Embed Size (px)
Citation preview

Efficacy, safety and immunological profile of combining rituximab with belimumab for adults with persistent orchronic immune thrombocytopenia: results from a prospective phase 2b trial
by Matthieu Mahévas, Imane Azzaoui, Etienne Crickx, Florence Canoui-Poitrine, Delphine Gobert, Laetitia Languille, Nicolas Limal, Constance Guillaud, Laure Croisille, Mohamed Jeljeli, Fréderic Batteux, Samia Baloul, Olivier Fain, France Pirenne,Jean-Claude Weill, Claude-Agnès Reynaud, Bertrand Godeau, and Marc Michel
Haematologica 2020 [Epub ahead of print]
Citation: Matthieu Mahévas, Imane Azzaoui, Etienne Crickx, Florence Canoui-Poitrine, Delphine Gobert, Laetitia Languille, Nicolas Limal, Constance Guillaud, Laure Croisille, Mohamed Jeljeli, Fréderic Batteux, Samia Baloul, Olivier Fain, France Pirenne, Jean-Claude Weill,Claude-Agnès Reynaud, Bertrand Godeau, and Marc Michel. Efficacy, safety and immunological profile of combining rituximab with belimumab for adults with persistent or chronic immune thrombocytopenia: results from a prospective phase 2b trial. Haematologica. 2020; 105:xxxdoi:10.3324/haematol.2020.259481
Publisher's Disclaimer.E-publishing ahead of print is increasingly important for the rapid dissemination of science.Haematologica is, therefore, E-publishing PDF files of an early version of manuscripts thathave completed a regular peer review and have been accepted for publication. E-publishingof this PDF file has been approved by the authors. After having E-published Ahead of Print,manuscripts will then undergo technical and English editing, typesetting, proof correction andbe presented for the authors' final approval; the final version of the manuscript will thenappear in print on a regular issue of the journal. All legal disclaimers that apply to thejournal also pertain to this production process.
Copyright 2020 Ferrata Storti Foundation.Published Ahead of Print on August 13, 2020, as doi:10.3324/haematol.2020.259481.

1
Efficacy, safety and immunological profile of combining
rituximab with belimumab for adults with persistent or
chronic immune thrombocytopenia: results from a
prospective phase 2b trial
Matthieu Mahévas1,2,3, Imane Azzaoui1,3* Etienne Crickx1,2,3*, Florence Canoui-Poitrine4,
Delphine Gobert5, Laetitia Languille1, Nicolas Limal1, Constance Guillaud1, Laure Croisille6,
Mohamed Jeljeli7, Fréderic Batteux7, Samia Baloul4, Olivier Fain5, France Pirenne3, Jean-
Claude Weill2 and Claude-Agnès Reynaud2, Bertrand Godeau1,3and Marc Michel1,3
Short title: Rituximab combined with belimumab for adult ITP
* these authors contributed equally to this work 1 Service de Médecine Interne, Centre National de Référence des Cytopénies Auto-Immunes de l’Adulte, Centre Hospitalier Universitaire Henri-Mondor, Assistance Publique-Hôpitaux de Paris, Université Paris Est Créteil, Créteil, France 2 Institut Necker Enfants Malades, INSERM U1151/CNRS UMS 8253, Université Paris Descartes, Sorbonne Paris Cité, 75993 Paris Cedex 14, France 3 IMRB - U955 – INSERM Equipe n°2 "Transfusion et maladies du globule rouge" EFS Île-de-France, Hôpital Henri-Mondor, AP-HP, 51, avenue du Maréchal-de-Lattre-de-Tassigny 4 University Paris-Est, Paris Est Créteil University (UPEC), CEpiA (Clinical Epidemiology and Ageing), EA 7376-IMRB, Créteil, France; AP-HP, Henri-Mondor Hospital, Department of Public Health, Clinical Research Unit (URC-Mondor), Créteil, France 5 Sorbonne Université, Service de Médecine Interne, Hôpital Saint-Antoine, Assistance Publique-Hôpitaux de Paris, Paris, France 6 Etablissement Français du Sang, Service d'immunologie plaquettaire, Hôpital Henri Mondor, Créteil, France 7 Service d'Immunologie biologique, Hôpital Cochin, APHP, Paris, France. INSERM U1016, Institut Cochin, Paris, France

2
Corresponding author: Matthieu Mahévas
Service de Médecine Interne, Centre de Référence des Cytopénies Auto-Immunes de l’Adulte,
Centre Hospitalier Universitaire Henri-Mondor, Assistance Publique-Hôpitaux de Paris,
Université Paris Est Créteil, Créteil, France
Email: [email protected]
Phone number : +33149812076
Fax number : +33149812772
Word count:
Abstract: 250 words
Main text: 3983 words
32 references
10 figures (including 6 supplementary figures) and 7 tables (including 5 supplementary
tables)

3
Abstract
B-cell activating factor may be involved in the failure of B-cell depleting therapy with
rituximab in immune thrombocytopenia (ITP) by promoting the emergence of splenic long-
lived plasma cells. From results obtained in mouse models, we hypothesized that combining
rituximab with sequential injections of belimumab could increase the rate of response at one
year in patients with persistent or chronic ITP by preventing the emergence of these long-
lived plasma cells. The study was a single-center, single arm, prospective phase 2b trial
investigating the safety and efficacy of rituximab given at a fixed dose of 1000 mg, two weeks
apart, combined with five infusions of belimumab, 10 mg/kg at week 0 (W0)+2 days, W2+2
days, W4, W8 and W12 for adults with primary persistent or chronic ITP. The primary
endpoint was the total number of patients achieving an overall response (complete response +
response) at W52 according to a standard definition. In total, 15 non-splenectomized adults,
nine (60%) with persistent IPT and six (40%) with chronic ITP, were included. No severe
adverse event, infection, or severe hypogammaglobulinemia was observed. Thirteen patients
achieved an initial overall response. At W52, 12 (80%) patients achieved an overall response,
including ten (66.7%) with complete response. When compared with a cohort of patients
receiving rituximab alone, the kinetics of B-cell repopulation appeared similar, but the
number of circulating T follicular helper cells was significantly decreased with belimumab
combination therapy. Combining rituximab and belimumab seems a promising strategy in ITP,
with high efficacy and acceptable safety.
ClinicalTrials.gov identifier: NCT03154385

4
Introduction
Primary immune thrombocytopenia (ITP) is a bleeding disorder mainly mediated by
autoreactive B cells and plasma cells (PCs) secreting pathogenic anti-platelet auto-antibodies,
eventually leading to accelerated platelet destruction and impaired megakaryopoiesis.1,2 First-
line treatments include steroids and intravenous immunoglobulins (IVIgs). Because less than
40% of newly diagnosed ITP adults will achieve a spontaneous remission within 12 months
after disease onset, second-line treatments are frequently needed.3 Over the past 20 years, the
anti-CD20 monoclonal antibody rituximab (RTX) has been considered an off-label second-
line option in many countries and most guidelines. RTX leads to an overall response rate of
40% at one year.4,5 Whereas an almost complete B-cell depletion is achieved in peripheral
blood and in secondary lymphoid organs after RTX in ITP,6 approximately half patients do
not respond to RTX, which raises many questions and has led to some investigations in the
past years.
In ITP, pathogenic antibody-secreting PCs are constantly generated in the spleen,
mainly through the germinal center pathway.6,7 Because most of these splenic PCs are short-
lived and have lost CD20 expression, the clinical improvement observed after RTX is thought
to result mainly from germinal center depletion, thus limiting PC generation.8,9 However,
analysis of spleen samples from ITP patients with failure of RTX revealed that despite
complete peripheral B-cell depletion, residual splenic PCs secreting anti-platelet antibody
persisted.6 More surprisingly, transcriptomic analysis showed that these splenic PCs had
acquired a long-lived program, similar to bona fide bone-marrow long-lived PCs.
Quantitatively, the data suggested that B-cell depletion had induced the differentiation of
short-lived PCs into long-lived ones, rather than the selection of pre-existing long-lived PCs,
thus providing clues for explaining RTX failure in the context of ITP.6
By using a fate mapping mouse model, we recently demonstrated that B-cell activating factor

