Embed Size (px)
Citation preview

Thorax 1984;39:641-646
Editorial
Giving up smokingSince the recognition of the health hazards associ-ated with tobacco smoking' techniques designed toaid smokers to quit have proliferated. The con-cerned physician or layman is faced with a bewilder-ing array of methods to apply to the individualsmoker to aid abstention from tobacco and with anumber of conflicting strategies to apply to societyas a whole to limit tobacco smoking.At the centre of this controversial subject is our
basic lack of knowledge about why an individual firsttakes up the habit of smoking and why he or shecontinues despite recognising the hazard. Further-more, over the last decade millions of people havevoluntarily given up smoking2 without any directassistance from the health agencies. Again we havelittle information on the makeup of the successfulex-smoker and what contributes to this modificationin behaviour.
Despite the lack of basic understanding there is anextensive array of publications on smoking with-drawal. The individual physician finds it hard todraw useful guidance from the diverse informationavailable. In this editorial a selection of the morepopular approaches to aid quitting-smoking will bereviewed and particular attention will be given tothose making use of substitutes for tobacco smoking.
Before we consider these approaches it may behelpful to describe what is at present understoodabout the psychological makeup of smokers and,perhaps more importantly, of successful ex-smokers.In addition, it is important to understand some ofthe external factors which influence the prevalenceof cigarette smoking.
Profile of a smoker
Smokers are considered to differ from non-smokersin their psychological makeup, tending towardsextraversion3 that is, tending to be people whocrave excitement, who are willing to take risks, andwho are more sociable and easy going. This is par-ticularly true for men. Neuroticism or anxiety maybe also important in their make up,4 althoughtobacco dependence may itself lead to greaterneuroticism.5 A further interesting psychQlogical
Address for reprint requests: Dr Tim Higenbottam, Adden-brooke's Hospital, Hills Road, Cambridge.
classification that has been applied to smokers andnon-smokers is the concept of internal and externalloci of control. Smokers tend to be more externallycontrolled,6 believing that fate, luck, or things gen-erally outside themselves control their lives. Finally,smokers consume more caffeine, alcohol, and otherpsychotropic drugs than do non-smokers.7Adult smokers are likely to have many smoking
friends.8 Probably the most important familyinfluence on maintenance of smoking is the smokinghabit of the spouse or cohabitant.9 The increasingmilitancy of non-smokers and increasing restrictionof public opportunities to smoke'0 may act to tightenthe ranks of smokers, making support from smokingfriends all the more important.
Professional and technical workers have the low-est cigarette smoking rates, while unskilled workershave the highest." This relationship is strong inmen, though women show the opposite trend.Furthermore, the most upwardly mobile individualsin social terms, with respect to their parents, are theleast likely to smoke.'2One of the most striking findings to emerge from
surveys over the last 20 years has been the increasein smoking among teenage girls, with no correspond-ing increase in the prevalence in teenage boys.'2 Thechanging sex role of women as manifested bychanges in higher education and the nature of theirwork may be important.
Profile of a successful ex-smoker
Discrimination on psychological grounds between asuccessful ex-smoker and a continuing smoker is lesseasy than that between non-smoker and smoker.For example, ex-smokers tend to be more extrovertbut less neurotic than smokers.'3 Those with "typeA" personalities, who are hard driving, ambitious,and competitive, are less likely to quit than "type B"people, with the opposite characteristics.'4 Heavyuse of other drugs, such as caffeine or alcohol, les-sens the chances of successful abstinence from smok-ing.4The most important considerations in determining
the success of abstinence, however, are the smokers'own use of cigarettes and that of his or her friends.There is mounting evidence that heavier cigarette
641
copyright. on January 17, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.39.9.641 on 1 S
eptember 1984. D
ownloaded from

642
smokers are markedly less able to quit than lightersmokers, who perhaps have less dependence ontobacco.'5 A further important powerful influenceon ability to quit is whether the smoker's spouse orcohabitant continues to smoke.9 Successful abstain-ers are also more likely to have friends who areformer smokers.'6Men are much more likely to succeed in abstain-
ing than women.'6 With the growing convergence ofmale and female roles in society, however, this effectmay be lessening.
