Embed Size (px)
Citation preview

E
AGa
b
ARRAA
KAEPALLLAC
1
pT1(Amcv[pItf
cf
PY
0h
Leukemia Research 37 (2013) 1027– 1034
Contents lists available at SciVerse ScienceDirect
Leukemia Research
j o ur nal ho me page: www.elsev ier .com/ locate / leukres
arly T-cell precursor leukemia/lymphoma in adults and children
shleigh Allena, Anthony Sirecia, Adrianna Colovaia, Kerice Pinkneyb, Maria Sulisb,ovind Bhagata, Bachir Alobeida,∗
Department of Pathology, Columbia University Medical Center and New York Presbyterian Hospital, New York, NY, USADepartment of Pediatrics, Division of Hematology and Oncology, Columbia University Medical Center, New York, NY, USA
a r t i c l e i n f o
rticle history:eceived 10 January 2013eceived in revised form 28 May 2013ccepted 8 June 2013vailable online 1 July 2013
eywords:LLarly T-cell precursors
a b s t r a c t
Early T-cell precursor-ALL (ETP-ALL) is a subtype of T-ALL with a poor prognosis in children. We analyzedETP-ALL compared to conventional T-ALL/LBL in both adults and children to determine any differencesin clinical outcomes, based on the following parameters: induction failure, relapse, and survival. Patientswith ETP-ALL have a higher risk of relapse, especially in children (in all patients, HR = 4.08, p = 0.127, andchildren, HR = 11.63, p = 0.025). ETP-ALL seems to have an increased risk of adverse outcomes, particularlyin children. Larger studies are needed to better determine the prognosis of this subtype of T-ALL.
© 2013 Elsevier Ltd. All rights reserved.
rognosiscute leukemiaeukemiaymphomaymphoblasticdults
hildren. Introduction
T lymphoblastic leukemia/lymphoma (T-ALL/T-LBL) is a neo-lasm of immature hematopoietic precursors committed to the-cell lineage (T lymphoblasts). T-ALL comprises approximately5% of childhood and 25% of adult acute lymphoblastic leukemiaALL) [1]. Despite the relatively high morbidity and mortality of T-LL compared to B-cell ALL, outcomes in T-ALL have improved usingodern treatment protocols [2]. Multiple studies have reported
omplete remission rates as high as 94% [3–5], and long term sur-ival as high as 85% in both pediatric and adult T-ALL patients3,4]. However, there remains a subset of pediatric and adult T-ALLatients who fail to respond to treatment and have poor outcomes.
n an effort to determine the causes of these poor outcomes, inves-igators have attempted to sub-classify T-ALL based on moleculareatures [6–11] with disparate conclusions.
A physiologic subset of precursor T-cells, known as early T-ell precursors (ETPs), are considered early thymic immigrantsrom the bone marrow [12–16]. These cells have a unique
∗ Corresponding author at: Columbia University Medical Center, Department ofathology and Cell Biology, 630 West 168th Street, Vanderbilt Clinic 14-229, Nework, NY 10032, USA. Tel.: +1 212 342 0545; fax: +1 212 305 2301.
E-mail address: [email protected] (B. Alobeid).
145-2126/$ – see front matter © 2013 Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.leukres.2013.06.010
immunophenotype and have multi-lineage differentiation poten-tial [12,16]. A recent study by Coustan-Smith et al. looked atgene expression profiles of pediatric T-ALL patients and foundthat leukemic blasts in a subset of cases had gene expression pro-files similar to ETP and a characteristic immunophenotype [7]. Theauthors concluded that ETP-ALL is associated with poor outcomesin pediatric patients.
The aim of this study was to elucidate the clinical outcomesof ETP-ALL in a patient population comprising both adults andchildren diagnosed with T-ALL/LBL and followed at our institutionusing standard treatment protocols adopted for use in T-ALL. In thisanalysis, we sought to identify these cases using only immunophe-notypic techniques available for routine diagnosis.
2. Materials and methods
2.1. Cases
We searched our departmental database to identify all cases of T-ALL/LBL diag-nosed between January 2000 and August 2011. Cases were separated into ETP-ALLand non-ETP ALL based on immunophenotype as determined by flow cytometryanalysis at the time of diagnosis. Morphologic evaluation was performed using
hematoxylin & eosin stained sections of bone marrow and lymph node biopsies, aswell as Giemsa stained bone marrow aspirate/peripheral blood smears. All cases metthe current diagnostic criteria for T-ALL/LBL [1]. All patients were treated accord-ing to standard treatment protocols available at the time of diagnosis. All pediatricT-LBL patients were staged according to the St. Jude staging criteria [17].
1 Research 37 (2013) 1027– 1034
aeomccc
2
iseCosCCwCtdiaaodwa
2
amtmptpwu(a
2
Fvaadrfc
3
3
2adeccvtata
Table 1Patient demographics.
All T-ALL/LBL ETP-ALL p value
Number of patients 48 41 7
SexMale 34 28 6 0.66Female 14 13 1
Age<1 1 1(2%) 0 11 < 10 18 16 (39%) 2 (29%) 0.7010–18 19 17 (41%) 2 (29%) 0.69>18 10 7 (17%) 3 (43%) 0.15
WBC>50 17 16 (39%) 1 (14%) 0.4<50 31 25 (61%) 6 (86%)
Pediatric 38 34 (83%) 4 (57%) 0.62High risk 24 22 (65%) 2 (50%)
EthnicityBlack 4 3 (7%) 1 (14%) 0.48Caucasian 19 17 (41%) 2 (29%) 0.69Hispanic 13 11 (27&) 2 (29%) 1Other 12 10 (24%) 2 (29%) 1
Residual disease>5% 6 5 (12%) 1 (14%) 1<5% 3 2 (5%) 1 (14%) 0.38
Lymphoma 15 15 (37%) 0 1Induction Failure 9 7 (17%) 2 (29%) 0.60
028 A. Allen et al. / Leukemia
Electronic medical records were reviewed for the following clinical parameterst diagnosis: age, white blood cell count and percentage of marrow and periph-ral blood blasts. Response to therapy, remission status, survival data and clinicalutcomes were obtained. We examined induction failure, initial response to treat-ent (assessed by comparing day 10–18 bone marrow and peripheral blood blast
ounts with those at diagnosis), and residual disease post induction. Risk stratifi-ation groups for pediatric patients were defined by the National Cancer Instituteriteria [18].
