-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
1/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs=…
Offi cial reprint from UpToDatewww.uptodate.com ©2015
UpToDate
AuthorsNelson B Schiller, MDXiushui Ren, MDBryan Ristow, MD,
FACC,
FASE, FACP
Section Editor Warren J Manning, MD
Deputy Editor Susan B Yeon, MD, JD,FACC
Echocardiographic evaluation of the thoracic and proximal
abdominal aorta
All topics are updated as new evidence becomes available
and our peer review process is complete.
Literature review current through: Aug 2015. | This topic
last updated: Jul 16, 2015.
INTRODUCTION — Echocardiography enables qualitative and
quantitative evaluation of the thoracic and proximal
abdominal aorta. Transthoracic echocardiography (TTE) provides
views of the proximal ascending aorta, aortic
arch and portions of the descending aorta. However,
transesophageal echocardiography (TEE) rather than TTE is
indicated for comprehensive imaging of the aorta, especially in
the emergency evaluation of aortic dissection or
traumatic rupture of the aortic isthmus. (See "Clinical
manifestations and diagnosis of aortic dissection" and
"Transesophageal echocardiography in traumatic rupture of the
aortic isthmus".)
Echocardiographic evaluation of the aorta for atherosclerotic
plaque, sinus of Valsalva aneurysms, aortic dilation,and dissection
will be reviewed here.
NORMAL AORTIC ROOT AND ASCENDING AORTA — The proximal
ascending aorta attaches to the left
ventricle at the annulus (hinge line of the aortic leaflets) and
includes the aortic root (comprised of the three
sinuses of Valsalva), the sinotubular junction, and the tubular
ascending portion of the aorta. The aortic root is a
direct continuation of the left ventricular outflow tract and is
located right and posterior to the pulmonary
infundibulum. The lower portion of the aortic root is connected
to the muscular interventricular septum, the
membranous septum, and to the mitral-aortic fibrous continuity
(also known as the mitral-aortic intervalvular
fibrosa).
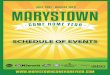
Two-dimensional echocardiography — Transthoracic
echocardiography (TTE) examination of the proximal
ascending aorta is generally performed in the left parasternal
long-axis view (image 1). Many sonographers limit
their interrogation of the aorta to the proximal sinuses of
Valsalva, missing the opportunity to more fully visualize
the aorta. Moving up an intercostal interspace, moving the probe
closer to the sternum, or tilting the probe cranially
enables imaging of the more superior ascending aorta.
Right parasternal views, recorded with the patient in a right
lateral decubitus position, may also be revealing [1].
This method is especially useful when the aorta dilates to
the right of the sternum.
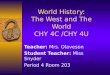
A cr oss sectional image of the aortic root is
obtained in the parasternal short-axis view (figure 1). The
suprasternal
notch view visualizes the aortic arch.
Transesophageal echocardiography (TEE) provides more highly
resolved images of the ascending aorta, aortic
arch, and descending thoracic aorta than TTE, although a
small portion of the distal ascending aorta and proximal
arch cannot be seen due to interposition of the left mainstem
bronchus and trachea.
All imaged portions of the aorta should be evaluated for
the presence of plaque, dilation and dissection (including
intramural hematoma). Views used for measurement should be those
that show the maximum diameter of the
aortic root [1]. The aortic root at the level of the sinuses
generally has the largest diameter (normal ≤3.7 cm), while
the ascending aortic diameter at the sinotubular junction and
above is slightly smaller (normal
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
2/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs=… 2
views on adequate TTE or TEE images. The left main artery can
often be followed to and beyond its bifurcation
into the anterior descending artery and circumflex artery (image
2A-B); the right coronary artery can usually be
followed for up to 3 cm from its origin. While echocardiography
is not a practical method to detect luminal
obstruction, careful gain manipulation makes it possible to
detect larger bright densities along the course of the
vessel that probably represent proximal calcification.
In adults, an anomalous origin of the coronary arteries is
difficult to establish with an echocardiogram. The best
clue to the presence of a single coronary artery, or one that
ends in a coronary cameral fistula, is to observe the
greatly enlarged coronary artery origin often associated with
this abnormality. At times, these vessels dilate to the
point that they may be confused with a sinus of Valsalva
aneurysm. (See "Congenital and pediatric coronary artery
abnormalities".)
Most cameral fistulae that terminate in one of the ventricles
can be detected and localized by observing the
abnormal color flow signal that marks the entrance of the
fistula into the chamber. There are several reports from
Japan of success in identifying the proximal aneurysms of
Kawasaki's disease by echocardiography. (See
"Cardiovascular sequelae of Kawasaki disease".)
M-mode echocardiography — The motion of the aortic root on
the M-mode echocardiogram is an indicator of
global left ventricular systolic and diastolic function [3-5].
Since aortic root motion reflects the events of atrial filling
and emptying, it also provides information about left atrial
function (image 3A-C).
During systole, the aortic root normally moves anteriorly over 7
mm and returns almost completely to its starting
point immediately after the conclusion of ejection. The atrial
or presystolic contribution to aortic root motion is
normally minimal.
Abnormal aortic root motion on M-mode echocardiography —
If the systolic excursion of the aortic root is
decreased, stroke volume is probably reduced, an effect that is
independent of the left ventricular ejection fraction.
As an example, if the left ventricle is hypovolemic but
contracts normally, the aortic root motion will be decreased.
Aortic root motion will also be decreased if the ejection
fraction is severely reduced and the ventricle is increased
in size (image 4).
AORTIC PLAQUE — Atherosclerotic plaque is visualized as a
region of intimal thickening or protrusion. Plaquemay be
accompanied by focal calcifications, ulcerations, and/or
superimposed thrombi. The presence of thoracic
aortic plaque, even when visualized in the descending aorta, has
been associated with an increased risk of
ischemic stroke [6]. Aortic plaque may be a marker of vascular
disease and other risk factors for cerebrovascular
disease [7,8]. Care must be taken not to confuse anterior aortic
wall thickening with the right coronary artery.
