Embed Size (px)
Citation preview
British Heart3Journal, I975, 37, I069-I076.
Dual atrioventricular nodal pathwaysA common electrophysiological response'
Pablo Denes, Delon Wu, Ramesh Dhingra, Fernando Amat-y-Leon, Christopher Wyndham,and Kenneth M. RosenFrom the Section ofCardiology, Abraham Lincoln School ofMedicine, University of Illinois College ofMedicine,and the West Side Veterans' Administration Hospital, Chicago, Illinois, U.S.A.
Evidence of dual atrioventricular nodal pathways (a sudden jump in H1-H2 at critical A1-A2 coupling in-tervals) was shown in 4I out of 397 patients studied with atrial extrastimulus techniques. In 27 of these 41,dual pathways were demonstrable during sinus rhythm, or at a cycle length close to sinus rhythm (CL1).In the remaining 14, dual pathways were only demonstrated at a shorter cycle length (CL2). Allpatients with dual pathways at cycle length1 who were also tested at cycle length2 (iI patients) had dualpathways demonstrable at both cycle lengths. In these II patients both fast and slow pathway effective refrac-tory periods increased with decrease in cycle length. Twenty-two of the patients (54%) had either an aetio-logicalfactor strongly associated with atrioventricular nodal dysfunction or one or more abnormalities suggest-ing depressed atrioventricular nodalfunction. Evaluation offast pathway properties suggested that this path-way was intranodal.
Seventeen of the patients had previously documented paroxysmal supraventricular tachycardia (group I).Eight patients had recurrent palpitation without documented paroxysmal supraventricular tachycardia(group 2), and I6 patients had neither palpitation nor paroxysmal supraventricular tachycardia (group 3).Echo zones were demonstrated in I5 patients (88%) ingroup i, no patients in group 2, and 2 patients (I3%) ingroup 3.
The normal atrioventricular nodal conduction curverelating A1-A2 to H1-H2, generated with atrial extra-stimulus technique is smooth (Krayer, Mandoki,and Mendez, i95i; Mendez, Gruhzit and Moe,I956; HofEman et al., I963; Wit et al., I970;Goldreyer, I972; Van Cappelle, Du Perron, andDurrer, I97I; Ferrier and Dresel, I973, 1974). Abroken curve, with abrupt reproducible increase inH1-H2 responses over a critical range of A1-A2coupling intervals suggests the presence of dualatrioventricular nodal pathways (Moe, Preston, andBurlington, I956; Mendez et al., I965; Schuilen-burg and Durrer, I969; Denes et al., I973; Rosen,Mehta, and Miller, I974; Wu et al., 1974). We havereported extrastimulus studies suggestive of dualatrioventricular nodal pathways in a patient withtwo PR intervals, and in a limited number of
Received ii March 1975.'Supported in part by the Myocardial Infarction Program,National Heart and Lung Institutes, National Institutes ofHealth, Education and Welfare, and the West Side Veterans'Administration Hospital, Chicago Basic Institutional Support.
patients with atrioventricular nodal re-entrantparoxysmal supraventricular tachycardia (Deneset al., I973; Rosen et al., I974; Wu et al., I974).In these earlier studies, the presence of dualatrioventricular nodal pathways was related to thepatients' clinical and/or electrocardiographic find-ings.Our recent experience suggests that electro-
physiological responses suggestive of dual atrio-ventricular nodal pathways are a common occurrenceand often without apparent relation to the patients'clinical or electrocardiographic findings. In thisreport, we describe our total experience withpatients having extrastimulus studies suggestive ofdual atrioventricular nodal pathways. Clinical,electrocardiographic, and electrophysiological ob-servations are reported in this group, in order toelucidate further the significance of this interestingelectrophysiological phenomenon.
