Embed Size (px)
Citation preview

Educational Content Developed by ASBMR and the Faculty Listed Below
Stuart L. Silverman, MD, FACP, FACR (Chair)Medical DirectorCedars-Sinai Bone Center of ExcellenceLos Angeles, California
Cheryl L. Lambing, MD, FAAFPClinical Professor University of California, Los AngelesLos Angeles, California
E. Michael Lewiecki, MD, FACP, FACEClinical Assistant Professor of MedicineUniversity of New Mexico School of MedicineAlbuquerque, New Mexico
Michael McClung, MD, FACP, FACEDirectorOregon Osteoporosis CenterPortland, Oregon Ethel S. Siris, MDMadeline C. Stabile Professor of Clinical MedicineColumbia UniversityNew York, New York Nelson B. Watts, MD, FACP, MACEDirectorMercy Health Osteoporosis and Bone Health ServicesCincinnati, Ohio

Osteoporosis Education for the PCP?
Osteoporosis is under-recognized
Fractures are not recognized as sentinel
events
PCPs are critical for screening, diagnosis, and
treatment
Osteoporosis is under-treated
ASBMR and The France Foundation
Curriculum for PCPsAAFP chapter meetings
www.osteocme.org

Learning Objectives• Improve the ability to assess risk factors for osteoporosis and
apply evidence-based screening recommendations to these at-risk patients within one’s practice
• Develop strategies to improve the treatment of patients with osteoporosis
• Utilize the tools and other information provided within this initiative, including patient education tools and systems-based approaches to facilitate improving the assessment and care being provided to patients with osteoporosis

• What is osteoporosis?• Why you should care?• Whom to test and how?• Whom to treat and how?
Postmenopausal Osteoporosis in the Primary Care Setting

