.
9 ii.
8 k
6.8
a.2
k 2.
7
4.5
f 2.
0 a.
8 2
1.6
1.7
k 0.
8 2.
4 k
0.8
1.5
k 0.
8
Val
ues
pre
sen
ted
ar
e m
ean
i
SD
. T
her
e w
ere
13 a
dd
icts
in
th
e cl
on
idin
e co
nd
itio
n,
5 ad
dic
ts
in t
he
salin
e co
nd
itio
n.
and
14
co
ntr
ols
in
th
e cl
on
idin
e co
nd
itio
n.

300
Mean basal PRL levels were 6.8 + 5.3 and 6.6 * 2.5 ngi ml in addicts and controls, respectively @ = N’S). Four patients (Nos. 7, 8, 10, and 12) had moderately elevated PRL levels compared to normal values from our laboratory (e.g., 17.5, 18.0,2 1 S, and 27.0; upper limit in men, 11 .O ng/ ml). Mean basal FSH levels were 10.1 + 7.1 and 12.4 f 7.4 mu/ml in addicts and controls, respectively @ = NS). Six patients (Nos. 3,4,8,9, 12, and 13) had low baseline FSH levels(3.1,2.0,3.0,0.5,4.0, and 3.0, respectively, vs. 545 mU / ml). Mean basal LH levels were 9.1 * 4.0 and 7.1 f 2.5 mU/ ml in addicts and controls, respectively @ q NS). Four patients (Nos. 6, 7, 8, and 14) had low baseline LH levels (3.2,3.5,4.5, and 4.8 mU / ml, respectively; range of normal values for men, 5-25 mU/ ml). Mean basal TSH levels were 1.6 + 0.7 and 1.3 f 1.0 mU/ ml in addicts and controls, respectively @ = NS). In both addicts and controls clonidine did not change plasma PRL, FSH, LH, or TSH levels; in addicts, no changes in these hormones occurred after saline either (Table 2).
Mean basal P-endorphin levels were 38.7 f 17.0 fmole/ ml in addicts and 45.9 * 22.2 fmole/ml in controls @ q NS). In both addicts and controls, administration of clonidine induced peak rises in plasma /3-endorphin that occurred at 45- 120 minutes posttreatment. Mean /3-endorphin peak increments were 42.0 + 15.1 fmole/ml in addicts and 56.3 * 20.3 fmole/ ml in controls @ q NS) (Fig. 2). After clonidine, the AUC was 11.2 + 34.2 and 134.5 + 87.0 fmole/ ml in addicts and controls, respectively (p = NS). Evaluation of the results with ANOVA revealed that the difference between the
Fig. 2. /3-Endorphin response to clonidine in 10 addicts and 7 controls
.
sddlcls controls
Also shown IS the effect of saline admlnistratlon in 5 addicts. See legend to Fig. 1

301
two groups was not statistically significant (F= 0.5329). Three addicts (Nos. 7,8, and 13) and two controls showed a decrement in plasma /3-endorphin levels after clonidine (~2 = 0.002, p q NS).
After saline, addicts showed a trend toward lower /3-endorphin levels. The differ- ence between P-endorphin levels after saline and after clonidine in addicts was significant at 45 minutes @ < 0.05) (Table 2). In the four addicts who received both clonidine and saline, no difference was observed in PRL, LH, FSH, and TSH maximal variations (a) recorded (Student’s I test for paired data).
After clonidine, all addicts and controls experienced drowsiness, beginning 30 minutes after drug administration and lasting for 2-6 hours. Mean basal blood pressure was normal in both addicts and controls. After clonidine, blood pressure dropped from 130-120/80-70 to 1 lo-90/70-60 mmHg in addicts, and from 140- 120/90-80 to lOO-90/70-60 mmHg in controls, with the nadir around 15-30 minutes and a return to baseline at 120 minutes.
Discussion
Mean fasting levels of all hormones were within normal range in heroin addicts, a finding in keeping with the observations in other studies of opiate users (Dent and Tolis, 1976; Cushman, 1980). Scrutiny of individual hormone values, however, shows that a few cases had elevated plasma GH and PRL levels, and low plasma levels of gonadotropins, though no relationship could be found between hormone levels and the pattern of heroin intake. The presence of elevated basal PRL and GH levels, and of low gonadotropins, in heroin addicts has been previously described (Brambilla, 1980).
