Embed Size (px)
Citation preview

Edward O. LaumannUnivers i ty o f Ch icago
andBen jamin Cornwel lCorne l l Un ivers i ty
*Presentat ion a t the X i ’an Workshop on Soc ia l Networks and Hea l th
Ju ly 12-15 , 2013
Sexual problems of erectile function and orgasm in older men: Implications of
social network structure for masculinity*

Social Networks and Masculinity
• Traditional models of masculinity emphasize power, authority, control, and anything else that perpetuates men’s dominance over women (Cheng 1999; Connell 1987, 1995; Connell and Messerschmidt 2005).
• Social network structure is a key source of social resources that we know are highly gendered, including power, influence, and independence (e.g., Burt 1992; Emerson 1962; Freeman 1979).
• But men’s access to these resources may depend on the position of his female partner in his network…


Possible Mechanisms
• Partner betweenness may index social isolation, which could lower men’s self-esteem, sense of control and autonomy, and thus their sense of masculinity (Avison and Cairney 2003).
‒ These factors may affect the processing of stimulatory and inhibitory messages in the brain, the relaxation of penile muscles, and other processes that occur between the introduction of stimuli and the onset of erection, leading to “psychogenic” ED (Masters and Johnson 1966)
• Partner betweenness may also create feelings of resentment toward and lower satisfaction with the female partner, leading to strain and reduced mutual attraction (Foreman and Dallos 1992).

National Social Life, Health and Aging Project (NSHAP)
NSHAP is national probability survey of 3,005 community-dwelling adults aged 57-85, conducted in 2005-6, from the sampling frame of the Health and Retirement Survey (HRS), oversamples of African Americans and Hispanics.
Completion rate: 75%, two hour face-to-face interview plus 1/2 hour for collection of bio-measures.
Collected data on sexuality and intimacy, social networks, physical and mental health, medications, and bio-measures, including sensory function, functional capacity (e.g., Get up and Go), BMI, etc., and elder mistreatment.

Sexual Dysfunction Module
Sometimes people go through periods in which they are not interested in sex or are having trouble with sexual gratification. We have just a few questions about whether during the last 12 months there has ever been a period of several months or more when you …
1. were unable to climax (experience an orgasm), a form of dysfunction that is sometimes referred to as anorgasmia; or
2. had trouble getting or maintaining an erection.

Social Network Module
From time to time, most people discuss things that are important to them with others. For example, these may include good or bad things that happen to you, problems you are having, or important concerns you may have. Looking back over the last 12 months, who are the people with whom you most often discussed things that were important to you?
• Listed up to five confidants (Roster A)
• Spouse/partner is added (in Roster B) if not named
• Information is collected about ego’s frequency of contact with and closeness to each network member, as well as each network member’s frequency of contact with each of the others

Table 1. Descriptions of Key Variables Used in the Main Analyses (N = 678)a
Weighted Standard Variable Mean Deviation Dependent variables Erectile dysfunction R had trouble getting/maintaining an erection {1= Yes, 0 =No} .362 .483 Anorgasmiab R had trouble achieving orgasm {1= Yes, 0 =No} .207 .407 Compound dysfunctionb R experienced both of the above {1= Yes, 0 =No} .163 .363 Independent variables Partner betweenness R's spouse/partner has more contact with at least one of R's core confidants than R himself {1= Yes, 0 =No} .252 .449 Number of confidants Number of non-partner confidants in the network. Range 1 to 5. 2.738 1.214 Proportion kin Proportion of confidants who are kin. Range 0 - 1. .570 .387 Proportion female Proportion of confidants who are female. Range 0 - 1. .344 .325 Age group (Ref) R is between 57 and 64 years of age {1 =Yes, 0 =No} .546 .500
R is between 65 and 74 years of age {1 =Yes, 0 =No} .322 .484
R is between 75 and 85 years of age {1 =Yes, 0 =No} .131 .349 … … Spend time together R and partner usually spend free time together {1 =Yes, 0 =No} .536 .499 Partner satisfaction Average of 3 standardized items assessing relationship happiness, .220 .753 emotional satisfaction, and pleasure (α =.78). Range: -2.31 to 1.04. Partner demanding Partner often makes too many demands on R {1 =Yes, 0 =No} .093 .305
Prostate trouble R reports having an enlarged prostate {1 =Yes, 0 =No} .267 .442 Diabetes R has diabetes {1 =Yes, 0 =No} .195 .407 Self-rated health R reports being in "poor" or "fair" health {1 =Yes, 0 =No} .180 .369 R reports being in "good" health {1 =Yes, 0 =No} .260 .443 R reports being in "very good" health {1 =Yes, 0 =No} .395 .492 (Ref) R reports being in "excellent" health {1 =Yes, 0 =No} .165 .370
… …
Medications R takes at least one type of medication that is associated with erectile dysfunction {1 =Yes, 0 =No} .712 .440 a Means are estimated using NSHAP person-level weights, with post-stratification adjustments for non-response and adjustments for probability of inclusion in the main analysis. Estimates are calculated for all cases for which data are available on all key variables in the multivariate analysis. b Includes cases with valid data on this dependent variable and the independent variables (N = 670 and 667, respectively).

