Embed Size (px)
Citation preview
eEdE-21

No disclosure
Illustrating Neuro-Behçet disease
P Bienvenot, D Saadoun, D Galanaud, A Drier,
C Comarmond, S Gerber, F Ouamer, D Dormont, D Leclercq
Neuroradiology Department
Pitie Salpetriere Hospital
ASNR 2015 Annual Meeting

• Behçet disease (BD) is a rare multisystem immune related vasculitis
• Is worldwide spread but is reported to be most prevalent in the countries of the eastern Mediterranean and the eastern rim of Asia
• Is a nonspecific vasculitis involving various-sized vessels in multiple organs
Introduction

Introduction
• Although the pathogenesis of Behçet disease is largely unknown, association with human leukocyte antigen HLA-B51, genetic mutations including factor V Leiden and triggering by microbial antigens have been identified
• The diagnosis is primarily based on clinical criteria since: There is no specific diagnostic laboratory test There is no specific histopathologic finding
• The classical triad of oral and genital ulcerations with uveitis was originally described by a Turkish dermatologist (Hulusi Behçet) in 1937

Introduction
1. Recurrent oral ulcers
2. Plus two of the following features:
recurrent genital ulcers eye lesions (anterior and posterior uveitis and retinal
vasculitis) skin lesions (erythema nodosum, pseudofolliculitis,
papulopustular lesions and acneiform nodules) positive pathergy test
According to the International Study Group for Behçet disease, the diagnosis is based on the presence of these criteria:

Introduction
• BD has a multiorgan involvement
• Other structures reported to be involved through the course of the disease are the cardiovascular, pulmonary, gastrointestinal and central nervous (CNS) systems
• The frequency of neurologic manifestations of BD ranges from 10% to 50% of patients

Introduction• Neurologic involvement in BD is one of the most devastating
manifestations of the disease and usually occurs 1–10 years after the first symptom of BD has appeared
• Diagnosis becomes challenging when the first symptom of BD is neurologic (as in 3 to 33% of cases)
• The neurological manifestations of BD are classified as parenchymal and non parenchymal
• The 2 types rarely occur in the same individual, and their pathogeneses are probably different
• Non parenchymal involvement is less frequent
(less than a third of cases of BD neurologic involvement)

Parenchymal involvementLocation
• Parenchymal involvement of Behçet disease, also called neurobehçet disease (NBD), most often involves the brainstem, especially the meso-diencephalic junction and the pons

Parenchymal involvementLocation
• The next most common sites of involvement are the thalamus and the basal ganglia

Parenchymal involvementLocation
• It can also be located in the cerebral hemispheres, the cerebellum or the spinal cord
• Optic neuritis is rare

Parenchymal involvementClinical manifestations
• The most frequent clinical manifestations of NBD are non specific and include:
HeadachePyramidal syndromeBrainstem syndromeCerebellar ataxiaSphincter impotenceEncephalitis with cognitive impairement
• Meningitis may be absent in about 30% of cases
• Inital acute phase with acute attacks followed by chronic phase with secondary progressive evolution

• CT is of little diagnostic help and may reveal areas of low attenuation in the brainstem, basal ganglia, thalami or cerebral hemispheres, with possible homogeneous or patchy enhancement
• Magnetic resonance (MR) is the most accurate exam for NBD diagnostic
Parenchymal involvementTypical pattern in NBD acute phase

• Most frequent location = brainstem
• Typical MR pattern reveals:
Ill defined areas of high signal intensity on T2-WI and iso- or hypo-intensity on T1-WI
Swelling
No restricted diffusion
Parenchymal involvementTypical pattern in NBD acute phase

