Embed Size (px)
Citation preview

What will it take to End TB?
The Snell Memorial LectureBritish Thoracic Society 2016
Christopher DyeWorld Health Organization

Snell Memorial Lectures in the MDG era• 2015 BCG – old story with new twists. Paul Fine• 2014 Mycobacterium tuberculosis: where did it come from
and where is it going? Douglas Young • 2012 The pathway to the development of TB
vaccines. Helen McShane• 2009 New anti-TB drugs and how to test them. Denis
Mitchison• 2008 Novel diagnostic approaches to tuberculosis. Ajit
Lalvani• 2006 The current treatment of tuberculosis: Should we be
doing better before new drugs arrive? Peter Ormerod• 2005 The origin of tuberculosis. Stewart Cole• 2003 Taking risks in tuberculosis. John Moore-Gillon• 2001 Tuberculosis: A global view. Philip Hopewell

Sustainable Development Goals: 2016-2030New impetus to End TB?

Sustainable Environments
Health & Well-being
Growing Economies
Inclusive Societies Systems & ServicesUniversal Health Coverage
Systems:Shared inputs,
mutually beneficial outcomes

TB ↔ SDGs
235 indicators 21 important
7 critical 5 UHC>1 R&D
≥ 8 of 17 Goals


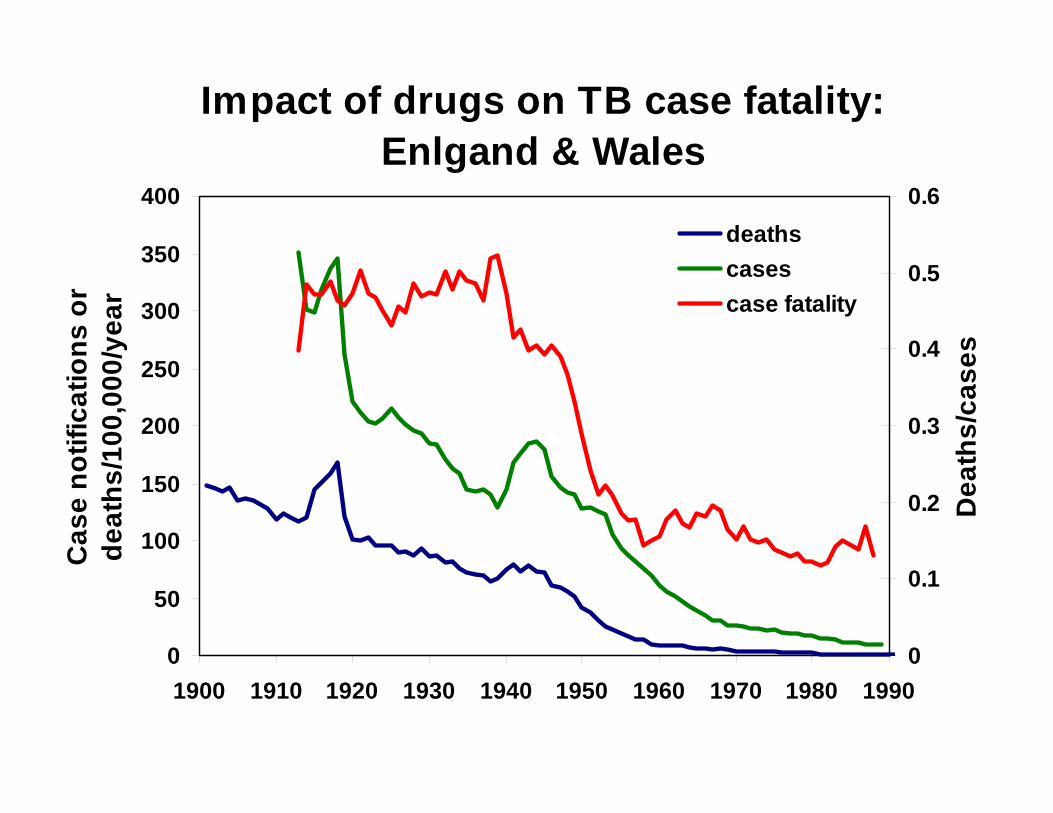
Impact of drugs on TB case fatality: Enlgand & Wales
0
50
100
150
200
250
300
350
400
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990
Cas
e no
tific
atio
ns o
r de
aths
/100
,000
/yea
r
0
0.1
0.2
0.3
0.4
0.5
0.6
Dea
ths/
case
s
deathscasescase fatality