Some general influences on smoking in society
In addition to those factors influencing an individu-al's attitudes and behaviour, powerful forces are atwork within society. The dramatic changes noted inadult smoking, especially among middle aged menand professional groups, may in part be attributableto the information and education campaigns whichhave taken place since 1964.'7 While specific eventslike the publication of the 1964 Surgeon General'sreport and the Royal College of Physicians' reportmay have had only small and transitory effects onsmoking cessation, the cumulative effects of persis-tent publicity probably has had more influence. Banson television advertising for cigarettes in severalcountries, including the United Kingdom, Denmark,Ireland and New Zealand, have had only a smalleffect upon per capita cigarette consumption.'8 Inthe United Kingdom the ban on television advertis-ing produced a statistically insignificant fall of 3%.1'The loss of advertising on the television was com-pensated for by the channelling of advertising intodisplays and promotion, making it difficult to evalu-ate the television ban per se. Cigarette smokingremains prevalent, however, in Communist coun-tries, where there is no advertising.The price of cigarettes may well be important in
determining consumption.'9 This may be particu-larly so at the present time of slow rates of growth ofreal income in the face of an increasing range ofconsumer products.
Factors other than price, level of advertising, andantismoking policy must be at work in determiningthe considerable differences in sales of tobaccogoods between countries and the variation of marketsize in any one country with time. This is clearlyshown by a recent comparison of per capita sales oftobacco in countries in the Organisation forEconomic Cooperation and Development that havesimilar gross national product to the United King-dom.20 Interestingly, the countries with the mostwell developed antismoking policies-for example,Norway and Finland-are those in which thetobacco market was least well developed.
Withdrawal techniques and strategies
It is against this background of multiple factorsinfluencing both an individual's smoking habit andsociety's attitudes to smoking that a physician is leftwith the task of evaluating the many alternativeapproaches to aid cessation in his smoking patient.
There have been considerable improvements inthe quality of data on smoking cessation methods inrecent years. In particular, controls and randomassignment of treatment have been introduced intostudies. Long term follow up for at least six monthsand often for over a year have been included.Perhaps the most important advance has been theintroduction of biochemical tests to verify selfreported abstinence from smoking. While thesetests-measurement of alveolar carbon monoxide,2'blood carboxyhaemoglobin,22 nicotine, cotinine,23and thiocyanate24-remain imperfect they permitthe identification of up to 20% of self reportingcigarette abstainers who are actually continuing tosmoke.25
Despite these definite improvements, broadgeneralisations about efficacy of measures againstsmoking are still made without proper reference tofactors such as age, sex, social class, or previoussmoking habit. Little effort is made to control forclinical zeal. Many studies remain methodologicallydeficient in some respects. The clinician needs to becautious when attempting to assess the relativemerits of new methods.
Specific intervention: nicotine substitution
Recently attention has focused on the so calledpharmacological and psychological aspects oftobacco smoking in which nicotine dependence orhabituation plays an important role.
Tobacco smoke inhalation appears to satisfy bothphysiological and psychological needs in the smoker.Among the myriad of compounds in smoke, nicotineis the most powerful pharmacological agent,26 actingon both sympathetic and parasympathetic ganglia.Two psychopharmacological models contribute toour understanding of the role of nicotine. The first isthe suggestion that nicotine is a drug of addiction,and the second is that nicotine is used as apsychological tool.
Several aspects of the smoker's behaviour suggestthat nicotine dependence is a primary reinforcer ofthe smoking habit. Some smokers appear to titratetheir requirement for nicotine27 and many smokersexperience symptoms of withdrawal.28 Nicotine doesnot, however, appear to have the characteristics ofabuse liability of the established "drugs of addic-tion": beyond overcoming the initial aversive prop-
copyright. on January 17, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.39.9.641 on 1 S
eptember 1984. D
ownloaded from

643
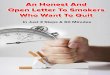
Table Rates ofsuccessful abstinence from smoking using nicotine gum
Reference Validation method Follow Percentage treatment success Diseased or Allocated orup (m) healthy volunteer
Chewing gum Advice Controlonly
Active Placebo
36 COHb and 12 10 14 9 Diseased Passivethiocyanate
37 COHb 6 26 28 Healthy Volunteer38 Expired CO 6 63 45 Healthy Volunteer39 Expired CO 12 47 21 Healthy Volunteer40 COHb 6 23 5 14 Healthy Passive41 COHb or expired CO 12 38 14 Healthy Volunteer42 COHb 12 23 Healthy Volunteer43 Expired CO 12 9 4 4 Healthy Passive44 Expired CO 12 30 20 Healthy Volunteer
CO-Carbon monoxide; COHb-Carboxyhaemoglobin.