No enhancement or nodular and irregular enhancement (blood brain barrier disruption)
Haemorrhagic signal
Parenchymal involvementTypical pattern in NBD acute phase
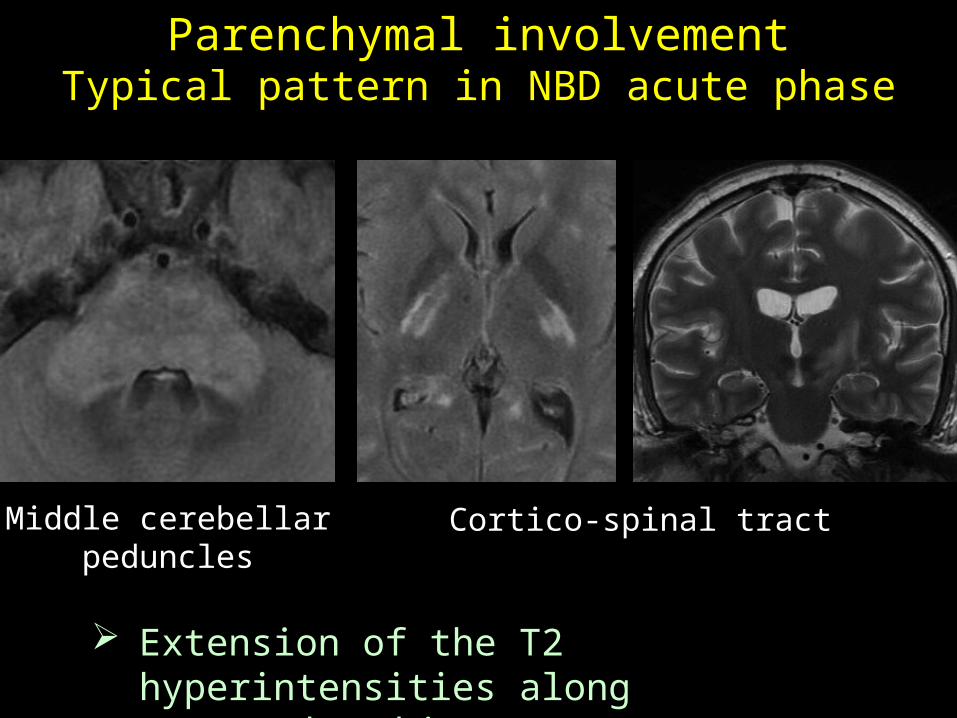
Middle cerebellarpeduncles
Cortico-spinal tract
Extension of the T2 hyperintensities along the white matter (WM)
tracts
Parenchymal involvementTypical pattern in NBD acute phase
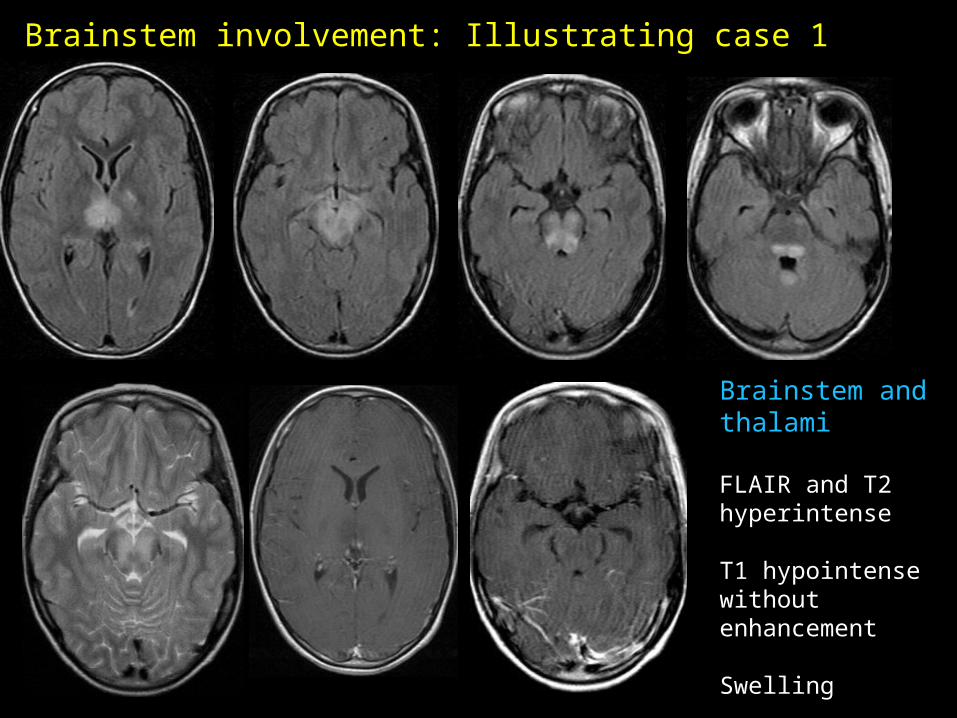
Brainstem and thalami
FLAIR and T2 hyperintense
T1 hypointense without enhancement
Swelling
Brainstem involvement: Illustrating case 1

Brainstem
FLAIR hyperintense
Swelling
Irregular peripheralenhancement
Brainstem involvement: Illustrating case 2