5
(BAFF) played a major role in the emergence of these splenic long-lived PCs.10 BAFF is a
pro-survival key cytokine for the B-cell lineage,11 and elevated levels of unconsumed BAFF
are observed in serum and spleen after RTX therapy in ITP patients.6 Combining anti-CD20
with 4 infusions of anti-BAFF antibodies in this mouse model significantly reduced the
number of splenic PCs, with little impact on bone-marrow PCs.10
Hence, we hypothesized that combining two fixed doses of 1000 mg of RTX with five
sequential injections of belimumab (Benlysta®, 10 mg/kg dose) could increase the rate of
response at one year in patients with persistent or chronic ITP by preventing the emergence of
autoreactive splenic long-lived PCs. Here, we report the efficacy and safety of this new
strategy in ITP during a prospective phase 2b pilot trial.

6
Methods
Study design and study drugs
The study was a single-center, single arm, prospective phase 2b trial (RITUX-PLUS,
NCT03154385) investigating the safety and efficacy of RTX at a fixed dose of 1000 mg, two
weeks apart, combined with five intravenous infusions of belimumab (Benlysta®, 10 mg/kg)
at week 0 (W0) + 2 days, W2 + 2 days, W4, W8 and W12 (see supplemental Figure 1). The
rationale for the choice of this schedule was based on previous results obtained in a mouse
model showing that BAFF inhibition should start early.10 The belimumab dosing was similar
to the one approved in systemic lupus erythematosus. Research was conducted in accordance
with the Declaration of Helsinki and was approved by the Comité de Protection des Personnes
Ile-de-France VI.
Inclusion and exclusion criteria
Inclusion and exclusion criteria were reported Online Supplementary Methods.
Primary endpoint
The primary endpoint was the total number of patients achieving an overall response
(complete response [CR] + response [R]) at W52. CR was defined by platelet count >100
x109/L and R by platelet count 30 to 100 x109/L with at least a 2-fold increase from baseline
according to international definitions.12 Patients who required any other treatment for ITP
including rescue therapy more than six weeks after inclusion were considered non-responders
regardless of platelet count.

7
Secondary endpoints
Secondary endpoints were the number of patients achieving an overall response (CR +R)
initially and at W12, W24, W36, number of bleeding events, number of patients showing
severe hypogammaglobulinemia (gammaglobulin level < 4 g/L at W24, W36, W52), duration
of severe hypogammaglobulinemia, variation in gammaglobulin subclass levels during the
study, and number of severe infections requiring hospitalization during the study.
Adverse events
Adverse effects were graded according to the National Cancer Institute Common Terminology
Criteria for Adverse Events (CTCAE) v5.0
(https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick
_Reference_8.5x11.pdf).
Immunological analysis, Antibody titer tests, Free-Blys assay
Phenotype of circulating T- and B-cell subpopulations was analyzed by flow cytometry at
weeks 0, 4, 12, 24, 36, and 52 for every included patient and in a prospective control cohort of
ITP patients not included in this trial who received two infusions of fixed-dose RTX (1000
mg) at W0 and W2 after premedication with 100 mg intravenous methylprednisolone as a
standard of care for ITP (Online Supplementary Methods, supplemental Table 1, and
supplemental Figure 2 for gating strategy). Antibody titers for pneumococcal, tetanus, measles
vaccine were measured by ELISA. Serum-free BAFF level was measured using the assay
developed by Glaxo Smith Kline pharmaceuticals (Online Supplementary Methods).

8
Direct monoclonal antibody‐specific immobilization of platelet antigen (MAIPA) assay
Anti-platelet antibodies on patient platelets were detected by using the MAIPA assay (ApDia,
Turnhout, Belgium).
Statistical analysis
The statistical analysis was performed as described in the Online Supplementary Methods.
9
Results
Baseline characteristics
We included 15 patients (12 females) with median age 50 years [range 20-70]. All patients
had previously received corticosteroids and/or IVIgs (n=8) as first-line treatment, and ten had
received a second-line treatment (Table 1). All but one had a previous transient response to
corticosteroids. Within the month before inclusion, the median platelet count nadir was 16
x109/L [3-28]. All but one patient had cutaneous bleeding manifestations and four had
mucosal bleeding. Six patients had positive anti-nuclear antibody titers > 1/160 with no
features of systemic lupus erythematosus. When receiving the first RTX infusion, the median
duration of ITP was 11 months [range 4-52]. Nine (60%) patients had persistent ITP and six
(40%) had chronic ITP.
Safety
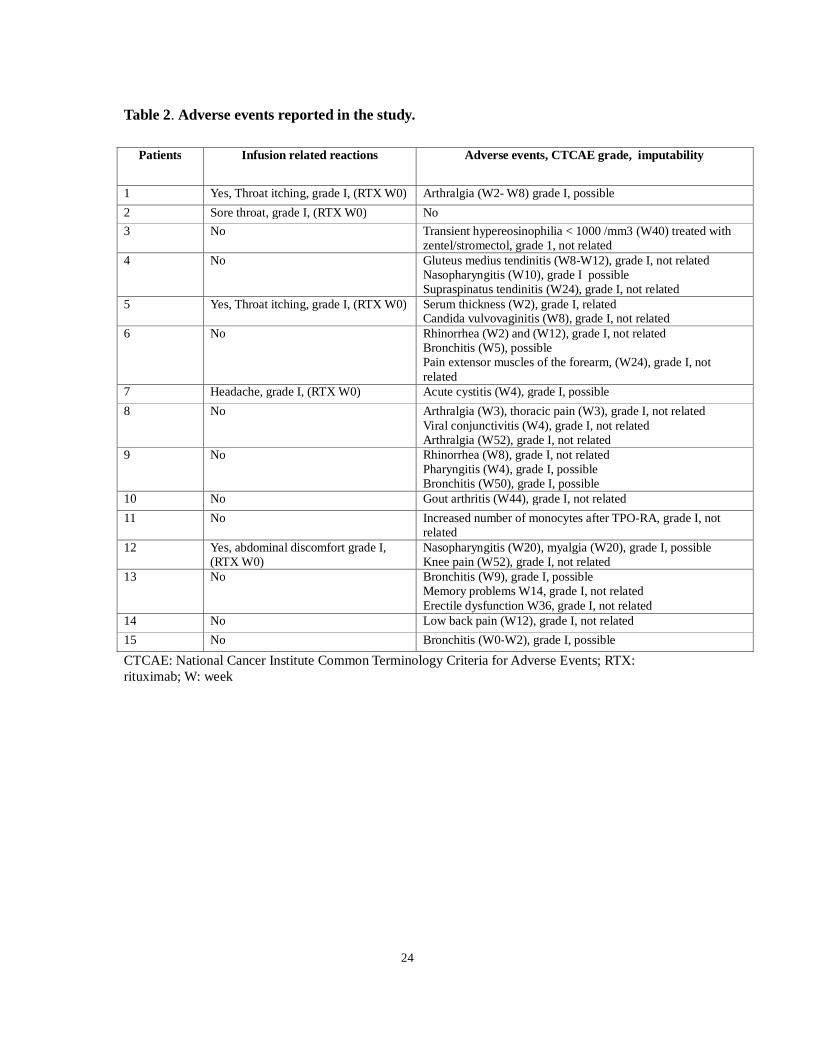
Overall, 31 adverse events were reported during the study (Table 2); five were infusion-
related reactions during the first RTX administration (all grade I according to the CTCAE
classification). No infusion-related reaction was reported with belimumab. All but one of 26
adverse events occurring during the study were grade I, and eight were possibly related to
treatment (bronchitis, n=2; nasopharyngitis, n=3; arthralgia, n=1; candida vulvovaginitis, n=1;
cystitis, n=1). One patient experienced grade II serum sickness with moderate arthralgia and
rash one day after the second infusion of RTX.
Gammaglobulin levels were systematically monitored during the study (Figure 1A-D). We
observed no severe infection and no severe hypogammaglobulinemia (total serum
immunoglobulin < 4 g/L or IgG < 4.5 g/L). We observed a significant decrease in IgG and
IgM titers (Figure 1 and supplementary Table 2) between baseline and W24 (0,98 g/L and
0,42 g/L decrease in median IgG and IgM titers, respectively). One patient experienced