erties of nicotine, smokers do not appear to developan increasing tolerance to the drug. Studies ofintravenous self administration show that nicotine isa less robust reinforcer of habit than other drugs ofabuse-for example, heroin.29 Nevertheless, theproportion of smokers who appear to be dependenton their habit appears large by comparison withthose dependent on other socially sanctioneddrugs-for example, alcohol.An alternative model for the smoker's behaviour
views smoking as a "psychological tool."30 Analysisof questionnaire data suggests that, in addition todependence on nicotine, both the stimulant and thesedative action of smoking are important motivesfor smoking.3' Administration of nicotine to non-smoking subjects improved their short term perfor-mance in tasks requiring rapid information proces-sing,32 presumably through control of electrocorticalarousal. Several animal studies have shown that theeffect of nicotine on arousal is biphasic, initial stimu-lation being followed by a compensatory phase ofdepression. It is likely that smokers could learn tomodulate their level of arousal through smoking.Whichever of these models is preferred, the
potential value of sources of nicotine other thantobacco in controlling smoking is clear, particularlyduring initial withdrawal. Interest in substitutes fortobacco has been wide ranging, encompassing bothpharmacological analogues such as lobeline andalternative means of nicotine administration such asnicotine chewing gum,33 snuff,34 and nasal sprays oraerosols of nicotine.35 The most thoroughly exploredof these substitutes is nicotine containing chewinggum.The results of some of the studies of the use of
nicotine chewing gum in which abstinence fromsmoking was verified biochemically are summarisedin the table. Follow up in these studies varied fromsix months to one year. Healthy people and thosewith diseases associated with smoking have been
included and studies on individuals who volunteeredto participate in a study of withdrawal have beendistinguished from those in which participantsmerely agreed to receive treatment to discouragesmoking. Although we must be cautious about com-paring these different studies it becomes clear thatpeople who volunteer for smoking abstinence pro-grammes are more likely to succeed whatever isoffered them than those smokers who are simplyallocated a treatment. In general, however, smokerswho volunteer for smoke cessation appear capableof being aided by nicotine containing chewing gum.This probably offers a simple means of identificationof those smokers attending a physician who wouldbe most suitable for this approach. How long thetobacco substitution should continue remains uncer-tain. It is maintained usually for only three monthsduring the initial withdrawal period, but a case couldbe made for extending this period. Further work inthis area is necessary.The physician is still left with the question of how
best to help the patient with a low level of motiva-tion to quit smoking. The size of this problem inclinical practice is well illustrated in the BritishThoracic Society (BTS) study (p 651), where longterm abstinence was achieved by less than 10% ofpatients with smoke related disease. Treatment wasrandomly allocated and nicotine chewing gum wasfound to offer no more help in giving up smokingthan advice or placebo gum.
Non-specific intervention
Bernstein45 commented over 15 years ago that clin-ics specialising in smoking withdrawal, where coun-sellors offer advice and guidance, have had moreeffect on research and clinical activity than on smok-ing behaviour. The comment remains valid in 1984.In general, fairly equivocal results have beenreported by specially designed antismoking clinics.
copyright. on January 17, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.39.9.641 on 1 S
eptember 1984. D
ownloaded from

644
Most achieve 15-20% long term abstinence, butinferior results are seen where biochemical ver-ification of self reporting is used.24
In contrast to smoking withdrawal clinics thatoffer general advice, a physician's advice to a patientto quit smoking may have a greater impact, particu-larly in the presence of dramatic symptoms.46 Thiseffect is seen in patients recovering from myocardialinfarction.23 This trend is further supported by theBTS study (p 651), again particularly in men whohave suffered a myocardial infarction. Otheridentifiable health professionals, such as nurses, maybe as effective as doctors.4' Although there remainsuncertainty about the content of the advice thatshould be given, there is clearly a need to exploit allof the opportunities offered when a smoker presentswith concurrent medical problems.