Studies have found increased risk of stroke among patients with
protruding aortic atheroma ≥ 4 or 5 mm thick. Our
institution uses the following transesophageal echocardiography
(TEE) grading scale for aortic intimal thickness:
grade 0 = normal, grade 1 = mild intimal thickening, grade 2 =
moderate intimal thickening less than 5 mm, grade 3
= protruding atheroma ≥ 5 mm thick, and grade 4 = mobile thrombi
on atheroma.
On TEE, the presence of large, mobile, or ulcerated plaques is
associated with increased risk of stroke [ 9,10]. The
Augmented root motion with full opening of the aortic
valve suggests a high cardiac output. High output
states are quite easy to recognize and their appreciation is
helpful in clinical management. (See "High-outputheart
failure".)
●
Normal or augmented systolic motion of the aortic root in the
face of reduced aortic leaflet separation
suggests atrial filling out of proportion to aortic flow and is
typical of mitral insufficiency.
●
If the initial diastolic posterior motion of the aortic root is
slowed, and the late diastolic posterior motion of the
aorta is exaggerated with atrial systole, reduced LV compliance
is suspected.
●
Aortic root motion tends to be flat in restrictive
diastolic states, reflecting the reduced cardiac output
generally associated with restrictive cardiomyopathy.
●
http://www.uptodate.com/contents/high-output-heart-failure?source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/9,10http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/7,8http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/6http://www.uptodate.com/contents/image?imageKey=CARD%2F53355&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F58902%7ECARD%2F56155%7ECARD%2F79751&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/3-5http://www.uptodate.com/contents/cardiovascular-sequelae-of-kawasaki-disease?source=see_linkhttp://www.uptodate.com/contents/congenital-and-pediatric-coronary-artery-abnormalities?source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F79123%7ECARD%2F54573&topicKey=CARD%2F5293&rank=1%7E150&source=see_link
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
3/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs=… 3
management of aortic plaques is discussed separately. (See
"Embolism from aortic plaque: Thromboembolism"
and "Embolism from atherosclerotic plaque: Atheroembolism
(cholesterol crystal embolism)".)
Calcification of the aortic valve, aortic root, and sino-tubular
junction is associated with reduced survival among
individuals with coronary artery disease [11]. The presence of
calcification along these sites may be a marker of
increased vascular disease independent of other medical risk
factors.
SINUS OF VALSALVA ANEURYSMS — Sinus of Valsalva aneurysms
are occasionally seen on long- and short-
axis views of the two-dimensional echocardiogram. However,
quantitative criteria for sinus of Valsalva aneurysm
are lacking. Since asymmetry of the sinuses is occasionally
encountered in clinical practice, such a definitionwould be
helpful. Lacking a published definition, we propose that a diameter
from the widest portion of the
asymmetric sinus to the opposing wall of greater than 4 cm in
adults be adopted as a working definition.
The most common location is the right sinus of Valsalva, from
which rupture may extend into the right ventricle or,
less frequently, the right atrium or interventricular septum [
12].
The next most likely location of the aneurysm is the noncoronary
sinus, followed by the left sinus. Infrequently, the
aneurysm ruptures into the left ventricle (mimicking aortic
regurgitation) or into the left atrium. In a report of 86
patients undergoing sinus of Valsalva aneurysm repair, 44
percent had associated aortic regurgitation [12].
Contrast echocardiography is helpful in delineating the aneurysm
and shunt arising from rupture [13]. However,
color flow Doppler imaging is the technique of choice for
identifying a ruptured sinus of Valsalva aneurysm.
AORTIC DILATION — The 2011 ACC/AHA practice guidelines for
echocardiography recommend
echocardiography for evaluation of suspected dilation of the
proximal aorta (movie 1) [14]. Transthoracic
echocardiography (TTE) is recommended as the first choice for
this indication with transesophageal
echocardiography (TEE) used only if the TTE examination is
incomplete or additional information is needed.
Multimodality imaging guidelines from the American Society of
Echocardiography recommend measuring aortic
dimensions from leading edge to leading edge at end diastole,
based on reference studies using this technique
[15].
The ACC/AHA guidelines also recommend echocardiography to
evaluate aortic root dilation in Marfan syndrome or
other connective tissue syndromes. In addition, the guidelines
recommend TTE to examine first-degree relatives of
patients with Marfan syndrome or other connective tissue
disorders. The 2010 ACC/AHA guidelines for the
diagnosis and management of patients with thoracic aortic
disease recommend echocardiogram should be
performed at the time of diagnosis of Marfan syndrome, six
months thereafter to determine the rate of
enlargement, and annually if stability of the aortic diameter is
documented and less than 4.5 cm [16]. The
diagnosis and management of the Marfan syndrome are discussed
separately. (See "Genetics, clinical features,
and diagnosis of Marfan syndrome and related disorders"
and "Management of Marfan syndrome and related
disorders".)
The 2014 ACC/AHA practice guidelines for valvular disease
recommend measuring the diameters of the aortic root
and ascending aorta by TTE for patients with a bicuspid aortic
[17]. Magnetic resonance imaging (MRI) or
computed tomography (CT) is recommended if the aortic root or
ascending aorta cannot be adequately measured
by echocardiography. Yearly echocardiography, MRI, or CT is
recommended for patients with bicuspid aortic
valves and dilation of the aortic root or ascending aorta
(diameter greater than 4.0 cm, with consideration of a
lower threshold for patients of small stature). Issues related
to bicuspid aortic valve disease are discussed
separately. (See "Clinical manifestations and diagnosis of
bicuspid aortic valve in adults" and "Management
of
adults with bicuspid aortic valve disease" and "Natural
history and management of chronic aortic regurgitation in
adults" and "Pregnancy in women with a bicuspid aortic
valve" .)