This study was approved by our institutional review board (IRB).
.2. Flow cytometry analysis
Fresh bone marrow aspirate, peripheral blood and/or lymph node biopsy spec-mens were processed for multiparameter flow cytometry analysis (FC) usingtandard methods as described previously [19]. In summary, four-color flow cytom-try was performed using FACSCalibur flow cytometer (BD Bioscience, San Jose,A, USA) according to standard procedures and utilizing a comprehensive panelf monoclonal antibodies. The antigens tested included: CD45, CD2, cytoplasmic &urface CD3, CD5, CD7, CD4, CD8, CD43, TCR alpha beta, TCR gamma delta, CD10,D34, CD1a, TdT, CD16/56, CD19, CD20, CD79a, cytoplasmic IgM, HLA-DR, CD13,D33, CD117, and MPO (BD Bioscience). Data were analyzed using BD FacsDiva soft-are (BD Bioscience), and different hematopoietic elements were gated using theD45/side scatter display. Lymphoblasts were defined as CD45dim cells (comparedo normal lymphocytes) with low- to intermediate side scatter profiles. Cases wereefined as ETP-ALL when T lymphoblast phenotype was CD1a−, CD8−, CD5dim+,
n conjunction with expression of at least one of the following myeloid or stem cellntigens: CD13, CD33, CD34, CD117, and/or HLA-DR. T lymphoblasts were defineds CD5dim if the median fluorescence index (MFI) of the blasts was less than thatf the mature T lymphocytes in the sample. Cases with inadequate flow cytometryata to differentiate between ETP-ALL and conventional T-ALL/LBL were excluded, asere cases lacking sufficient clinical follow-up information to determine outcomes
s defined above.
.3. Cytogenetic and molecular analysis
As part of the diagnostic process, all cases underwent routine cytogeneticnalysis. G-banding of metaphase preparations was performed using standardethods, and the karyotypes were described according to the International Sys-
em of Human Cytogenetic Nomenclature (ISCN) 2009 [20]. FISH was performed onethanol–acetic acid fixed cells according to standard protocols, and the panel of
robes used targeted the common recurrent chromosome abnormalities for hema-ologic malignancies using the following probes: TEL/AML1, MLL, BCR/ABL, and16/CEP9, and MYC (Abbott Molecular, Des Moines, IL, USA). Fluorescence signalsere captured after counterstaining with 4′ ,6-diamidino-2-phenylindole (DAPI)sing the Cytovision Imaging system attached to a Nikon Eclipse 600 microscopeApplied Imaging, Santa Clara, CA, USA). Polymerase chain reaction analyses of IGHnd/or T-cell receptor (TCR) gene rearrangements were also performed.
.4. Statistical analysis
Statistical analysis was performed using SAS version 9.2 and Graph Pad Prism.isher’s exact test was used to compare proportions between groups. Continuousariables were compared using a Mann–Whitney U test. For all above analyses,ge stratification was performed using a cut off of 18 years to separate childrennd adults. Kaplan–Meyer curves were created with induction failure, relapse andeath as end points in both groups and were compared using the log-rank test. Cor-esponding Cox proportional hazards model with built in ETP phenotype as a riskactor for these outcomes was performed. Values with a p-value less than 0.05 wereonsidered statistically significant.
. Results
.1. Characteristics of cases
We retrieved 54 cases of T-ALL/LBL diagnosed between January000 and August 2011. Of these, 6 cases were excluded due to lack ofdequate clinical data. Seven (15%) of the remaining 48 cases, wereetermined to be ETP-ALL and 41 conventional T-ALL/LBL. How-ver, if the T-LBL cases are excluded, the percentage of ETP-ALLases rises to 21%. Thirteen patients were females (1 ETP-ALL, 12onventional T-ALL/LBL) and 35 were males (6 ETP-ALL and 29 con-entional T-ALL/LBL). Follow up periods ranged from 3 weeks (due
o early death during induction in one patient) to 11.8 years with anverage of 3.5 years. The age of the patients ranged from 8 monthso 81 years, median 13 years and mean of 17.3 years. There were 10dults over the age of 18, 3 ETP-ALL and 7 conventional T-ALL/LBL.Relapse 14 11 (27%) 3 (43%) 0.40Death 12 11 (27) 1 (14%) 0.66
The rest (38) were children age 18 and under, 4 ETP-ALL and34 conventional T-ALL/LBL. Other patient demographics are listedin Table 1. Patients were treated according to Dana Farber Can-cer Institute (DFCI), Children’s Oncology Group (COG), Cancer andLeukemia Group regimen B (CALGB), or Memorial Sloan Kettering(NY-I or NY-II) research protocols with the following exceptions: 1patient was treated with hyper CVAD, one with the Berlin-FrankfurtMunster (BFM90-HR) protocol and one with L-CHOP. One patient’streatment protocol was unknown (Table 2).
