Embed Size (px)
Citation preview

gpge
Operative Techniques in Otolaryngology (2012) 23, 275-281
Dynamic reconstruction of the paralyzed face, part II:Extensor digitorum brevis, serratus anterior, andanterolateral thigh
Kristoffer B. Sugg, MD,a Jennifer C. Kim, MDb
From the aSection of Plastic and Reconstructive Surgery, Department of Surgery, University of Michigan Health System,Ann Arbor, Michigan; and
bDepartment of Otolaryngology, University of Michigan Health System, Ann Arbor, Michigan.Rehabilitation of the paralyzed face requires consideration of the functional, esthetic, and psychologicalconcerns of the afflicted patient. Lack of spontaneous facial animation significantly impairs the capacityto interact socially and convey emotion. With the advent of microneurovascular free tissue transfer, anew era of dynamic reconstruction was introduced, and symmetry with movement became a clinicalreality. Although the gracilis is highly touted as the workhorse flap in facial reanimation surgery, abetter understanding of flap physiology and neurovascular anatomy has contributed to the increasedversatility in flap design while minimizing donor site morbidity. The purpose of this manuscript is toexplore alternative donor muscle groups used in the surgical management of chronic facial paralysis anddescribe their operative technique, namely, the extensor digitorum brevis, serratus anterior, andanterolateral thigh flaps.© 2012 Published by Elsevier Inc.
KEYWORDS:Facial reanimation;Facial paralysisreconstruction;Neuromuscular freeflap
The face is the medium through which we express our-selves. It imparts emotion by providing visual cues in theform of spontaneous coordinated movement of the mimeticmusculature. When efferent signals traveling within thefacial nerve are lost due to injury or disease, facial harmonyis disrupted and detrimental effects on communication areobserved.1 Concurrent with the development of microsur-ical techniques, a dynamic approach to rehabilitation of thearalyzed face began in 1976 with the introduction of theracilis as the first free muscle transfer performed by Hariit al.2 Since then, numerous flaps have been described, but
the primary goals of facial reanimation surgery have notchanged: corneal protection, facial symmetry at rest, andrestoration of smile.
The surgical management of chronic facial paralysis isno different from any other peripheral nerve injury. An
Address reprint requests and correspondence: Jennifer C. Kim,MD, Department of Otolaryngology, University of Michigan, 1904 Taub-man Center, 1500 East Medical Center Drive, Ann Arbor, MI 48109-5312.
E-mail address: [email protected].
1043-1810/$ -see front matter © 2012 Published by Elsevier Inc.http://dx.doi.org/10.1016/j.otot.2012.11.002
exhaustive history can often discern the underlying cause,with most cases being idiopathic.3 It is important to deter-mine the amount of time elapsed since the onset of paraly-sis, as this will directly influence the treatment algorithm:nerve transfer alone through cross-facial nerve grafting(CFNG) for denervation time of �6 months, CFNG with“babysitter” procedure (minihypoglossal transfer) for dener-vation time between 6 and 18 months, or CFNG in combi-nation with free muscle transfer for denervation time of�18 months.4,5 Residual function of the facial nerve shouldbe clearly documented as well as the presence of additionalcranial nerve deficits, to aid in the selection of the mostappropriate donor nerve for reinnervation of the free muscletransfer. Ancillary studies can sometimes be helpful in pro-viding electrophysiological data for prognostication, but areof limited value in patients with long-standing paralysis dueto neurogenic atrophy of the underlying mimetic muscula-ture.
Once the patient is deemed an appropriate surgical can-
didate, a multitude of factors contribute to the choice of the
abmttswpilc
paf
amprvu
276 Operative Techniques in Otolaryngology, Vol 23, No 4, December 2012
optimal donor muscle group, including muscle excursionand bulk, number of required independent force vectors,donor site morbidity, comfort level of the clinician with thetechnical aspects related to flap harvest, and patient prefer-ences. Part I of this manuscript series described the latissi-mus dorsi, rectus abdominis, and pectoralis minor as someof the less common flaps used in facial reanimation surgerytoday. Building on this previous work, a new set of alter-native donor muscle groups are spotlighted in the followingtext to further broaden the reconstructive landscape andreplenish the facial reconstructive surgeon’s armamentar-ium, namely, the extensor digitorum brevis (EDB), serratusanterior (SA), and anterolateral thigh (ALT) flaps.