Brainstem
FLAIR and T2 hyperintense
Swelling
Faint irregular Enhancement
Brainstem involvement: Illustrating case 3
Brainstem
FLAIR hyperintense
Swelling
Haemorrhage
T1 hypointense
Irregular enhancement
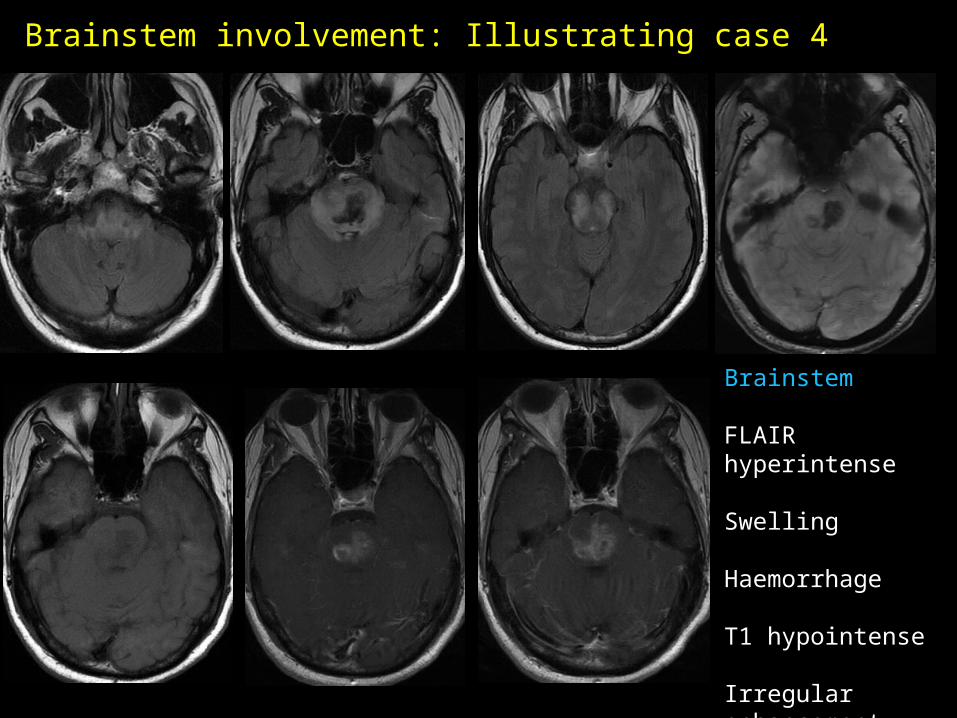
Brainstem involvement: Illustrating case 4
Brainstem
FLAIR hyperintense
Swelling
Extension along the cortico-spinal tracts
Faint enhancement
Haemorrhage on T2* and SWI(SWI > T2*)
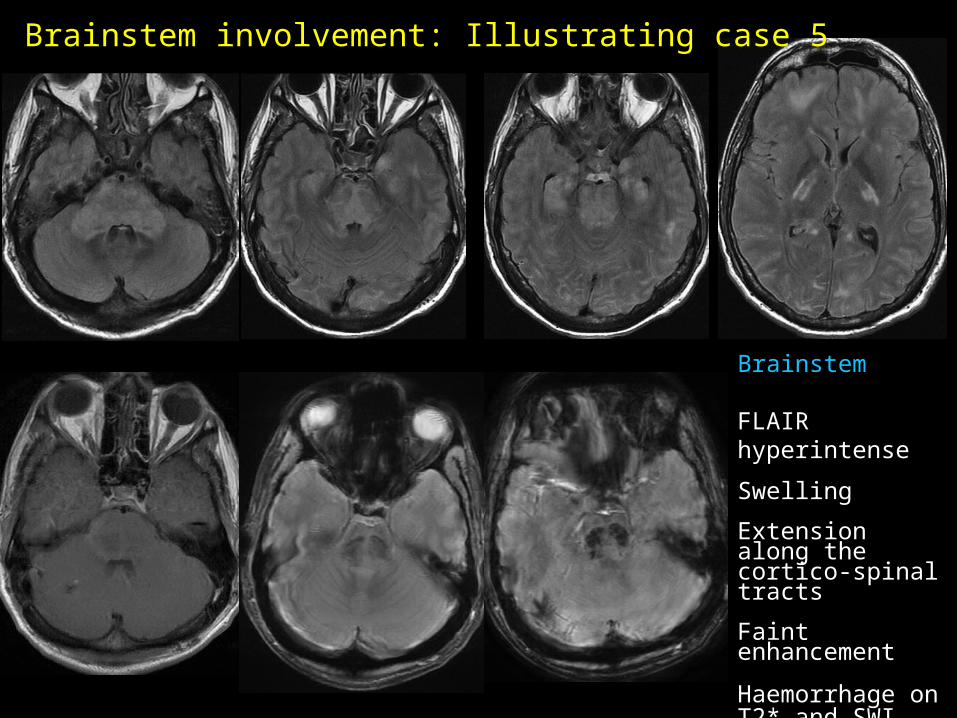
Brainstem involvement: Illustrating case 5
Brainstem
FLAIR hyperintense
Asymetrical extension along left cortico-spinal tract and left middle cerebellar peduncle
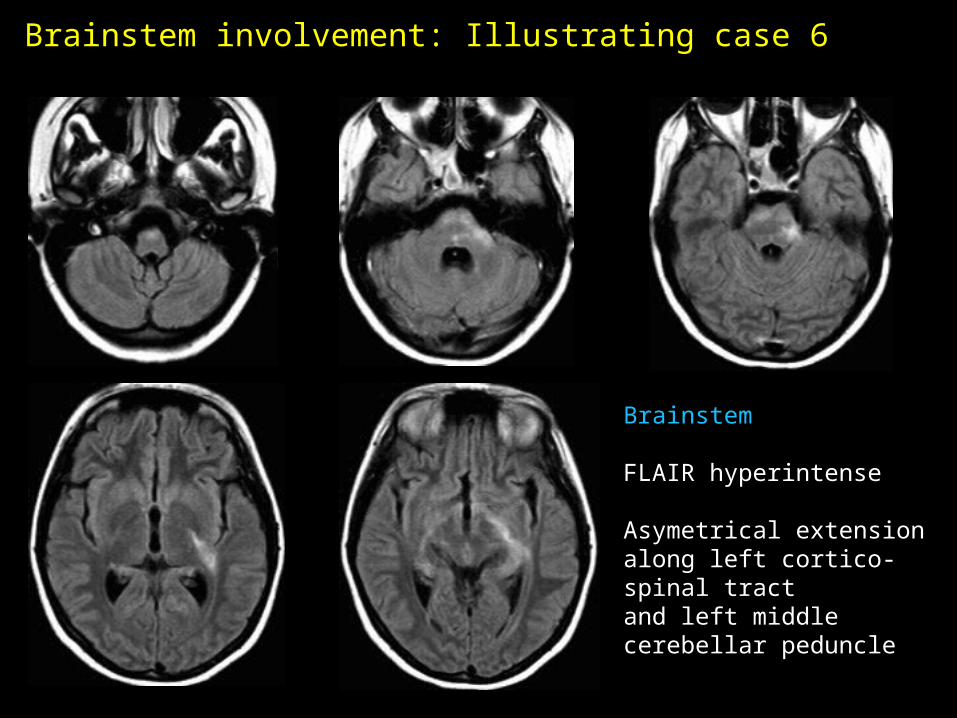
Brainstem involvement: Illustrating case 6