2000 NIH Consensus Development Conference
Definition of Osteoporosis
Normal Bone
Osteoporotic Bone
• A skeletal disorder characterized by– Compromised bone strength predisposing to
– An increased risk of fracture
• Bone strength reflects the integration of two main features: – Bone density
– Bone quality
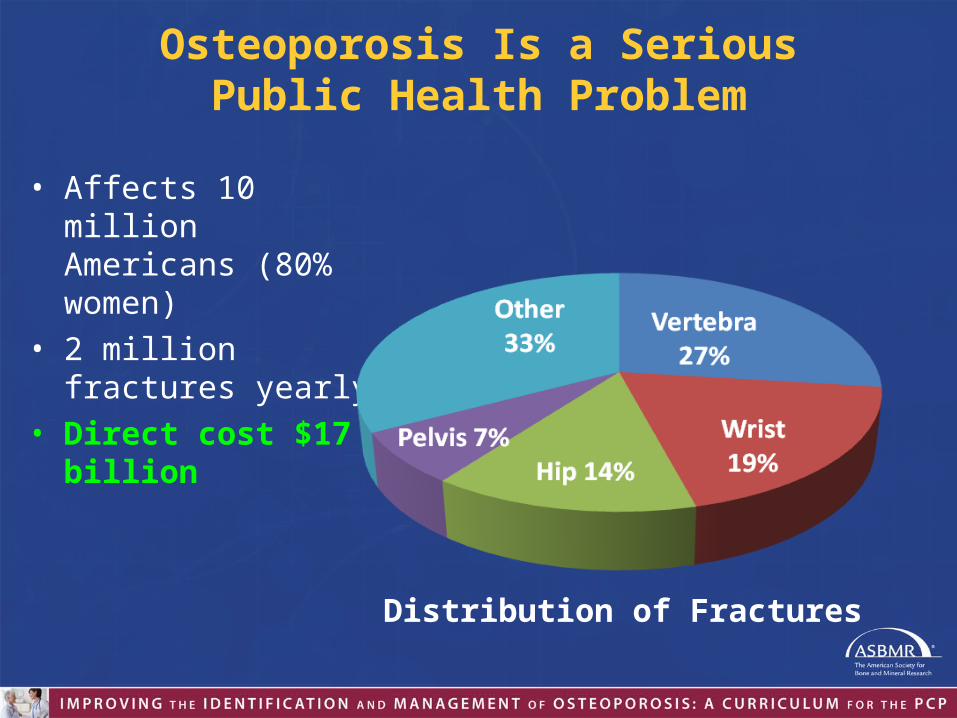
Osteoporosis Is a SeriousPublic Health Problem
• Affects 10 million Americans (80% women)
• 2 million fractures yearly• Direct cost $17 billion
Distribution of Fractures
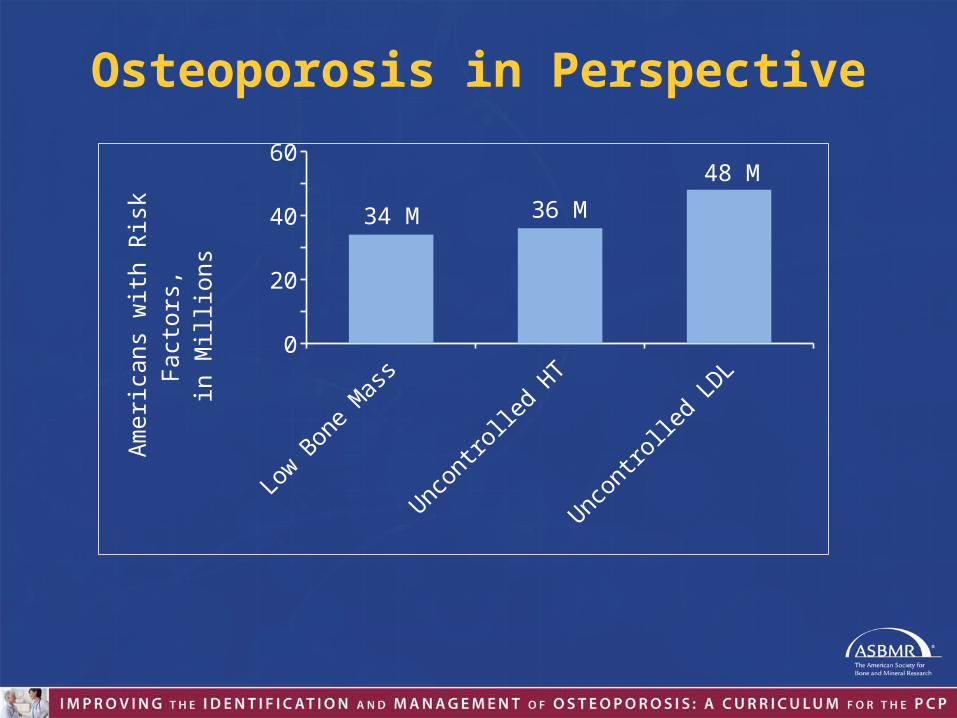
Osteoporosis in Perspective
Low Bone Mass Uncontrolled HT Uncontrolled LDL0
10
20
30
40
50
60
34 M 36 M
48 M
Amer
ican
s with
Ris
k Fa
ctor
s,in
Mill
ions