Operative technique
Extensor digitorum brevis
The EDB is a trapezoid-shaped muscle whose primaryfunction is to assist the extensor digitorum longus (EDL) inextension of the second through fourth toes. Because bothmuscles are synergistic in action, harvesting the EDB forfacial reanimation surgery produces little to no functionaldeficit at the donor site.6,7 It originates from the dorsolateralspect of the calcaneus immediately anterior to the peroneusrevis tendon, and then courses obliquely from lateral toedial across the dorsum of the foot deep to the EDL
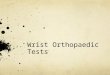
endons. The muscle is of modest bulk and terminates as 4endons, with the lateral 3 tendons inserting into the lateralide of the corresponding EDL tendon of the central 3 toes,hereas the most medial tendon inserts onto the base of theroximal phalanx of the hallux (Figure 1). This medial slips often referred to as the extensor hallucis brevis, but theiterature is inconsistent as to whether an independent mus-le belly truly exists.8-10
According to the Mathes–Nahai classification scheme,the EDB is considered a type II muscle flap with the lateraltarsal artery, a direct branch from the dorsalis pedis artery,being the dominant blood supply.6,8,9,11,12 Additional minoredicles include smaller branches from the dorsalis pedisrtery supplying the lateral surface and perforating branchesrom the peroneal artery supplying the deep surface.6,13,14
The EDB receives its innervation from the lateral terminalbranch of the deep peroneal nerve, which enters the muscleon its deep surface in close proximity to the lateral tarsalartery and its accompanying venae comitantes.6 Advantagesof the EDB for dynamic reconstruction of the paralyzed faceinclude a predictable and constant blood supply with similarmuscle bulk to the facial muscles, and whose tendinousstructures facilitate the fixation and function of the musclestrips. Furthermore, the EDB entails a straightforward flapdissection, minimal donor site morbidity, multiple indepen-dent force vectors, and it can be used in both single- anddouble-stage procedures. However, the disadvantages aresacrifice of the dorsalis pedis artery and smaller size com-
pared with other donor muscle groups.As part of the preoperative planning, a complete vascularexamination must be performed of the lower extremity andfoot to identify any potential inflow problems. Peripheralvascular occlusive disease is an absolute contraindication tothe use of the EDB in this clinical context, as the dorsalispedis artery may represent the only source of blood supplyto the remaining foot. In addition, although calcification ofthe tunica media often contributes to technical difficultiesduring microvascular anastomosis, narrowing of the vessellumen due to atherosclerotic-induced intimal thickening isthought to increase the rate of reconstructive failures in thehead and neck region.15-18 Although this literature primarilyddresses oncological defects in an older population whereicroneurovascular free tissue transfer for chronic facial
aralysis is less likely to be performed, it is important toemember that congenital aberrations of the lower-extremityasculature may exist such as the peronea arteria magna inp to 5.3% of patients.19 Therefore, any suspicion of com-
promised arterial patency of the lower extremity or footwarrants further investigation with either ankle–brachialindexes or computed tomography angiogram as indicated.
The contralateral foot is often used in relation to theaffected side of the face due to the medial to lateral trajec-
Figure 1 On the dorsal surface of the midfoot, the extensordigitorum brevis (EDB) is located deep to the tendons of theextensor digitorum longus (EDL). The lateral 3 tendons of theEDB insert onto the lateral side of the corresponding EDL tendonsof the central three toes, whereas the most medial tendon insertsonto the base of the proximal phalanx of the hallux. The EDB issupplied by the lateral tarsal artery and the lateral terminal branchof the deep peroneal nerve, which both enter the muscle belly onthe medial aspect of its deep surface.
