Embed Size (px)
Citation preview
Educate the Young…Emerging Trends in Quality and Safety
David Mayer, MDCorporate Vice-President Quality and Safety
MedStar Health
Disclosure Statement:I do not have, and have not had, in the last 12 months, any relevant financial
or other relationship with any proprietary entity producing health care goods or services including the manufacturer of any commercial product or device I will
discuss during my presentation.

MedStar Health• Mid-Atlantic Region
• Large Healthcare System
• Ten hospitals
• 150 Outpatient sites of care
• Center for Human Factors Engineering in Healthcare
• MedStar Research Institute
• Nationally Recognized simulation Center (SiTEL)
• MedStar Institute for Innovation (MI2)
• Medicaid MCO
• 26,000 Associates
• 6,700 Physicians
• 162,000 Inpatient Admissions
• 762,000 Inpatient Days
• 1,492,000 Outpatient Visits
• 215,000 Home Health Visits 2
Leading Change in Quality and Safety
“Medicine used to be simple, ineffective and relatively safe. Now it is complex, effective, and potentially dangerous.”
Sir Cyril Chantler,
Dean of London’s Guy’s Hospital
3

Healthcare’s Triple AimPursuing the Triple Aim: Seven Innovators Show the Way to Better Care, Better
Health and Lower Costs. Maureen Bisognano and Charles Kenney. 2012
• Strong Leadership Commitment
• Transparency
• Patient Engagement
• Interprofessional Teamwork
• Reporting Everything
• Measuring Everything
• Organizational Respect and Support
4

Leading Change in Quality and Safety
• Transparency
• High Reliability
• Patient-Partnership
• Respect and caring for fellow workers
• Education
5

Leading Change in Patient Safety
• Transparency (Honesty)– Transparency in Communications
• Disclosure after harm
• Reporting events, near misses and unsafe conditions
• Informed Consent/Shared Decision-Making
– Transparency in Outcomes
6
7

Definition of Professionalism
AAMC & NBME:
• Altruism
• Honor and Integrity
• Caring and Compassion
• Respect
• Responsibility
• Accountability
• Excellence and Scholarship
• Leadership
8

Definition of Professionalism
AAMC & NBME:
• Altruism
• Honor and Integrity
• Caring and Compassion
• Respect
• Responsibility
• Accountability
• Excellence and Scholarship
• Leadership
9

What about a “Principled Approach”
• Benefits• Barriers
10
What about a “Principled Approach”
• Benefits
– Maintain trust
– Learn from mistakes
– Improve patient safety
– Employee morale
– Psychological well-being
– Accountability
– Money
• Barriers
– Money
– Reputation
– “Shame and blame”
– Loss of control
– Loss of license
– Resource intense
– Uncertainty
11

Condition Predicate to a “Principled Approach”
12
Condition Predicate to a “Principled Approach”
• Courage…… and Leadership
13

14
“Principled Approach”
• What patients want to hear:
– Recognition: investigation
– The truth
– Regret: apology if appropriate
– Responsibility: prevention of further harm to others
– Remedy (“benevolent gestures”)
15
16
National Recognition of the “Seven Pillars” Program
17

Linking honesty with quality and safety
Investigation, Full Disclosure, Apology, Remedy, Prevention
and Accountability
Event
Becomes the Trojan Horse for Cultural Transformation
18

Transparency
“There is a ‘Magic’ that occurs when we are transparent and share our outcomes”
Paul Levy
19