10
moderate hypogammaglobulinemia (total serum Ig titers: 4.9 g/dL, IgG: 4.7 g/L) at W12,
which was transient and recovered at W24. One patient had IgM titers < 0.4 g/dl at W12 (IgM
baseline: 0.7 g/L) that did not recover at W52. IgA titers did not vary throughout the study.
Efficacy
Thirteen (86.7%) patients achieved an initial overall response at W12, including nine (60%)
with CR (Figure 2). Two patients had a response at W7 and W8, respectively; other patients
achieved a response after W4. One non-responder had bleeding symptoms at W4 and required
thrombopoietin receptor agonists at W6. No other patient required ITP-directed therapy until
W30. Among initial responders (R), one relapsed at W30, with moderate bleeding
(cutaneous), and one eventually achieved CR at W36. At W52, the median platelet count
among responders was 189 x109/L [range 69-416] and 12/15 (80%) patients achieved overall
response (95% confidence interval [CI], 52-96), including ten (66.7%) with CR (95% CI 38-
88). After a follow-up of 18 months, one patient with an initial complete response eventually
relapsed at 16 months (supplemental figure 3).
Vaccine response
All patients had received vaccination with pneumococcal polysaccharide vaccine
(Pneumovax-23®, n=2) or conjugate vaccine PCV13 (Prevenar 13®, n=13) at least 15 days
before inclusion [range 15-90 days]. When considering a protective threshold ≥ 1 µg/ml for
anti-pneumococcal antibodies,13 13 patients were protected for at least 11 of the 13 serotypes
tested (1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, 23F), and two patients (who had
received Prevenar 13®) were protected for eight serotypes at baseline (Supplemental Table 3).
At W52, eight (53%) patients had no change (n=6) or < 2 serotypes (n=2) loss in protection
among the 13 serotypes tested. Two patients who were protected for eight serotypes at

11
baseline had lost two and four other serotypes, respectively, at W52. Finally, five patients
(30%) had lost protection for a median of seven serotypes [range 4-8]. Overall, at W52, 11
(73%) patients had protective titers for at least 11 serotypes. All patients had received
vaccination with tetanus and measles at different times before enrollment. Fourteen patients
(93%) had no significant change in anti-tetanus antibody titers between W0 and W52. There
were also no significant changes in anti-measles antibody titers, which remained at protective
level > 200 UA/m (Protective > 16.5 UA/m) for all patients at W52.
Antiplatelet antibody testing
Direct MAIPA was performed at inclusion in all but one patient and was positive in ten (71%)
patients, including nine with glycoprotein IIb/IIIa (GpIIb/IIIa) specificity, and one with
GpIb/IX specificity (Supplemental Table 4). Among these patients, seven (70%) achieved
response and had negative MAIPA results at W52, two achieved response (one CR and one R)
and still had anti-GpIIb/IIIa antibodies at W52, and one did not respond but had negative
MAIPA results at W52.
Immunological analysis
To precisely assess the impact of blocking BAFF concomitantly with B-cell depletion on B-
and T-cell subsets, we analyzed in parallel a prospective cohort of 12 ITP patients who
received RTX without belimumab as a standard of care (Supplemental table 5). As previously
reported, we observed a significant increase in BAFF serum levels in patients receiving RTX
alone at W12, W24, W36 and W52 (all p<0.001) after RTX, as compared to baseline. In the
RITUX-PLUS study, belimumab treatment effectively reduced BAFF levels at W12 as
compared to baseline (1210±248 vs 90±38 pg/ml, p<0.0001). BAFF levels started to return to

12
baseline at W24 (730±294 pg/ml, p<0.01), then strongly increased at W36 (2199±1498 pg/ml,
p<0.0001) and reached a plateau at W52 (2937±1561 pg/ml p<0.0001) (Figure 3A). BAFF
levels at W36 and W52 did not significantly differ between patients receiving belimumab +
RTX in the study and control patients receiving RTX alone.
To evaluate the effect of the RTX and belimumab combination on B-cell depletion and
reappearance, we analyzed circulating CD19+ B cells in both cohorts at baseline, W4, W12,
W24, W36, and W52 (Figure 3B). All patients showed complete depletion of circulating
CD19+ B cells at W4 and W12 (Figure 3C).
Reappearance of B cells in peripheral blood varied among patients. We observed no
significant delay in B-cell reconstitution in patients receiving belimumab plus RTX versus
controls receiving RTX alone, despite a slight difference at W36. Transitional B cells
(CD19+IgD+CD24+CD38+CD10+), which are precursors of naïve B cells in peripheral
blood,14,15 emerged early during B-cell reconstitution (Figure 3D-E). Indeed, two out of 15
patients receiving belimumab showed transitional B cells in peripheral blood at W24 as
compared with five out of 12 patients receiving RTX alone. All but one patient in both groups
showed naïve and transitional B cells at W52. The absolute number of CD19+ cells remained
significantly decreased at W52 in both groups as compared to baseline, and B-cell depletion
mainly affected memory B cells and IgD+CD27+ B cells (Figure 3F-G).
A previously reported, the number of circulating CD27highCD38high cells (mainly plasmablasts
expressing the Ki67 marker) was increased at baseline in ITP patients as compared with
healthy donor controls (n=11, p<0.05 supplemental Figure 4). A marked reduction of
plasmablasts/PCs was observed from W4 and lasted until W52, when the number of
circulating plasmablasts was low and comparable to that in healthy donors (Figure 3H and
supplemental Figure 5).