tory of EDB’s neurovascular pedicle. This will facilitate

bitnttmmvl
277Sugg and Kim Dynamic Reconstruction of the Paralyzed Face, Part II
insetting of the flap because the vessels will be optimallypositioned for microvascular anastomosis in the neck.Given the relatively bloodless operative field, a pneumatictourniquet is not required, which also helps limit the isch-emic insult to the flap before pedicle division. With thepatient in the supine position, a gentle curvilinear incision isdesigned on the dorsum of the foot extending from thelateral malleolus to the first webspace following the obliquecourse of EDB’s muscle belly (Figure 2). This incisionalpattern will protect against contracture formation by avoid-ing a longitudinal incision that crosses the ankle joint at aperpendicular angle. The lateral tarsal artery is first identi-fied in the interval between the EDL and extensor hallucislongus tendons, distal to the inferior edge of the extensorretinaculum. The lateral terminal branch of the deep per-oneal nerve is also found in this location running parallel tothe lateral tarsal artery. Both the artery and nerve courseinferolaterally for approximately 2 cm before entering theunderside of the proximal EDB.6 A plane is then developedetween the superficial surface of the EDB and the overly-ng EDL tendons proceeding from medial to lateral. Care isaken to protect the branches of the superficial peronealerve to prevent postoperative numbness on the dorsum ofhe foot. Next, the EDB tendons are transected distally andhe muscle belly is dissected off the tarsal bones of theidfoot while clipping the smaller feeding vessels. After theuscle’s origin is released from the calcaneus, the neuro-
ascular pedicle can be mobilized proximally, aided byigation of a fairly constant branch to the sinus tarsi.8 If
additional length is required, the dorsalis pedis artery canalso be ligated distal to the takeoff of the lateral tarsal artery.
Figure 2 A typical incisional pattern used to harvest the EDBextending from the lateral malleolus to the first webspace followijoint to prevent postoperative contracture formation.
After pedicle division, the surgical site is reapproximated in
layers, and a closed-suction drain is not routinely required.The patient can bear weight as tolerated but may benefitfrom a short posterior boot splint for a few days until theinitial swelling has resolved.
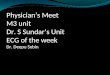
For inset of the flap, the proximal insertion is fixated tothe deep temporalis fascia. Distally, the tendinous insertionsare secured to the nasal alar base, the upper lip just medialto the nasolabial fold, the modiolus, and to the midline ofthe lower lip at the labiomental crease (Figure 3). This canall be accomplished through a modified post-tragal faceliftincision and a counter labiomental incision, with the latterbeing well camouflaged in a natural skin crease.
Serratus anterior
The SA is a fan-shaped muscle consisting of 9 or 10independent slips originating from the upper 8 or 9 ribs.20-22
There is often 1 more slip than rib because 2 slips usuallyarise from the second rib. Each slip’s origin is locatedmedial to the anterior axillary line, but lateral to the nipple,and all slips insert onto the ventral surface of the scapula’smedial border, forming the medial boundary of the axillaryspace.23,24 The primary function of the SA is to stabilize thescapula against the chest wall together with the rhomboids,such that the lower one-third of the muscle can then rotatethe scapula forward and laterally, allowing arm elevationabove the shoulder.23,25,26 Three or 4 of the most inferiorslips can be harvested for functional muscle transfer withoutcausing winging of the scapula.21,23,27
According to the Mathes–Nahai classification scheme,the SA is considered a type III muscle flap with 2 dominant
entle curvilinear incision is designed on the dorsum of the footoblique course of EDB’s muscle belly. Avoid crossing the ankle
. A gng the
blood supplies: the lateral thoracic artery supplies the upper

pfirdanAwnsmo
eubseosia
tmolatnpmtapra
ottl
ai
pdc
278 Operative Techniques in Otolaryngology, Vol 23, No 4, December 2012
two-thirds, whereas the subscapular system through theserratus branch of the thoracodorsal artery supplies thelower one-third.27-29 The posterior entry of the vascularedicle allows separation of the slips anteriorly to fill de-ects such as the eyelids and lips. The SA receives itsnnervation from the long thoracic nerve, which arises fromoots C5-7 of the brachial plexus. Advantages of the SA forynamic reconstruction of the paralyzed face include a longnd consistent pedicle, ease of flap harvest, acceptable do-or site morbidity, and multiple independent force vectors.lthough the SA provides thin pliable slips of muscle,hich is ideal for patients who require minimal bulk, it mayot provide enough volumetric fill in patients with largeoft-tissue defects. Another disadvantage of the SA is that itust be harvested from the lateral decubitus position, which
ften requires an intraoperative position change.During the preoperative workup, a detailed neurological
xamination of the upper extremity and hand must be doc-mented, with special emphasis on the upper roots of therachial plexus. This is systematically performed by testinghoulder abduction (C5), elbow flexion (C6), and elbowxtension (C7). Medial scapular winging is a rare disorderf neuromuscular imbalance, which can sometimes be vi-ualized at rest while viewing the patient from behind, butt usually becomes evident when the patient pushes againststationary object.30 It is important to remember that mild
Figure 3 The flap is inset using a modified post-tragal faceliftincision and a counter labiomental incision. The proximal flap isfixated to the deep temporalis fascia. The distal tendinous inser-tions are secured to the nasal alar base, the upper lip just medial tothe nasolabial fold, the modiolus, and to the midline of the lowerlip at the labiomental crease. The transferred muscle should beoriented along the vector of the zygomaticus major. Microneuro-vascular anastomosis is performed to recipient vasculature in theneck and to the clinician’s choice of donor nerve.