Clonidine is an effective a,-adrenergic receptor stimulant and GH releaser in many animal species, including man (as reviewed in the beginning of this article). Recently, studies in rats and monkeys whose NE terminals were pharmacologically denervated have shown that depletion of brain CAs does not prevent the clonidine-induced GH rise (Krulich et al., 1982; McWilliam and Meldrum, 1983). These findings have been interpreted as suggesting that the influence of clonidine on GH secretion is mediated by postsynaptic a,-adrenergic receptors.
Clonidine has been successfully used to blunt opiate withdrawal in opiate-addicted subjects (La1 and Fielding, 1983). The rationale underlying its use is that the neuronal activity of the noradrenergic systems chronically inhibited by exogenous opiate administration (Atweh and Kuhar, 1977) results in the increased sensitivity of postsy- naptic a,-adrenergic receptors; this enhanced sensitivity becomes behavioral1.y evident with the appearance of the acute withdrawal syndrome when exogenous opiates have been discontinued. Clonidine, by virtue of its ability in low doses to inhibit NE release by nerve terminals (Gold et al., 1978), should reverse opiate withdrawal by replacing opiate-mediated inhibition with a,-adrenergic inhibition of noradrenergic activity. Since postsynaptic cY,-adrenergic sites have been implicated in the clonidine-induced GH rise (see above), a greater GH rise after clonidine would be anticipated in subjects with continuous opiate intake. An enhanced GH response to clonidine resultingfrom denervation supersensitivity has recently been demonstrated in dogs receiving chronic administration of the a,-adrenoceptor antagonist yohimbine (Cella et al., 19836).
In the present study, however, an opposite pattern was found. In fact, the GH rise

302
induced by clonidine in addicts was intermediate between that induced by saline and that induced by clonidine in controls, and did not differ to a statistically significant degree from either. Although no certain explanation for this finding is readily appar- ent, some hypotheses can be offered.
The postulated opiate interactions with noradrenergic areas that may account for clonidine-induced suppression of opiate withdrawal symptoms are believed to occur in the pons at the level of the locus ceruleus, an area which may be regulated by both a,-adrenergic and opiate receptors (Gold et al., 1978). Such interactions may not be operative at the level of the higher (hypothalamic?) centers, where the neuroendocrine action of clonidine is presumably manifested (Rudolph et al., 1980). Alternatively, chronic intake of opiates may induce tolerance to the inhibitory action of opioid receptors on noradrenergic neurons implicated in GH release (Eden et al., 198 1). Such tolerance would avoid the occurrence of postsynaptic a,-adrenergic denervation with NE being released from its presynaptic terminals unopposed in chronic opiate users. Mitigating against this explanation, however, is the observation that heroin addicts do not develop tolerance to the GH-releasing effect of the met-enkephalin analogue FK 33-824 (Brambilla et al., 1981).
A more plausible explanation would be that in man, in contrast to rat and monkey (see above), clonidine-induced GH increases result from activation of a,-presynaptic sites, a possibility that we have recently proposed based on studies performed in the dog (Cella et al., 1983a, 19836).
In the present study, the trend observed toward lower GH increments after cloni- dine in heroin addicts than in controls suggests the presence of cy,-adrenergic presy- naptic hyposensitivity.
A considerable controversy revolves around the effects of the a-adrenergic system on adrenocorticotropic hormone (ACTH) and ACTH-related peptides (Mtiller et al., 1978) which share the same control mechanisms and are released together from the corticotrophs (Guillemin et al., 1977). An extensive series of studies performed in either rats or dogs has shown that activation of the hypothalamic noradrenergic system results in inhibition of ACTH release (Van Loon, 1973), while in primates some evidence points to the existence of stimulatory noradrenergic influences (Rees et al., 1970; Sachar et al., 1980). Recently, it has been shown that a single injection of clonidine in rats induces a brisk rise in plasma levels of immunoreactive /3-endorphin, an effect mediated by activation of a-adrenergic receptors that is partially or fully blocked by a series of a-adrenergic antagonists (Pettibone and Mueller, 1981). Con- sistent with the rat data, in our study administration of clonidine induced a clear-cut rise in plasma P-endorphin in most of the heroin addicts and controls, thus pointing to the existence in man of a stimulatory a-adrenergic tonic effect on ACTH-related peptide secretion. The actual locus of action of clonidine in stimulating fi-endorphin release in man is presently unknown. In rats evidence has been provided that clonidine may stimulate b-endorphin (D.J. Pettibone and G.P. Mueller, unpublished observa- tions) and ACTH (Labrie et al., 1983) secretion by acting directly on corticotrophs. Our results are in partial disagreement with the findings of Farsang et al. (1983) who reported that daily administration of clonidine (150 r.rg/ b.i.d.) for 3 days increased plasma /3-endorphin levels in patients with essential hypertension but not in normo-

303
tensive subjects. Differences in the dosage and schedule of clonidine administration may explain the discrepancy.