13
Because changes in T-cell homeostasis have been described with RTX, we investigated
peripheral T-cell compartments before and after treatment. We observed no significant
changes in the distribution of CCR7+CD45RA+ naive (TN), CCR7−CD45RA− memory (TEM),
and CCR7+CD45RA− central memory (TCM) in CD4+ and CD8+ cells. The expression of
CD38 and HLA-DR activation markers on CD4+ or CD8+ T cells was not modified with
treatment. Finally, we observed no significant change in CD4 T-cell polarization
(TH1/TH2/TH17) based on the expression of CXCR3, CXCR5, CCR6 (Supplemental Figure
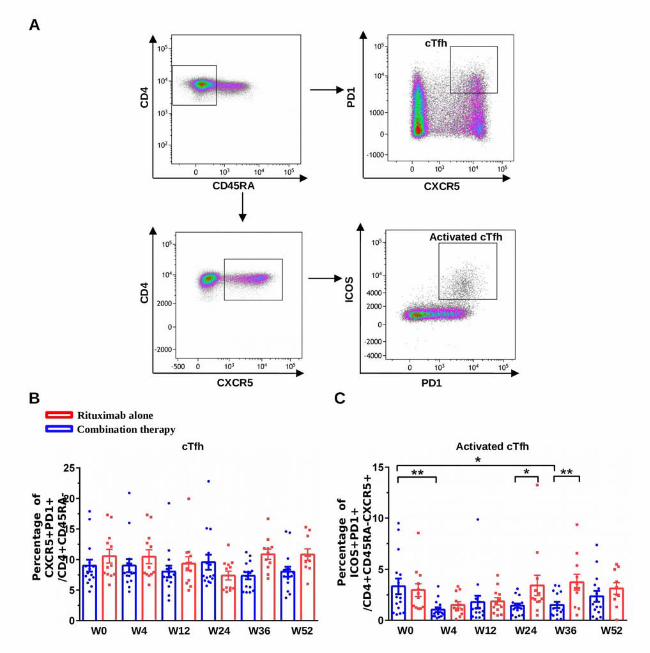
6). By contrast, the activated subset of circulating follicular helper T cells (activated cTfh)
identified as CD4+CD45RA-CXCR5+ Inducible T-cell costimulator (ICOS)+ programmed
death1 (PD1)+ cells16 (Figure 4A) was increased at baseline in ITP patients as compared with
healthy controls (Supplemental Figure 4). While circulating Tfh percentage remained stable
throughout the study, the percentage of activated cTfh cells was significantly decreased in
patients receiving RTX plus belimumab but not RTX alone despite a trend at W4, and
remained significantly decreased at W24 and W36 in patients receiving RTX plus belimumab
versus RTX alone (Figure 4B and Figure 4C). There was no correlation between the
response (initial response or at W52) and BAFF or cTfh (not shown).

14
Discussion
The rationale of this study was based on three observations: 1) the presence of anti-platelet
long-lived PCs in the spleen of patients who did not respond to RTX; 2) the increased BAFF
level in the spleen and serum of these patients, and 3) the observation that combining an anti-
BAFF antibody with anti-CD20 treatment induced a major depletion of long-lived PCs in a
mouse model.6,9,10 The results of this prospective phase 2b pilot trial of ITP showed that
combining RTX with five infusions of belimumab led to an overall response rate of 80% with
a 66.7% CR rate at 1 year. Although the sample size was limited, these response rates were
higher than expected with RTX alone (overall response rates of 40% to 50% at 1 year, with
30% of CR, according to most previous studies conducted in ITP).4,5,17,18 These response rates
were also higher but closer to those obtained with RTX and dexamethasone19 or RTX
associated with high-dose dexamethasone and ciclosporin.20 Hence, these results are
promising and provide a real proof of concept for this new combination.
Most consecutive patients included in this study were women with persistent ITP. Disease
duration < 12 months, young age and female sex have been found associated with better
outcomes,4,5,17,18 which could represent a bias although these factors were not associated with
the overall long-term response in our large French prospective registry study.21
The combination strategy was well tolerated, with no severe adverse events and in particular
no severe infection. Despite a significant decrease in IgG and IgM titers, we did not observe
severe hypogammaglobulinemia. This finding contrasted with the results of the phase 2a
study conducted in severe systemic lupus erythematosus, in which severe
hypogammaglobulinemia developed in three out of 16 patients, with IgG titers < 4.5 g/L.22
However, these patients had previously received immunosuppressive therapies, which was not
the case for our patients. No significant changes in IgG or IgM titers were observed in patients
receiving two infusions of 1000 mg of RTX or 375 mg/m2 once weekly for four weeks.5,23,24,25

15
Therefore, the slight decrease in IgG/IgM titers may reflect the impact on splenic PCs,
because anti-tetanus and anti-measles antibody titers, which are secreted by bone-marrow
long-lived PCs, remained stable over time. The study was not specifically designed to assess
the vaccine response; indeed, the timing of pneumococcal vaccination was heterogenous, and
two patients received T-cell–independent vaccines. Half showed no decrease in serological
protection for most serotypes with treatment, and only four patients had lost protection for
more than seven serotypes. In the absence of a control cohort, it was not possible to measure
the specific impact of combination therapy versus rituximab given alone. Vaccine-induced
antibody titers against measles and tetanus toxoid were not reduced at one year, suggesting
that bone-marrow long-lived PCs were not affected by the combination therapy. Altogether,
these results suggest that belimumab and RTX did not induce significant immunodepression.
From an immunological perspective, achieving a sustained CR indicates that pathogenic PCs
were efficiently targeted. This is exemplified by the disappearance of platelet autoantibodies
in all but one patient with an initial positive test. Despite the absence of a control cohort to
clearly assess the impact of this combination on PCs, our results support previous results
obtained in mouse models showing that combination of RTX and belimumab inhibits the
emergence of pathogenic splenic long-lived PCs and anti-platelets antibodies.10 Of note, the
addition of belimumab had no significant impact on residual circulating PCs/plasmablasts,
which were mainly expressing IgA and have been described as originating from resident
mucosal B cells.26
The kinetics of B-cell repopulation seemed similar regardless of belimumab exposure. We
observed a slight delay in the beginning of B-cell reconstitution (i.e., reappearance of naïve
and transitional B cells), but at W52, all but one patient had detectable B cells in peripheral
blood. As previously reported, the memory B-cell pool was profoundly depleted until W52 in
both cohorts.

16
Elevated BAFF levels may lower the stringency of the B-cell selection and allow for rescuing
autoreactive cells.27 This hypothesis is supported by studies showing that negative selection of
high-affinity DNA-reactive B cells was impaired by increased levels of BAFF during B-cell
depletion in an auto-immune mouse model.28 This was the basis for studies conducted in
systemic lupus erythematosus in which belimumab is maintained for more than 52 weeks after
RTX. In the present study, the last belimumab infusion was administered at W12 and resulted
in a complete blockade of BAFF at least until W24. Therefore, B-cell reconstitution occurred
in a milieu with increased BAFF levels. Maintaining belimumab for six to nine months after
RTX may allow for dampening BAFF levels during B-cell reconstitution and improve the
stringency of B-cell selection, thus limiting the risk of relapse after B-cell reconstitution.
Our results also suggest that RTX followed by belimumab had an unexpected effect on
activated cTfh cells, which are essential for germinal center formation, B-cell affinity
maturation and plasmablast generation.29 In humans, the majority of cTfh are central memory
T cells expressing PD1 but no ICOS,16 but germinal center recruitment and support for B cell
differentiation requires up-regulation of ICOS.30 Splenic Tfh cells can contribute to ITP
pathogeny and, as previously reported,7 the number of activated cTfh cells was increased at
baseline in the peripheral blood of ITP patients. Although some cTfh cells were shown to
express BAFF-R in systemic lupus erythematosus, this was not the case in ITP (data not
shown),31 so their sensitivity to belimumab remains unexplained so far. Of note, local BAFF
production by Tfh cells has been identified as an important factor for promoting germinal
center B-cell survival.32 Belimumab might also prevent, through such pleiotropic effects, the
re-emergence of germinal centers in lymphoid organs at the time of B-cell repopulation, an
effect that would be further strengthened by extending the duration of its administration.
These preliminary results support a new rationale for the addition of BAFF blockade to B-cell
depletion in auto-immune diseases.