Limited data are available to compare echocardiography and CT
evaluation of thoracic aortic dilation and thoracic
aneurysm. In a small prospective study of 44 patients with known
ascending aortic aneurysm, TTE and CT
measurements of aortic diameters correlated well [18]. Ectasia
is defined as aortic dilation up to 50 percent greater
http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/18http://www.uptodate.com/contents/pregnancy-in-women-with-a-bicuspid-aortic-valve?source=see_linkhttp://www.uptodate.com/contents/natural-history-and-management-of-chronic-aortic-regurgitation-in-adults?source=see_linkhttp://www.uptodate.com/contents/management-of-adults-with-bicuspid-aortic-valve-disease?source=see_linkhttp://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-bicuspid-aortic-valve-in-adults?source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/17http://www.uptodate.com/contents/management-of-marfan-syndrome-and-related-disorders?source=see_linkhttp://www.uptodate.com/contents/genetics-clinical-features-and-diagnosis-of-marfan-syndrome-and-related-disorders?source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/16http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/15http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/14http://www.uptodate.com/contents/image?imageKey=CARD%2F79876&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/13http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/12http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/12http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/11http://www.uptodate.com/contents/embolism-from-atherosclerotic-plaque-atheroembolism-cholesterol-crystal-embolism?source=see_linkhttp://www.uptodate.com/contents/embolism-from-aortic-plaque-thromboembolism?source=see_link
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
4/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs=… 4
than the normal reference diameter, and aneurysm is defined as
greater than 50 percent dilation [16].
Causes of aortic root and ascending aortic dilation and aneurysm
formation include hypertension (the most
common cause), atherosclerosis, aortic dissection, aortic
stenosis (post-stenotic dilation), bicuspid aortic valve
(associated with aortic dilation even without significant
stenosis), aortic regurgitation, and the Marfan syndrome
and other causes of annuloaortic ectasia. Less common etiologies
of aortic dilation include inflammatory causes,
such as Takayasu arteritis and infectious causes, such as
syphilis. (See "Clinical manifestations and diagnosis of
thoracic aortic aneurysm".)
Various disease processes are associated with different patterns
of aortic dilation:
Aortic dissection — TEE is an appropriate initial test to
evaluate suspected aortic dissection (image 7) [25].
Choice among TEE, MRI or CT for initial noninvasive imaging of
aortic dissection is governed by clinical
considerations and availability (see "Clinical manifestations
and diagnosis of aortic dissection").
TEE imaging can help determine the potential for aortic
valve-sparing operations [ 26]. The 0-degree high
esophageal view is appropriate for diagnosing ascending aortic
dissection. However, TEE evaluation of branch
vessel involvement may be incomplete and additional imaging with
other techniques may be required [ 27].
The role of TTE in suspected aortic dissection is primarily for
diagnosis of cardiac complications of dissection,including aortic
insufficiency, pericardial effusion/tamponade, and regional left
ventricular systolic function.
Advances in echocardiography have improved the sensitivity
of TTE for aortic dissection to approximately 85
percent or more [15], although TTE remains less sensitive for
detection of aortic dissection than TEE, CT, and
MRI. Thus, absence of a dissection flap on TTE should not be
used to exclude aortic dissection. In a study of 172
consecutive patients receiving operations for proximal aortic
dissection, TTE identified intimal dissection flaps in
159 [28]. TTE may be able to visualize an undulating intimal of
a dissection (image 8), but the normal
brachiocephalic vein can often be seen adjacent and superior to
the aortic arch in the suprasternal notch view
(image 9), and this should not be mistaken for a dissection.
DESCENDING THORACIC AORTA AND AORTIC ARCH — The descending
thoracic aorta can be seen
posterior to the long- and short-axis parasternal views on
transthoracic echocardiography (TTE) ( image 10A-D). Inthe
parasternal long-axis view, the descending aorta can be seen in
cross-section at the posterior atrioventricular
groove, situated outside the pericardium. In the parasternal
short-axis plane, an oblique longitudinal section of the
descending aorta can be seen.
Imaging can identify dilation or an aneurysm and may permit
detection of dissection. The descending aorta is a
useful landmark for distinguishing pleural and pericardial
effusions, since the pericardium encloses the heart
anterior to the descending aorta.
On TTE, the aortic arch is visualized in the suprasternal notch
view. This view is recommended as a routine
component of TTE examination, particularly in cases with
bicuspid aortic valve which is frequently associated with
Hypertension appears to have a minor impact on aortic root
diameter at the level of the sinuses of Valsalva
[19-21], but is associated with enlargement at the sinotubular
junction and tubular ascending aorta [ 19].
●
Congenital aortic stenosis is associated with more significant
post-stenotic dilation than degenerative aortic
stenosis with similar valve areas (image 5) [22].
●
Symmetric dilation of the three sinuses is most commonly seen in
patients with Marfan syndrome [23,24].
This dilation usually, but not always, terminates abruptly at
the sinotubular junction and gives these roots a
distinctive appearance unlike that of other causes of
annuloaortic ectasia (image 6A-B). In addition to root
dilation, patients with Marfan syndrome frequently have aortic
regurgitation because aortic annulus dilation
causes cusp malcoaptation (image 6A-B). Issues related to
echocardiography in Marfan syndrome arediscussed separately. (See
"Genetics, clinical features, and diagnosis of Marfan syndrome and
related
disorders".)
●
http://www.uptodate.com/contents/genetics-clinical-features-and-diagnosis-of-marfan-syndrome-and-related-disorders?source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F52118%7ECARD%2F50641&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F52118%7ECARD%2F50641&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/23,24http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/22http://www.uptodate.com/contents/image?imageKey=CARD%2F51528&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/19http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/19-21http://www.uptodate.com/contents/image?imageKey=CARD%2F60999%7ECARD%2F53998%7ECARD%2F79701%7ECARD%2F61910&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F103367&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F75705&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/28http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/15http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/27http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/26http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-aortic-dissection?source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/25http://www.uptodate.com/contents/image?imageKey=CARD%2F69205&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-thoracic-aortic-aneurysm?source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/16
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
5/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs=… 5
coarctation of the aorta. In the suprasternal notch view, color
and spectral Doppler interrogation of the proximal
descending aorta may detect accelerated flow characteristic of
coarctation. If forward velocity in the descending
aorta by continuous-wave Doppler exceeds 2 m/sec, aortic
coarctation should be suspected. If the run-off at the
site of coarctation is delayed, severe coarctation must be
considered, and alternate imaging modalities such as
MRI can be helpful in confirming diagnosis and grading severity.