scapular winging can be a relatively common finding in the a
general population, and it does not necessarily indicate along thoracic nerve palsy is present. In these situations, SAweakness is more readily detected by lack of forward andlateral rotation of the scapular tip with arm elevation.
Similar to the EDB, the contralateral SA is often used inrelation to the affected side of the face due to the cranial tocaudal trajectory of its neurovascular pedicle. With thepatient in the lateral decubitus position, the upper extremityis left undraped to facilitate exposure of the operative field.A longitudinal incision is designed parallel to the anteriorborder of the latissimus dorsi, extending from the axilla tothe ninth rib (Figure 4). Every attempt should be made toavoid placement of the incision within the hair-bearing skinof the axilla, to prevent unsightly distortion of the hairfollicles postoperatively. Once the clavipectoral fascia isdivided, both the axillary contents and latissimus dorsi areretracted posteriorly, exposing the SA along the chest wall.The long thoracic nerve is easily visualized on the surface ofthe muscle beneath the investing fascia descending alongthe junction of the middle and posterior thirds. It joins theserratus branch of the thoracodorsal artery at approximatelythe level of the fifth rib,23,28 where it divides into 2 fascicleshat can be teased apart from the proximal trunk under loupeagnification, to both isolate the separate axial innervation
f the most inferior 3 or 4 slips and to provide additionalength if required.31 The slips of interest are then exposedlong their entire length, and a tunnel is developed beneathhe posterior third using blunt dissection. To protect theeurovascular pedicle from iatrogenic injury, 2 fingers arelaced into the tunnel and the muscle is released from theedial border of the scapula using electrocautery. Finally,
he slips are dissected off their respective ribs toward thenterior axillary line while making sure not to enter theleural space. After pedicle division, the surgical site iseapproximated in layers, and a closed-suction drain is usedt the discretion of the clinician.
For inset of the flap, the plan is analogous to the previ-usly described inset for the EDB. Proximal fixation is tohe deep temporalis fascia and individual slips are securedo the nasal alar base, upper lip, modiolus, and midlineower lip (Figure 3).