20
Leading Change in Quality and Safety
High-reliability organizations (HROs):
“Subset of hazardous organizations that have operated nearly error-free for very long periods of time”.
Karlene Roberts (1990)
21
Leading Change in Quality and Safety
High-reliability organizations, or HROs, share two essential characteristics:
1. They constantly confront the unexpected
2. They operate with remarkable consistency and effectiveness
22
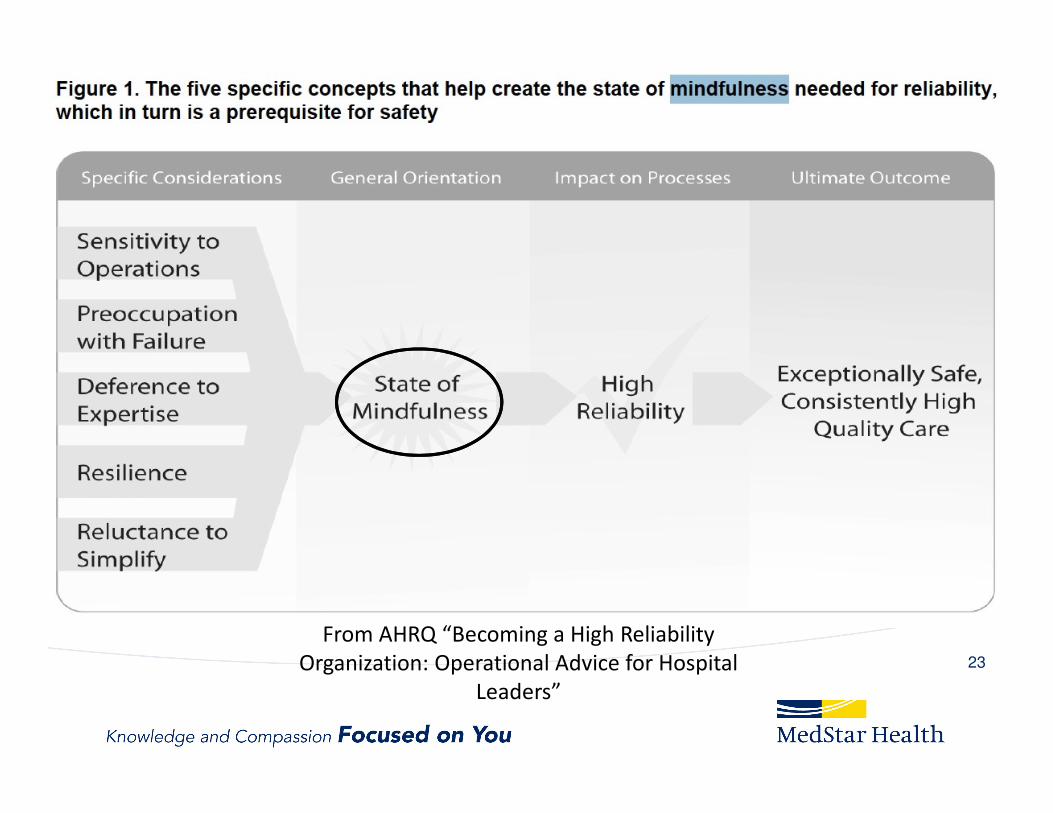
From AHRQ “Becoming a High Reliability
Organization: Operational Advice for Hospital
Leaders”
23
Collective Mindfulness
Goals of mindful practice:
• To become more aware of one’s own mental
processes, listen more attentively, become
flexible, and recognize bias and judgments, and
thereby act with principles and compassion.
24

Leading Change in Quality and Safety
How can we engage and partner with patients and families in our quality
and safety mission?
25