3.2. Clinical features
The presenting features of the patients were varied. The mostcommon presenting symptom in both groups was lymphadeno-pathy (LAD). In both groups, many patients presented with signsand symptoms of cytopenias (anemia and thrombocytopenia)including fatigue, petechial hemorrhages, nosebleeds and dizzi-ness. Three conventional T-ALL/LBL patients presented with heartmurmur. All three had mediastinal masses. In total, 25 (61%) ofthe conventional T-ALL/LBL patients presented with mediastinalmasses, however, only one ETP-ALL patient had a mediastinal masson presentation (p = 0.0376 compared to all T-ALL/LBL, p = 0.20compared to T-ALL only). One ETP-ALL patient presented with chestpain and cough. This patient did not have a mediastinal mass. Therewere no other unique presenting symptoms to distinguish the twogroups.
For the seven ETP-ALL patients, the clinical information is asfollows: At presentation, patient 1 was a 30-year old male whopresented with chest pain and dry cough. He was treated withDFCI protocol and remains disease free after 2 years. Patient 2 wasa 13-year old Hispanic boy who presented with bilateral diffuselymphadenopathy. He was treated with BFM95 protocol with ini-
tial remission but relapsed after a year. He was placed on DFCIprotocol for second treatment and remains in remission 8 yearsafter diagnosis of relapse. Patient 3 is a 42-year old male who pre-sented with lymphadenopathy, abdominal pain and fever. He was
Research 37 (2013) 1027– 1034 1029
tmot1apawHfdcssiihpiwpc6
3
pcvew
3
npAbhhg(trpNbccFg(twT
pc(dIst
Fig. 1. CD 5 expression of T-lymphoblasts. (A) shows the fluorescence intensity ofCD5 in blasts (green) and non-neoplastic T-lymphocytes (red) in an ETP-ALL patient.
A. Allen et al. / Leukemia
reated with DFCI protocol with successful induction. However, 5onths later, he relapsed and was treated with hyper CVAD with-
ut success. He later received a matched, unrelated donor, stem cellransplant and has since been disease free (8 years). Patient 4 was a5-year old Caucasian female who presented with bilateral cervical,xillary and inguinal lymphadenopathy. She was treated with DFCIrotocol with successful remission induction. She has been off ther-py for 6 years. Patient 5 was a 49-year old African American maleho was transferred from an outside hospital emergency room.is initial presentation and treatment are unknown; however he
ailed induction (residual symptoms and residual disease > 5%). Heied two months after diagnosis. Patient 6 was a 7-year old Cau-asian male who presented with sore throat, diarrhea and facialwelling. He was treated with COG protocol ALL0434 but had remis-ion failure (residual symptoms and residual disease of 3% afternduction). Ifosfamide and mesna were added to his induction reg-men for remission induction and were successful. One year later,e had relapse requiring COG protocol ALL101P2 and 5/10 matchederipheral blood stem cell transplant from his father. He has been
n remission for 3 years. Patient 7 was a 4-year old Hispanic maleho presented with upper respiratory infection symptoms, chestain and fever. He was treated with DFCI protocol and achievedomplete remission without relapse. He has been in remission for
years.
.3. Flow cytometry analysis
Mean fluorescence index (MFI) of CD5 expression of T lym-hoblasts in the ETP-ALL patients was lower compared to internalontrol mature T-cells (4.5–80 fold lower than controls). The con-entional T-ALL/LBL had lymphoblasts with much brighter CD5xpression compared to ETP-ALL, most having an MFI ratio of 1:1hen compared to mature T-cell controls (see Fig. 1).
.4. Laboratory parameters
In order to determine if factors other than the immunophe-otype contributed to a difference in outcomes, the followingarameters were compared between ETP-ALL and conventional T-LL/LBL groups: age, peripheral blood white cell count, and marrowlast percentage. Sixteen (39%) conventional T-ALL/LBL patientsad a white blood cell count >50 × 109/L. Only one ETP-ALL patientad a white blood cell count >50 × 109/L. For the pediatric ETP-ALLroup, 2 patients were high risk by age (<1 year or ≥10 years of age)NCI definition of high risk for pediatric ALL patients [18]). Nine-een (56%) conventional T-ALL/LBL patients belonged to the highisk age group. Additionally, 3 pediatric conventional T-ALL/LBLatients had WBC counts >50 × 109/L (high risk by WBC count perCI criteria). The p values listed in Table 1 show that the differenceetween these two groups for these parameters was not statisti-ally significant. Comparison of distributions for white blood cellounts and marrow blasts are shown in Fig. 2a and b, respectively.ig. 2c shows peripheral blood blast counts (in ×109/L) in bothroups. An age group comparison was done by separating adultsover 18) and children (18 and under). The difference in thesewo parameters between ETP-ALL and conventional T-ALL/LBL,hen stratifying by age, also was not statistically significant (see
able 3).Most of the patients in this study had leukemic phase since lym-
hoblasts comprised > 25% of the bone marrow cellularity. Fifteenonventional T-ALL/LBL patients had lymphoblastic lymphoma<25% blast involvement of the marrow). Of these, 12 were chil-
ren with the following stages at diagnosis: 5 patients were stage, 1 patient was stage II, and 6 were stage IV. All three adults hadtage III lymphoma at diagnosis as per the Ann Arbor staging sys-em [17]. All of the T-LBL patients were treated according to the ALL
B. shows CD5 expression intensity in conventional T-ALL/LBL blasts. (For interpre-tation of the references to color in this figure legend, the reader is referred to theweb version of the article.)
protocols listed above. All of the ETP-ALL patients were classifiedas acute leukemia by the standard definition.
Although it is controversial to consider T-LBL and T-ALL as thesame disease with different bone marrow infiltration, the lym-phoblastic lymphoma patients were not excluded from our study.This is because, as per the current WHO classification, the distinc-tion between these two biologically related entities is still arbitrary[1]. In addition, our statistical analysis did not find leukemia to bean independent predictor of outcomes when lymphoma cases wereexcluded (data not shown). Statistical analysis of clinical parame-ters, excluding T-LBL cases, is provided in Table 4. There was nostatistical difference between ETP-ALL patients and T-ALL patientsfor any of the parameters analyzed.