Evidence has been presented that the central ol-adrenergic system, through NE and
perhaps epinephrine, plays an excitatory role in the pulsatile release of LH in ovarec- tomized rats (Estes et al., 1982). In ovarectomized rats with drug-induced depletion of brain NE levels, there is a marked dampening of pulsatile LH secretion, which is normalized by a single bolus injection of clonidine. In our study, clonidine did not induce any change in plasma LH levels in either controls or addicts, thus failing to support a role for the brain noradrenergic system in baseline LH secretion in man. Similarly, a clonidine-induced alteration of the brain NE system did not modify plasma levels of PRL, FSH, and TSH in our subjects, an observation in keeping with previous data of La1 et al. (1975).
In conclusion, these studies failed to provide evidence in heroin addicts of an enhanced sensitivity attributable to clonidine administration of a,-receptor sites involved in GH and P-endorphin release or the appearance of qualitative abnormal responses in the secretion of the other AP hormones investigated. In addition, they have confirmed the lack of a noradrenergic mechanism in the regulation of tonic PRL, FSH, LH, and TSH secretion in man.
References
Anden, N.-E., Grabowska, M., and Strombom, U. Different alpha adrenoceptors in the central nervous system mediating biochemical and functional effects of clonidine and receptor blocking agents. Naunrn Schmiedeberg’s Archives of Pharmacology, 292,43 (1976).
Atweh, S.F., and Kuhar, M.J. Autoradiographic localization of opiate receptors in rat brain: 11. The brain stem. Brain Research, 129, 1 (1977).
Blackly, P.H. Management of opiate abstinence syndrome. American Journalof Psychiatry, 122, 742 (1966).
Brambilla, F. Hormonal changes in addiction. In: De Wied, D., and Van Keep, P.A., eds. Hormones and the Brain. M.T.P. Press, Lancaster, p. 313 (1980).
Brambilla, F., Casanueva, F., Lovati, C., Penalva, A., Madeddu,‘A., Martinez-Campos, A., and Miiller, E.E. Lack of tolerance in heroin addicts to the neuroendocrine effects of an enkephalin analogue. Life Sciences, 29, 493 ( 198 I).
Brambilla, F., Smeraldi, E., Sacchetti, E., Negri, F., Cocchi, D., and Mtiller, E.E. Deranged anterior pituitary responsiveness to hypothalamic hormones in depressed patients. Archives of General Psychiatry, 35, 123 I ( 1978).
Cella, S.G., Picotti, G.B., Mantegazza, P., and Mtiller, E.E. Evidence in favor of an inhibi- tory role of CNS noradrenergic system on growth hormone release in the dog. (Abstract) Proceedings of the 65th Annual Meeting of the Endocrine Society, p. 213 (1983a).
Cella, S.G., Picotti, G.B., and Mfiller, E.E. a,-Adrenergic stimulation enhances growth hormone secretion in the dog: A presynaptic mechanism? Life Sciences, 32, 2785 (19836).
Cushman, P. The major medical sequelae of opioid addiction. Drug and Alcohol Depend- ence, 5,239 (1980).
Dent, R., and Tolis, G. Hypothalamic-pituitary-target organ axis in patients on methadone maintenance. (Abstract) Proceedings of the 58th Annual Meeting of the Endocrine Society, p. 165 (1976).
Eden, S., Eriksson, E., Martin, J.B., and Modigh, K. Evidence for a growth hormone releasing factor mediating alpha-adrenergic influence on growth hormone secretion in the rat. Neuroendocrinology,, 33, 24 ( 1981).

304
Estes, K.S., Simpkins, J.W., and Kalra, S.P. Resumption with clonidine of pulsative LH release following acute norepinephrine depletion in ovarectomized rats. Neuroendocrinology~, 35, 56 (1982).