Anterolateral thigh
The ALT flap is not a muscle flap, it is a fasciocutaneousflap based on 1-3 septocutaneous or musculocutaneous per-forators from the descending branch of the lateral circum-flex femoral artery.32 It was initially described by Song etl33 in 1984, and has since become widely popularized forts role in head and neck reconstruction.34-37 Owing to its
lack of functional muscle, it cannot be used alone to restoremotion to the paralyzed face, unless combined with anotherdynamic procedure, including any iteration of the tempora-lis tendon transfer.38-40 However, Iida et al41 recently re-orted the functional reconstruction of full-thickness ab-ominal wall defects in 2 patients using a free ALT flapombined with innervated vastus lateralis. These findings
re promising for the potential application of a similar
ibsmi
rmlu
279Sugg and Kim Dynamic Reconstruction of the Paralyzed Face, Part II
conjoint flap design in facial reanimation surgery, in whichthe typical ALT flap is transformed into a dynamic proce-dure. The inclusion of a cuff of vastus lateralis with the ALTflap is already a common practice to augment soft-tissuebulk,42-45 and although Yang et al46 and others47-49 havepreviously described the rectus femoris and short head ofthe biceps femoris as alternative donor muscle groupswithin the thigh, no report documenting the use of inner-vated vastus lateralis in facial reanimation surgery currentlyexists in the literature. Combined ALT flap-reinnervatedrectus femoris or sartorius muscle flaps have been used fordynamic reconstruction.48 Advantages of the ALT flap in-clude a long pedicle, versatility in flap design, large soft-tissue yield, ability to be sensate or raised as a compositeflap, and minimal donor site morbidity.37,44,50,51 However,the disadvantages are inconsistent flap thickness and vari-able perforator route and location.32,52
The benefits of preoperative computed tomography an-giogram in mapping the perforators of the ALT flap havebeen well established,53-58 but we do not routinely used thismaging modality unless vastus lateralis is not expected toe included in the flap harvest, because it then aids in theelection of the largest perforators with favorable courses toinimize tedious intramuscular dissection. With the patient
Figure 4 The long thoracic nerve descends along the superficiaposterior thirds. It is joined by the serratus branch of the thoracostructures provide separate axial innervation to the most inferior 3incision extends from the axilla to the ninth rib. Avoid placementthe hair follicles postoperatively.
n the supine position, a line is drawn from the anterosupe-
ior iliac spine to the lateral patella representing the inter-uscular septum between the rectus femoris and vastus
ateralis. Using Doppler examination, 1-3 perforators aresually found within the middle third.32 A skin paddle is then
designed overlying these perforators with its long axis orientedparallel to the line, and based on the predetermined need forsoft-tissue bulk, the size of the flap is adjusted accordingly.However, if skin is not required in the final reconstruction, theflap can be de-epithelialized and buried. It is important to limitthe width of the flap to approximately 8 cm to avoid the needfor skin grafting at the donor site.59,60
The anterior incision is made first, and the flap is ele-vated in a subfascial plane off the rectus femoris, preservingall vessels near or at the intermuscular septum. The rectusfemoris is then retracted medially exposing the descendingbranch of the lateral circumflex femoral artery and its asso-ciated perforators. There is often a proximal perforator foundin close proximity to the terminal insertion of the tensor fasciaelatae and more distal perforators traveling through the sub-stance of the vastus lateralis.61 Once the posterior portion ofthe flap is elevated, the clinician is now ready for perforatordissection. The choice of perforator will depend on size andavailability as well as the type of flap to be elevated. If only afasciocutaneous flap is required as a soft-tissue adjunct, then
ce of the serratus anterior (SA) at the junction of the middle andartery at approximately the level of the fifth rib. Together these
slips. A, A typical incisional pattern used to harvest the SA. Thescar within the hair-bearing skin to prevent unsightly distortion of
l surfadorsal
or 4of the
the proximal perforator is preferred owing to its superficial

pd
280 Operative Techniques in Otolaryngology, Vol 23, No 4, December 2012
course and easier dissection, but the inclusion of a cuff ofvastus lateralis necessitates use of the more distal perforators.If functional muscle is desired, the motor nerve to the vastuslateralis is preserved within the flap, and is most often foundmedial and deep to the descending branch of the lateral cir-cumflex femoral artery within the intermuscular septum.62,63
The neurovascular pedicle is dissected proximally to the levelof the branch to the rectus femoris, and the lateral cutaneousfemoral nerve can also be included within the flap to providesensation.64 After pedicle division, the surgical site is reap-roximated in layers, and a closed-suction drain is used at theiscretion of the clinician.
Conclusions
Although much attention has been given to the search for anideal donor muscle group over the past few decades, theantiquated notion of “one flap fits all” in facial reanimationsurgery is impractical. A detailed understanding of neuro-vascular anatomy has expanded the reconstructive possibil-ities, enabling the clinician to choose from a collection ofdonor sites to precisely tailor the flap to the specific needs ofthe patient. The EDB, SA, and ALT flaps are less commonlyused but represent innovative surgical solutions that sharethe primary goal of ameliorating the inanimate stigmata ofthe paralyzed face.