Osteoporosis in PerspectiveLifetime risk at age 50
Fracture Breast Cancer0%
10%
20%
30%
40%
50%
60%50%
12%
Women
Fracture Prostate Cancer0%
5%
10%
15%
20%
25%
30%
20%17%
Men
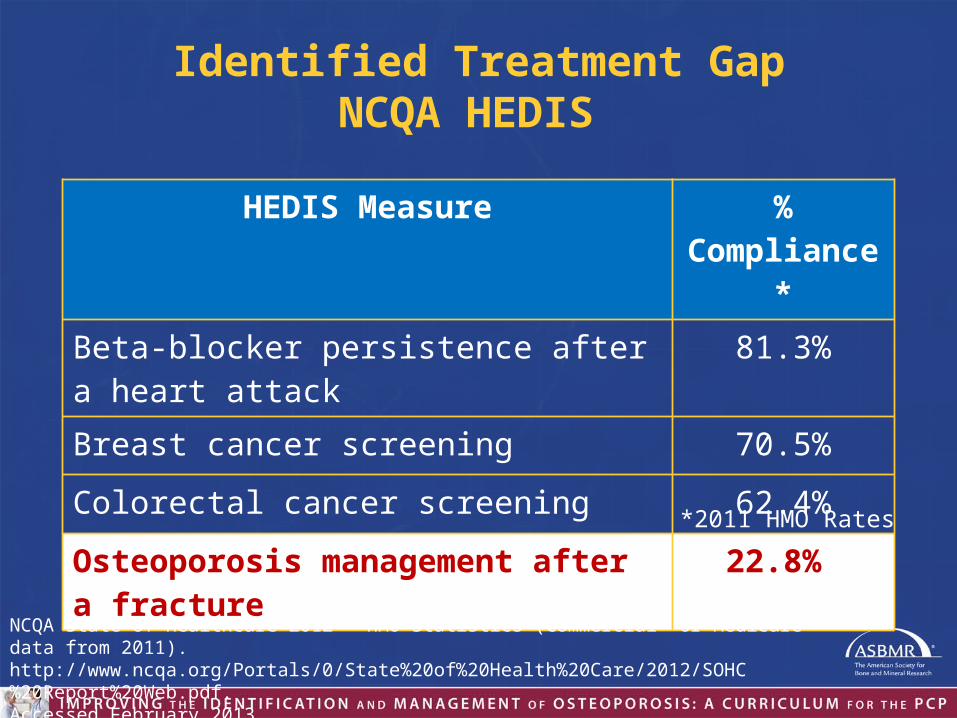
Identified Treatment GapNCQA HEDIS
HEDIS Measure % Compliance*
Beta-blocker persistence after a heart attack 81.3%
Breast cancer screening 70.5%
Colorectal cancer screening 62.4%
Osteoporosis management after a fracture 22.8%
NCQA State of Healthcare 2012 - HMO Statistics (Commercial or Medicare data from 2011). http://www.ncqa.org/Portals/0/State%20of%20Health%20Care/2012/SOHC%20Report%20Web.pdf. Accessed February 2013.
*2011 HMO Rates
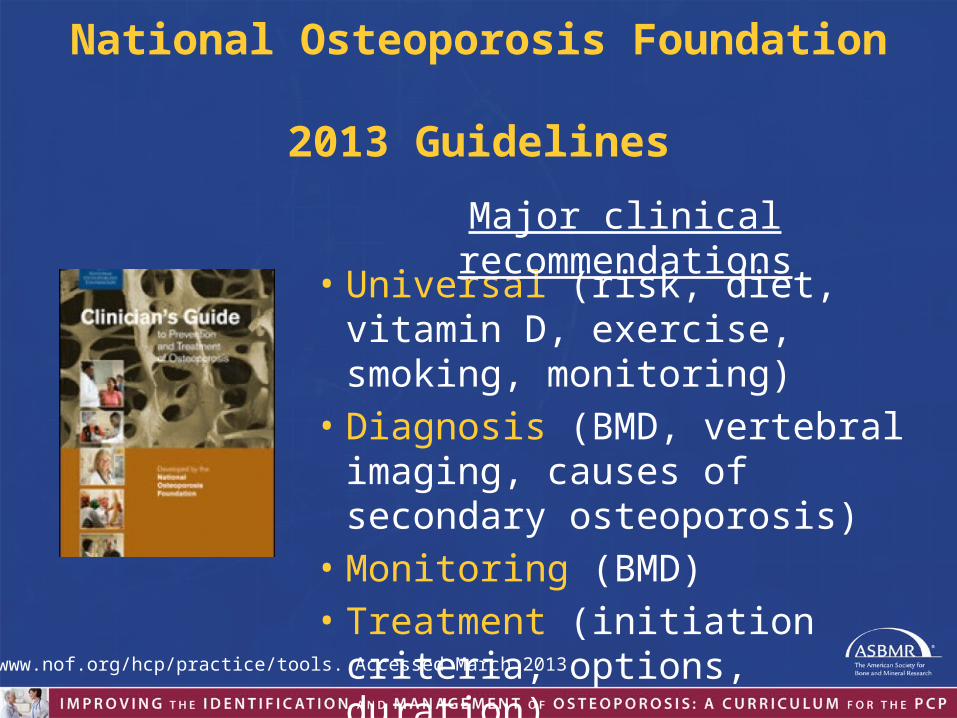
National Osteoporosis Foundation 2013 Guidelines
• Universal (risk, diet, vitamin D, exercise, smoking, monitoring)
• Diagnosis (BMD, vertebral imaging, causes of secondary osteoporosis)
• Monitoring (BMD)• Treatment (initiation criteria, options,
duration)
Major clinical recommendations
http://www.nof.org/hcp/practice/tools. Accessed March 2013.