Farsang, C., Vajda, L., Kapocsi, J., Mali&k, Z., Alfoldi, S., Varga, K., JuhBsz, l., and Kunos. G. Diurnal rhythm of beta endorphin in normotensive and hypertensive patients: The effect of clonidine. Journal of Clinical Endocrinology and Metabolism, 56, 865 (1983).
Gold, M.S., Redmond, D.E., Jr., and Kleber, H.D. Clonidine blocks acute withdrawal symptoms. Lancet, II, 599 (1978).
Guillemin, R., Vargo, T., Rossier, J., Ling, N., Rivier, C., Vale, W., and Bloom, F. Beta- endorphin and adrenocorticotropin are secreted concomitantly by the pituitary gland. Science, 197, 1367 (1977).
Krulich, L., Mayfield, M.A., Steele, M.K., McMillen, B.A., and McCann, S.M. Differential effects of pharmacologic manipulations of central Q, and a2 adrenergic receptors on the secretion of thyrotropin and growth hormone in male rats. Endocrino1og.v. 110, 796 (1982).
Labrie, F., Ciguere, V., Proulx-Ferland, L., Cot& J., Veilleux, R., Lefevre, G., Raymond, V., and Leung, P. Mechanism of control of ACTH secretion in the anterior lobe of the pituitary gland. In: Endriiczi, E., De Wied, D., Angelucci, L., and Scapagnini, U., eds. Integrative Neurohumoral Mechanisms. Elsevier Biomedical Press, Amsterdam, p. 25 1 (1983).
Lal, H. Narcotic dependence, narcotic action and dopamine receptors. Life Sciences, 17,483 (1975).
Lal, H., and Fielding, S. Clonidine in the treatment of narcotic addiction. Trends in Pharmacological Sciences, 4, 70 (1983).
Lal, S., Tolis, G., Martin, J.B., Brown, G.M., and Guyda, H. Effect of clonidine on growth hormone, prolactin, luteinizing hormone, follicle-stimulating hormone, and thyroid-stimu- lating hormone in the serum of normal men. Journal of Clinical Endocrinology and Metabo- lism, 41, 827 (1975).
McWilliam, J.R., and Meldrum, B.S. Noradrenergic regulation of growth hormone secretion in the baboon. Endocrinology, 112, 254 (1983).
Mtiller, E.E., Nisticb, G., and Scapagnini, U. Brain NeurotransmittersandAnterior Pituitaq Function. Academic Press, New York (1978).
Panerai, A.E., Martini, A., De Giulio, A.M.. Fraioli, F., Vegni, C., Pardi, G., Marini, A., and Mantegazza, P. Plasma P-endorphin, /3-lipotropin and met-enkephalin in normal and drug addicted women and their newborn. Journal of Clinical Endocrinology and Metabolism, 57, 537 (1983).
Pettibone, D.J., and Mueller, G.P. o-Adrenergic stimulation by clonidine increases plasma concentrations of immunoreactive P-endorphin in rats. Endocrinology, 109, 798 (198 I).
Rees, L., Butler, P.W.P., Gosling, C., and Besser, G.M. Adrenergic blockade and the corticosteroid and growth hormone responses to methyl amphetamine. Nature, 228,565 (1970).
Rudolph, C.D.. Kaplan, S.L., and Ganong, W.F. Sites at which clonidine acts to affect blood pressure and the secretion of renin, growth hormone and ACTH. Neuroendocrinology, 31,121 (1980).
Sachar, E.J., Asnis, G., Halbreich, U., Nathan, R.S., and Halpern, F. Recent studies in the neuroendocrinology of major depressive disorder. In: Sachar, E.J., ed. Psychiatric, Clinics of North America. B. Saunders Co., Philadelphia, p. 327 (1980).
Spector, S., and Parker, C.W. Morphine: Radioimmunoassay. Science, 168, 1347 (1970). Van Loon, G.R. Brain catecholaminesand ACTH secretion. In: Ganong, W.F., and Martini,
L., eds. Frontiers in Neuroendocrinology. Oxford University Press, New York, p. 209 (1973).













![Heroin maintenance for chronic heroin-dependent individualsharmreductionactioncenter.org/HRAC_DOCUMENTS/ADDICTION AND... · [Intervention Review] Heroin maintenance for chronic heroin-dependent](https://img.dokumen.tips/doc/110x75/5b87383e7f8b9a1a248c3f66/heroin-maintenance-for-chronic-heroin-dependent-individualsharmr-and-intervention.jpg)