References
1. Coulson SE, O’Dwyer NJ, Adams RD, et al: Expression of emotionand quality of life after facial nerve paralysis. Otol Neurotol 25:1014-1019, 2004
2. Harii K, Ohmori K, Torii S: Free gracilis muscle transplantation, withmicroneurovascular anastomoses for the treatment of facial paralysis.A preliminary report. Plast Reconstr Surg 57:133-143, 1976
3. Fattah A, Borschel GH, Manktelow RT, et al: Facial palsy and recon-struction. Plast Reconstr Surg 129:340e-352e, 2012
4. Terzis JK, Konofaos P: Nerve transfers in facial palsy. Facial PlastSurg 24:177-193, 2008
5. Terzis JK: Babysitters. An exciting new concept in facial reanimation,in: Proceedings of the 6th International Symposium on the FacialNerve, Rio de Janeiro, Brazil, 1988
6. Alagöz MS, Alagöz AN, Comert A: Neuroanatomy of extensor digi-torum brevis muscle for reanimation of facial paralysis. J CraniofacSurg 22:2308-2311, 2011
7. Pai CH, Lin GT, Lin SY, et al: Extensor digitorum brevis rotationalmuscle flap for lower leg and ankle coverage. J Trauma 49:1012-1016,2000
8. del Piñal F, Herrero F: Extensor digitorum brevis free flap: anatomicstudy and further clinical applications. Plast Reconstr Surg 105:1347-1356, 2000
9. Baltensperger MM, Ganzoni N, Jirecek V, et al: The extensor digito-rum brevis island flap: possible applications based on anatomy. PlastReconstr Surg 101:107-113, 1998
10. Crocker AD, Moss AL: The extensor hallucis brevis muscle flap.J Bone Joint Surg Br 71:532, 1989
11. Gahhos FN, Jaquith M, Hidalgo R: The extended digitorum brevismuscle flap. Ann Plast Surg 23:255-262, 1989
12. Giordano PA, Argenson C, Pequignot JP: Extensor digitorum brevis asan island flap in the reconstruction of soft-tissue defects in the lower
limb. Plast Reconstr Surg 83:100-109, 198913. Landi A, Soragni O, Monteleone M: The extensor digitorum brevismuscle island flap for soft-tissue loss around the ankle. Plast ReconstrSurg 75:892-897, 1985
14. Man D, Acland RD: The microarterial anatomy of the dorsalis pedisflap and its clinical applications. Plast Reconstr Surg 65:419-423, 1980
15. le Nobel GJ, Higgins KM, Enepekides DJ: Predictors of complicationsof free flap reconstruction in head and neck surgery: analysis of 304free flap reconstruction procedures. Laryngoscope 122:1014-1019,2012
16. de Bree R, Quak JJ, Kummer JA, et al: Severe atherosclerosis of theradial artery in a free radial forearm flap precluding its use. Oral Oncol40:99-102, 2004
17. Alberdas JL, Shibahara T, Noma H: Histopathologic damage to vesselsin head and neck microsurgery. J Oral Maxillofac Surg 61:191-196,2003
18. Serletti JM, Higgins JP, Moran S, et al: Factors affecting outcome infree-tissue transfer in the elderly. Plast Reconstr Surg 106:66-70, 2000
19. Rosson GD, Singh NK: Devascularizing complications of free fibularharvest: Peronea arteria magna. J Reconstr Microsurg 21:533-538,2005
20. Takayanagi S, Ohtsuka M, Tsukie T: Use of the latissimus dorsi andthe serratus anterior muscles as a combined flap. Ann Plast Surg20:333-339, 1988
21. Takayanagi S, Tsukie T: Free serratus anterior muscle and myocuta-neous flaps. Ann Plast Surg 8:277-283, 1982
22. Buncke HJ, Alpert BS, Gordon L: Microvascular serratus anteriortransplantation, in Proceedings of the 51st Annual Convention of theAmerican Society of Plastic and Reconstructive Surgeons. Honolulu,HI, Plastic Surgery Education Foundation, and American Society ofMaxillofacial Surgeons, 1982
23. Whitney TM, Buncke HJ, Alpert BS, et al: The serratus anteriorfree-muscle flap: experience with 100 consecutive cases. Plast Recon-str Surg 86:481-490, 1990; discussion 491