Who Should Have a Bone Density Test?AAFP1 and NOF2
1. Sweet MG, et al. Am Fam Physician. 2009;79(3):193-200.2. National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. www.nof.org. Accessed February 2013.
Women age 65 and older and men age 70 and older
Younger postmenopausal women and men ages 50–69 with clinical risk factors
Adults who have a fracture after age 50
Adults with a condition (e.g., rheumatoid arthritis) or taking a medication (e.g., glucocorticoids) associated with low bone mass or bone loss

Reimbursement for DXAFinal Rule
1. Estrogen-deficient women at clinical risk for osteoporosis
2. Patients with vertebral abnormalities
3. Patients receiving long-term glucocorticoids (prednisone ≥ 5 mg/d or equivalent for 3+ months)
4. Patients with primary hyperparathyroidism
5. Patients being monitored to assess the response to an approved drug
Federal Register. 2006;71(231):67783-67784.
Since 2006, Medicare covers bone densitometry for five indications

WHO Criteria forPostmenopausal Osteoporosis
The T-score compares an individual’s BMD with themean value for young adults and expresses
the difference as a standard deviation score.
Category T-score
Normal -1.0 and above
Low bone mass (osteopenia) Between -1.0 to -2.5
Osteoporosis -2.5 and below

Whom to Treat: NOF Guidelines 2013Women ≥ 65 and men ≥ 70(younger with risk factors)
T-score between -1.0 and -2.5and increased fracture risk
T-score ≤ -2.5 in the lumbar spine, total hip, or femoral neck
or Hip or spine fracture (clinical or radiographic)
DXA test
≥ 3% for hip fracture or
≥ 20% for major osteoporotic fractures
FRAX10-y fracture risk
Candidate for TREATMENT
YES
YES
http://www.nof.org/hcp/practice/tools. Accessed March 2013.