Diencephalic junction
FLAIR and T2 hyperintense
Asymetrical extension along the left cortico-spinal tract
Brainstem involvement: Illustrating case 7
Brainstem, thalami, periventricular
FLAIR hyperintense
T1 hypointensewithout enhancement
Faint haemorrhage on T2*
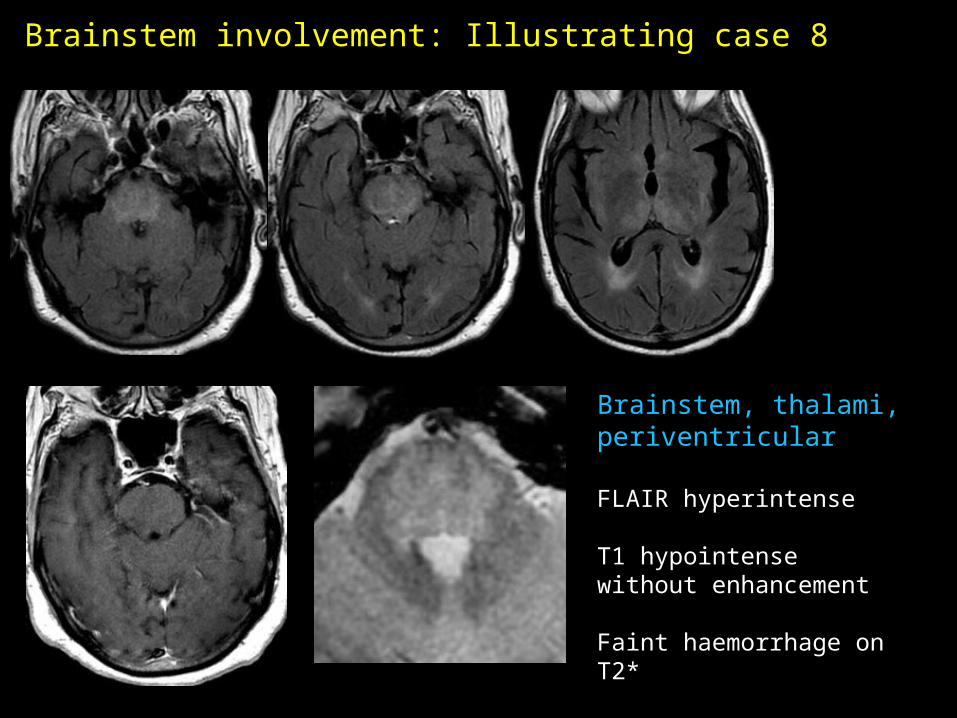
Brainstem involvement: Illustrating case 8