Subjects and methodsForty-one patients out of a total number of 397 patients
on 8 April 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.10.1069 on 1 October 1975. D
ownloaded from
1070 Denes, Wu, Dhingra, Amat-y-Leon, Wyndham, and Rosen
studied with atrial extrastimulus technique betweenJuly I971 and July I974 showed electrophysiologicalevidence of dual atrioventricular nodal pathways. Theseare the subject ofthe present report. Patients with electro-cardiographic evidence of pre-excitation (short PRinterval (<O.I2 s), and/or presence of a delta wave)were excluded. Historical, physical, electrocardio-graphic, and electrophysiological findings were reviewedin each patient. Of these 4I patients, 8 have been thesubjects of previous reports (Denes et al., I973; Rosenet al., I974; Wu et al., I974).
Electrophysiological studies were performed in thepost-absorptive, non-sedated state. All cardiac drugswere discontinued 48 hours before study. Informed con-sent was obtained from each patient. His bundle electro-grams were recorded by a catheter technique (Dhingra,Rosen, and Rahimtoola, I973). Refractory periods weremeasured with the atrial extrastimulus method duringsinus rhythm, or at a cycle length slightly shorter thansinus (CL1) (Denes et al., 1973). In 25 patients, theeffect of shortening of cycle length on refractory periodswas also examined. In these patients, a second pacedcycle length (CL2) was selected, which was shorter thanCL1, but longer than the cycle length inducing atrio-ventricular nodal Wenckebach periods.
DefinitionsEstablished criteria for electrocardiographic diagnosis ofmyocardial infarction and arrhythmias were used (Lip-man and Massie, I965; Katz and Pick, 1956). 'Docu-mented arrhythmias' were defined as spontaneousarrhythmias with electrocardiographic documentation.Two PR intervals were diagnosed when surface electro-cardiograms revealed two non-overlapping ranges ofPR intervals (Rosen et al., I974).Dual atrioventricular nodal pathways were defined
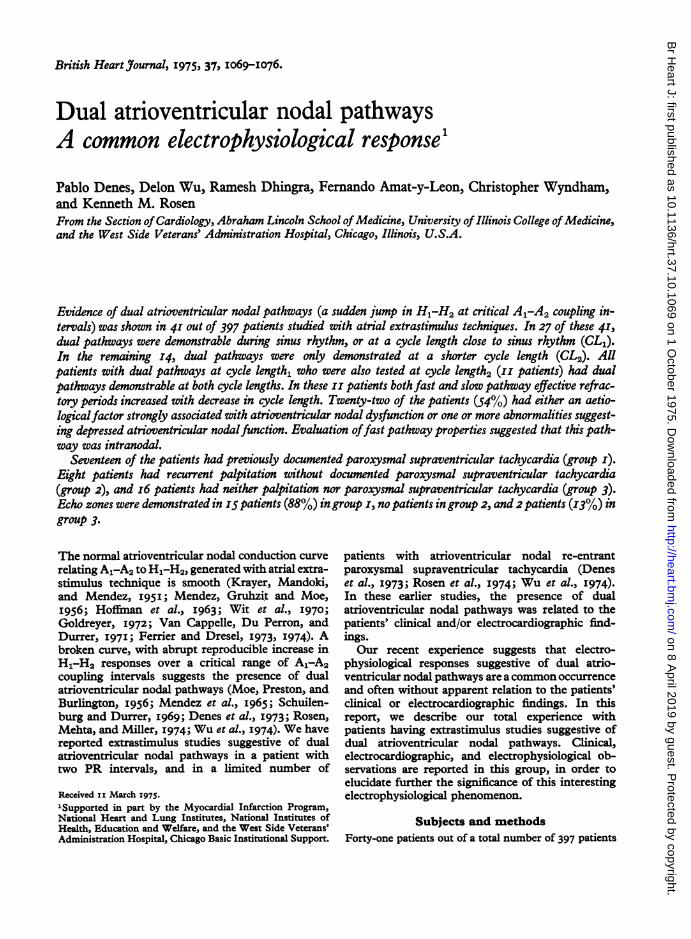
with atrial extrastimulus technique. Dual pathwaycurves were characterized by a sudden jump in H1-H2at a critical range of A1-A2 coupling intervals (Deneset al., I973; Rosen et al., 1974; Wu et al., I974). Noneof these curves conformed to previously describednormal atrioventricular nodal curves. The portion of thecurve to the right of the jump represented the fast path-way, and to the left, the slow pathway. The slope of theslow pathway could be positive (decrease in H1-H2 withdecreasing A1-A2 intervals), flat (no change in H1-H2with decreasing A1-A2), or negative (increase in H1-H2with decreasing A1-A2). Though repeated scanning withthe atrial test stimuli close to the A1-A2 interval pro-ducing the jump frequently demonstrated an overlap ofH1-H2 corresponding to the fast and slow pathways,intermediate H1-H2 intervals were not elicited inthis zone of overlap (Rosen et al., 1974). Curve fittinganalysis was used in any of the cases where the diag-nosis of dual pathways was equivocal (Denes et al., 1973).The fast pathway effective refractory period was de-