Web Version 3.4


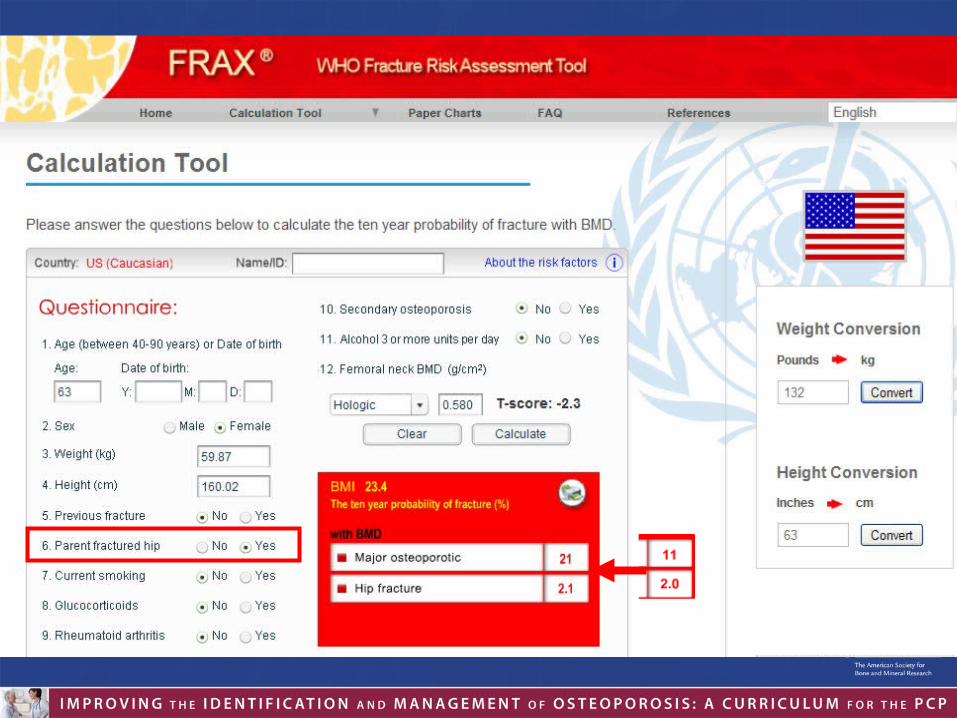
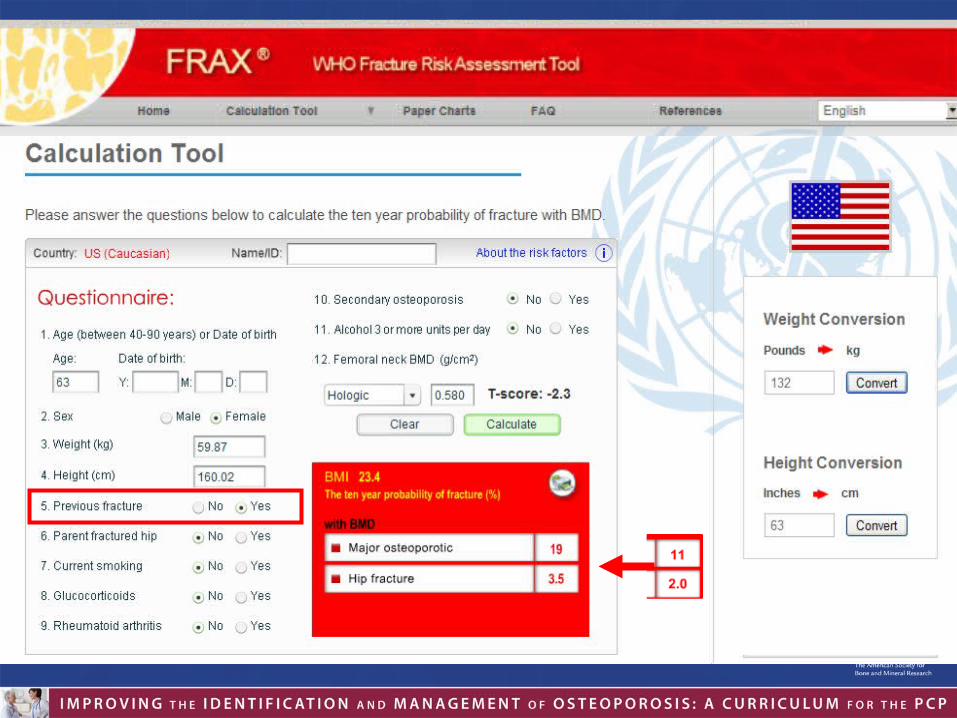


Clinical Benefits of FRAXDerives 10-year probability of clinical event
from measurable parameters
Internationally recognized and validated
Based on data from multiple cohorts
Easily accessible on the Internet or DXA software
Helps identify patients who need treatment

Limitations of FRAX
Watts NB, et al. J Bone Miner Res 2009;24:975-979.
Not valid to monitor patients on treatment
Only femoral neck BMD is considered
Risk is “yes/no” – there is no consideration of “dose” (e.g., fractures, glucocorticoids, smoking, alcohol)
Not all risk factors are included
Clinical judgment is required
Do patients with high FRAX scores benefit from medication? (Unknown)
Patient Care Goals
• Identify patients at risk of fractures• Reduce incidence of fractures• Maintain quality of life
– Activity– Independence– Health

Universal Recommendations for Bone Health• Counsel on the risk of fractures
• Eat a diet rich in fruits and vegetables (supplemented if necessary) to a total calcium intake of– 1000 mg per day for men 50-70
– 1200 mg per day for women ≥ 51
– 1200 mg per day for men ≥ 71
• Vitamin D intake should be 800-1000 IU per day, supplemented if necessary (age ≥50)
• Regular weight-bearing and muscle-strengthening exercise
• Fall prevention evaluation and training
http://www.nof.org/hcp/practice/tools. Accessed March 2013.


FDA-approved Medications Osteoporosis Post-
menopausalGlucocorticoid
-induced MaleDrug Prevent Treat Prevent Treat
Estrogen
Calcitonin* (Miacalcin®, Fortical®)
Raloxifene (Evista®)
Ibandronate (Boniva®)
Alendronate (Fosamax®)
Risedronate (Actonel®, Atelvia®)
Risedronate (Atelvia®)
Zoledronate (Reclast®)
Denosumab (Prolia™)
Teriparatide (Forteo®)

Drug Vertebral Fracture
Nonvertebral Fracture
Hip Fracture
Calcitonin
Raloxifene
Ibandronate
Alendronate Risedronate Zoledronic acid Denosumab
Teriparatide
Evidence for Fracture Reduction
Adapted from Murad MH, et al. J Clin Endocrinol Metab. 2012;97(6):1871-1880.

