Embed Size (px)
Citation preview

Eccrine Syringofibroadenoma of the eyelid associated with
prosthesis
C Keohane, N Bermingham, M Guerin, S Fenton
University Depts of Neuropathology & Ophthalmology Cork University Hospital
BAOP 2011

Eccrine syringofibroadenoma (ESFA)• A rare benign adnexal eccrine neoplasm
• Face, trunk and distal extremities in elderly individuals
• This case involved the eyelid, associated with enucleation and long standing prosthesis.
Case History
• 65-yo man • Superomedial left eyelid lesion posterior to his lash line • Present for 3 years, slowly enlarging• Left enucleation aged 1 year for a congenital
abnormality of unknown aetiology • Well -fitted prosthesis in situ.• Solitary elevated, non-tender polypoid lesion on the
upper left eye lid posterior to the gray line, 9 x 5 x 3mm. • Eye socket was unremarkable, no other skin lesions. • The mass was excised.


Pseudoepitheliomatous hyperplasia
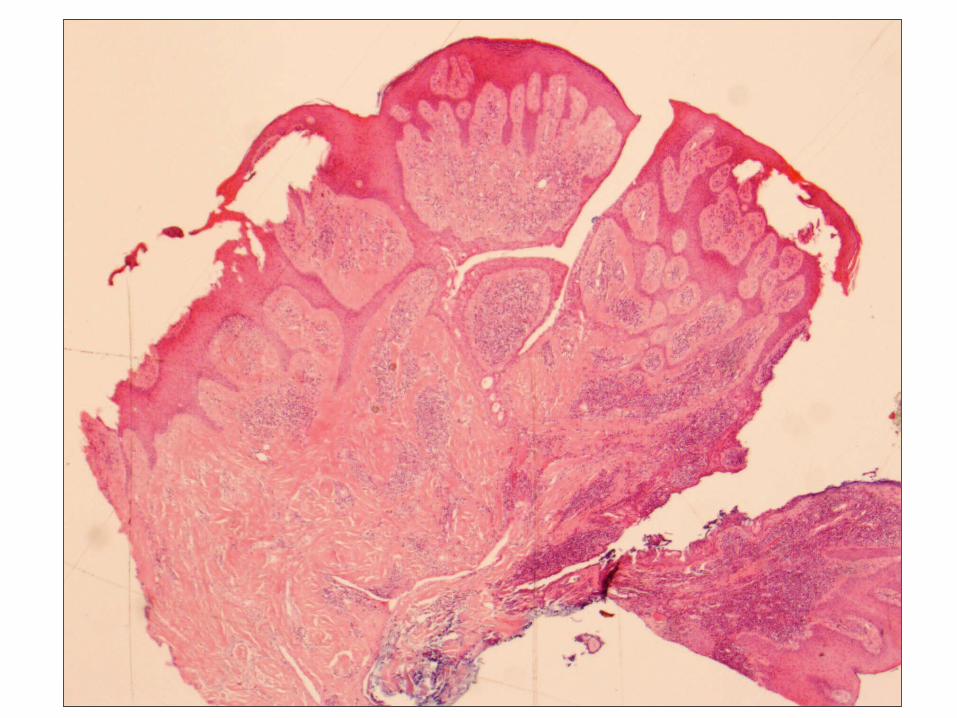

Lattice like epithelial strands

AE1-3 B
B

CEA
Glandular structuresCEA positive

Eccrine syringofibroadenoma ESFA
• Rare lesions on skin of elderly people
• Very similar to a type of tumour ‘’fibroepithelial tumour of Pinkus’• Surgical excision curative
• May occur in association with chronic active inflammation and as a reactive phenomenon
• Histology branching anastomosing strands of epithelium with ductal structures in a fibrovascular stroma. Epithelial strands are attached to the undersurface of the epidermis.
• The luminal cells show positive staining for carcinoembryonic antigen.
• A few cases have been associated with syringofibrocarcinoma

Differential Diagnosis
• Fibroepithelial tumour of Pinkus
• Pseudoepitheliomatous hyperplasia.
• The ductal differentiation in the epithelial strands demonstrated by EMA and CEA exclude these possibilities.

• The prominence of plasma cells has been previously noted .
• The rarity of this lesion, its occurrence in association with a longstanding prosthetic eye and dense chronic inflammation and fibrosis suggests that in this case it may me reactive in nature.

An unusual presentation and a new treatment of eccrine SyringofibroadenomaJowkar F, Naseri M, Aslani FJournal of Pakistan Association of Dermatologists 2006; 16: 112-115.