fined as the longest A1-A2 that failed to conduct via thefast pathway, even in those cases where overlap be-tween fast and slow pathway curves occurred. The fastpathway functional refractory period was defined as theshortest attainable H1-H2 interval on the fast pathway
curve. The effective refractory period of the slow path-way was the longest A1-A2 not conducted via the slowpathway. When atrial functional refractory period limi-ted slow pathway conduction, the slow pathway effec-tive refractory period could not be measured, and wasconsidered to be less than the shortest conducted A1-A2interval. The slow pathway functional refractory periodwas the shortest attainable H1-H2 interval on the slowpathway curve.
Atrioventricular nodal re-entry was diagnosed bynoting atrial echoes with low to high activation sequencerelated to achievement of a critical AH interval (Gold-reyer, 1972; Denes et al., I973; Wu et al., I974). Thisoccurred with or without sustained paroxysmal supra-ventricular tachycardia (Wu et al., I974).
ResultsClinical data (Table i)There were 26 male and IS female patients, meanage 50 years (range I3 to 8i years). Eighteen (44%)patients had no evidence of organic heart disease, 7(17%) had arteriosclerotic cardiovascular disease, 7(I7%) had hypertensive cardiovascular disease, 3(7.3%) had primary conduction disease (intraven-tricular conduction defect without other evidenceof organic heart disease), 3 (7.3%) had congenitalheart disease (i postoperative ventricular septaldefect, i postoperative coarctation of the aorta, andi secundum atrial septal defect), and 3 (7.3%) hadhypothyroidism. Cardiomegaly was present in 32per cent (I3/41) of the patients.The resting electrocardiogram was normal in ii
(27%) of the patients, and I5 (37%) had an intra-ventricular conduction defect. (The high incidenceof patients with bundle-branch block presumably
800 A . B . C7QQ~00 CL 640 CL00 b CL720700- ..
300 500 700 400 bOO 400 b00ms Al A2 A1A2 AlA2
FIG. i Three types of dual atrioventricular nodalcurves. In eachpanel,A1-A2 coupling intervals are plot-tedon the abscissa andH1-H2 responses on the ordinate.CL = cycle length. Intervals are expressed in ms.Note a sudden jump in H1-H2 at a critical A1-A2coupling interval. The portion of the curve to the rightof the jump represents the fast pathway, and to theleft, the slow pathway. Panel A shows a slow pathwaycurve with negative slope, Panel B shows a slow path-way curve with flat slope, and Panel C shows a slowpathway curve with positive slope.