(See "Clinical manifestations and diagnosis of
coarctation of the aorta", section on 'Echocardiography'.)
Views of the descending thoracic aorta as it courses along the
spine can be obtained in the apical views; posterior
angulation often produces long-axis (in the two chamber view)
and short-axis (in the four chamber view) images
(image 10C). Although the aorta is too deep in the far field to
be well resolved, the size of the aorta can generally
be measured. A normal caliber aorta is evidence against
dissection at that location.
3D echocardiographic imaging provides an intuitive overview of
structures and their relation to each other as
illustrated by an example of a mobile aortic mass (movie 2).
However, 2D images (movie 3) provide additional
clues to the accurate diagnosis of a vegetation, including
thickening of the aortic wall consistent with
inflammation, a fluid-filled collection around the aorta
consistent with abscess, and the absence of calcification
or
shadowing that would have been more typical of atherosclerotic
disease with adjacent thrombus.
When aortic dissection involves the thoracic aorta, especially
if there is extravasation of blood around the aorta,
the vessel can be imaged from the left paraspinal window. This
strategy can be used to supply additional evidence
about the state of the thoracic aorta. However, transesophageal
echocardiography is the method of choice for detecting
pathology of the thoracic aorta.
Abdominal aorta — Subcostal imaging of the proximal
abdominal aorta is often included in the TTE examination
[29]. The structure can be found to the left of the spine
running parallel, but to the left of and deep to, the
inferior
vena cava (image 11A-B). Differentiation of the aorta from the
vena cava can be made by appreciating the systolic
pulsations of the aorta, which are usually easy to
recognize.
Using the subcostal approach, atheromatous irregularities and
aneurysms of the proximal abdominal aorta are
readily seen (image 12A-C). Since the descending aorta is closer
to the transducer in this view than in other TTE
views, the yield for intimal flaps of aortic dissection is
higher from this window. In addition, comparing the
smoothness of the inner layer of the aorta to the vena cava
gives some indication of the degree of atheromatous
change that is present in the aorta and, by inference, in the
remainder of the vascular tree. Atheromatous change
is typically appreciated as obvious irregularities along the
usually smooth interior of the vessel.
Although transesophageal echocardiography (TEE) is the
preferred technique for evaluating the aorta, it does not
image the aorta very far below the diaphragm [30]. Ideally,
linear arrays should be used for more comprehensive
evaluation of the abdominal aorta.
Transcatheter aortic valve implantation — Echocardiographic
evaluation of the aorta is a critical component of
multimodality imaging for transcatheter aortic valve replacement
as discussed in detail separately. (See "Imaging
for transcatheter aortic valve replacement".)
OTHER GREAT VESSELS — Transthoracic echocardiography (TTE)
is useful in evaluating the other great
vessels.
Pulmonary artery — In the parasternal long-axis view,
imaging just superior to the left atrium usually
demonstrates the left pulmonary artery as it crosses under the
ascending aorta. Inspecting the bifurcation of the
pulmonary artery in its long-axis (in the parasternal short-axis
view) may reveal the relationship between the left
pulmonary artery and the descending aorta (image 13A-B). Color
Doppler near the pulmonary artery bifurcation in
this view can detect the retrograde continuous flow
characteristic of a patent ductus arteriosus.
Carotid arteries and subclavian vessels — The innominate,
left common carotid, and left subclavian vessel
origins can be imaged by TTE from the suprasternal notch. From
the neck, the carotid and vertebral arteries can
be studied effectively by trained vascular sonographers using
dedicated linear array transducers. Skill in
http://www.uptodate.com/contents/image?imageKey=CARD%2F64091%7ECARD%2F63066&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/imaging-for-transcatheter-aortic-valve-replacement?source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/30http://www.uptodate.com/contents/image?imageKey=CARD%2F67861%7ECARD%2F81130%7ECARD%2F60665&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F77731%7ECARD%2F77191&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/29http://www.uptodate.com/contents/image?imageKey=CARD%2F103369&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F103368&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/image?imageKey=CARD%2F79701%7ECARD%2F60999&topicKey=CARD%2F5293&rank=1%7E150&source=see_linkhttp://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-coarctation-of-the-aorta?source=see_link§ionName=Echocardiography&anchor=H21#H21
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
6/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs=… 6
performing this examination is helpful when evaluating a patient
for dissection of the aorta because detection of
extension of the dissection into the carotid arteries has
important clinical implications.
SUMMARY AND RECOMMENDATIONS
Use of UpToDate is subject to the Subscription and License
Agreement.
REFERENCES
1. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for
cardiac chamber quantification byechocardiography in adults: an
update from the American Society of Echocardiography and the
European
Association of Cardiovascular Imaging. J Am Soc
Echocardiogr 2015; 28:1.
2. Campens L, Demulier L, De Groote K, et al. Reference values
for echocardiographic assessment of thediameter of the aortic root
and ascending aorta spanning all age categories. Am J Cardiol 2014;
114:914.
3. Djalaly A, Schiller NB, Poehlmann HW, et al. Diastolic aortic
root motion in left ventricular hypertrophy.Chest 1981; 79:442.
4. Strunk BL, Fitzgerald JW, Lipton M, et al. The posterior
aortic wall echocardiogram. Its relationship to leftatrial volume
change. Circulation 1976; 54:744.