3.5. Treatment response and outcomes
42 of the 48 patients had follow-up peripheral blood counts atday 10–18, and only 18 patients had follow-up bone marrow biop-sies during this period. One of the ETP-ALL patients had residualperipheral blood blasts at this interval. This patient died dur-ing treatment. Two additional ETP-ALL patients had residual bone
marrow blasts greater than 5% at day 10–18. Of these, one hadresidual disease post induction. The same patient also relapsedone year after diagnosis and underwent a bone marrow trans-plant. The second achieved long term complete remission. Four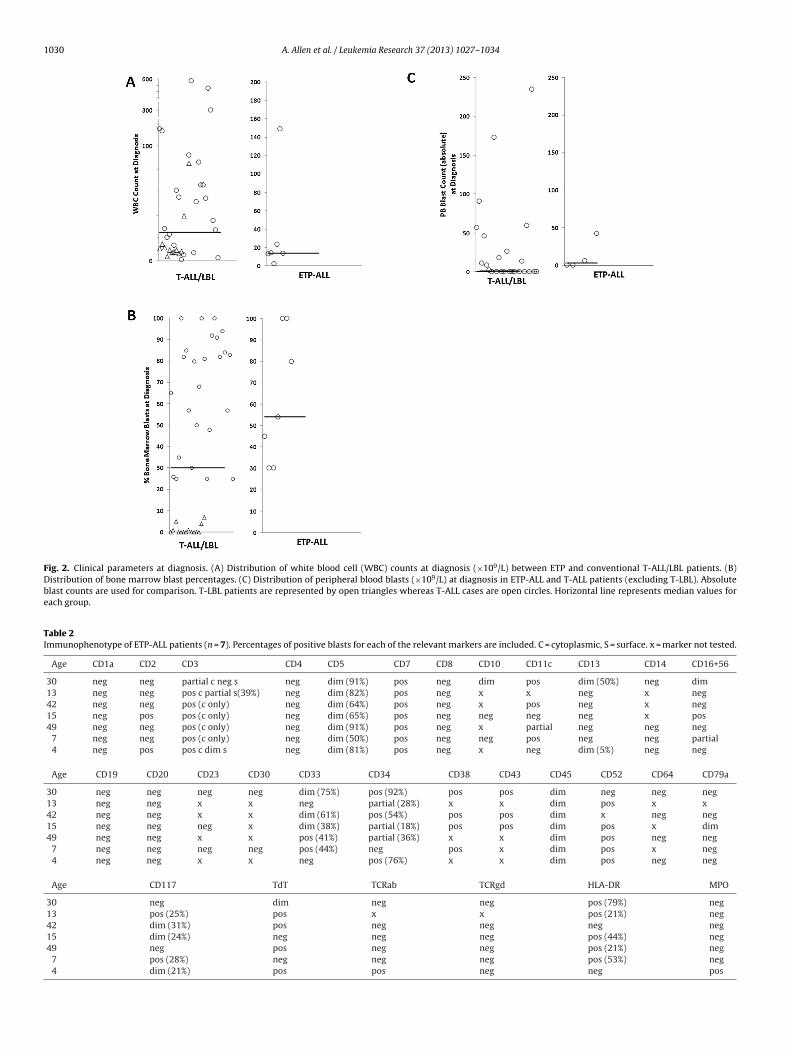
1030 A. Allen et al. / Leukemia Research 37 (2013) 1027– 1034
Fig. 2. Clinical parameters at diagnosis. (A) Distribution of white blood cell (WBC) counts at diagnosis (×109/L) between ETP and conventional T-ALL/LBL patients. (B)Distribution of bone marrow blast percentages. (C) Distribution of peripheral blood blasts (×109/L) at diagnosis in ETP-ALL and T-ALL patients (excluding T-LBL). Absoluteblast counts are used for comparison. T-LBL patients are represented by open triangles whereas T-ALL cases are open circles. Horizontal line represents median values foreach group.
Table 2Immunophenotype of ETP-ALL patients (n = 7). Percentages of positive blasts for each of the relevant markers are included. C = cytoplasmic, S = surface. x = marker not tested.
Age CD1a CD2 CD3 CD4 CD5 CD7 CD8 CD10 CD11c CD13 CD14 CD16+56
30 neg neg partial c neg s neg dim (91%) pos neg dim pos dim (50%) neg dim13 neg neg pos c partial s(39%) neg dim (82%) pos neg x x neg x neg42 neg neg pos (c only) neg dim (64%) pos neg x pos neg x neg15 neg pos pos (c only) neg dim (65%) pos neg neg neg neg x pos49 neg neg pos (c only) neg dim (91%) pos neg x partial neg neg neg
7 neg neg pos (c only) neg dim (50%) pos neg neg pos neg neg partial4 neg pos pos c dim s neg dim (81%) pos neg x neg dim (5%) neg neg
Age CD19 CD20 CD23 CD30 CD33 CD34 CD38 CD43 CD45 CD52 CD64 CD79a
30 neg neg neg neg dim (75%) pos (92%) pos pos dim neg neg neg13 neg neg x x neg partial (28%) x x dim pos x x42 neg neg x x dim (61%) pos (54%) pos pos dim x neg neg15 neg neg neg x dim (38%) partial (18%) pos pos dim pos x dim49 neg neg x x pos (41%) partial (36%) x x dim pos neg neg
7 neg neg neg neg pos (44%) neg pos x dim pos x neg4 neg neg x x neg pos (76%) x x dim pos neg neg
Age CD117 TdT TCRab TCRgd HLA-DR MPO
30 neg dim neg neg pos (79%) neg13 pos (25%) pos x x pos (21%) neg42 dim (31%) pos neg neg neg neg15 dim (24%) neg neg neg pos (44%) neg49 neg pos neg neg pos (21%) neg
7 pos (28%) neg neg neg pos (53%) neg4 dim (21%) pos pos neg neg pos

A. Allen et al. / Leukemia Research 37 (2013) 1027– 1034 1031
Table 3Age Stratification of adults (over 18) and pediatrics (18 and under). The top chart shows the comparison of outcomes between adults and pediatrics in each group. The bottomchart shows patient demographics stratified for age.