ESFA• First described by Mascaro in 1963
• Five clinical variants
• 1) solitary lesions
• 2) multiple lesions associated with ectodermal dysplasia (autosomal recessive Schopf Schulz Passarge and Cloustons syndrome)
• 3) Multiple lesions without associated cutaneous anomalies
• 4) Non-familial unilateral multiple linear lesions
• 5) A reactive process associated with chronic inflammatory or other skin lesions ; dermatosis, bullous pemphigus, palmoplantar erosive lichen planus and chronic diabetic foot ulcers.

ESFA Variants• Variant: The clear cell variant was reported by Fretzin in 1995. It is
characterized by nests of periodic acid Schiff-positive clear cells resembling the clear-cell variant of syringoma.
• Multiple palmoplantar Eccrine syringofibroadenomas are a cutaneous marker of the Schopf syndrome- hidrocystomas of the eyelid, hypotrichosis- less than normal amount of hair on the head or body, hypodontia- fewer than the normal number of teeth, and nail dystrophy
• • ESFA has also been described in association with Clouston
syndrome, a genetically determined autosomal dominant ectodermal dysplasia with hypotrichosis, nail dystrophy, palmoplantar hyperkeratosis and pigmentation over joints. The causative mutations are in GJB6 gene (Connexin 30).
Ocular lesions with ESFA• To our knowledge, solitary eyelid ESFA has not previously been
described. • Chen et al. described familial ESFA with ophthalmic abnormalities in
both parent and children including ectropians and entropians, absence of punctae, corneal vascularisation and scarring, and absent eyelashes and meibomian glands. ESFA plaques in those cases were on the feet, toes, scrotum , thighs and back.
• Multiple ESFAs associated with ectodermal dysplasia (Schopf Schulz Passarge Syndrome) can also involve the eyelid, but the hand lesions in that syndrome are ESFAs, the eyelid lesions are apocrine hidrocystomas. Optic atrophy can be found in some cases.
• There were no features of this syndrome in our patient and family history was negative.

• ReferencesBrenn T & Mc Kee PH . Tumors of the Sweat Glands. Ch 29 In : Mc Kee PH, Calonje E, Granter SR eds Pathology of the Skin vol 2 3rd edition Elsevier Mosby, Philadelphia 2005 Mascaro JM. Considerations sur les tumeurs fibroepitheliales: le syringofibroadenome eccrine. Ann Dermatol Syphiligr.1963;90 :143-153
Clarke LE, Joffreda M, Abt AB Eccrine Syringofibroadenoma Arising in Peristomal Skin. A Report of Two Cases. Int J Surg Pathol;11;1, 61-63 2003
Schöpf E, Schulz HJ, Passarge E. Syndrome of cystic eyelids, palmo-plantar keratosis, hypodontia and hypotrichosis as a possible autosomal recessive trait. Birth Defects Orig Artic Ser 1971; 7: 219–221.
Castori M, Ruggieri S, Giannetti L, Annessi G, Zambruno G.Schöpf-Schulz-Passarge Syndrome: Further Delineation of the Phenotype and Genetic ConsiderationsActa Derm Venereol 2008; 88: 607–612
Chen S. Eccrine syringofibroadenoma: A report of a familial case with ophthalmologic findings.J Am Acad Dermatol 1998;39 :356-8
Acknowledgement:Dr J Fitzgibbon


• Schöpf-Schulz-Passarge syndrome is a rare ectodermal dysplasia, • multiple eyelid apocrine hidrocystomas, palmo-plantar keratoderma,
hypodontia, hypotrichosis and nail dystrophy.• The clinical spectrum and the most likely inheritance pattern(s)
have not yet been completely defined. Optic atrophy. Both individuals were born to consanguineous parents, and one also has affected siblings. A literature review identified 23 additional cases. Multiple eyelid apocrine hidrocystomas, described in all of the cases, are the hallmark of this condition, although they usually appear in adulthood. The concomitant presence of eccrine syringofibroadenoma in most patients and of other adnexal skin tumours in 44% of affected subjects indicates that Schöpf-Schulz-Passarge is a genodermatosis with skin appendage neoplasms. However, the risk of skin and visceral malignancies is not increased. 9 of the 13 published familial cases may be explained by an autosomal recessive mutation, while the remaining pedigrees show apparent vertical transmission compatible with genetic heterogeneity. The benign disease course and advanced age at diagnosis could also suggest locus homogeneity for a recessive mutation with instances of pseudodominant inheritance.