5. Pratt RC, Parisi AF, Harrington JJ, Sasahara AA. The
influence of left ventricular stroke volume on aorticroot motion:
an echocardiographic study. Circulation 1976; 53:947.
6. Blackshear JL, Pearce LA, Hart RG, et al. Aortic plaque in
atrial fibrillation: prevalence, predictors, andthromboembolic
implications. Stroke 1999; 30:834.
7. Nam HS, Han SW, Lee JY, et al. Association of aortic plaque
with intracranial atherosclerosis in patientswith stroke. Neurology
2006; 67:1184.
8. Meissner I, Khandheria BK, Sheps SG, et al. Atherosclerosis
of the aorta: risk factor, risk marker, or innocent bystander?
A prospective population-based transesophageal echocardiography
study. J Am CollCardiol 2004; 44:1018.
9. Ferrari E, Vidal R, Chevallier T, Baudouy M. Atherosclerosis
of the thoracic aorta and aortic debris as amarker of poor
prognosis: benefit of oral anticoagulants. J Am Coll Cardiol 1999;
33:1317.
Transthoracic echocardiography (TTE) provides views of the
proximal ascending aorta, aortic arch, and
portions of the descending aorta. However, transesophageal
echocardiography (TEE) is superior to TTE for
comprehensive imaging of the aorta, especially in the emergency
evaluation of aortic dissection or traumatic
rupture of the aortic isthmus. (See "Clinical manifestations and
diagnosis of aortic dissection" and
"Transesophageal echocardiography in traumatic rupture of the
aortic isthmus".)
●
TEE provides more highly resolved images of the ascending aorta,
aortic arch, and descending thoracic aorta
than TTE, although a small portion of the distal ascending aorta
and proximal arch cannot be seen by TEE
due to interposition of the left mainstem bronchus and trachea.
(See 'Two-dimensional echocardiography'
above.)
●
The presence of large, mobile, or ulcerated plaques in the
thoracic aorta on TEE is associated with an
increased risk of stroke. (See 'Aortic plaque' above.)
●
Echocardiography is the primary modality for identification of
sinus of Valsalva aneurysms and any
associated shunt arising from rupture. (See 'Sinus of Valsalva
aneurysms' above.)
●
Echocardiography enables identification of aortic dilation and
is indicated for monitoring of individuals at risk
for progressive aortic dilation, particularly those with Marfan
syndrome or a bicuspid aortic valve. (See 'Aortic
dilation' above.)
●
TEE is an appropriate initial test to evaluate suspected aortic
dissection. Choice among TEE, MRI, or CT for
initial noninvasive imaging of aortic dissection is governed by
clinical considerations and availability. (See
"Clinical manifestations and diagnosis of aortic
dissection".)
●
http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-aortic-dissection?source=see_linkhttp://-/?-http://-/?-http://-/?-http://www.uptodate.com/contents/transesophageal-echocardiography-in-traumatic-rupture-of-the-aortic-isthmus?source=see_linkhttp://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-aortic-dissection?source=see_linkhttp://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/9http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/8http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/7http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/6http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/5http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/4http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/3http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/2http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/1http://www.uptodate.com/contents/license
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
7/34
27/9/2015 Echocardiographic evaluation of the thoracic
and proximal abdomi nal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs=… 7
10. Milani RV, Lavie CJ, Gilliland YE, et al. Overview of
transesophageal echocardiography for the chestphysician. Chest
2003; 124:1081.
11. Saha SA, Beatty AL, Mishra RK, et al. Usefulness of an
Echocardiographic Composite Cardiac CalciumScore to Predict Death
in Patients With Stable Coronary Artery Disease (from the Heart and
Soul Study).
Am J Cardiol 2015; 116:50.
12. Moustafa S, Mookadam F, Cooper L, et al. Sinus of Valsalva
aneurysms--47 years of a single center experience and
systematic overview of published reports. Am J Cardiol 2007;
99:1159.
13. Terdjman M, Bourdarias JP, Farcot JC, et al. Aneurysms of
sinus of Valsalva: two-dimensional
echocardiographic diagnosis and recognition of rupture into the
right heart cavities. J Am Coll Cardiol 1984;3:1227.
14. American College of Cardiology Foundation Appropriate
Use Criteria Task Force, American Society of Echocardiography,
American Heart Association, et al.
ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011
Appropriate Use Criteria for Echocardiography. A Report of the
American College of Cardiology Foundation Appropriate Use
CriteriaTask Force, American Society of Echocardiography, American
Heart Association, American Society of Nuclear Cardiology,
Heart Failure Society of America, Heart Rhythm Society, Society for
Cardiovascular
Angiography and Interventions, Society of Critical Care
Medicine, Society of Cardiovascular ComputedTomography, Society for
Cardiovascular Magnetic Resonance American College of Chest
Physicians. J AmSoc Echocardiogr 2011; 24:229.
15. Goldstein SA, Evangelista A, Abbara S, et al. Multimodality
imaging of diseases of the thoracic aorta in
adults: from the American Society of Echocardiography and the
European Association of Cardiovascular Imaging: endorsed by
the Society of Cardiovascular Computed Tomography and Society for
Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr 2015;
28:119.
16. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010
ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVMGuidelines for the
diagnosis and management of patients with thoracic aortic disease.
A Report of the
American College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines, American
Association for Thoracic Surgery, American College of
Radiology,American Stroke Association,Society of Cardiovascular
Anesthesiologists, Society for Cardiovascular Angiography and
Interventions,Society of Interventional Radiology, Society of
Thoracic Surgeons,and Society for Vascular Medicine. J AmColl
Cardiol 2010; 55:e27.
17. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC
guideline for the management of patients withvalvular heart
disease: a report of the American College of Cardiology/American
Heart Association Task
Force on Practice Guidelines. J Am Coll Cardiol 2014; 63:e57.18.
Tamborini G, Galli CA, Maltagliati A, et al. Comparison of
feasibility and accuracy of transthoracic
echocardiography versus computed tomography in patients with
known ascending aortic aneurysm. Am JCardiol 2006; 98:966.