Age 18 or under ETP-ALL (n = 4) T-ALL/LBL (n = 34) p-Value
Induction failure 1 (25%) 7 (21%) 1Relapse 2 (50%) 9 (27%) 0.56Death 0 7 (21%) 0.57
Age over 18 ETP-ALL (n = 3) T-ALL/LBL (n = 7) p-Value
Induction failure 1 (33%) 0 0.3Relapse 1 (33%) 2 (29%) 1Death 1 (33%) 4 (57%) 0.99
18 or under ETP-ALL (n = 4) T-ALL/LBL (n = 34) p-Value
WBC count range 2.4–14.2 × 109/L 1.2–593.4 × 109/LWBC count mean 9.9 × 109/L 77.7 × 109/L 0.76Marrow blast mean 55% 39% 0.20Age mean 9.8 years 8.9 years 0.52Caucasians 2 (50%) 12(35%) 0.62African Americans 0 3 (9%) 1Hispanics 2 (50%) 11 (32%) 0.59Other nationality 0 8 (24%) 0.56
Over 18 ETP-ALL (n = 3) T-ALL/LBL (n = 7) p-Value
WBC count range 13.4–148.8 × 109/L 6.6–300 × 109/LWBC count mean 61.9 × 109/L 60.8 × 109/L 0.27Marrow blast mean 70.0% 38% 0.35Age mean 40 years 52 years 0.79Caucasians 0 5(71%) 0.17
(biy
TAa
African Americans 1(33%)
Hispanics 0
Other nationality 2(67%)
10%) of conventional T-ALL/LBL patients had residual peripherallood blasts between days 14 and 18. Three of these patients failed
nduction. One patient who failed induction also relapsed within 2ears of diagnosis. The other three patients with residual blasts
able 4nalysis excluding T-LBL patients. Comparison of clinical parameters previouslynalyzed between conventional T-ALL (n = 26) and ETP-ALL (n = 7) patients.
T-ALL (n = 26) ETP (n = 7) p-Value
Induction failure 6 (23%) 2 (29%) 1Relapse 9 (35%) 3 (43%) 0.69Death 7 (27%) 1 (14%) 0.65
RaceBlack 3 (12%) 1 (14%) 1Caucasian 9 (35%) 2 (29%) 1Hispanic 7 (27%) 2 (29%) 1Other 7 (27%) 2 (29%) 1
Residual disease>5% 5 (19%) 1 (14%) 1<5% 1 (4%) 1(14%) 0.38
Age<1 1 (4%) 0% 11- < 10 9 (35%) 2 (29%) 110–18 13 (50%) 2 (29%) 0.41>18 3 (12%) 3 (43%) 0.09
Mean 14.2 22.9 1
WBC>50 15 (58%) 1 (14%) 0.09<50 11 (42%) 6 (86%) 0.09Range 1.2–593.4 × 109̂/L 2.4–148.8 × 109/LMean 105.8 × 109/L 35.8 × 109/L 1
Pediatric 23 (88%) 4 (57%) 0.09High risk 18 (69%) 2 (29%) 0.17
Mediastinal mass 13 (50%) 1 (14%) 0.20Marrow blast mean 67% 63% 1Peripheral blast mean 30.9 × 109/L 12.0 × 109/L 1
0 0.30 12(29%) 0.5
achieved long term complete remission. No additional conven-tional T-ALL/LBL patients had residual disease during this interval.
Nine (19%) patients had induction failure, (7 conventional T-ALL/LBL and 2 ETP-ALL, p = 0.60) and 8 of these patients, including1 ETP-ALL patient, were of the pediatric age group. Three hadinduction failure with <5% lymphoblasts but with continued clin-ical disease in addition to residual lymphoblasts in the marrow.Six patients with induction failure had residual disease of greaterthan 5% lymphoblasts. This included 1 (14%) of the adult ETP-ALL patients and 5 (12.2%) of the conventional T-ALL/LBL patients(p value = 1). The conventional T-ALL/LBL patients were all chil-dren. Four of these children were high risk by age or WBC count.Three patients had residual disease <5%, including 2 conventionalT-ALL/LBL (5%) and 1 ETP-ALL (14%, p = 0.3857) patients. One of theconventional T-ALL/LBL patients in this group was high risk. Allthree of these patients were children.
Fig. 3 shows Kaplan–Meyer curves for event free survival, over-all survival and cumulative incidence of relapse. The log rank testshowed no statistically significant difference in the event free sur-vival, overall survival or cumulative incidence of relapse betweenthe ETP-ALL and conventional T-ALL/LBL groups.
The results of univariate cox regression analysis of ETP forrelapse and death are summarized in Table 5. Without stratify-ing for age, risk of relapse was 4.08 times higher in patients with
ETP-ALL relative to controls. This finding did not reach statisticalsignificance (p = 0.127). When analysis was restricted to pediatricpatients (age < 18) ETP-ALL carried a nearly 12 fold increased riskTable 5Cox Proportional Hazard Model. Univariate analysis summary for risk of relapse anddeath associated with ETP phenotype.