17
The main limitations of this pilot exploratory and single-center trial are the sample size and
the open design. These results should be confirmed in a multicenter double-blind randomized
prospective trial.
In conclusion and despite these limitations, in adult ITP, adding belimumab to RTX at the
initial phase of B-cell depletion seems to be a promising strategy with high efficacy and
acceptable safety.
18
Role of the funding source
This study was initiated by the investigators and partially financed with an open grant from
GSK, which played no role in designing the study, collecting and analyzing the data, or
writing the article. The study was funded by a grant from Programme Hospitalier de
Recherche Clinique - PRTS 2013 (Ministère de la Santé). The sponsor was Assistance
Publique – Hôpitaux de Paris (Département de la Recherche Clinique et du Développement).

19
Acknowledgments
This study was initiated by the investigators and partially financed with an open grant from
GSK, which played no role in designing the study, collecting and analyzing the data, or
writing the article. The study was funded by a grant from Programme Hospitalier de
Recherche Clinique - PRTS 2013 (Ministère de la Santé). The sponsor was Assistance
Publique – Hôpitaux de Paris (Département de la Recherche Clinique et du Développement).
The authors thank Laura Smales for editorial assistance; Roxane Kaponou Johnson and Alexis
Vandenberghe for technical assistance. E. Crickx was supported by a Poste d’accueil Inserm.
Authorship Contributions
M.Ma designed the study and initiated this work; M.Ma, B.G., M.Mi., IA and E.C wrote the
report; all authors made substantial contributions to acquisition of data, revised the article
critically and gave final approval of the manuscript to be submitted.
Conflict of Interest Disclosures
M.Ma received funds for research from GSK, and received fees from LFB. B.G. served as an
expert for Amgen, Novartis, LFB and Roche. He received funds for research from Amgen and
Roche. M.Mi. received consultancy fees from Amgen, Novartis and Argenx. D. G. received
consultancy fees from Novartis and Shire Takeda.

20
References
1. Cines DB, Cuker A, Semple JW. Pathogenesis of immune thrombocytopenia. Presse Médicale Paris Fr. 1983 2014;43(4 Pt 2):e49-59.
2. Audia S, Mahévas M, Samson M, Godeau B, Bonnotte B. Pathogenesis of immune thrombocytopenia. Autoimmun Rev. 2017;16(6):620-632.
3. Moulis G, Germain J, Comont T, et al. Newly diagnosed immune thrombocytopenia adults: Clinical epidemiology, exposure to treatments, and evolution. Results of the CARMEN multicenter prospective cohort. Am J Hematol. 2017;92(6):493-500.
4. Khellaf M, Charles-Nelson A, Fain O, et al. Safety and efficacy of rituximab in adult immune thrombocytopenia: results from a prospective registry including 248 patients. Blood. 2014;124(22):3228-3236.
5. Chugh S, Darvish-Kazem S, Lim W, et al. Rituximab plus standard of care for treatment of primary immune thrombocytopenia: a systematic review and meta-analysis. Lancet Haematol. 2015;2(2):e75-81.
6. Mahévas M, Patin P, Huetz F, et al. B cell depletion in immune thrombocytopenia reveals splenic long-lived plasma cells. J Clin Invest. 2013;123(1):432-442.
7. Audia S, Rossato M, Santegoets K, et al. Splenic TFH expansion participates in B-cell differentiation and antiplatelet-antibody production during immune thrombocytopenia. Blood. 2014;124(18):2858-2866.
8. Mahévas M, Michel M, Vingert B, et al. Emergence of long-lived autoreactive plasma cells in the spleen of primary warm auto-immune hemolytic anemia patients treated with rituximab. J Autoimmun. 2015;62:22-30.
9. Mahévas M, Michel M, Weill J-C, Reynaud C-A. Long-lived plasma cells in autoimmunity: lessons from B-cell depleting therapy. Front Immunol. 2013;4:494.
10. Thai L-H, Le Gallou S, Robbins A, et al. BAFF and CD4+T cells are major survival factors for long-lived splenic plasma cells in a B-cell-depletion context. Blood. 2018;131(14):1545-1555.
11. Mackay F, Schneider P. Cracking the BAFF code. Nat Rev Immunol. 2009;9(7):491-502.
12. Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113(11):2386-2393.
13. Grabar S, Groh M, Bahuaud M, et al. Pneumococcal vaccination in patients with systemic lupus erythematosus: A multicenter placebo-controlled randomized double-blind study. Vaccine. 2017;35(37):4877-4885.
14. Anolik JH, Friedberg JW, Zheng B, et al. B cell reconstitution after rituximab treatment of lymphoma recapitulates B cell ontogeny. Clin Immunol Orlando Fla.

21
2007;122(2):139-145.
15. Sanz I, Wei C, Jenks SA, et al. Challenges and Opportunities for Consistent Classification of Human B Cell and Plasma Cell Populations. Front Immunol. 2019;10:2458.
16. Locci M, Havenar-Daughton C, Landais E, et al. Human circulating PD-1+CXCR3-CXCR5+ memory Tfh cells are highly functional and correlate with broadly neutralizing HIV antibody responses. Immunity. 2013;39(4):758-769.
17. Lucchini E, Zaja F, Bussel J. Rituximab in the treatment of immune thrombocytopenia: what is the role of this agent in 2019? Haematologica. 2019;104(6):1124-1135.
18. Zaja F, Volpetti S, Chiozzotto M, et al. Long-term follow-up analysis after rituximab salvage therapy in adult patients with immune thrombocytopenia. Am J Hematol. 2012;87(9):886-889.
19. Bussel JB, Lee CS, Seery C, et al. Rituximab and three dexamethasone cycles provide responses similar to splenectomy in women and those with immune thrombocytopenia of less than two years duration. Haematologica. 2014;99(7):1264-1271.
20. Choi PY-I, Roncolato F, Badoux X, Ramanathan S, Ho S-J, Chong BH. A novel triple therapy for ITP using high-dose dexamethasone, low-dose rituximab, and cyclosporine (TT4). Blood. 2015;126(4):500-503.
21. Deshayes S, Khellaf M, Zarour A, et al. Long-term safety and efficacy of rituximab in 248 adults with immune thrombocytopenia: Results at 5�years from the French prospective registry ITP-ritux. Am J Hematol. 2019;94(12):1314-1324.
22. Kraaij T, Kamerling SWA, de Rooij ENM, et al. The NET-effect of combining rituximab with belimumab in severe systemic lupus erythematosus. J Autoimmun. 2018;91:45-54.
23. Stasi R, Pagano A, Stipa E, Amadori S. Rituximab chimeric anti-CD20 monoclonal antibody treatment for adults with chronic idiopathic thrombocytopenic purpura. Blood. 2001;98(4):952-957.
24. Cooper N, Stasi R, Cunningham-Rundles S, et al. The efficacy and safety of B-cell depletion with anti-CD20 monoclonal antibody in adults with chronic immune thrombocytopenic purpura. Br J Haematol. 2004;125(2):232-239.
25. Arnold DM, Heddle NM, Carruthers J, et al. A pilot randomized trial of adjuvant rituximab or placebo for nonsplenectomized patients with immune thrombocytopenia. Blood. 2012;119(6):1356-1362.
26. Mei HE, Frölich D, Giesecke C, et al. Steady-state generation of mucosal IgA+ plasmablasts is not abrogated by B-cell depletion therapy with rituximab. Blood. 2010;116(24):5181-5190.
27. Liu Z, Davidson A. BAFF and selection of autoreactive B cells. Trends Immunol. 2011;32(8):388-394.
22
28. Boneparth A, Woods M, Huang W, Akerman M, Lesser M, Davidson A. The effect of BAFF inhibition on autoreactive B cell selection in murine SLE. Mol Med. 2016;22:173-182.
29. Ueno H, Banchereau J, Vinuesa CG. Pathophysiology of T follicular helper cells in humans and mice. Nat Immunol. 2015;16(2):142-152.
30. Heit A, Schmitz F, Gerdts S, et al. Vaccination establishes clonal relatives of germinal center T cells in the blood of humans. J Exp Med. 2017;214(7):2139-2152.
31. Coquery CM, Loo WM, Wade NS, et al. BAFF regulates follicular helper t cells and affects their accumulation and interferon-γ production in autoimmunity. Arthritis Rheumatol. 2015;67(3):773-784.
32. Goenka R, Matthews AH, Zhang B, et al. Local BLyS production by T follicular cells mediates retention of high affinity B cells during affinity maturation. J Exp Med. 2014;211(1):45-56.

