Embed Size (px)
Citation preview

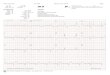
LBBB VT: It’s Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
• LBBB morphology wide QRS tachycardia: Why VT?• QRS width 160 ms
• Intrinsicoid deflection = 80 ms
• Atypical QRS pattern for LBBB: Observe precordial lead polarity V1 (negative), V2 (positive), v3-6 (negative)
• QS in leads v5, v6
Dr Jaspal Arneja DM, Dr Vinay Pandey MD

ARVD / ARVC : MORPHOLOGY
• Autosomal dominant inheritance,
variable penetrance
• Mutation in genes encoding for
desmosomal proteins
• Replacing cardiomyocytes by
adipose and fibrous tissue
• >1 mutation, worse outcome
Prevalence 1 in 5000
SCD IN YOUNG ADULTS

ARVD / ARVC: DISEASE PROGRESSION
• Phase 1 (Concealed): subtle RV structural changes, ±VAs
• Phase 2 (overt electrical disorder): symptomatic (PVCs / NSVT) or life-
threatening VAs with obvious RV morpho-functional abnormalities
• Phase 3 (RV failure): progression of RV disease (dyspnea)
• Phase 4 (biventricular failure): pronounced LV disease (fluid overload)
Presentation: Palpitations(VAs), Syncope, SCD
Presentation: HF
Onset 2nd or 3rd decade

ECG in Sinus rhythm in ARVC
• P wave: notched, widened (p wave duration>110 ms), flat or small peaked P wave.
• PR interval: Prolonged. First degree AV block in 16% patients.
• QRS complex: QRS prolongation (duration>110 ms) and terminal S wave prolongation (>55ms) in V1-V3.
• Fragmented QRS (notch before the end of R or S wave) seen in 51%
• Epsilon wave: most specific finding. Seen in 30% pts