Hypnosis48 and acupuncture49 have been sug-gested as aids to abstinence and both enjoy somepopular support. Reports of controlled studies have,however, shown little convincing evidence and alegacy of chaotic early studies leaves considerabledoubt about the efficacy of these forms of treatment.The use of aversive stimuli to reduce the probabil-
ity of smoking-for example, electric shocktreatment-does not appear to contributesignificantly to the response of human subjects.50Rapid smoking procedures may be an effective aver-sion treatment, but concern has been expressedabout their safety." Interestingly, there are noreports on the effect of behavioural treatments suchas yoga on smoking cessation.
Controlled smoking
The disappointing results of these measures forcethe physician to consider how best to cope with themajority of patients who continue to smoke despiteall the aids to abstinence. Although strictly notwithin the realm of quitting smoking, a case can bemade for considering controlled smoking, to lessenthe risks to health associated with continued smok-ing.The first step is to reduce the amount of inhaled
smoke. There have been dramatic changes in thetypes of cigarette smoked over the last 20 years.Filter cigarettes have become the norm and averagetar yields have declined significantly.'2 This probablyreflects the desire of most smokers to reduce therisks of smoking. Anxieties have been expressedabout this approach because of uncertainty aboutwhat components of tobacco smoke are associatedwith the development of disease. Reduction in taryield is, however, likely to contribute to a decline inthe risk of developing lung cancer and ischaemicheart disease.'3 Furthermore, human smokers do
not necessarily smoke in the same way as the analyt-ical smoking machines on which cigarette tar yieldsare determined. For example, when smokers"switch" from higher to lower tar cigarettes there isevidence that they inhale more smoke or "over-smoke."27 This may be the result of a need toincrease the uptake of nicotine, as the falls incigarette yields of tar have been generally associatedwith a corresponding reduction in nicotine yield.There seems to be some uncertainty about thedegree of "oversmoking" of low tar cigarettes.Rawbone demonstrates in this issue (p 657) that inthe smokers' own environment, as opposed to thelaboratory setting, the degree of oversmoking of lowtar cigarettes appears to be small. Interestingly, likeother workers he did not find any increase in thenumber of low tar cigarettes consumed daily.One way to avoid oversmoking of lower tar
cigarettes is to increase the yield of nicotine relativeto tar.'4 Such higher nicotine but low tar cigaretteswould be unlikely to require compensatory over-smoking. Indeed, there is now some evidence thatlower tar cigarettes with enhanced nicotine yield areproving popular among smokers.
It is possible to control the level of tobacco expos-ure not only by reducing the number and strength ofthe cigarettes smoked but also by altering the man-ner in which cigarettes are smoked." Smokers canbe encouraged to take fewer puffs of smoke from acigarette and to inhale less. The long term stabilityof such changes still needs to be verified before thisbehavioural approach can be applied generally.
Alternatively, cigarette smokers may switch tosmoking pipes and cigars.46 While these forms ofsmoking are not usually associated with inhalationand pipe and cigar smokers carry only a smallincreased risk, ex-cigarette smokers who switchappear to continue to inhale.24 Inhalation presum-ably is controlled at an unconscious level. Thecigarette smoker who switches can therefore achievecomparable or even increased tobacco smokeexposure. The change in form of tobacco use cannotbe recommended as a form of controlled smokingunless specific training is offered to alter the mannerof smoking.
How should a physician approach smoking cessa-tion?
From this review it is clear that there are only weakpointers to the best course of action. Neverthelesssome tentative guidelines can be offered.