0
200
400
600
800
1000
1960 1970 1980 1990 2000 2010
Pre
vale
nce
TB/1
00k
“Model DOTS" accelerates TB decline in S India
2.1
2.0
14.4
13.27.2
15.84.2
0.8
Intervention1999-2006
Culture+
Smear+
Model: early Dx/Rx cuts transmissionNot model: hard to scale


MDG 6 TB target achieved but still a top 10 cause of death
Target
Mortality
49 million lives saved between 2000 and 2015
Incidence
Falling 1.4% per year (2000-5)
18% drop since 2000
TB epidemic reversed, 47% fall in TB mortality

Millions

Where is TB falling fastest?Decline incidence rate since 2010 >4%/year in:
Zimbabwe (-11%)Lesotho (-7%)
Tanzania (-6.8%)Ethiopia (-6.7%)Namibia (-6.2%)Kenya (-5.0%)Russia (-4.2%)
All countries with increase in incidence 1990sHigh %HIV+, or Russia, high proportion recent infectionWHO Global TB Control 2016
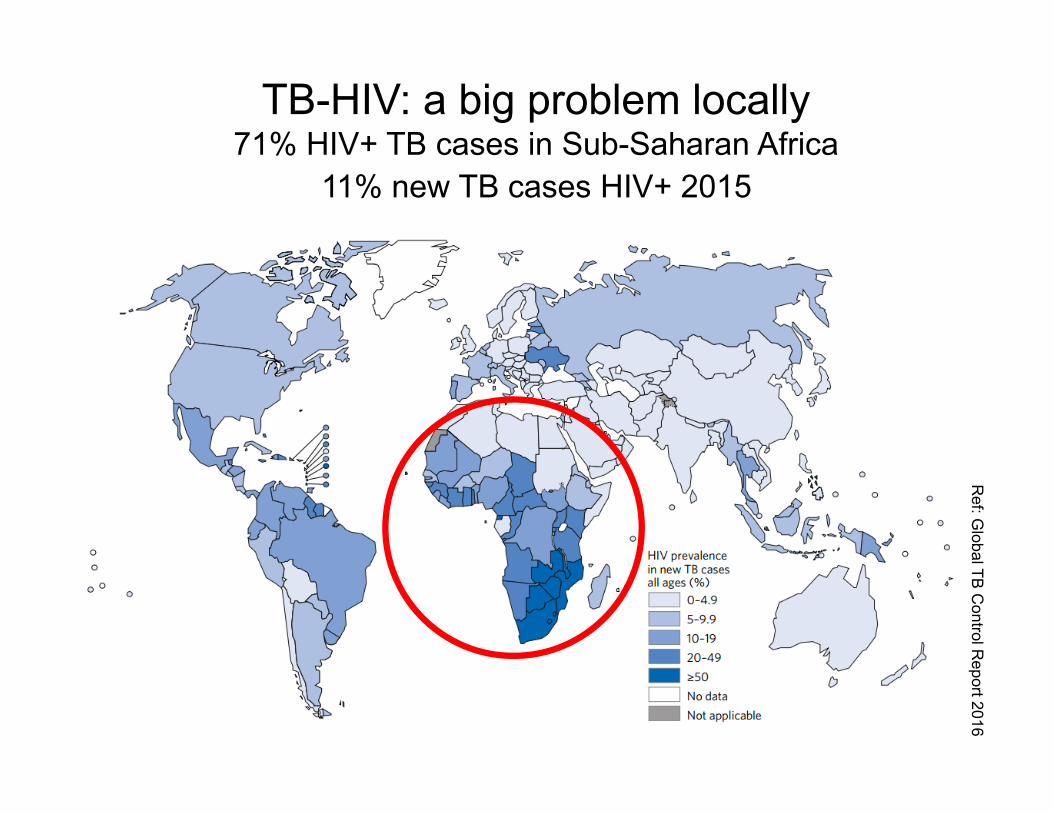
Ref: G
lobal TB C
ontrol Report 2016
TB-HIV: a big problem locally71% HIV+ TB cases in Sub-Saharan Africa
11% new TB cases HIV+ 2015