Leading Change in Quality and Safety
• Patient-Centered, Patient-Engaged, Patient-Driven– Dana Farber
– Virginia Mason
– Cincinnati Children’s Hospital
26
Paul O’Neill on Quality and Safety
Every worker’s experience, every day:
• I am treated with respect by everyone else,
regardless of position, education or pay.
• I have the education, training, tools, and the
support to develop to my full potential.
• My work is noticed and appreciated.
27
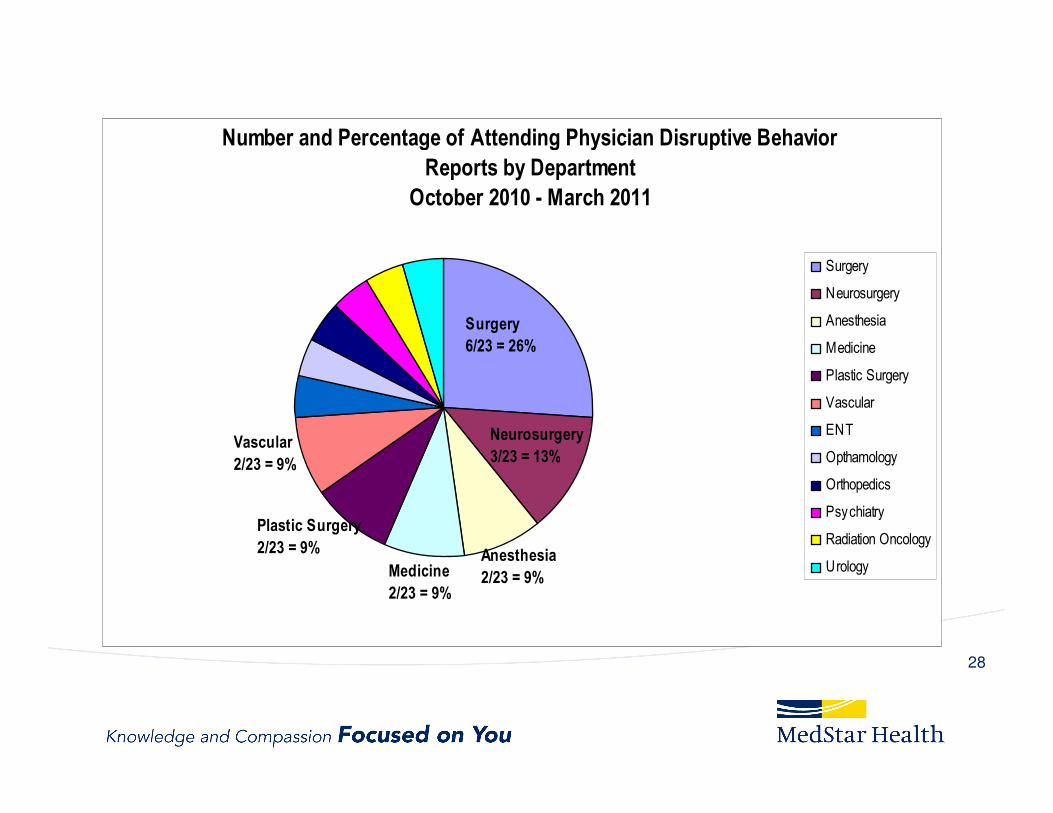
Number and Percentage of Attending Physician Disruptive Behavior
Reports by Department
October 2010 - March 2011
Surgery
Neurosurgery
Anesthesia
Medicine
Plastic Surgery
Vascular
ENT
Opthamology
Orthopedics
Psychiatry
Radiation Oncology
Urology
Neurosurgery
3/23 = 13%
Anesthesia
2/23 = 9%
Surgery
6/23 = 26%
Medicine
2/23 = 9%
Plastic Surgery
2/23 = 9%
Vascular
2/23 = 9%
28
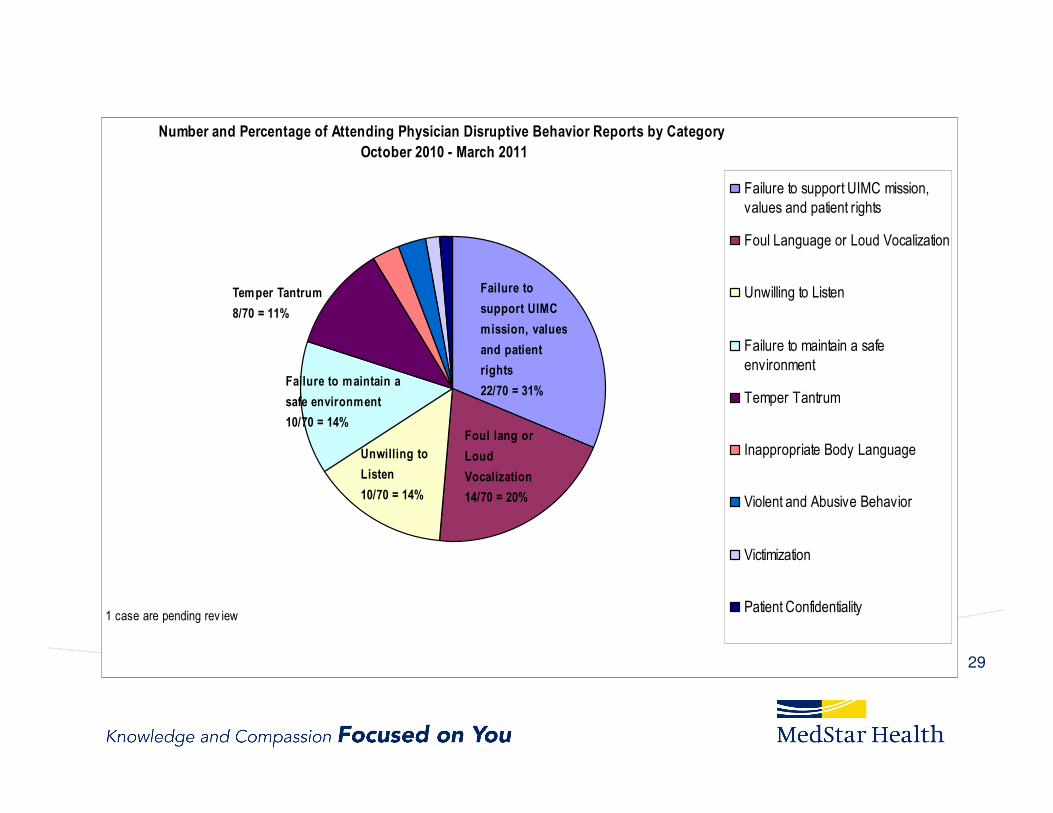
Number and Percentage of Attending Physician Disruptive Behavior Reports by Category
October 2010 - March 2011
Failure to support UIMC mission,
values and patient rights
Foul Language or Loud Vocalization
Unwilling to Listen
Failure to maintain a safe
environment
Temper Tantrum
Inappropriate Body Language
Violent and Abusive Behavior
Victimization
Patient Confidentiality1 case are pending rev iew
Failure to
support UIMC
mission, values
and patient
rights
22/70 = 31%
Foul lang or
Loud
Vocalization
14/70 = 20%
Unwilling to
Listen
10/70 = 14%
Failure to maintain a
safe environment
10/70 = 14%
Temper Tantrum
8/70 = 11%
29