on 8 April 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.10.1069 on 1 October 1975. D
ownloaded from

Dual AV nodal pathways I07I
TABLE I Clinical and electrocardiographic findings
Case No. Age Sex Symptom Chest x-ray Cardiovascular ECG Documentedheart size diagnosis arrhythmia
I 50 F Palpitation Normal Hypothyroidism2 55 M Palpitation Normal NHD3 62 F Palpitation Normal NHD4 44 M Palpitation Normal NHD5 62 M Palpitation Normal HCVD
6 68 F Palpitation Normal NHD7 52 M Palpitation Normal NHD8 50 M Palpitation Normal NHD9 54 M Palpitation Normal NHDI0 20 F Palpitation Normal NHDII 6o F Palpitation Normal NHDI2 63 F Palpitation Normal NHD13 5i F Palpitation Normal HypothyroidismI4 32 M Palpitation Normal NHDI5 22 F Palpitation Normal ASDI6 28 M Palpitation Normal NHD17 26 M Palpitation Normal NHD18 73 M Palpitation Cardiomegaly HCVDI9 32 F Palpitation Normal NHD20 22 F Palpitation Normal NHD2I 68 M Palpitation Normal NHD22 54 F Palpitation Cardiomegaly HCVD, SSNS
23 55 M Palpitation Cardiomegaly ASHD
Low voltage, ST-T PSVTWNL PSVTST-T PSVTST-T PSVTAMI, I° AVB,LAD PSVT
ST-T PSVTWNL PSVTWNL PSVTWNL PSVTWNL PSVTST-T PSVTST-T PSVTWNL PSVTWNL PSVTIRBBBWNL PSVTWNL PSVTLBBB, I° AVB PSVTLow atrial rhythmWNLWNL -ST-T Sinus bradycardia,
atrial flutterIMI Ventricular tachy-
cardia24 59 M Angina,
palpitation Cardiomegaly ASHD IMI Atrial flutter25 40 M Dyspnoea Cardiomegaly ASHD IMI26 64 M Dyspnoea Cardiomegaly ASHD CRBBB and RAD -
27 54 M Dyspnoea Cardiomegaly Post-surgicalcoarctation LVH
28 68 M Angina, Cardiomegaly ASHD CRBBB and LAD, Ventricularpalpitation IMI tachycardia
29 58 M Angina Normal ASHD IMI30 70 F Dyspnoea Cardiomegaly HCVD CRBBB and LAD31 58 M Dyspnoea Cardiomegaly HCVD CRBBB and LAD,
Io AVB32 59 M Angina Normal ASHD RDBBB33 8i F Syncope Normal PCD, SSNS CRBBB and LAD Sinus bradycardia34 22 M Asymptomatic Normal PCD CRBBB and LAD -
35 22 M Asymptomatic Normal PCD CRBBB and LAD -
36 21 F Asymptomatic Normal NHD I° AVB37 13 M Asymptomatic Normal Post-surgical VSD CRBBB and LAD -
38 98 M Dyspnoea Cardiomegaly HCVD CRBBB and LAD -39 24 F Dyspnoea Normal NHD Io AVB40 67 M Dyspnoea Cardiomegaly Hypothyroidism CRBBB and LAD -
41 69 M Dizziness Cardiomegaly HCVD LBBB Sinus bradycardia
Abbreviations: ASHD = arteriosclerotic heart disease; HCVD = hypertensive cardiovascular disease; PCD = primary conductiondisease; NHD =no heart disease; ASD =atrial septal defect; VSD = ventricular septal defect; CRBBB= complete rightbundle-branch block; LAD =left axis deviation; IMI = inferior wall myocardial infarction; AMI = anterior wall myocardialinfarction; LVH=left ventricular hypertrophy; WNL=within normal limits; RAD=right axis deviation; ST-T=ST-Twave changes; IRBBB=incomplete right bundle-branch block; PSVT=paroxysmal supraventricular tachycardia; i° AVB=first degree atrioventricular block; SSNS = sick sinus node syndrome; RDBBB = rate dependent bundle-branch block;LBBB=left bundle-branch block.
on 8 April 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.10.1069 on 1 October 1975. D
ownloaded from
zo72 Denes, Wu, Dhingra, Amat-y-Leon, Wyndhwam, and Rosen
90u * A -B .