Drug-resistant TB in every country rise of XDR but no increase in MDR globally
480k new cases of MDR-TB in 2015+100k new rifampicin-resistant TB eligible for MDR-TB treatment
0-2.93-5.96-11.912-17.9>18
% cases with MDR/RR-TB

1
10
100
1000
10000
1990 2000 2010 2020 2030 2040 2050
TB c
ases
/mill
ion/
year
Year
Up to 10%/yr with currenttechnologyBeyond currenttechnology
Elimination <1/M
2%/yr
20%/yr
10%/yr
TB cases: elimination by 2050?
UHC
New tools
20%/yr
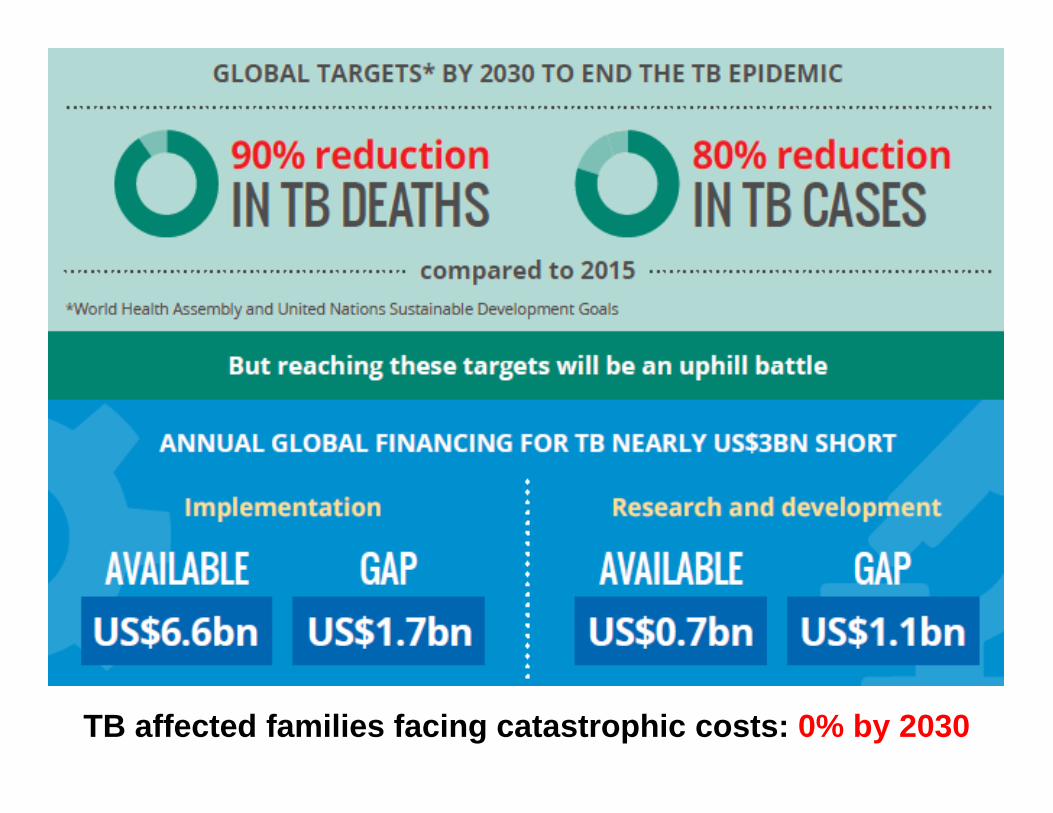
TB affected families facing catastrophic costs: 0% by 2030

SDG 3.8Achieve universal health
coverage
UHC: Everyone can get the health services they need without suffering financial hardship when paying for them
Goal 3: Ensure healthy lives and promote well-being for all at all ages