Brainstem andSupratentorial
FLAIR and T2 hyperintense
Extension alongCorticospinal tract
Haemorrhage
Brainstem involvement: Illustrating case 9
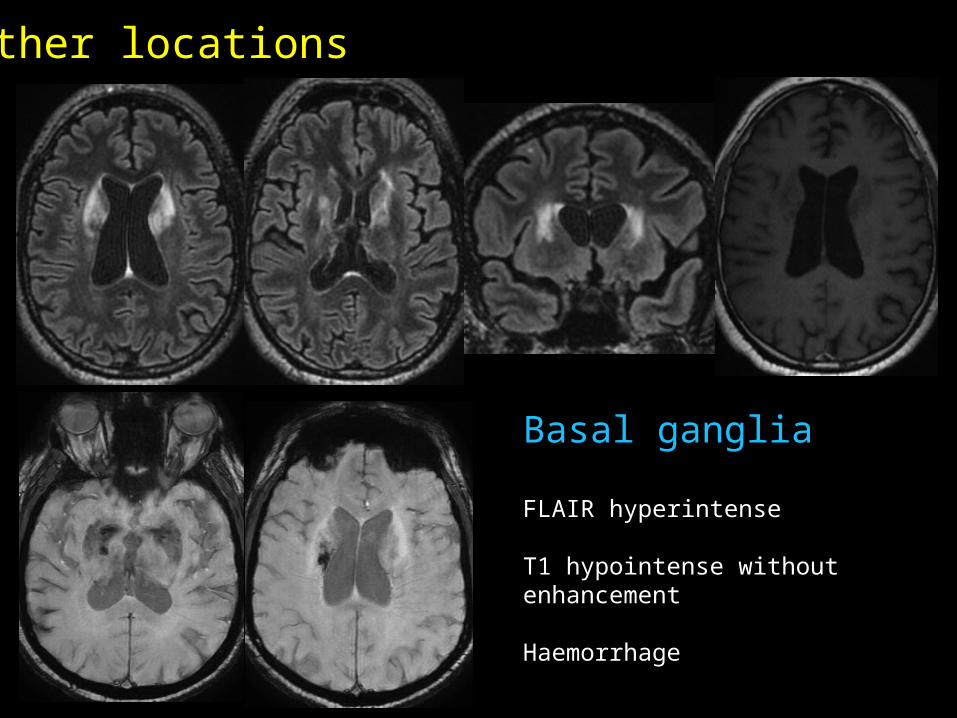
Basal ganglia
FLAIR hyperintense
T1 hypointense without enhancement
Haemorrhage
Other locations
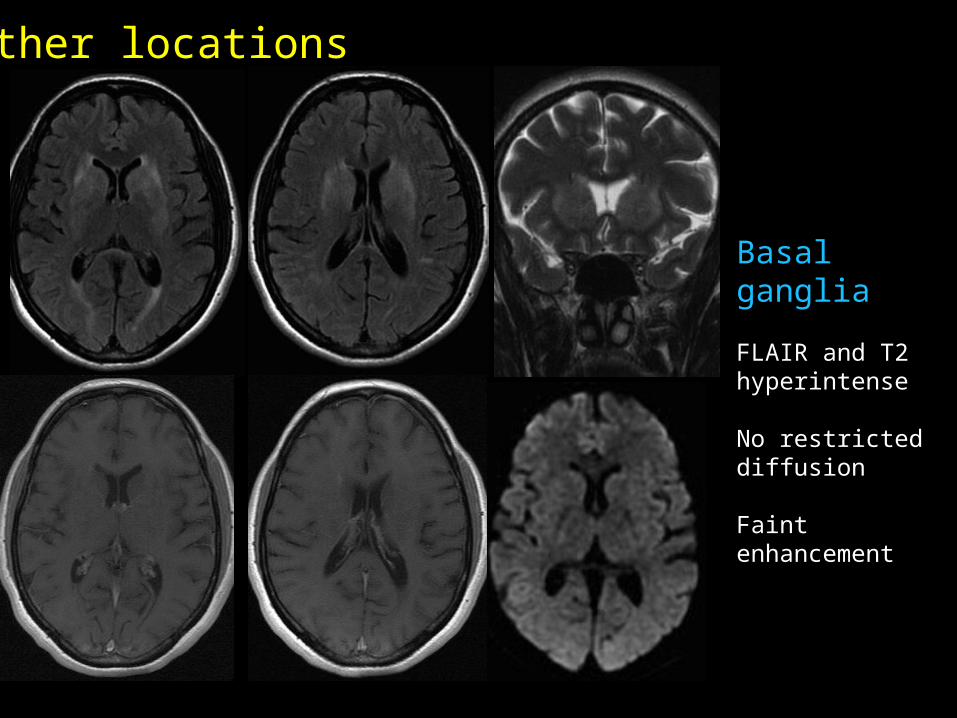
Basal ganglia
FLAIR and T2 hyperintense
No restricteddiffusion
Faint enhancement
Other locations
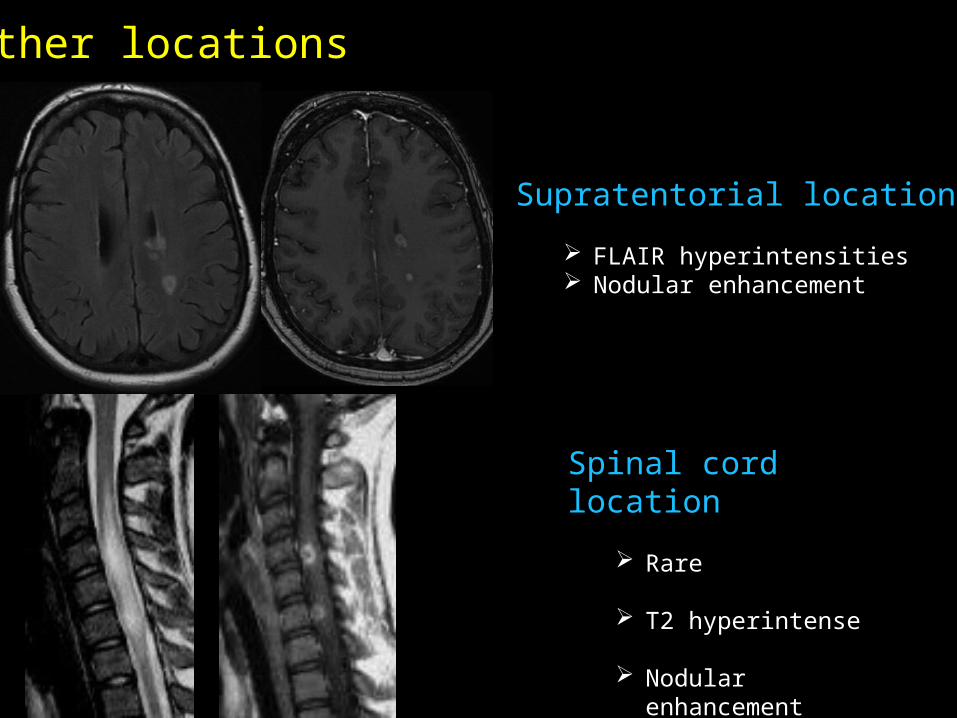
Supratentorial location
FLAIR hyperintensities Nodular enhancement
Spinal cord location
Rare
T2 hyperintense
Nodular enhancement
Other locations
Parenchymal involvementDifferential diagnoses
• Infectious diseases:Viral rhomboencephalitisListeria
• Inflammatory diseases:Multiple sclerosis Sarcoidosis