24. Bharihoke V, Gupta M: Muscular attachments along the medial borderof the scapula. Surg Radiol Anat 8:71-73, 1986
25. Hurwitz MT, Tocantins LM: Isolated paralysis of the serratus anterior(magnus) muscle. J Bone Joint Surg 20:720-725, 1938
26. Fitchet SM: Injury to the serratus magnus (anterior) muscle. N EnglJ Med 203:818-823, 1930
27. Godat DM, Sanger JR, Lifchez SD, et al: Detailed neurovascularanatomy of the serratus anterior muscle: implications for a functionalmuscle flap with multiple independent force vectors. Plast ReconstrSurg 114:21-29, 2004; discussion 30-31
28. Cuadros CL, Driscoll CL, Rothkopf DM: The anatomy of the lowerserratus anterior muscle: a fresh cadaver study. Plast Reconstr Surg95:93-97, 1995; discussion 98-99
29. Vu P, Guedon C, Gehanno P, et al: Anatomic basis of serratus anteriormuscle flap transposition. Surg Radiol Anat 10:173-185, 1988
30. Meininger AK, Figuerres BF, Goldberg BA: Scapular winging: anupdate. J Am Acad Orthop Surg 19:453-462, 2011
31. Nguyen HV, Nguyen H: Anatomical basis of modern thoracotomies:the latissimus dorsi and the “serratus anterior-rhomboid” complex.Surg Radiol Anat 9:85-93, 1987
32. Seth R, Manz RM, Dahan IJ, et al: Comprehensive analysis of theanterolateral thigh flap vascular anatomy. Arch Facial Plast Surg13:347-354, 2011
33. Song YG, Chen GZ, Song YL: The free thigh flap: A new free flapconcept based on the septocutaneous artery. Br J Plast Surg 37:149-159, 1984
34. Elliott RM, Weinstein GS, Low DW, et al: Reconstruction of complextotal parotidectomy defects using the free anterolateral thigh flap: aclassification system and algorithm. Ann Plast Surg 66:429-437, 2011
35. Yu P, Hanasono MM, Skoracki RJ, et al: Pharyngoesophageal recon-struction with the anterolateral thigh flap after total laryngopharyngec-tomy. Cancer 116:1718-1724, 2010
36. Yu P: Reinnervated anterolateral thigh flap for tongue reconstruction.Head Neck 26:1038-1044, 2004
37. Yu P: Characteristics of the anterolateral thigh flap in a westernpopulation and its application in head and neck reconstruction. Head
Neck 26:759-769, 2004
281Sugg and Kim Dynamic Reconstruction of the Paralyzed Face, Part II
38. Revenaugh PC, Knott PD, Scharpf J, et al: Simultaneous anterolateralthigh flap and temporalis tendon transfer to optimize facial form andfunction after radical parotidectomy. Arch Facial Plast Surg 14:104-109, 2012
39. Labbé D, Huault M: Lengthening temporalis myoplasty and lip rean-imation. Plast Reconstr Surg 105:1289-1297, 2000
40. McLaughlin CR: Surgical support in permanent facial paralysis. PlastReconstr Surg 11:302-314, 1953
41. Iida T, Mihara M, Narushima M, et al: Dynamic reconstruction offull-thickness abdominal wall defects using free innervated vastuslateralis muscle flap combined with free anterolateral thigh flap. AnnPlast Surg (in press)
42. Posch NA, Mureau MA, Flood SJ, et al: The combined free partialvastus lateralis with anterolateral thigh perforator flap reconstructionof extensive composite defects. Br J Plast Surg 58:1095-1103, 2005
43. Chana JS, Chen HC, Sharma R, et al: Use of the free vastus lateralisflap in skull base reconstruction. Plast Reconstr Surg 111:568-574,2003; discussion 575
44. Kuo YR, Seng-Feng J, Kuo FM, et al: Versatility of the free antero-lateral thigh flap for reconstruction of soft-tissue defects: review of 140cases. Ann Plast Surg 48:161-166, 2002
45. Demirkan F, Chen HC, Wei FC, et al: The versatile anterolateral thighflap: a musculocutaneous flap in disguise in head and neck reconstruc-tion. Br J Plast Surg 53:30-36, 2000