Clinical Benefit of Bisphosphonates• Relative risk reduction for fractures • Postmenopausal women with osteoporosis• 3 years bisphosphonate treatment
Vertebrae Hip
Khosla S, et al. J Clin Endocrinol Metab. 2012;97(7):2272-2282.
BisphosphonatesSide Effects/Safety Concerns
• Oral formulations may cause esophageal irritation • Can cause acute phase response (IV and high-dose oral)• Contraindicated in patients with hypocalcemia• Limited to patients with good kidney function (GFR > 30 or
35 mL/min)• Musculoskeletal pain?• Osteonecrosis of the jaw?• Atypical femur fractures?
• Bisphosphonates have a long residence time in bone– Does long-term treatment create safety concerns that limit
the duration of treatment?
– Given the long retention in bone, with release and possibly recycling of drug, does cumulative exposure lead to a reservoir in bone, so that after therapy is stopped, sufficient drug will be released to exert a continuing benefit?
How Long Should Bisphosphonate Treatment Last?
Porras AG, et al. Clin Pharmacokinet. 1999;36(5):315-328.Watts NB, et al. J Clin Endocrinol Metab. 2010;95(4):1555-1565.

Long-term Experience with AlendronateFit Long-term Extension (FLEX) Study
• 5-year extension to 5 year alendronate trial• Alendronate patients re-randomized
– Continue alendronate (n = 662) – Switch to placebo (n = 437)
• Results– Clinical vertebral fractures were reduced by 55% overall in
continuation group– Nonvertebral fractures were reduced by 50% in continuing
women with T-scores -2.5 or below at the start of FLEX
Schwartz AV, et al. J Bone Miner Res. 2010;25:976-982.
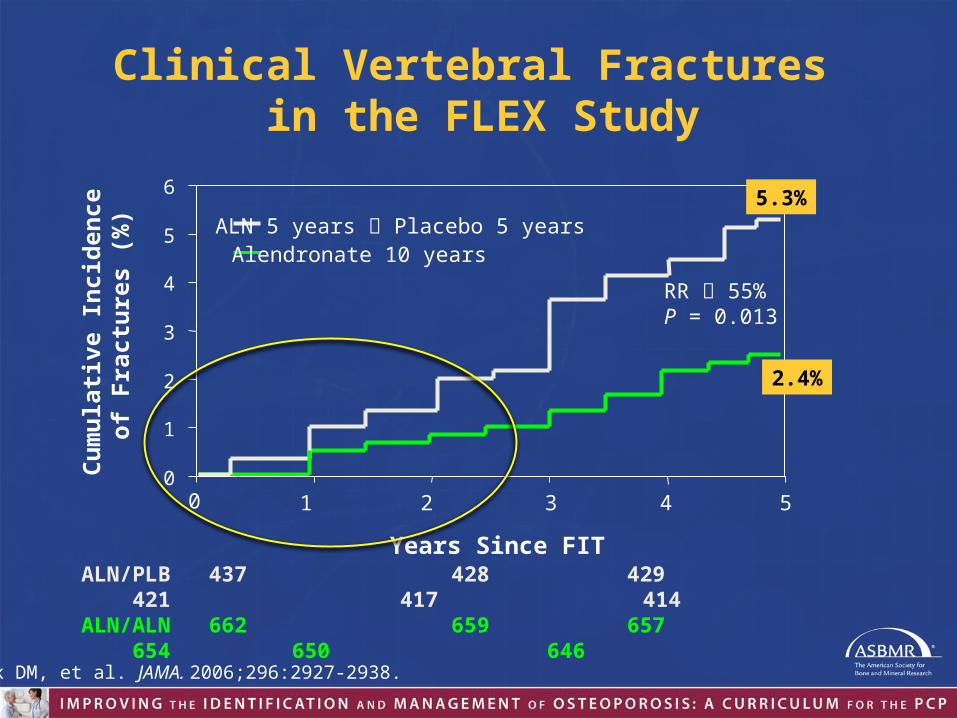
Clinical Vertebral Fractures in the FLEX Study
0 1 2 4 5
Cum
ulati
ve In
cide
nce
of F
ract
ures
(%)
Years Since FITALN/PLB 437 428 429 421 417
414 ALN/ALN 662 659 657 654 650
646
30
1
2
3
4
5
6
ALN 5 years Placebo 5 yearsAlendronate 10 years
5.3%
RR 55%P = 0.013
2.4%
Black DM, et al. JAMA. 2006;296:2927-2938.