19. Kim M, Roman MJ, Cavallini MC, et al. Effect of hypertension
on aortic root size and prevalence of aorticregurgitation.
Hypertension 1996; 28:47.
20. Palmieri V, Bella JN, Arnett DK, et al. Aortic root
dilatation at sinuses of valsalva and aortic regurgitation
inhypertensive and normotensive subjects: The Hypertension Genetic
Epidemiology Network Study .Hypertension 2001; 37:1229.
21. Vasan RS, Larson MG, Levy D. Determinants of
echocardiographic aortic root size. The Framingham HeartStudy.
Circulation 1995; 91:734.
22. Ben-Dor I, Sagie A, Weisenberg D, et al. Comparison of
diameter of ascending aorta in patients with severeaortic stenosis
secondary to congenital versus degenerative versus rheumatic
etiologies. Am J Cardiol 2005;96:1549.
23. Eisenberg MJ, Rice SA, Paraschos A, et al. The clinical
spectrum of patients with aneurysms of theascending aorta. Am Heart
J 1993; 125:1380.
24. Dev V, Goswami KC, Shrivastava S, et al. Echocardiographic
diagnosis of aneurysm of the sinus of Valsalva. Am Heart J
1993; 126:930.
25. Douglas PS, Khandheria B, Stainback RF, et al.
ACCF/ASE/ACEP/ASNC/SCAI/SCCT/SCMR 2007appropriateness criteria for
transthoracic and transesophageal echocardiography: a report of the
AmericanCollege of Cardiology Foundation Quality Strategic
Directions Committee Appropriateness Criteria WorkingGroup,
American Society of Echocardiography, American College of Emergency
Physicians, American
http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/25http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/25http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/24http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/23http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/22http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/21http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/20http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/19http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/18http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/17http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/16http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/15http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/14http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/13http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/12http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/11http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/10
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
8/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta?topicKey=CARD%2F5293&elapsedTimeMs=…
Society of Nuclear Cardiology, Society for Cardiovascular
Angiography and Interventions, Society of Cardiovascular
Computed Tomography, and the Society for Cardiovascular Magnetic
Resonance endorsedby the American College of Chest Physicians and
the Society of Critical Care Medicine. J Am Coll Cardiol2007;
50:187.
26. David TE, Feindel CM, Webb GD, et al. Long-term results of
aortic valve-sparing operations for aortic rootaneurysm. J Thorac
Cardiovasc Surg 2006; 132:347.
27. Cheitlin MD, Armstrong WF, Aurigemma GP, et al. ACC/AHA/ASE
2003 guideline update for the clinicalapplication of
echocardiography: summary article: a report of the American College
of Cardiology/AmericanHeart Association Task Force on Practice
Guidelines (ACC/AHA/ASE Committee to Update the 1997
Guidelines for the Clinical Application of Echocardiography).
Circulation 2003; 108:1146.28. Sobczyk D, Nycz K. Feasibility and
accuracy of bedside transthoracic echocardiography in diagnosis
of
acute proximal aortic dissection. Cardiovasc Ultrasound 2015;
13:15.
29. Eisenberg MJ, Geraci SJ, Schiller NB. Screening for
abdominal aortic aneurysms during transthoracicechocardiography. Am
Heart J 1995; 130:109.
30. Banning AP, Masani ND, Ikram S, et al. Transoesophageal
echocardiography as the sole diagnosticinvestigation in patients
with suspected thoracic aortic dissection. Br Heart J 1994;
72:461.
Topic 5293 Version 12.0
http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/25http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/30http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/29http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/28http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/27http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/26http://www.uptodate.com/contents/echocardiographic-evaluation-of-the-thoracic-and-proximal-abdominal-aorta/abstract/25
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
9/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs=… 9
GRAPHICS
Two-dimensional transthoracic echocardiogram
(2D TTE) parasternal long axis view
This parasternal long axis echocardiogram was obtained in
systole;
the aortic valve is open and the mitral is closed.
RV: right ventricle; IL: inferolateral left ventricular wall;
IVS: interventricular
septum; NCC: noncoronary cusp of the aortic valve; RCC: right
coronary cusp
of the aortic valve; aML: anterior mitral valve leaflet; pML:
posterior mitral
valve leaftlet; dAo: descending aorta.
Graphic 77446 Version 4.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
10/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 10
Two-dimensional transthoracic echocardiogram (2D TTE)
parasternal
short axis view of the aortic root
(A) A diagram of the transducer position for obtaining a short
axis two dimensional image; the
short axis is obtained by a 70° to 110° clockwise rotation of
the transducer from the parasternal
long axis, with superior and inferior transducer manipulations
and the plane is oriented at the
base of the heart (left panel).
(B and C) The parasternal short axis view from a transthoracic
echocardiogram shows the
noncoronary (NCC), right coronary (RCC) and left coronary (LCC)
leaflets of the aortic valve.
Also seen are the left atrium (LA), right atrium (RA), tricuspid
valve (TV), right ventricle (RV)
and pulmonic valve (PV).
Graphic 67673 Version 4.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
11/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 1
Short axis view of left main coronary artery
The short axis view, with the imaging plane through the aortic
root
(AO) just above the aortic valve, demonstrates the left main
coronary
artery (LMCA). Panel B shows the M-mode echocardiogram of
the
LMCA.
PV: pulmonary valve.
Graphic 79123 Version 2.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
12/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 12
Two-dimensional transthoracic echocardiogram
(2D TTE) from the parasternal short axis view at
the level of the coronary arteries
The origins of the right (RCA) and left (LCA) coronary arteries
can be
seen on the short axis precordial view, obtained through the
aortic
root (Ao) just above the valves; there is a vague "pinwheel"
relationship of the sweep of the arteries. Additionally, the
left atrial
appendage (LAA) is seen just inferior to the LCA and the
pulmonary
valve (PV) just superior.
LA: left atrium.