Firstly, it should be recognised that initial cessa-tion is only the start of treatment. Continued assis-tance and support should be planned from the start,perhaps by the use of health professionals other than
copyright. on January 17, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.39.9.641 on 1 S
eptember 1984. D
ownloaded from

645
physicians.In the presence of illness associated with smoking,
advice on its own appears effective when offered bya physician or other health professional. Considera-tion should be given to counselling the spouse orcohabitant who continues to smoke. Above all,advice should be offered with kindness, enthusiasm,and awareness of the many factors which may beinfluencing the continuation of the smoker's habit.Punitive approaches may be counterproductive andlack compassion. Explanation of the psychologicaleffects of withdrawal should be offered and fears ofsymptoms such as weight gain during abstineneeshould be allayed.
Alternative sources of nicotine other than tobaccoin the form of nicotine gum or nasal spray may havea particular place in the withdrawal programme forsmokers who are highly motivated to stop. Thisapproach may also be more effective in smokersshowing a pharmacological dependence on nicotineas determined by the smoking patterns test ques-tionnaire.3'For those smokers who consistently fail to quit,
advice should be directed towards controlled smok-ing with the aim of achieving at the least a significantreduction in the number of cigarettes smoked and achange to the brand of cigarette offering the lowesttar yield.
ConclusionMore information is needed about why people takeup smoking, particularly in the case of the young, sothat coherent strategies for prevention can bedevised. An historical analysis of international com-parisons of usage of tobacco goods might be usefulin identifying the cultural factors which determinesmoking habits within each country. For thoseinveterate smokers who are unable or unwilling toquit we need to know even more about the elementsof tobacco smoke which are associated withdevelopment of disease so that at least their riskscan be minimised. There is a need to identify moreclearly the factors which most influenced the mil-lions of smokers who have successfully abstainedwithout requiring direct medical advice. The rela-tively limited success of intervention in smoking ces-sation programmes compared with spontaneous ces-sation emphasises the fact that we remain largelyignorant about the causes of a form of behaviourundertaken by just under 40% of the population inthe United Kingdom. TIM HIGENBOlTAM
ANDREW CHAMBERLAINAddenbrooke's Hospital
Hills RoadCambridge
References
'Doll R, Hill AB. Smoking and carcinoma of the lung. BrMed J 1950;ii: 739-48.
2 General Household Survey. Cigarette smoking: 1972 to1982. OPCS Monitor. GHS 83/3. London: Govern-ment Statistical Service 1983.
Eysenck HJ. Personality and the maintenance of thesmoking habit. In: Dunn, WL Jun, ed. Smokingbehaviour: motives and incentives. Washington DC:VH Winston and Sons, 1973:113-46.
4 Guilford JS. Factors related to successful abstinence fromsmoking: final report. Washington DC: US PublicHealth Service, Division of Chronic Diseases Bureauof State Service, 1966:170.
5 Russell MAH. Cigarette smoking: natural history ofdependence disorder. Br J Med Psychol 1977;44: 1-16.
6 Smith GM. Personality correlates of cigarette smoking instudents of college age. Ann Aca Sci 1967; 142:308-21.
Kandel D. Stages in adolescent involvement in drug use.Science 1975; 190:912-4.
8 McKennell AC. British research into smokingbehaviour. In: Borgatta EF, Evans RR, eds. Smokinghealth and behaviour. Chicago: Aldine PublishingCompany, 1968:140-64.
9Meyer AS, Friedland LN, Lazarsfield PF. Motivationalconflicts engendered by the on-going discussion ofcigarette smoking. In: Dunn WL, ed. Smokingbehaviour: motives and incentives. Washington DC:VH Munstor and Sons, 1973:243-54.
'0 US Public Health Service. State legislation on smokingand health 1976. Washington: US Department ofHealth, Education and Welfare, Public Health Ser-vice, Centre for Disease Control, Bureau of HealthEducation, National Cleaninghouse for Smoking andHealth. 1976:73.
"Schuman LM. Patterns of smoking behaviour. In: JarvikME, Cullen JW, Gritz ER, Vogt TM, West LJ, eds.Research on smoking behaviour. (NIDA ResearchMonograph 17.) Washington DC: Department ofHealth, Education and Welfare, 1977:36-65. (Publi-cation No (ADM) 578-581.)