700 0.
5001 * CL667
300 500 700 1100 X100 500 700 Sooms AlAl Ms AAgAi
Slow Fost Slow FootERP 360 460 ERP 470 640
FRP600
550 FRP 825 640
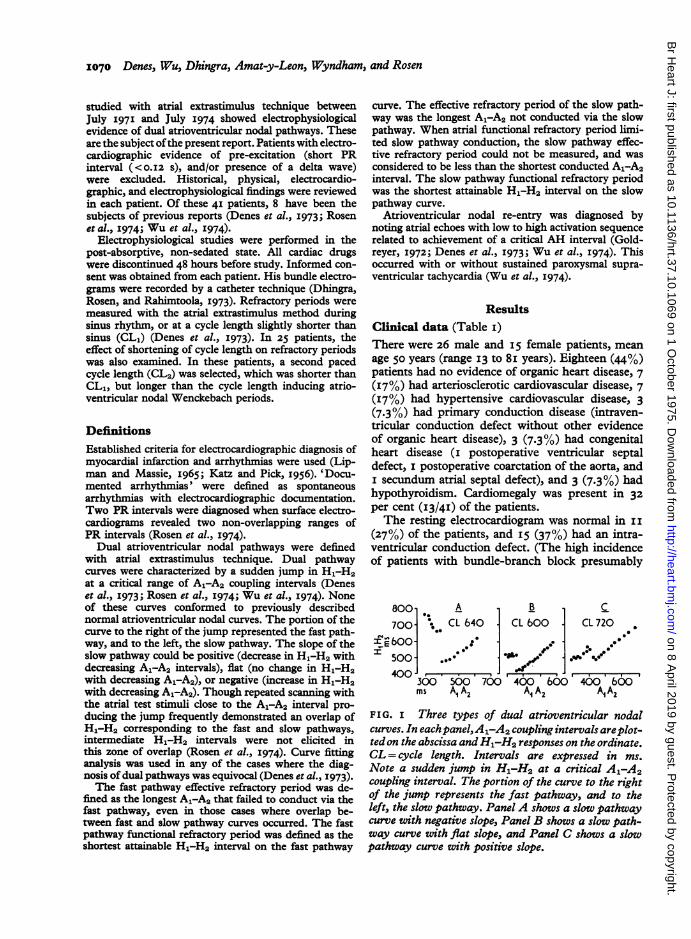
FIG. 2 An example of the effect of shortening cyclelength on fast and slow pathway refractory periods.CL=cycle length; ERP=effective refractory period;FRP=Junctional refractor-y period. Intervals are
expressed in ms. Panels A and B represent dual A-Vnodal curves at two different CL's in the same patient.Note the increase in ERP and FRP of both slow andfast pathways with decrease in CL.
reflects the large number of patients with intraven-tricular conduction defect studied at our laboratoryunder an NIH contract.) In 3 patients, two PRintervals were observed on the surface electro-cardiogram. One of these cases has been reported indetail in a separate publication (Rosen et al., I974).