• Histopathologically, these parenchymal lesions represent inflammatory cellular infiltration (mainly neutrophils and activated T cells) around peripheral small venules and capillaries and indicate demyelination and edema
• Autopsy studies and biopsy specimens of the CNS lesions show a clear venous predominance
Parenchymal involvementPathophysiology

• Lesions observed in MRI may be caused by vasculitis small vein infarctions since:
Topography is not compatible with arterial territories
Significant vasogenic edema with central haemorrhage and tendency to disappear with disproportionally small residua is observed, as in venous infarction
Parenchymal involvementPathophysiology
• Venous anatomic arrangements might explain the predilection of NBD lesions:
In the brainstem, there is nearly no collateral pathway: thrombosis of small veins might lead to a large and possibly haemorrhagic lesion
On the contrary, the telencephalic structures are drained by superficial and deep venous system which interconnect via medullary veins: the possibility of a flow in both direction could explain smaller lesions caused by venous thrombosis
Parenchymal involvementPathophysiology
• Since venous theory is supported in NBD, SWI can be a useful diagnostic tool
• SWI uses tissue magnetic susceptibility differences to generate an unique contrast
• Is very sensitive to detect venous deoxygenated blood products inside and outside the blood vessels
Parenchymal involvementSWI
• In a study by S. Albayram, comparing the proportion of NBD lesion detection and the performance of haemorrhage detection with T2 FSE, T2* and SWI:
Most of the lesions were found to be haemorrhagic with SWI
SWI was most successful than T2 or T2* to detect haemorrhagic foci
In addition, prominent venous structures and occlusion of venous and collateral venous structures were revealed by SWI in the lesion vicinity
Evaluation of parenchymal neuro-behçet disease by using susceptibility-weighted imaging, S. Albayram, AJNR Am J Neuroradiol. 2011 Jun-Jul;32(6):1050-5
Parenchymal involvementSWI