Graphic 54573 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
13/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 13
2D and M mode echocardiographic images of the
normal aortic root from the parasternal short axis
position
The M-mode beam is directed through the two dimensional image of
the
aortic root at the base of the heart (panel A). The resulting
M-mode
echocardiogram (panel B) demonstrates normal systolic and
diastolicmotion patterns; the anterior excursion is over 14 mm and
the diastolic
posterior excursion mainly occurs early in diastole. The aortic
(Ao) valve
leaflets open as widely as the internal dimensions of the root
permit and
remain open throughout systole, creating a box-like
configuration. The
anterior motion of the root and the behavior of the valve are
typical
findings when the stroke volume is normal.
PA: main pulmonary artery; LA: left atrium; RVOT: right
ventricular outflow tract.
Graphic 58902 Version 5.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
14/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 14
M-mode echocardiogram of normal aorta and left
atrium
The M-mode echocardiogram is obtained from the long
axisparasternal two dimensional view (panel A); the dotted line
represents
the M-mode beam passing through the aortic root, the right (R)
and
noncoronary (N) cusps of the aortic valve, and the left atrium
(LA).
The atrium is measured at end systole (arrows) when the descent
of
the left ventricle base has resulted in maximal filling.
Graphic 56155 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
15/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 15
Two-dimensional transthoracic echocardiogram (2D TTE) and
M mode echocardiographic images along with a
phonocardiogram of the normal aortic root from the
parasternal short axis position
Panel A shows the short axis view from a two-dimensional
echocardiogram recorded
at the base of the heart at the level of the aortic valve; the
line (M) bisecting the
aortic valve represents the plane of the M-mode beam used to
generate the M-
mode echocardiogram in panel B. The aortic valve opens nearly to
the aortic (Ao)
walls (panel B) and while opened it has a box-like
configuration. The line marks the
peak of the R wave on the ECG. There is a brisk anterior
systolic motion of the
entire Ao root and even faster earlier diastolic relaxation
(posterior motion); the
posterior movement of the aortic root occurs predominantly in
early diastole with
very little movement in late diastole. This pattern occurs in
young healthy hearts
that rely predominantly on early relaxation for filling rather
than atrial contraction.
The M-mode echocardiogram with simultaneous phonocardiogram is
seen in panel
C. The vibrations on the posterior moving non-coronary aortic
leaflet (down arrows)
are similar in timing and frequency with the low intensity,
early systolic "innocent"
murmur recorded on the phonocardiogram (up arrows). These
vibrations are
common in normal valves with normal or elevated cardiac
output.
Graphic 79751 Version 4.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
16/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 16
M-mode echocardiogram of aortic root in
cardiomyopathy
In cardiomyopathy with reduced stroke volume the systolic
anterior
excursion of the aortic (Ao) root is greatly reduced in
comparison to
the normal pattern. Additionally, the aortic valve (AoV) opening
is
greatly reduced and its duration abbreviated. Just after
achieving their
maximum separation, the AoV leaflets immediately begin
drifting
closed, with a loss of the normal box-like configuration.
Graphic 53355 Version 2.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
17/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 17
Aortic dilation in aortic stenosis
Aortic pathology can be better seen by imaging the ascending
aorta
one interspace above the usual long axis precordial window.
The
normal appearance of the sinuses and ascending aorta (Asc Ao)
is
seen in panel A. For comparison, panel B shows poststenotic
dilatation
which is quite typical and almost always found in aortic
stenosis.
AV: aortic valve; LA: left atrium; LV: left ventricle.
Graphic 51528 Version 2.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
18/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 18
M-mode echocardiogram of aortic regurgitation
The M-mode echocardiographic findings in aortic regurgitation,
due to
the Marfan syndrome in this case, include fluttering of the
mitral
valve (MV) (panel A) and a greatly dilated aortic root (Ao),
measuring
48 mm, in relationship to a small appearing left atrium (LA)
(panel B),
which measures 27 mm. The aortic to atrial diameter ratio has
been
used as a sign of the Marfan syndrome.
Graphic 52118 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
19/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 19
Aortic root enlargement
The normal aortic root (RT) and ascending aorta (AAo) are seen
in
panel A; slight prominence of the sinuses of Valsalva (SinV) can
be
appreciated. Panel B is the aortic RT and AAo from a patient
with the
Marfan syndrome; the SinV are large while the AAo is
relatively
normal, a pattern that seems unique to the Marfan syndrome. In
panel
C, a greatly enlarged aortic (Ao) RT is also seen, but the
pattern
differs from that seen in the Marfan patient; the dilatation
begins at
the aortic ring and continues beyond the sinotubular junction
well into
the AAo, considered to represent aortoannular ectasia.
Graphic 50641 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
20/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 20
TEE descending aortic dissection
Aortic dissection is characterized by the formation of an
"intimal flap" seen as a hyperechoic line
extending across the vessel delimiting two distinct lumens (A).
Color flow Doppler (B) depicts
higher (orange) blood flow velocity and intraluminal velocity in
the inferior of the two lumens,
but does not provide definitive information regarding which is
the true lumen and false lumen.
Courtesy of W Manning, MD.
Graphic 69205 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
21/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 2
Ascending aortic dissection on echocardiogram
Modified long axis view shows a proximal dissection of the
aortic root
(Ao), with a flap extending to the aortic valve (V). This
aortic
pathology is seen by imaging the ascending aorta one
interspace
above the usual long axis precordial window.
LA: left atrium; LV: left ventricle.
Graphic 75705 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
22/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 22
Suprasternal notch view of aortic arch and brachiocephalic
vein
In this view, taken with the neck extended and the probe
positioned at the suprasternal notch and
caudally, the aortic arch is visualized centrally. The aortic
vessel wall is a linear structure that se
the aorta from the brachiocephalic vein; this should not be
confused with a dissection. The
brachiocephalic vein has continuous flow in both systole and
diastole when visualized by color Do
and this further differentiates the structure from the aorta or
branch arteries.