How Long to Treat with Bisphosphonates?
• 5–10 years appears to be safe for most patients• Assess for risk:
Watts NB and Diab D. J Clin Endocrinol Metab. 2010;95(4):1555-1565.
Drug Holiday After 3-5 years
Drug Holiday After 10 years
Higher RiskLower Risk

Denosumab
• Human monoclonal antibody to RANKL
• Decreases osteoclast number and function
• Reduces risk of spine, hip and nonvertebral fractures
• For osteoporosis, SQ dosing every 6 months
• No dose adjustment for decreased kidney function
• Effect is reversible within 6–12 months of stopping
Cummings SR, et al; FREEDOM Trial. N Engl J Med. 2009;361(8):756-765.Jiang X, et al. Menopause. 2013;20(2):117-119.

Differences Among Antiresorptive Agents
Efficacy “broad spectrum” antifracture efficacy (alendronate, risedronate, zoledronate, denosumab)
Route of administration oral (fasting or with food) or parenteral
Frequency of administration
daily, weekly, monthly, quarterly, twice yearly, once yearly
Side effects/tolerability depends on agent and patient
Non-skeletal effects breast cancer reduction (raloxifene)
Cost/insurance coverage
generic oral; drugs “administered by health professional” covered by Medicare Part B

Teriparatide
• Recombinant human PTH (rhPTH [1-34])• Mechanism of action different from other agents (anabolic)• Daily SC injection • Indicated for patients at high risk for fracture
– Postmenopausal women with osteoporosis– Men with primary or hypogonadal osteoporosis– Men and women with osteoporosis associated with sustained
systemic glucocorticoid therapy• Treatment limited to 2 years, follow with antiresorptive
agentForteo PI. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/021318s012lbl.pdf. Accessed Feb 2013. Han SL, Wan SL. Int J Clin Pract. 2012;66:199-209.

• Monitor with DXA every 1–2 years – Do not "over-interpret" change– Be happy when BMD is stable OR increasing
• Why do some patients lose BMD on treatment?– Adherence– Drug pharmacokinetics– Underlying disorders that need to be addressed
• Patients on treatment whose BMD remains low are at high risk of fracture and may benefit from longer treatment
Monitoring

Secondary Fracture Prevention
• A fracture is a sentinel event
• A fracture in a person over 50 is the most powerful risk factor for a future fracture
• Many high risk patients have the fracture successfully treated but do NOT receive subsequent medical assessment and treatment to prevent the next fracture

Where Are We Now? The Good News
Improved awareness
Excellent diagnostic tools available
FRAX is a quantitative risk assessment
Safe and effective individualized treatment
Better understanding of pathogenesis
Federal initiatives to improve care

Where Are We Now? The Bad News
Ross S, et al. Value Health. 2011;14(4):571-581.Reynolds K, et al. Osteoporos Int. 2013 Apr 18. [Epub ahead of print].
Under-recognition of patients at risk for fracture
Decreasing access to DXA
Poor patient understanding of risk/benefitIncreasing patient concerns about side effects
Fewer patients on therapy
Poor adherence• 30% of patients don’t fill new bisphosphonate prescriptions • Risk of fracture increased 30–40%

What Can I Do as a PCP?
Practical Steps
Patient Dialog• Risk/benefit
communication• Shared decision makingDecision Aids
• Electronic med records• Checklist for risk• Handouts• Web resourcesEngage the Care Team
• Counseling, follow-up• ID high-risk patients
Manage Nonadherence• Identify individual barriers• Address barriers