23
Table 1: Baseline characteristics of patients with immune thrombocytopenia (ITP)
receiving rituximab and belimumab.
CST: corticosteroids, IVIg: Intravenous immunoglobulin
Age/Gender ITP
duration (months)
Bleeding manifestations
Treatments received before inclusion
Nadir platelet count during the month before
inclusion (x 10 9/L) 25/F 11 Cutaneous CST 16 29/F 4 Cutaneous + mucosal CST 3
42/F 15 No CST, IVIg,
hydroxychloroquine 3
51/F 15 Cutaneous CST, Dapsone 28 31/F 5 Cutaneous CST, IVIg 16 57/F 52 Cutaneous CST, IVIg 27
39/F 44 Cutaneous CST,
hydroxychloroquine 18
33/F 11 Cutaneous CST,
hydroxychloroquine 18
70/F 3 Cutaneous CST,
hydroxychloroquine 18
66/M 42 Cutaneous CST, IVIg, dapsone, hydroxychloroquine
9
66/M 5 Cutaneous + mucosal CST, IVIg, dapsone 15 20/F 4 Cutaneous CST, IVIg, romiplostim 15 50/M 31 Cutaneous + mucosal CST, IVIg 6 54/F 4 Cutaneous CST, eltrombopag 7
57/F 4 Cutaneous + mucosal CST, IVIg, vinblastin,
romiplostim, eltrombopag
17
24
Table 2. Adverse events reported in the study.
CTCAE: National Cancer Institute Common Terminology Criteria for Adverse Events; RTX: rituximab; W: week
Patients Infusion related reactions Adverse events, CTCAE grade, imputability
1 Yes, Throat itching, grade I, (RTX W0) Arthralgia (W2- W8) grade I, possible
2 Sore throat, grade I, (RTX W0) No
3 No Transient hypereosinophilia < 1000 /mm3 (W40) treated with zentel/stromectol, grade 1, not related
4 No Gluteus medius tendinitis (W8-W12), grade I, not related Nasopharyngitis (W10), grade I possible Supraspinatus tendinitis (W24), grade I, not related
5 Yes, Throat itching, grade I, (RTX W0)
Serum thickness (W2), grade I, related Candida vulvovaginitis (W8), grade I, not related
6 No Rhinorrhea (W2) and (W12), grade I, not related Bronchitis (W5), possible Pain extensor muscles of the forearm, (W24), grade I, not related
7 Headache, grade I, (RTX W0) Acute cystitis (W4), grade I, possible
8 No Arthralgia (W3), thoracic pain (W3), grade I, not related Viral conjunctivitis (W4), grade I, not related Arthralgia (W52), grade I, not related
9 No Rhinorrhea (W8), grade I, not related Pharyngitis (W4), grade I, possible Bronchitis (W50), grade I, possible
10 No Gout arthritis (W44), grade I, not related
11 No Increased number of monocytes after TPO-RA, grade I, not related
12 Yes, abdominal discomfort grade I, (RTX W0)
Nasopharyngitis (W20), myalgia (W20), grade I, possible Knee pain (W52), grade I, not related
13 No Bronchitis (W9), grade I, possible Memory problems W14, grade I, not related Erectile dysfunction W36, grade I, not related
14 No Low back pain (W12), grade I, not related
15 No Bronchitis (W0-W2), grade I, possible

25
Figure legends
Figure 1. Serum level of total gammaglobulins and immunoglobulin (Ig) isotypes (IgG, IgA, IgM) during the study of rituximab and belimumab combined. Serum level of total gammaglobulins (A) and IgG (B), IgM (C), and IgA (D) were assessed by nephelometry at week 12 (W12), W24, W36, W52. Dotted line represents normal threshold for each isotype. *P<0.05, **P<0.01, ***P<0.001; ns, not significant Figure 2. Efficacy of rituximab and belimumab combination in adults with persistent and chronic immune thrombocytopenia (ITP). (A) Outcome at week 4 (W4), W12, W24, W36, and W52 according to international recommendations. Complete response (CR) was defined by a platelet count >100 x109/L and response (R) by a platelet count 30 to 100 x109/L with at least a 2-fold increase from baseline. Non-responders are labeled in red; platelet counts were censured when an ITP-directed therapy was started. (B) Evolution of platelet count for each patient during the study. CR, complete response; R, response; NR, no response Figure 3. B-cell activating factor (BAFF) and B-cell subsets in ITP patients receiving the combination therapy or rituximab alone. (A) BAFF concentrations were assessed by ELISA in serum of patients receiving rituximab and belimumab (in blue) or rituximab alone (in red) at week 0 (W0), W12, W24, W36 and W52. Data are mean ± SEM (pg/ml). (B) Gating strategy of B-cell subpopulations. Single lymphoid cells on peripheral blood mononuclear cells (PBMCs) were gated by using scatter parameters, and dead cells were eliminated by using zombie violet. Plasmablasts/plasma cells (PBs/PCs) were defined as CD27hiCD38hi cells among CD3-CD14-CD16- cells. After excluding CD3/CD14/CD16-positive cells and PBs/PCs from the CD19+ gate, B-cell subsets were separated according to their expression of CD27 and IgD and defined as memory B cells (CD27+IgD-), CD27+IgD+ B cells, and naïve B cells (CD27-IgD+). Transitional B cells were defined as CD38hiCD24hiCD10+ cells among naïve B cells. (C) Circulating B-cell subset count per million PBMCs at W0, W4, W12, W24, W36 and W52. ****P<0.0001 Figure 4. Rituximab and belimumab combination affects activated circulating T follicular helper cells. (A) Gating strategy for cTfh cells. After gating on CD4+CD45RA- memory T-CD4+ cells in whole blood, cTfh cells were defined as CXCR5+PD1+, and activated cTfh cells as CXCR5+PD1+ICOS+. (B) Percentages of cTfh and (C) Activated Tfh cells at week 0 (W0), W4, W12, W24, W36 and W52 in patients receiving rituximab and belimumab or rituximab alone. *P<0.05, **P<0.01