Graphic 103367 Version 1.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
23/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 23
Mildly dilated thoracic aorta
The long axis precordial view shows slight dilation of the
thoracic
aorta (Th Ao).
CS: coronary sinus.
Graphic 60999 Version 2.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
24/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 24
Two-dimensional transthoracic echocardiogram
(2D TTE) from the parasternal long and short axis
views showing the descending thoracic aorta
The descending thoracic aorta can be seen from the parasternal
long
axis view. Both the long (panel A) and short axis (panel B)
precordial
views show the descending thoracic aorta (TAo). Note that the
short
axis imaging plane demonstrates the long axis of the TAo.
LV: left ventricle; RA: right atrium; LA: left atrium; Ao R:
aortic root.
Graphic 53998 Version 4.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
25/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 25
Two-dimensional transthoracic echocardiogram
(2D TTE) from a modified two-chamber view
showing the descending thoracic aorta
The descending thoracic aorta (T Ao) can be imaged from the
apical
two- and four-chamber view. Posterior angulation of the
transducer
(panel A) often opens the T Ao such that it can be seen in its
longaxis. Major pathology such as aneurysms can often be detected
in this
way. Anterior angulation in the apical two chamber view (panel
B)
demonstrates the proximal aortic arch (Ao).
LA: left atrium; LV: left ventricle; rpa: right pulmonary
artery.
Graphic 79701 Version 7.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
26/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 26
Two-dimensional transthoracic echocardiogram
(2D TTE) from a modified four-chamber view
showing the descending thoracic aorta
The thoracic or descending aorta (T Ao) can be imaged from
the
apical two- and four-chamber view. Posterior angulation (panel
B)
shows the T Ao in its short axis, located below the left atrium
(LA).Anterior angulation in four-chamber view (panel A) shows the
origin of
aortic root (Ao).
RA: right atrium; LA: left atrium.
Graphic 61910 Version 7.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
27/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 27
Two-dimensional transthoracic echocardiogram
(2D TTE) from the subcostal view showing the
abdominal aorta
The abdominal aorta (Ab Ao) can be seen in subcostal long (panel
A)
and short axis (panel B) views. The neural canal (NC) is seen
through
the intervertegral disc in this thin patient.
Graphic 77731 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
28/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 28
Echocardiographic image of the abdominal aorta
The abdominal (Ab) aorta (Ao) is seen from the subcostal long
axis(panel A) and short axis views (panel B). In this thin patient
the
neural canal (NC) is seen through the intervertegral disc in the
short
axis view.
RA: right atrium.
Graphic 77191 Version 2.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
29/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 29
Abdominal aortic aneurysm long and short axis
(A) The long axis view shows an aneurysm of the abdominal aorta
(A
Ao An) as the aorta crosses the diaphragm. Prominent plaques
just
beyond the aneurysm can be appreciated.
(B) The short axis through the aneurysm (An) also shows the
inferiorvena cava (IVC).
Graphic 67861 Version 5.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
30/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 30
Dissection of the abdominal aorta on longitudinal
ultrasound
The long axis view shows a dissection of the abdominal aorta
(AAo)
and the presence of a spiral flap (f).
Graphic 81130 Version 4.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
31/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 3
Dissection of the abdominal aorta on transverse
ultrasound
The short axis view shows a dissection (Dis) of the abdominal
aorta(AoAb) and a spiral flap (arrows).
Graphic 60665 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
32/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 32
Two-dimensional transthoracic echocardiogram
(2D TTE) from the right ventricular (RV) outflow
tract view showing the pulmonic valve and the
pulmonary artery bifurcation
Pulmonary artery (PA) bifurcation into the right (RPA) and left
(LPA)
pulmonary arteries can be seen in the short axis precordial
view. Note
that in this view the LPA is proximal to the descending aorta
(dAo).
Ao: aorta; RVOT: right ventricular outflow tract; pv:
pulmonic valve.
Graphic 64091 Version 3.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
33/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
http://www.uptodate.com/contents/echocardiographic-
evaluation-of-the-thoracic-and-proximal-
abdominal-aorta?topicKey=CARD%2F5293&elapsedTim eMs… 33
Pulmonary artery
The right pulmonary artery (RPA) can be seen in the precordial
long
axis view as it crosses under the transverse aorta (Ao),
superior to
the left atrium (LA).
Graphic 63066 Version 2.0
-
8/17/2019 ECG Interpretation - Made Incredibly Easy 5th
Edition(Chy Yong)
34/34
27/9/2015 Echocardiographic evaluation of the thoracic and
proximal abdominal aorta
Disclosures: Nelson B Schiller, MD Nothing to disclose.
Xiushui Ren, MD Nothing to disclose. Bryan
Ristow, MD, FACC, FASE, FACP Nothing to disclose. Warren J
Manning, MD Equity Ownership/Stock
Options: Pfizer (Pharmaceuticals). Equity Ownership/Stock
Options (Spouse): General Electric (Imaging
equipment). Susan B Yeon, MD, JD, FACC Nothing to disclose.
Contributor disclosures are reviewed for conflicts of interest
by the editorial group. When found, these are
addressed by vetting through a multi-level review process, and
through requirements for references to be
provided to support the content. Appropriately referenced
content is required of all authors and mustconform to UpToDate
standards of evidence.
Conflict of interest policy
Disclosures
http://www.uptodate.com/home/conflict-interest-policy



![CHY-Graphs on a Torus arXiv:1607.01871v1 [hep-th] 7 Jul · PDF fileCHY-Graphs on a Torus Carlos Cardonaa and Humberto Gomezb;c ... 3.2 The n-gon and its CHY-Graph7 3.2.1 CHY-Graph](https://img.dokumen.tips/doc/110x75/5ab0e31b7f8b9a7e1d8bb37d/chy-graphs-on-a-torus-arxiv160701871v1-hep-th-7-jul-on-a-torus-carlos-cardonaa.jpg)