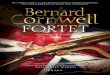
57 - 64 65 - 74 75 - 850
0.1
0.2
0.3
0.4
0.5
0.6
Age Group
Pre
vale
nce
of
ED

Table 2. Odds Ratios from Logistic Regression Models Predicting Erectile Dysfunction (N = 678) a
Predictor Model 1 Model 2b Model 3c Model 4b,c
Partner betweenness 1.759** 1.864** 1.711** 1.916** (.342) (.375) (.327) (.389)
……
Age (ref: 57-64): 65 - 74 2.282*** 2.393** 2.326** 2.284** (.456) (.558) (.543) (.565) 75 - 85 2.393** 2.290* 2.261* 2.229* (.737) (.769) (.694) (.755) … … Prostate trouble -- -- 2.189*** 2.134*** (.401) (.380)Diabetes -- -- 2.898** 2.873** (.970) (.909)Self-rated health (ref: excellent) Poor/Fair -- -- 4.184*** 4.002*** … (1.392) (1.321) … F 3.83** 4.25*** 4.29** 4.47***(d.f.) (9,43) (16,36) (24,28) (31,21)Fleiss, Williams, Dubro R2 .044 .087 .132 .159 * p < .05, ** p < .01, *** p < .001 (two-tailed tests)
a Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for network size, education, and whether R is out of the labor force.
b Includes control for amount of time spent with partner.
c Controls for obesity, cardiovascular problems, cancer, CES-D-ml, functional health, SPMSQ, use of medications, and rating of partner's health.

57 - 64 65 - 74 75 - 85-5.55111512312578E-17
0.05
0.1
0.15
0.2
0.25
0.3
0.35
No partner be-tweenness
Partner betweenness
Age Group
Pred
icte
d Pr
obab
ility
of
ED

Table 3. Odds Ratios from Logistic Regression Models Predicting Anorgasmia (N = 670)a
Predictor Model 1 Model 2b Model 3c Model 4b,c
Partner betweenness 1.515 1.678* 1.539 1.780* (.366) (.410) (.362) (.453)
……
Age (ref: 57-64): 65 - 74 2.203** 2.221** 2.070** 2.057* (.594) (.632) (.545) (.576) 75 - 85 3.736*** 3.168*** 3.460*** 3.060** (1.017) (.917) (1.034) (.996) … … Prostate trouble -- -- 1.910** 1.869** (.378) (.373)Diabetes -- -- 1.292 1.260 (.436) (.440)Self-rated health (ref: excellent) Poor/Fair -- -- 1.873 1.551 … (.945) (.849) … F 4.07*** 5.03*** 5.87*** 5.98***(d.f.) (9,42) (16,35) (24,27) (31,20)Fleiss, Williams, Dubro R2 .041 .077 .084 .109 * p < .05, ** p < .01, *** p < .001 (two-tailed tests)
a Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for network size, education, and whether R is out of the labor force.
b Includes control for amount of time spent with partner.
c Controls for obesity, cardiovascular problems, cancer, CES-D-ml, functional health, SPMSQ, use of medications, and rating of partner's health.

Table 3. Odds Ratios from Logistic Regression Models Predicting Compound Dysfunction (N = 667) a
Predictor Model 1 Model 2b Model 3c Model 4b,c
Partner betweenness 1.778* 1.954* 1.965* 2.316** (.506) (.544) (.564) (.705)
……
Age (ref: 57-64): 65 - 74 1.949* 1.996* 1.754* 1.764 (.554) (.578) (.466) (.504) 75 - 85 3.321*** 2.890** 2.939** 2.628** (1.004) (.956) (.874) (.921) … … Prostate trouble -- -- 2.665*** 2.658*** (.627) (.604)Diabetes -- -- 1.344 1.314 (.503) (.513)Self-rated health (ref: excellent) Poor/Fair -- -- 5.856** 5.426* … (3.817) (3.691) … F 4.49*** 5.54*** 3.12** 3.44**(d.f.) (9,42) (16,35) (24,27) (31,20)Fleiss, Williams, Dubro R2 .034 .068 .121 .147 * p < .05, ** p < .01, *** p < .001 (two-tailed tests)
a Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for network size, education, and whether R is out of the labor force.
b Includes control for amount of time spent with partner.
c Controls for obesity, cardiovascular problems, cancer, CES-D-ml, functional health, SPMSQ, use of medications, and rating of partner's health.


























![[Bernard Cornwell] Schwertgesang](https://img.dokumen.tips/doc/110x75/577cc0091a28aba7118ea00e/bernard-cornwell-schwertgesang.jpg)