• As the lesions become more chronic, excessive gliosis and atrophy appear, with possible thickening and fibrosis of the meninges
• The development and disappearance of lesions on MRI correlate with the course of clinical neurologic deficits
• NBD lesions may diminish in size in response to steroids alone or in combination with immunosuppressive drugs
• The more chronic cases can lead to atrophy, especially of the brainstem
Parenchymal involvementEvolution

initial 1 month 1 year
Regressionof swelling, FLAIR hyperintensitiesand enhancement
Regressionof swelling, FLAIR hyperintensitiesand enhancement
Sequelae
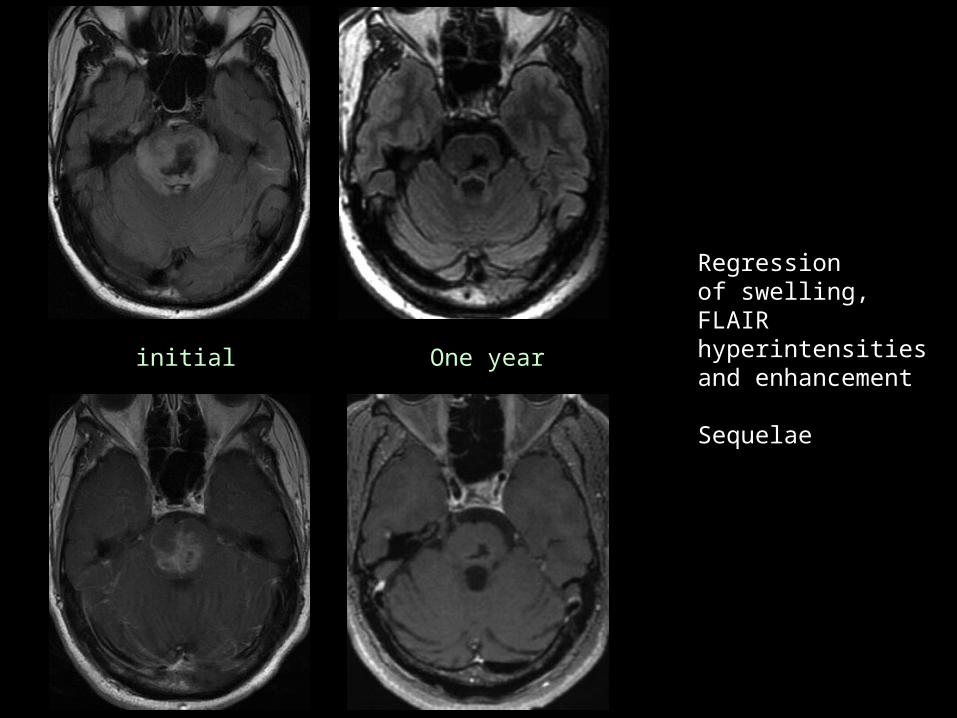
initial One year

Regression of the FLAIR hyperintensities
Brainstem atrophy
initial 3 months One year

Chronic NBD• Brainstem atrophy• Late cerebellar atrophy
Parenchymal involvementPseudotumoral presentation
• NBD can be seen as a space-occupying lesion and therefore mimick a brain tumor
• This pseudo-tumoral presentation makes diagnosis more difficult, especially when BD is unknown
• Differential diagnoses include lymphoma, other types of malignant tumors and abscess

• The pseudo-tumoral form of NBD is rare and life threatening condition
• MR shows pseudo-tumoral lesions, mainly in the capsulo-thalamic region
• Histological analysis reveals necrotic lesions with perivascular inflammatory without signs of tumoral or infectious lesion
• Immunosupressive therapy can improve neurological outcome
Parenchymal involvementPseudotumoral presentation

Heterogenous pseudomass lesion
DWI heterogeneous with restricted diffusion
Peripheral edema
T1 hypointense, T2 hyperintense
Capsulo-thalamic

Irregular enhancement
Spectroscopy unspecific, possiblymisleading: CholineNAALipids

initial 1 year
Evolution:Regression of the lesionSequelae

Initial:
Pseudo-tumoral capsulo thalamic
Peri lesionnal edema
Important mass effect
One year:
Importantregression
Other patient
Non parenchymal involvement
• The most frequent non parenchymal involvement is Cerebral Venous Thrombosis
• Frequency: 5%–25%• Clinical and radiological findings are similar
to those in patients with central venous thrombosis in other causes
• Most common occlusion sites: superior sagittal sinus, transverse sinus, deep cerebral veins and cavernous sinuses

Superior sagittal sinus thrombosis
Non parenchymal involvement
• Arterial Aneurysm, rareEight cases reported *
Sites of ordinary saccular aneurysms without radiologic features of vasculitis
• Arterial obstruction, rare (carotid and vertebral arteries)• Intracranial hypertension• Aseptic meningitis• Peripherical neuropathy (rare)
* Nakasu S, Kaneko M, Matsuda M. Cerebral aneurysms associated with Behçet's disease: a case report. J Neurol Neurosurg Psychiatry 2001; 70:682-684.