Relapse HR p value Death HR p value
ETP all 4.08 0.127 0.82 0.91ETP-pediatric 11.63 0.025 3.03 0.43

1032 A. Allen et al. / Leukemia Research 37 (2013) 1027– 1034
F rvival
C values
o(aohT
idhr
Fp
ig. 3. Kaplan–Meyer curves for all patients. Curves are shown for event free suonventional T-ALL/LBL (circles) is compared to ETP-ALL (squares). Log rank test p
f relapse independently. This finding was statistically significantp = 0.025). Kaplan–Meyer curves restricted to pediatric patientsre shown in Fig. 4. Also, when looking at induction failure as theutcome, ETP phenotype showed a markedly elevated risk with aazard ratio of 9.17 in all patients and 4.72 in pediatric patients.hese findings did not reach statistical significance.
When looking at death as the outcome in all patients, no
ncreased risk of death was observed for ETP-ALL patients indepen-ent of other variables (HR = 0.83, p = 0.91). In pediatric patients,owever, there were no ETP-ALL patients who died. The hazardatio for risk of death was 3.03. This finding also did not reachig. 4. Kaplan–Meyer curves in pediatric patients. Curves for event free survival (A) and
atients. Conventional T-ALL/LBL (circles) is compared to ETP-ALL (squares). Log rank tes
(A), overall survival (B), and cumulative incidence of relapse (C) for all patients. are shown.
statistical significance (p = 0.43). However, the relatively few deathevents in the pediatric subpopulation limit this portion of the anal-ysis.
3.6. Cytogenetics and PCR
Cytogenetic findings were diverse in both groups. The majority
of the patients had normal karyotypes. Two conventional T-ALL/LBLpatients had del 9(p21), 3 had abnormalities of the long arm ofchromosome 5, 2 had del 10(q24) and 2 had abnormalities involv-ing the short arm of chromosome 6. All but two of the deaths inoverall survival (B), and cumulative incidence of relapse (C) restricted to pediatrict p values are shown.

Resear
tm−3ccrT
ftcn
4
Caeaofsvsd1tfowepE
iTaatucistAlwsPenCEa
crgagl
s
A. Allen et al. / Leukemia
he conventional T-ALL/LBL group occurred in patients with nor-al cytogenetics. These final two patients were hypodiploid (45 XY and 44 XX, −1, −16, −17, −18 +mar1−4). In the ETP-ALL group,
patients had translocations or deletions involving the long arm ofhromosome 14 including one patient with t(1;14)(p32;q11.2). Oneonventional T-ALL/LBL patient had t(10;14)(q24;q11.2). No otherecurrent cytogenetic abnormalities were observed in this group.he single ETP-ALL patient who died had a normal karyotype.
PCR analysis for T-cell receptor gene rearrangement was per-ormed in 23 (56%) of the conventional T-ALL/LBL and 5 (71%) ofhe ETP-ALL patients. Nineteen (46%) conventional T-ALL/LBL hadlonal rearrangement vs. 4 (57%) of the ETP-ALL, the results wereot significantly different between the two groups (p = 1).
. Discussion
In 2009, a study at St. Jude’s children’s research hospital byoustan-Smith et al. defined a new subtype of T-ALL referred tos ETP-ALL. This new subset was defined by characteristic genexpression profile and immunophenotype i.e. lack of CD1a and CD8,nd dim expression of CD5 with expression of at least one myeloidr stem cell marker [7]. The same group provided further supportor ETP-ALL as a subtype of T-ALL by performing whole-genomeequencing in early 2012 [21]. ETP-ALL was characterized by acti-ating mutations in genes regulating cytokine receptor and RASignaling, and inactivating mutations disrupting hematopoieticevelopment and histone-modifying genes [21]. In the initial study,39 pediatric T-ALL cases, including 17 cases of ETP-ALL were iden-ified and ETP-ALL was shown to confer a higher risk of inductionailure and relapse. Other parameters studied included clearancef lymphoblasts during the first phase of induction chemotherapy,hich was worse for ETP-ALL patients and, minimal residual dis-
ase was also more common and of a higher magnitude, in ETP-ALLatients. Due to these findings, Coustan-Smith et al. concluded thatTP-ALL in pediatric patients had a worse prognosis [7].
A second study by the Tokyo children’s cancer group publishedn 2011 also looked at prognosis in pediatric ETP-ALL patients [22].heir cases were defined as ETP-ALL using a scoring system bydding points based on intensity of expression of 12 markers with
score of 7 or above indicating an ETP-ALL phenotype. In definingheir ETP-ALL, expression of CD117, CD65 or CD1a was not a req-isite, but lack of CD2, CD3, CD4, CD10 and CD56 expression wasonsidered essential. These 5 markers were not included in the def-nition of ETP-ALL in either the Coustan-Smith et al. group or in ourtudy. Furthermore, these markers are not included in the defini-ion of ETP in previous studies of T-cell development [12,13,15,16].lso of note, two patients included in the ETP-ALL arm of the study
acked flow cytometry for either CD1a or CD8. These two markersere considered part of the definition of ETP phenotype in previous
tudies [12,13,15,16] as well as the Coustan-Smith et al. study [7].atients without complete flow data for all specified markers werexcluded in our series to ensure that all patients had an ETP phe-otype. Missing data for these markers as well as non-inclusion ofD1a in their scoring system raise a question of whether or not theTP-ALL patients included in their study truly had an ETP phenotypes defined in previous studies.