12 Reeder LG. Sociocultural factors in the aetiology ofsmoking behaviour: An Assessment. In: Jaruik ME,Cullen JW, Gritz ER, Vogt TM, West LJ, eds.Research on smoking behaviour. Washington DC:Department of Health, Education and Welfare, 1978.(NIDA Research Monograph 17 Department ofHealth, Education and Welfare Publications N(ADM)78-581.)
'3 McArthur C, Waldron E, Dickinson J. The psychologyof smoking. Journal of Abnormal Psychology1958;56:267-75.
Caplan RD, Cobb S, French JRP. Relationships of cessa-tion of smoking with job stress, personality and socialsupport. J Appl Psychol 1975;60:211-9.
'5 Thomas CB. The relationship of smoking and habits ofnervous tension. In: Dunn WL Jun, ed. Smokingbehaviour: motives and incentives. Washington DC:VH Winston and Sons, 1973:153-70.
16 Eisinger RA. Psychosocial predictors of smoking. JHealth Social Behaviour 1971; 12:355-62.
7 National Cancer Institute. The smoking digest. Progress
copyright. on January 17, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.39.9.641 on 1 S
eptember 1984. D
ownloaded from

646
report on a nation kicking the habit. Washington DC:US Department of Health, Education and Welfare,Public Health Service, National Institutes of HealthNational Cancer Institute, 1977:127.
18 Levitt EE. The television cigarette commercial: teenagetransducer or paper tiger? Yale Scientific Magazine1970;45: 10-3.
'9 Peto J. Price and consumption of cigarettes: a case forintervention? Br J Prev Soc Med 1974;28:241-5.
20 Cox H, Marks L. Sales trends and survey findings: Astudy of smoking in 15 OECD countries. HealthTrends 1983; 15:48-52.
21 Lando HA. Measurement and technique innovations.An objective check upon self-reported smoking levels.A preliminary report. Behav Ther 1975;6:547-9.
22 Cohen SI, Perkins NM, Ury HK, Goldsmith JR. Carbonmonoxide uptake in cigarette smoking. Arch EnvironHealth 1971;22:55-60.
23 Wilcox RG, Hughes J, Roland J. Verification of smokinghistory in patients after infarction using urinarynicotine and cotinine measurements. Br Med J1979;ii: 1026-8.
24 Butts WC, Kuehneman M, Widdowson GM. Automatedmethod for determining serum thiocyanate, to distin-guish smokers from non-smokers. Clinical Chemistry1974;20: 1344-8.
25 DeLarue NC. The antismoking clinic: is it a potentialcommunity service? Canadian Medical AssociationJournal 1973; 108:1164-5,1168,1171-2,1192.
26 Artho AJ, Grob K. Nicotine absorption from cigarettesmoke. Zeitschrift fuer Praeventivmedizin1964;9:14-25.
27 Ashton H, Stepney R, Thompson JW. Self titration incigarette smokers. Br Med J 1979;ii:357-60.
28 Schneider NG, Jarvik ME. Time course of smokingwithdrawal symptoms as a function of nicotinereplacement. Psychopharmacology 1984;82: 143-4.
29 Henningfield JE, Goldberg SR. Nicotine as a reinforcerin human subjects and laboratory animals. Phar-macology, Biochemistry and Behaviour 1983;19:989-92.
301 Ashton H, Stepney R. Smoking as a psychological tool.In: Smoking psychology and pharmacology. AshtonH, Stepney R, eds. London: Tavistock Publications,1982:90.
31 Russell MAH, Peto J, Patel UA. The classification ofsmoking by a factorial structure of motives. Journal ofthe Royal Statistical Society 1974; 137:313-46.
32 Wesnes K, Warburton DM. Effects of scopalomine andnicotine on human rapid information processing per-formance. Psychopharmacology 1984;82: 147-50.
33 Ferno 0, Lichtnecket SJA, Lundgrem CEG. A substi-tute for tobacco smoking. Psychopharmacologia1973;31:201-4.
34 Russell MAH, Jarvis MJ, Feyerabend C. A new age forsnuff? Lancet 1980;i:474-5.
35 Jacobson NL, Jacobson AA, Philip J. Non-combustiblecigarette: alternative method of nicotine delivery.Chest 1979;76:355-6.