Take home messages
• Typical MR pattern in acute phase of NBD:
Brainstem +++
Ill defined areas of FLAIR and T2 hyperintensities
Swelling
Possible nodular and irregular enhancement
Frequent haemorrhage Extension along WM tracts

• Evolution of NBD:
Regression of T2 abnormalities
Can lead to atrophy (brainstem +++)
Take home messages

mainly capsulo-thalamic Immunosupressive therapy may lead to resolution of the lesions
The pseudo-tumoral form of NBD is rare
Take home messages
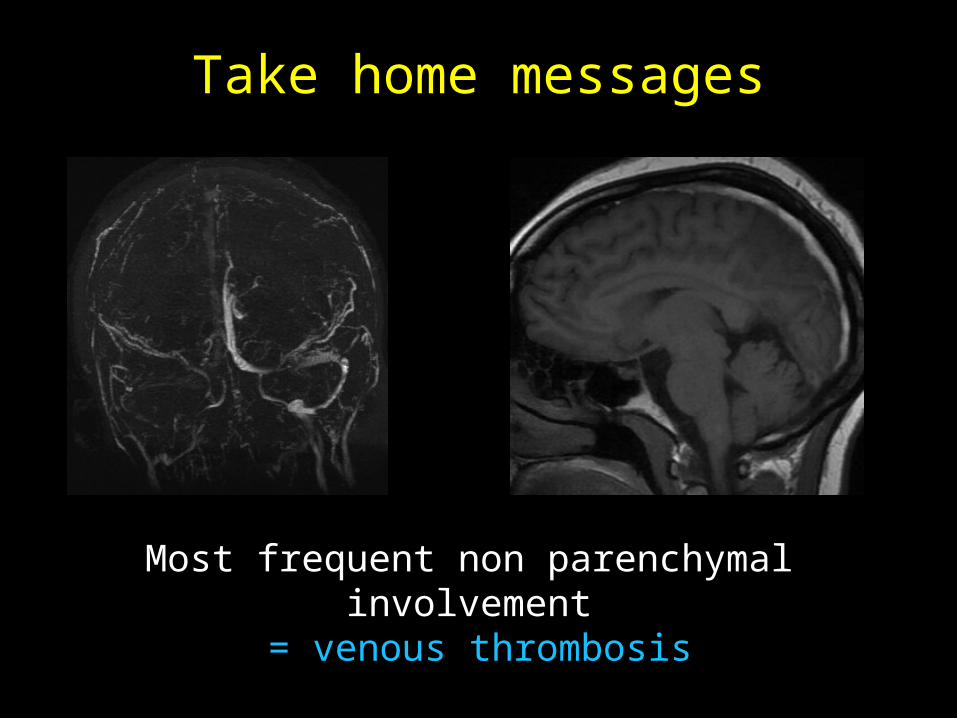
Most frequent non parenchymal involvement = venous thrombosis
Take home messages
Bibliography
• Radiologic and clinical findings of Behçet disease: comprehensive review of multisystemic involvement, EJ Chae and al, RadioGraphics 2008, 10.1148/rg.e31
• Neurologic Involvement in Behçet Disease: Imaging Findings in 16 Patients AJNR, M. Banna and al, AJNR Am J Neuroradiol. 1991 Jul-Aug;12(4):791-6
• CNS Involvement in Neuro-Behçet Syndrome: An MR Study, N. Koçer, AJNR Am J Neuroradiol. 1999 Jun-Jul;20(6):1015-24.
• Cranial MRI in Behc Met’s disease: 134 examinations of 98 patients, G. Akman-Demir and al, Neuroradiology. 2003 Dec;45(12):851-9.
• Clinical patterns of neurological involvement in Behçet's disease: evaluation of 200 patients, G Akman-Demir and al, The Neuro-Behçet Study Group. Brain 1999; 122 ( Pt 11):2171-2182.
• Neurological complications in Behçet's syndrome, D Kidd and al, Brain 1999; 122 ( Pt 11):2183-2194.
Bibliography
• Neurological aspects of Behçet’s disease: a case report and clinico-pathological review of the literature in Japan H Kawakita and al, J Neurol Sci 1967;5:417–438
• Neuro-Behçet’s disease: progressively enlarging temporal mass, Z Akar, J Ankara Med Sch 1992;14:295–300
• Pseudotumoral presentation of Neuro-Behçet’s disease: case series and review of literature, N. Noel and al, Rheumatology 2012; 51: 1216-25
• Neuro-Behçet Disease Mimicking Brain Tumor, K. Matsuo and al, AJNR Am J Neuroradiol 26:650–653, March 2005
• Evaluation of parenchymal neuro-behçet disease by using susceptibility-weighted imaging, S. Albayram, AJNR Am J Neuroradiol. 2011 Jun-Jul;32(6):1050-5.





