The differences in age, white blood cell count, marrow blast per-entage or incidence of induction failure, cumulative incidence ofelapse or death between the ETP-ALL and conventional T-ALL/LBLroups in our series were not statistically significant. Interestingly,ll of the ETP-ALL patients in our study were in leukemic phase sug-
esting that this phenotype may be more commonly seen in acuteeukemia than lymphoblastic lymphoma.Previous studies included only pediatric patients while ourtudy included adults as well as children. We analyzed the entire
ch 37 (2013) 1027– 1034 1033
group and the adult and pediatric groups separately to determinepossible reasons for the discrepant results compared to prior stud-ies. When only pediatric cases were analyzed in our cohort, theincidence of induction failure and death between ETP-ALL andconventional T-ALL/LBL patients were observed and were not sta-tistically significant. Similar results were obtained on analyzingadult patients. White blood cell counts in pediatric cases werealso compared and no statistical difference was observed. In thepediatric group, we found an 11.63 fold increased risk of relapsefor ETP-ALL patients. This is consistent with both of the previousstudies, which found increased risk of relapse in pediatric patients[7,22]. Caucasian race was found to be a protective factor for riskof relapse in pediatric patients in our study (HR = 0.33, data notshown). Coustan-Smith et al. also found a similar hazard ratio asso-ciated with ETP status and ethnicity [7].
ETP status in our study was not an independent predictor ofdeath in any age group. The low incidence of death overall, includ-ing 0 deaths in the pediatric ETP-ALL group, in our cohort limits thisanalysis. We found that the effect of ETP phenotype was more pro-nounced in the younger age group with a higher hazard ratio in thepediatric group alone compared to the combined group of pediatricand adult patients. Because age is an established risk factor in ALL[18,23], older age may mask the effects of ETP phenotype when allpatients are analyzed.
In the previous studies as well as this study, patients weretreated with various combinations of the following chemother-apeutic agents: daunorubicin, vincristine, methotrexate, pred-nisone, l-asparaginase, etopside, cytarabine and 6-mercaptopurine[2–4,24,25]. However, the St. Jude cohort was treated according tothe Total Therapy Study XIIIB protocol [26]. None of our patientswere treated with this protocol. Additionally, the Japanese groupused another, uniquely designed protocol not adopted at our insti-tution [22]. It was our aim to see if ETP phenotype still resulted inworse outcomes under standard treatment protocols used at our,and many other institutions. The use of multiple treatment regi-mens at our institution could potentially account for differencesin outcome with regard to death and induction failure. However,it should be noted, that both ETP-ALL and conventional T-ALL/LBLpatients in our study, were treated according to standard, high riskALL protocols with no unique therapies used in treatment of eithergroup based on their immunophenotype. In our study, the overallincidence of either induction failure or relapse (combined) in con-ventional T-ALL/LBL patients was 45% vs. 57% in ETP-ALL patients,compared to 18% vs. 53% respectively in the study of Coustan-Smith et al. [7]. This may indicate that the treatment used at St.Jude may accentuate differences in this outcome between the twogroups. While the treatment protocols used in our institution arefrequently used for T-ALL, their use may not bring about completeremission at end induction as well as the study protocols used inprevious studies and therefore may mask differences between ETP-ALL and conventional T-ALL/LBL in our population with regard toinitial induction failure.
Coustan-Smith et al. found del 13q in 8 patients (4 ETP-ALLand 4 conventional T-ALL) [7]. We did not detect abnormalitiesof chromosome 13 in any of our cases. In addition, in the studyof Coustan-Smith et al., 4 ETP-ALL patients had del 5q [7]. Wedetected del 5q only in 2 of our conventional T-ALL/LBL patients.This abnormality is known to be a recurrent cytogenetic aberrationin T-ALL [27] and was not found in our ETP-ALL patients. As previ-ously stated, several of our cases had abnormalities of the long armof chromosome 14 in the region of the TCR alpha–delta receptorgene located at 14q11. Certain translocations involving chromo-
some 14q11 are associated with a favorable prognosis [10]. Suchtranslocations were found in two of our patients (see above). It isunlikely the differences in cytogenetic abnormalities accounted fordifferences between our and prior studies.
1 Resear
pwSfnppp1esbisi
C
A
dfAit
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
2011;29:386–91.
034 A. Allen et al. / Leukemia
The number of patients in our study is smaller compared to therevious studies. However, this is a rare subtype of ALL. Despite this,e found a similar incidence of ETP phenotype compared with the
t. Jude study [7]. Differences in patient ethnicity may also accountor differences in outcome as the majority of our patients wereon-Caucasian while Coustan-Smith et al. had mainly Caucasianatients and the Tokyo Children’s group of Inukai et al. was com-osed entirely of Asian (Japanese) patients. Overall, our and therior two studies detected relatively few ETP-ALL patients (5.5%,2.5% and 14.5% of study populations in Inukai et al., Coustan-Smitht al. and our group, respectively). While ours and the prior twotudies had similar findings with regard to disease relapse, it maye that larger patient populations are needed to determine the true
nfluence of the ETP phenotype on overall survival. Additional largertudies are necessary to elucidate the impact of the ETP phenotypen both adult and pediatric patients with T-ALL/LBL.
onflict of interest statement
The authors have nothing to disclose.
cknowledgements
None. No funding to declare.Contributions. All authors contributed to the paper and study
esign. AA collected the case information wrote the paper. AS per-ormed the statistical analysis and wrote the statistical methods.C, GB and BA performed the analysis of histomorphology and
nterpretation of flow cytometry data. AA, KP and MS interpretedhe clinical data.
eferences
[1] Swerdlow SH, Jaffe ES, International Agency for Research on Cancer, WorldHealth Organization. WHO classification of tumours of haematopoietic andlymphoid tissues. Lyon: International Agency for Research on Cancer; 2008.
[2] Goldberg JM, Silverman LB, Levy DE, Dalton VK, Gelber RD, Lehmann L,et al. Childhood T-cell acute lymphoblastic leukemia: the Dana-Farber CancerInstitute acute lymphoblastic leukemia consortium experience. J Clin Oncol2003;21:3616–22.
[3] Hoelzer D, Gokbuget N, Digel W, Faak T, Kneba M, Reutzel R, et al. Outcome ofadult patients with T-lymphoblastic lymphoma treated according to protocolsfor acute lymphoblastic leukemia. Blood 2002;99:4379–85.