Supplemental Table 1. List of monoclonal antibodies used for flow cytometry.
Panel Antigen Fluorochrome Clones Company
T cell subsets CXCR5 BB515 RF8B2 BD bioscience
PD1 PE EH12.1 BD bioscience
CXCR3 PE-CY5 IC6/CXCR3 BD bioscience
CCR6 PeCy7 11A9 BD bioscience
CD45RA APC HI100 BD bioscience
CD3 AF700 UCHT1 BD bioscience
HLA-DR APC-H7 G46-6 BD bioscience
ICOS BV421 DX29 BD bioscience
CCR7 BV605 3D12 BD bioscience
CD27 BV711 L128 BD bioscience
CD4 BV786 SK3 BD bioscience
CD38 PerCy5,5 HIT2 BD bioscience
B cell subsets CD24 FITC ML5 BD bioscience
CD3 PE UCHT1 BD bioscience
CD14 PE M5E2 BD bioscience
CD16 PE 3G8 BD bioscience
IgD PE CF594 IA6-2 BD bioscience
CD38 PerCy5,5 HIT2 BD bioscience
CD27 PE CY7 M-T271 BD bioscience
CD19 AF700 HIB19 BD bioscience
CD10 APC HI10A BD bioscience

Supplemental Table 2. Serum level of total gammaglobulins and immunoglobulin (Ig) isotypes (IgG, IgA, IgM) during the study of
rituximab and belimumab combined.
W0 W12 W24 W36 W52
ΔValue W0/W24
Gammaglobulins 10,6 9 9 9,05 9 1,2 IgG 11 9,3 9,405 9,01 9,745 0,98 IgM 1,11 0,8 0,74 0,67 0,74 0,42 IgA 1,8 1,42 1,53 1,41 1,71 0,3
Median gammaglobulins, IgG, IgM and IgA titers at W ΔValue W0/W24 represents the decrease of median gammaglobulin
titers between W0 and W24.

Supplemental Table 3: Antibody titers to the 13 serotypes of pneumococcus serotypes contained in Prevenar 13® (1, 3, 4, 5, 6A, 6B, 7F, 9V,
14, 18C, 19A, 19F and 23F) for each patient at week 0 (W0) and W52.
Serotype
1 3 4 5 6A 6B 7F 9V 14 18C 19A 19F 23F
Concentration µg/ml
Patient W0 W52 W0 W52 W0 W52 W0 W52 W0 W52 W0 W52 W0 W52 W0 W52 W0 W52 W0 W52 W0 W52 W0 W52 W0 W52
1 7.3 4 5 1.4 11 6.7 5.3 3.9 2.7 1.7 7.4 4.9 19 6.6 40 18 103 84 6.4 2.7 2.6 2 38 29 18 10
2 9.37 2.4 1 0.66 1.8 0.36 3.9 0.71 2.8 0.67 7.8 1.3 9.8 2.4 1.9 0.27 6.6 1.44 17 4.4 25 6.6 8.8 2.6 2.7 0.38
3 23 13 0.2 0.22 6.6 4.1 12 6.9 99 73 82 39 16 5.8 3.2 1.7 48 52 17 10 26 20 11 6.7 177 70
4 12 10 1.7 1.8 9.8 8 15 13 69 58 8.5 6.7 3.1 2.7 12 8.8 20 15 4.5 3.5 14 15 18 15 11 8
5 1.6 0.54 0.89 0.43 5.4 1.4 1.8 1.1 45 16 13 4.2 20 7.9 8 3.8 51 21 4.9 2.6 11 7 21 8.4 21 7.4
6 67 93 0.51 0.29 1.5 0.42 30 29 1.5 1.1 2.4 0.97 1.6 0.79 0.93 0.47 21 23 1.4 0.79 2.5 1.4 3.3 2.4 1.6 1.2
7 23 12 1.8 1.5 33 19 11 6.9 16 13 26 17 41 26 22 12 170 78 33 20 12 8.5 115 54 95 40
8 0.65 0.24 0.33 0.24 1.4 0.62 0.52 0.22 1.6 0.91 3.2 1.7 0.98 0.45 0.64 0.24 133 68 4.7 1.9 14 4.5 27 14 25 5.5
9 12 3.2 1.8 3.6 16 4.7 36 2.7 3.8 1.7 13 2.5 15 5.3 14 4.3 5.3 1.2 19 16 8.6 3.4 7.6 2.7 17 26
10 5.8 0.39 0.27 <0.1 0.32 0.13 0.65 0.76 0.75 0.29 0.32 0.19 4.4 1.3 2.6 1.1 1.6 0.45 12 2 3.2 0.96 4.2 1.1 1 0.19
11 3 1.3 0.85 0.33 4.3 4.2 10 5.6 8.1 5.1 15 7.8 6.7 2.9 7.4 3.2 20 8.9 3.1 0.46 25 9.7 10 4.6 4.3 0.69
12 6.9 1.1 0.3 <0.1 2.9 0.52 1.6 0.35 2.7 1 5.2 1.6 6.9 0.55 2.5 0.25 25 6.7 7.1 1.9 25 7 17 4.5 86 12
13 4.7 0.53 0.84 0.13 2.3 0.43 1.9 0.13 3.5 0.38 11 0.76 28 5.9 4.1 0.55 26 5.9 3.4 0.22 19 1.1 21 1.5 107 8
14 8.1 25 0.45 1 1.7 2.3 0.98 8.6 4.1 5.3 1.7 2.9 3.5 8.5 1.7 4.5 4.7 7.8 11 14 1.3 2.4 1.9 2.8 0.45 2.5
15 2.8 1.1 0.39 0.23 2.6 0.5 1.7 0.52 2.2 1 2.7 0.94 12 4.7 1.4 0.22 3 0.61 1 0.35 30 12 4.7 1.4 1.9 0.38

Supplemental Table 4. Antiplatelet antibody testing. Results of direct monoclonal
antibody‐specific immobilization of platelet antigen (MAIPA) assay (ApDia, Turnhout,
Belgium).
W, week; Gp, glycoprotein; CR, complete response, NR, no response; R, response
Patients ITP Results of MAIPA W0
Results of MAIPA W24
Clinical outcome at
W24
Results of MAIPA W52
Clinical outcome at
W52
1 Persistent Not performed Negative CR Negative CR
2 Persistent Anti-GpIIb/IIIa Negative CR Negative CR
3 Chronic Anti-GpIIb/IIIa Negative CR Negative CR
4 Persistent Negative Not performed CR Not performed CR
5 Persistent Anti-GpIIb/IIIa Anti-GpIIb/IIIa CR Negative CR
6 Persistent Anti-GpIIb/IIIa Negative NR Negative NR
7 Chronic Anti-GpIIb.IIIa Anti-GpIIb/IIIa R Anti-GpIIb/IIIa R
8 Persistent Anti-GpIIb/IIIa Negative CR Negative CR
9 Persistent Anti-GpIIb/IIIa Anti-GpIIb/IIIa CR Negative CR
10 Chronic Anti-GpIb/IX Negative R Negative R
11 Persistent Negative Negative NR Negative NR
12 Persistent Anti-GpIIb/IIIa Anti-GpIIb/IIIa CR Negative CR
13 Chronic Undetermined Negative R Negative NR
14 Persistent Anti-GpIIb/IIIa Anti-GpIIb/IIIa CR Anti-GpIIb/IIIa CR
15 Persistent Negative Negative R Negative CR