30

Second Victim Recovery TrajectoryThanks to Susan Scott, RN, MSN University of Missouri, Columbia
Chaos &
Accident
Response
Intrusive
Reflections
Restoring
Personal
Integrity
Enduring
the
Inquisition
Obtaining
Emotional
First Aid
Moving On
Surviving
Impact Realization
31

Why introduce quality and safety into the health science curriculum?
• Experience gained in other safety critical industries has shown that if healthcare is to truly change its culture to one of safety and optimal quality care outcomes, education and experiential application “should be introduced
early in healthcare training –
32
Why introduce quality and safety into the health science curriculum?
– specifically at the student level as this is the period of acculturation into the profession. Health science schools must invest in curriculum development to address these safety issues at the earliest stages of training”.
Musson DM, Helmreich RL.
RL.
33
New ACGME CLER Program Requirements
CLER provides frequent on-site sampling of the
learning environment that will permit the
opportunity for sponsoring institutions to
demonstrate leadership in patient safety, quality
improvement, and reduction in health care
disparities.
34

New ACGME CLER Program Requirements
Through a series of unannounced site visits using
Tracer Methodologies, CLER reviewers will follow
residents through their daily patient care and
learning activities gathering information on how the
institution and residency program educate their
residents to the six core areas.
35

New ACGME CLER Program Requirements
CLER assesses sponsoring institutions in the following six focus areas:
• Patient Safety – including opportunities for residents to report errors, unsafe conditions, and near misses, and to participate in inter-professional teams to promote and enhance safe care.
• Quality Improvement – including how sponsoring institutions engage residents in the use of data to improve systems of care, reduce health care disparities and improve patient outcomes.
36

Telluride Patient Safety Roundtable
Ninth Annual Roundtable:
“The Power of Change Agents:
Teaching Caregivers Effective
Communication Skills to
Overcome the Multiple Barriers
to Patient Safety and
Transparency”
June 9th – June 18th, 2013
Telluride, CO
Supported by TDCF and MedStar Health 37

Telluride Roundtable and Summer Camps
38

Summer Camp Plans for 2013
• Resident Summer Camp week June 9th
– Telluride CO - 20 Resident Physicians
• Student Summer Camp week June 16th
– Telluride CO - 20 medical students and 10 Nursing Students
• Student Summer Camp week August 1st
– Washington DC - 20 medical students and 10 Nursing Students
Email: [email protected]

Creating a Culture of Quality and Safety
Educate the Young Blog:
http://educatetheyoung.wordpress.com/
Telluride Roundtable and Summer Camps
http://www.youtube.com/watch?v=Ikp4v10nvms
40





