[4] LeClerc JM, Billett AL, Gelber RD, Dalton V, Tarbell N, Lipton JM, et al. Treat-ment of childhood acute lymphoblastic leukemia: results of Dana-Farber ALLConsortium Protocol 87-01. J Clin Oncol 2002;20:237–46.
[5] Marks DI, Paietta EM, Moorman AV, Richards SM, Buck G, DeWald G, et al. T-cell
acute lymphoblastic leukemia in adults: clinical features, immunophenotype,cytogenetics, and outcome from the large randomized prospective trial (UKALLXII/ECOG 2993). Blood 2009;114:5136–45.[6] Baldus CD, Burmeister T, Martus P, Schwartz S, Gokbuget N, Bloomfield CD,et al. High expression of the ETS transcription factor ERG predicts adverse
[
ch 37 (2013) 1027– 1034
outcome in acute T-lymphoblastic leukemia in adults. J Clin Oncol 2006;24:4714–20.
[7] Coustan-Smith E, Mullighan CG, Onciu M, Behm FG, Raimondi SC, Pei D, et al.Early T-cell precursor leukaemia: a subtype of very high-risk acute lymphoblas-tic leukaemia. Lancet Oncol 2009;10:147–56.
[8] Lin C, Zheng H, Wang C, Yang L, Chen S, Li B, et al. Mutations increased over-expression of Notch1 in T-cell acute lymphoblastic leukemia. Cancer Cell Int2012;12:13.
[9] Van Vlierberghe P, Ambesi-Impiombato A, Perez-Garcia A, Haydu JE, Rigo I,Hadler M, et al. ETV6 mutations in early immature human T cell leukemias. JExp Med 2011;208:2571–9.
10] Graux C. Biology of acute lymphoblastic leukemia (ALL): clinical and therapeu-tic relevance. Transfus Apher Sci 2011;44:183–9.
11] Berquam-Vrieze KE, Nannapaneni K, Brett BT, Holmfeldt L, Ma J, Zagorodna O,et al. Cell of origin strongly influences genetic selection in a mouse model ofT-ALL. Blood 2011;118:4646–56.
12] Bell JJ, Bhandoola A. The earliest thymic progenitors for T cells possess myeloidlineage potential. Nature 2008;452:764–7.
13] Chi AW, Bell JJ, Zlotoff DA, Bhandoola A. Untangling the T branch of thehematopoiesis tree. Curr Opin Immunol 2009;21:121–6.
14] Rothenberg EV, Moore JE, Yui MA. Launching the T-cell-lineage developmentalprogramme. Nat Rev Immunol 2008;8:9–21.
15] Shortman K, Wu L, Early T. lymphocyte progenitors. Annu Rev Immunol1996;14:29–47.
16] Wada H, Masuda K, Satoh R, Kakugawa K, Ikawa T, Katsura Y, et al. Adult T-cellprogenitors retain myeloid potential. Nature 2008;452:768–72.
17] American Joint Committee on Cancer, Edge SB. AJCC Cancer Staging Manual.7th ed. New York/London: Springer; 2010.
18] Smith M, Arthur D, Camitta B, Carroll AJ, Crist W, Gaynon P, et al. Uniformapproach to risk classification and treatment assignment for children withacute lymphoblastic leukemia. J Clin Oncol 1996;14:18–24.
19] Sevilla DW, Emmons FN, Colovai AI, Beaubier NT, Baker C, Bhatia M, et al.Hematogones are markedly reduced in pediatric acquired aplastic anemia:multiparametric flow cytometric analysis. Leuk Lymphoma 2009;50:1951–7.
20] Shaffer LG, Slovak ML, Campbell LJ. ISCN 2009: An International System forHuman Cytogenetic Nomenclature. Vancouver, B.C.: Karger; 2009.
21] Zhang J, Ding L, Holmfeldt L, Wu G, Heatley SL, Payne-Turner D, et al. Thegenetic basis of early T-cell precursor acute lymphoblastic leukaemia. Nature2012;481:157–63.
22] Inukai T, Kiyokawa N, Campana D, Coustan-Smith E, Kikuchi A, KobayashiM, et al. Clinical significance of early T-cell precursor acute lymphoblasticleukaemia: results of the Tokyo Children’s Cancer Study Group Study L99-15.Br J Haematol 2012;156:358–65.
23] Shuster JJ, Falletta JM, Pullen DJ, Crist WM, Humphrey GB, Dowell BL, et al.Prognostic factors in childhood T-cell acute lymphoblastic leukemia: a PediatricOncology Group study. Blood 1990;75:166–73.
24] Liang DC, Yang CP, Lin DT, Hung IJ, Lin KH, Chen JS, et al. Long-term results ofTaiwan Pediatric Oncology Group studies 1997 and 2002 for childhood acutelymphoblastic leukemia. Leukemia 2010;24:397–405.
25] Stock W, La M, Sanford B, Bloomfield CD, Vardiman JW, Gaynon P, et al. Whatdetermines the outcomes for adolescents and young adults with acute lym-phoblastic leukemia treated on cooperative group protocols? A comparisonof Children’s Cancer Group and Cancer and Leukemia Group B studies. Blood2008;112:1646–54.
26] Pui CH, Pei D, Campana D, Bowman WP, Sandlund JT, Kaste SC, et al. Improvedprognosis for older adolescents with acute lymphoblastic leukemia. J Clin Oncol
27] Schneider NR, Carroll AJ, Shuster JJ, Pullen DJ, Link MP, Borowitz MJ, et al. Newrecurring cytogenetic abnormalities and association of blast cell karyotypeswith prognosis in childhood T-cell acute lymphoblastic leukemia: a pediatriconcology group report of 343 cases. Blood 2000;96:2543–9.





