46. Yang D, Morris SF, Tang M, et al: A modified longitudinally splitsegmental rectus femoris muscle flap transfer for facial reanimation:anatomic basis and clinical applications. J Plast Reconstr Aesthet Surg59:807-814, 2006; discussion 815-816
47. Hayashi A, Maruyama Y: Neurovascularized free short head of thebiceps femoris muscle transfer for one-stage reanimation of facialparalysis. Plast Reconstr Surg 115:394-405, 2005
48. Koshima I, Umeda N, Handa T, et al: A double-muscle transfer usinga divided rectus femoris muscle for facial-paralysis reconstruction. JReconstr Microsurg 13:157-162, 1997
49. Koshima I, Moriguchi T, Soeda S, et al: Free rectus femoris muscletransfer for one-stage reconstruction of established facial paralysis.Plast Reconstr Surg 94:421-430, 1994
50. Nosrati N, Chao AH, Chang DW, et al: Lower extremity reconstruc-tion with the anterolateral thigh flap. J Reconstr Microsurg 28:227-234, 2012
51. Nasajpour H, Steele MH: Anterolateral thigh free flap for “head-to-toe” reconstruction. Ann Plast Surg 66:530-533, 2011
52. Celik N, Wei FC, Lin CH, et al: Technique and strategy in anterolat-
eral thigh perforator flap surgery, based on an analysis of 15 completeand partial failures in 439 cases. Plast Reconstr Surg 109:2211-2216,2002; discussion 2217-2218
53. Garvey PB, Selber JC, Madewell JE, et al: A prospective study ofpreoperative computed tomographic angiography for head and neckreconstruction with anterolateral thigh flaps. Plast Reconstr Surg 127:1505-1514, 2011
54. Liu SC, Chiu WK, Chen SY, et al: Comparison of surgical result ofanterolateral thigh flap in reconstruction of through-and-through cheekdefect with/without CT angiography guidance. J CraniomaxillofacSurg 39:633-638, 2011
55. Chen SY, Lin WC, Deng SC, et al: Assessment of the perforators ofanterolateral thigh flaps using 64-section multidetector computed to-mographic angiography in head and neck cancer reconstruction. EurJ Surg Oncol 36:1004-1011, 2010
56. Kim EK, Kang BS, Hong JP: The distribution of the perforators in theanterolateral thigh and the utility of multidetector row computed to-mography angiography in preoperative planning. Ann Plast Surg 65:155-160, 2010
57. Rozen WM, Wagstaff MJ, Grinsell D, et al: The course of anterolateralthigh perforators does not correlate between sides of the body: the roleof preoperative imaging. Plast Reconstr Surg 125:132e-134e, 2010
58. Ribuffo D, Atzeni M, Saba L, et al: Angio computed tomographypreoperative evaluation for anterolateral thigh flap harvesting. AnnPlast Surg 62:368-371, 2009
59. Chang NJ, Waughlock N, Kao D, et al: Efficient design of splitanterolateral thigh flap in extremity reconstruction. Plast ReconstrSurg 128:1242-1249, 2011
60. Kimata Y, Uchiyama K, Ebihara S, et al: Anterolateral thigh flapdonor-site complications and morbidity. Plast Reconstr Surg 106:584-589, 2000
61. Saint-Cyr M, Oni G, Lee M, et al: Simple approach to harvest of theanterolateral thigh flap. Plast Reconstr Surg 129:207-211, 2012
62. Rozen WM, le Roux CM, Ashton MW, et al: The unfavorable anatomyof vastus lateralis motor nerves: a cause of donor-site morbidity afteranterolateral thigh flap harvest. Plast Reconstr Surg 123:1505-1509,2009
63. Casey WJ 3rd, Rebecca AM, Smith AA, et al: Vastus lateralis motornerve can adversely affect anterolateral thigh flap harvest. Plast Re-constr Surg 120:196-201, 2007
64. Ribuffo D, Cigna E, Gargano F, et al: The innervated anterolateralthigh flap: anatomical study and clinical implications. Plast Reconstr
Surg 115:464-470, 2005