Supplemental Table 5. Baseline clinical characteristics of patients with immune
thrombocytopenia (ITP) receiving rituximab alone.
F, female; M, male; IVIG, intravenous immunoglobulins; CST, corticosteroids; Neg, negative
Age/Sex ITP
duration (months)
Bleeding manifestations
Treatments received before inclusion
Nadir platelet count in the month before inclusion
(x 10 9/L)
Anti-nuclear antibodies
77/F 9 Yes CST, IVIG, romiplostim,
eltrombopag 6 1/400
92/F 2 Yes CST, IVIG, romiplostim,
eltrombopag 26 1/80
67/F 9 Yes CST, IVIG, romiplostim,
eltrombopag 26 1/80
47/F 3 Yes CST, IVIG 2 1/80
86/M 22 Yes CST, IVIG, dapsone,
eltrombopag 5 1/320
18/M 156 Yes IVIG, Azathioprine 30 Neg
76/F 7 Yes CST, eltrombopag, daspone 29 Neg
29/M 10 Yes CST, dapsone 7 Neg
38/F 84 Yes CST, IVIG, dapsone 22 1/500
75/M 3 Yes CST, IVIG 6 Neg
40/M 3 Yes CST 11 Neg
47/F 2 Yes CST, IVIG, revolade 28 Neg
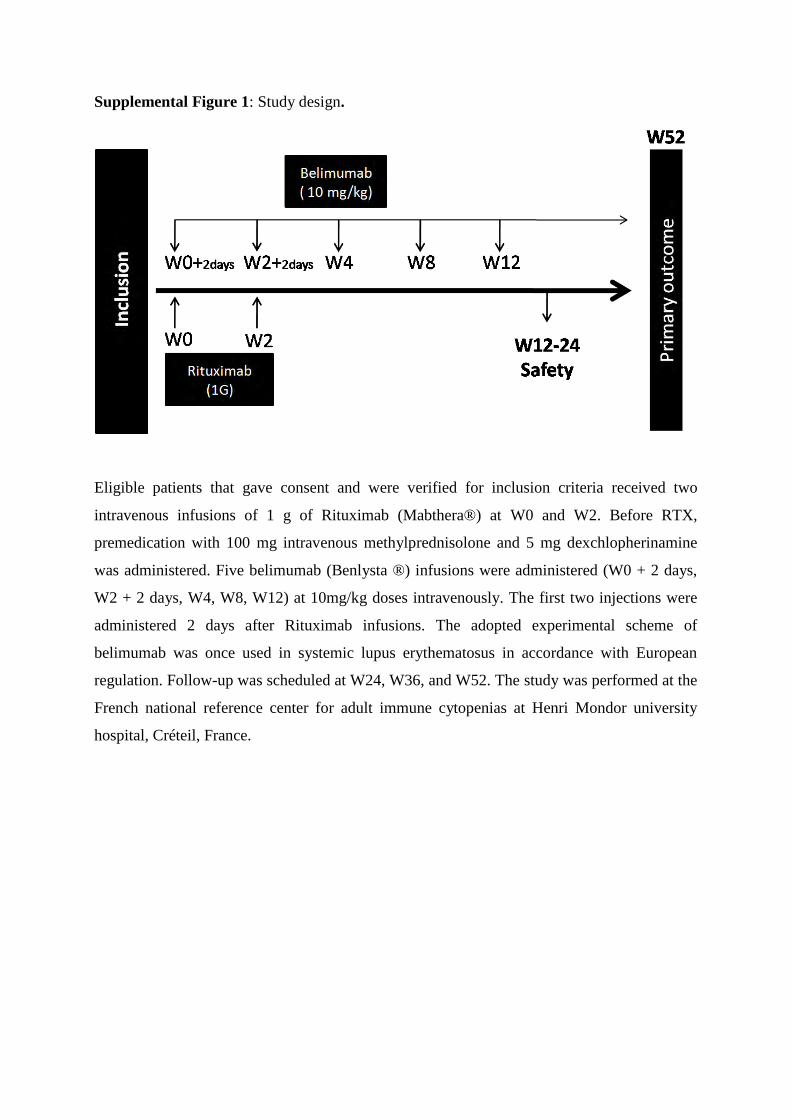
Supplemental Figure 1: Study design.
Eligible patients that gave consent and were verified for inclusion criteria received two
intravenous infusions of 1 g of Rituximab (Mabthera®) at W0 and W2. Before RTX,
premedication with 100 mg intravenous methylprednisolone and 5 mg dexchlopherinamine
was administered. Five belimumab (Benlysta ®) infusions were administered (W0 + 2 days,
W2 + 2 days, W4, W8, W12) at 10mg/kg doses intravenously. The first two injections were
administered 2 days after Rituximab infusions. The adopted experimental scheme of
belimumab was once used in systemic lupus erythematosus in accordance with European
regulation. Follow-up was scheduled at W24, W36, and W52. The study was performed at the
French national reference center for adult immune cytopenias at Henri Mondor university
hospital, Créteil, France.

Supplemental Figure 2. Gating strategy of T cell panel.
After gating on CD3+ we defined CCR7+CD45RA
+ naive (TN), CCR7
−CD45RA
− memory
(TEM), and CCR7+CD45RA
− central memory (TCM) in CD4+ and CD8+ cells. CD38 and
HLA-DR activation markers were gated on CD4+ or CD8+ T cells.

Supplemental Figure 3. Kaplan-Meier analysis of time-to-failure among initial
responders to rituximab + belimumab treatment (N=13).
0
.2
.4
.6
.8
1
Surv
ival (%
)
0 3 6 9 12 15 18Time(months)
13 13(0) 13(0) 13(0) 12(1) 12(0) 11(1)
Number at risk
95% CI Survivor function
Time-to-Failure Kaplan-Meier Curve

Supplemental Figure 4. Circulating T follicular helper (cTfh) cells and
plasmablasts/plasma cells (PBs/PCs) in patients with immune thrombocytopenia (ITP)
who were receiving the combination therapy or rituximab alone at baseline versus
healthy donors (HD). (A) Percentage of cTfh and activated cTfh cells at week 0 in ITP
patients before combination therapy (blue), rituximab treatment (red) and in healthy donors
(green). (B) Number of PBs/PCs at week 0 in ITP patients before combination therapy (blue),
rituximab treatment (Red) and in healthy donors (green). Data are mean±SEM. *P<0.05

Supplemental Figure 5. Number of plasmablasts/plasma cells (PB/PC) in healthy donors
(green) and at week W52 in ITP patients after combination therapy (blue) or rituximab
treatment (Red). Data are mean±SEM.
HD ITP ITP
0
21 0 3
41 0 3
61 0 3
81 0 3
Nu
mb
er
of
PB
/PC
/ 1
06 ly
mp
ho
id c
ell
s

Supplemental Figure 6: Frequencies of T cell subsets, activation and polarization in ITP patients treated with the combination therapy
or rituximab alone. (A) Percentage of CD4+
and CD8+ among CD3+ cells from whole blood obtained at week 0, 4, 12, 24, 36 and 52 in patients
receiving rituximab and belimumab (in blue) or rituximab alone (in red) (B) Naïve CD4+ and CD8
+ (CCR7
+CD45RA
+). (C) Effector memory
CD4+ and CD8
+ (CCR7
-CD45RA
-). (D) Central memory CD4
+ and CD8
+ (CCR7
+CD45RA
-). (E) Activated CD4+ and CD8+ T cells are defined
as HLA-DR+CD38
+. (F) Polarization of memory CD4
+ T cells using chemokine receptors, TH1 (CXCR3
+CCR6
−), TH2 (CXCR3
-CCR6
+) and
TH17 (CXCR3−CCR6
+) CD4
+ T cells. Data are mean±SEM.





