Fall Prevention
• Improve lighting• Remove loose rugs• Add grab bars near bathtubs, toilets and stairways • Formal home safety evaluation • Physical therapy for core strength and balance• Eliminate medications that can affect alertness and
balance• Assistive device evaluation and training
Sweet MG, et al. Am Fam Physician. 2009;79(3):193-200.
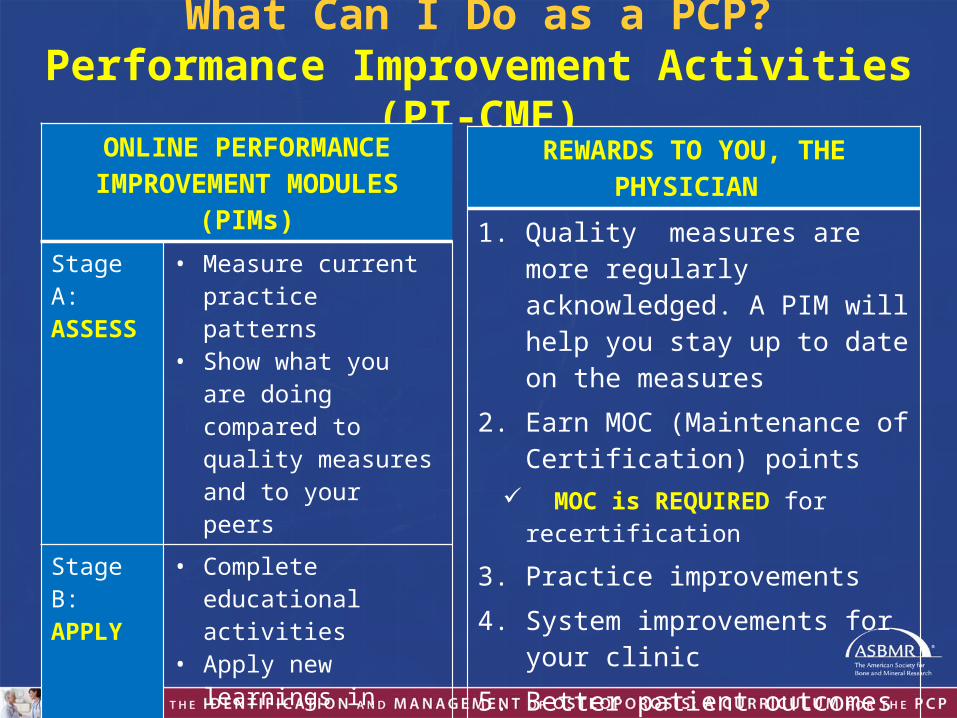
What Can I Do as a PCP?Performance Improvement Activities (PI-CME)
ONLINE PERFORMANCE IMPROVEMENT MODULES (PIMs)
Stage A: ASSESS
• Measure current practice patterns
• Show what you are doing compared to quality measures and to your peers
Stage B: APPLY
• Complete educational activities
• Apply new learnings in practice
Stage C: EVALUATE
• Complete follow-up practice pattern assessments
• See how your practice has changed
REWARDS TO YOU, THE PHYSICIAN
1. Quality measures are more regularly acknowledged. A PIM will help you stay up to date on the measures
2. Earn MOC (Maintenance of Certification) points
MOC is REQUIRED for recertification3. Practice improvements4. System improvements for your
clinic 5. Better patient outcomes

Performance Improvement CME MOC Part IV Approved
American Board of Family Medicine (ABFM)
https://achsos.community360.net/default.aspx. Accessed April 2013.
https://achsos.community360.net

Performance Improvement CME MOC Part IV Approved
American Board of Internal Medicine (ABIM)
www.pi-iq.com/osteoporosis2

Update on Management of Osteoporosis
What is osteoporosis?
Decreased bone strength predisposing to an increased risk of fracture
Why should you care?
Common, significant cost, morbidity and mortality
Whom to test and how?
DXA for all women by age 65, higher risk women earlier; FRAX is a useful tool
Whom to treat and how?
Individuals at high risk of fracture; approved agents are safe and effective; treatment decisions must be individualized

Online Tools and Resources
• www.osteoCME.org• FRAX• AAFP guidelines• NOF Clinician’s Guide 2013• ACP treatment guidelines 2008• NBHA resource center for Fracture Liaison Services

www.osteoCME.org