36 Comparison of four methods of smoking withdrawal inpatients with smoking related diseases. Report by asubcommittee of the Research Committee of the Brit-ish Thoracic Society. Br Med J 1983;286:595-7.
37 Axelsson A, Brantmark B. The antismoking effect ofchewing gum with nicotine of high and low bioavaila-bility. In: Proceedings ofthe 3rd World Conference on
Smoking and Health. Volume II. Steinfield J, GriffithsW, Ball K, Taylor RM, eds. Washington: Departmentof Health, Education and Welfare Publ No (NIH)77-1413, 1977:549-59.
38 Fagerstrom K. A comparison of psychological andpharmacological treatment in smoking cessation.Journal of Behavioural Medicine 1982;5: 343-51.
39 Jarvis MJ, Raw M, Russell MAH, Feyerabend C. Ran-domised controlled trial of nicotine chewing gum. BrMed J 1982;285:537-40.
40 Malcolm RE, Sillett RW, Turner JAM, Ball KP. The useof nicotine chewing gum and psychological treatmentsfor dependent smokers. Psychopharmacology1980;70:295-6.
41 Raw M, Jarvis MJ, Feyerabend C, Russell MAH. Com-parison of nicotine chewing gum and psychologicaltreatments for dependent smokers. Br Med J1980;281:481-2.
42 Russell MAH, Wilson C, Feyerabend C, Cole PV. Effectof nicotine chewing gum on smoking behaviour as anaid to cigarette withdrawal. Br Med J 1976;ii:391-3.
43 Russell MAH, Merriman R, Stapleton J, Taylor W.Effect of nicotine chewing gum as an adjunct togeneral practitionee s advice against smoking. Br MedJ 1983;287:1782-5.
44 Schneider NG, Jarvik ME, Forsythe AB. Nicotine gumin smoking cessation: a placebo controlled double-blind trial. Addiction Behaviour 1983;8:253-62.
45 Bernstein DA. Modification of smoking behaviour: anevaluative review. Psychological Bulletin1969;71:418-40.
46 Rose G. Physician counselling and personal interven-tion. In: Stenfield J, Griffiths W, Ball J, Taylor RM,eds. Proceedings of the Third World Conference onSmoking and Health, New York 1975. Volume II.Washington: Department of Health, Education andWelfare (Publ), No (NIH) 77-1413, 1977:515-23.
47 Raw M. Persuading people to stop smoking. Behaviour,Research and Therapy 1976;14:97-101.
48 Barkley RA, Hastings JE, Jackson TL. The effects ofrapid smoking and hypnosis in the treatment of smok-ing behaviour. International Journal of Clinical andExperimental Hypnosis 1977;25:7-17.
49 Steiner PP, Hay DL, Davis AW. Acupuncture therapyfor treatment of tobacco smoking addiction. AmericanJournal of Chinese Medicine 1982; 10:107-13.
50 Russell MAH, Armstrong E, Patel UA. Temporal con-tiguity in electric aversion therapy for cigarette smok-ing. Behaviour Research and Therapy 1976; 14:103-23.
Lichtenstein E, Glasgow RE. Rapid smoking: sideeffects and safe-guards. Journal of Consulting andClinical Psychology 1977;45:815-21.
52 Fairweather FA, Carmichael IA, Phillips GF, CopelandGKE. Changes in the tar, nicotine and carbon monox-ide yields of cigarettes sold in the United Kingdom.Health Trends 1981;13:77-81.
Higenbottam TW, Shipley MJ, Rose G. Cigarette lungcancer and coronary heart disease: the effects of inha-lation and tar yield. Journal of Epidemiology andCommunity Health 1982;36: 113-7.
54 Russell MAH. Low tar, medium nicotine cigarettes: anew approach to safer smoking. Br Med J1976;i: 1430-3.
5- Frederiksen LW. Single case designs in the modificationof smoking. Addictive Behaviour 1976; 1:311-9.
copyright. on January 17, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.39.9.641 on 1 S
eptember 1984. D
ownloaded from