Aaron MotsoalediUSAID’s TB Champion
“time to treat TB with the same urgency… as Ebola or Zika virus.”
Jim KimWorld Bank President
“to meet needs of the poor… functioning health systems in every country in the world.”
World TB Day 2016

Doctors and delays, Bangalore
No. doctors seen by TB patients
02040
6080
100120
140160180
1 2 3 4 5 6 7Number of doctors
No.
fem
ale
patie
nts
0
50
100
150
200
250
No.
mal
e pa
tient
s
WomenMen
0
20
40
60
80
0 1 2 3 4 5 6 7 8Number of doctors
Tota
l dur
atio
n (d
ays)
Each extra doctor seen
adds 12 days
More doctors, longer treatment
Pantoja 2009

Out-of-pocket expenditures on health too high
Mandatory prepayment
Voluntary prepayment
Out-of-pocket
Not-for-profit
Private, other
20%
40%
Shar
e of
tota
l hea
lth e
xpen
ditu
res
(%)
60%
80%
100%

R² = 0.650
10
20
30
40
50
60
70
80
1 2 3 4 5 6 7 8 9 10 11
Out of p
ocket a
s % expen
diture health
Government health spending as % of GDP
Azerbaijan
Sweden
Where governments spend more on health, with financial protection, patients pay less
European countries
WHO EURO

Vertical TB services with in-patient care are often inefficient
WHO EURO

Tallinn Charter: health systems for health and wealth
• Armenia out-patient TB treatment most effective to reduce costs and expand TB services
• Azerbaijan shift to out-patient treatment, TB services in State Benefit Package
• Kazakhstan integration of TB and HIV with primary health, disease management programme emphasizing risk groups
• Kyrgyzstan aligning financing and servicedeliveryWHO EURO

Mean cost of TB episode as
% yearly household income per capita
58%
81% 83%
40%
50%
60%
70%
80%
90%
100%
High livingstandard
Medium livingstandard
Low livingstandard
Bangalore
32%
68%
0%
20%
40%
60%
80%
100%
High living standard Low living standard
Yangon
Inequity ─ measurement exposes the problem

Inequity – few easy solutions?
USAID TB CARE II Project 2013
Thailand long waiting times discourage patients from obtaining services through national health insurance Philippines patients believe they face direct and indirect costs for TB services in the public sector, thus choose private, including pharmacies
General uncoordinated functions of NTPs and insurance agencies

Addis Ababa Action Agenda domestic $$ needed, but international $$ too
Share of global TB burden in 2015 (incident cases)
BRICS 42%
Other middle-income (42%)
Low-income (14%)
High-income (2%)
Shar
e of
ava
ilabl
e fu
ndin
g in
201
6

SDGs 3, 9…“Enhance scientific
research, foster innovation”

R&D for TB 2016
• ≈$2bn/year needed, $1.1bn gap• 4 diagnostic tests recommended by WHO• 9 drugs in advanced clinical trials for drug-
susceptible and drug-resistant TB or latent infection
• 13 vaccine candidates in clinical trials for prevention of infection and prevention of disease in people already infected

Best rapid diagnostic is Xpert MTB/RIF but not “point-of-care”

Treatment Action Group 2015

1
10
100
1990 2000 2010 2020 2030 2040 2050
Cas
es/m
illio
n/yr
Even USA needs more than current tools
Total
US born
Base
IPT HIV-
On course for elimination
Not on course for elimination: needs boost from IPT for HIV-
100

What could the SDGs do for TB?Case incidence: the first 10%• Early diagnosis & treatment
UHC in SDGs has shifted thinking on TB UHC isn’t simple, but good local solutions emerging
Case incidence: the second 10%• R&D critical
Point-of-care diagnosisTreatment latent infection (mass)Vaccination
Mortality• Drug treatment has bigger & quicker effects on
mortality than incidence

0
1
2
3
4
5
6
0
20
40
60
80
100
120
140
160
1980 1985 1990 1995 2000 2005 2010 2015
New
cases ('00
0s)per year ‐
Hun
gary
New
cases ('00
0s) p
er year ‐
Russia
Years
Undoing: TB and the collapse of the Soviet Union
RussiaHungary





