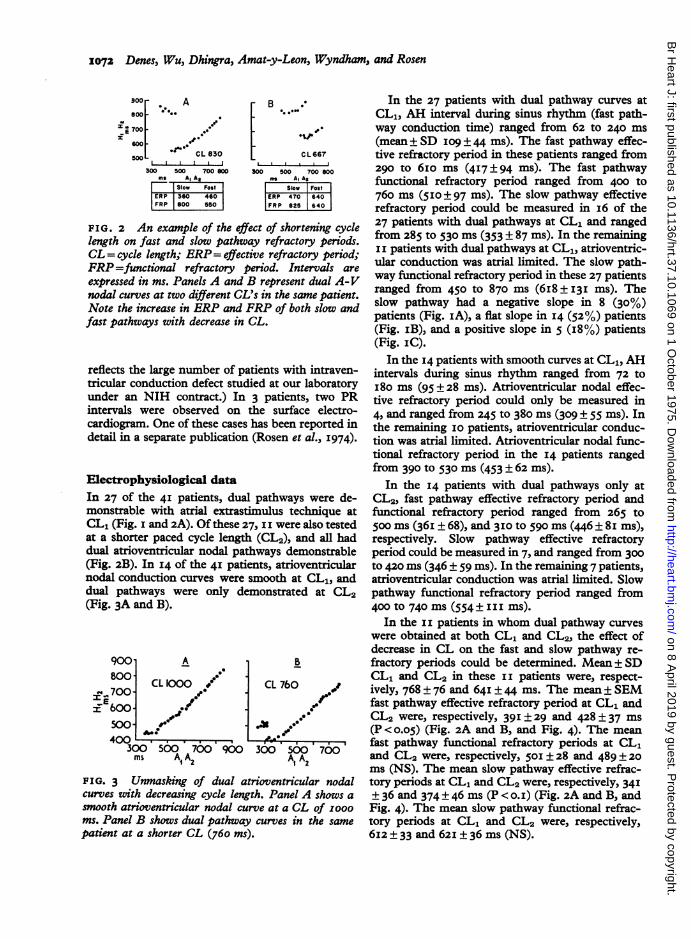
Electrophysiological dataIn 27 of the 4I patients, dual pathways were de-monstrable with atrial extrastimulus technique atCL1 (Fig. i and 2A). Of these 27, II were also testedat a shorter paced cycle length (CL2), and all haddual atrioventricular nodal pathways demonstrable(Fig. 2B). In 14 of the 4I patients, atrioventricularnodal conduction curves were smooth at CL1, anddual pathways were only demonstrated at CL2(Fig. 3A and B).
900 A B
800° CL 10D CL 7605700 70i600-
400300 5500' 7500 900 300 500 700ms A,A2 AlA2
FIG. 3 Unmasking of dual atrioventricular nodalcurves with decreasing cycle length. Panel A shows a
smooth atrioventricular nodal curve at a CL of 0OOOms. Panel B shows dual pathway curves in the samepatient at a shorter CL (760 ms).
In the 27 patients with dual pathway curves atCL1, AH interval during sinus rhythm (fast path-way conduction time) ranged from 62 to 240 ms(mean ± SD I09 ± 44 ms). The fast pathway effec-tive refractory period in these patients ranged from290 to 6Io ms (417 ± 94 ms). The fast pathwayfunctional refractory period ranged from 400 to760 ms (510±97 ms). The slow pathway effectiverefractory period could be measured in i6 of the27 patients with dual pathways at CL1 and rangedfrom 285 to 530 ms (353 ± 87 ms). In the remainingII patients with dual pathways at CL1, atrioventric-ular conduction was atrial limited. The slow path-way functional refractory period in these 27 patientsranged from 450 to 870 ms (6i8 ± I3I ms). Theslow pathway had a negative slope in 8 (30%)patients (Fig. IA), a flat slope in I4 (52%) patients(Fig. iB), and a positive slope in 5 (i8%) patients(Fig. IC).
In the I4 patients with smooth curves at CL1, AHintervals during sinus rhythm ranged from 72 toI8o ms (95 ± 28 ms). Atrioventricular nodal effec-tive refractory period could only be measured in4, and ranged from 245 to 380 ms (309 ± 55 ms). Inthe remaining I0 patients, atrioventricular conduc-tion was atrial limited. Atrioventricular nodal func-tional refractory period in the I4 patients rangedfrom 390 to 530 ms (453 ± 62 ms).
In the I4 patients with dual pathways only atCL2, fast pathway effective refractory period andfunctional refractory period ranged from 265 to500 ms (36i ± 68), and 3IO to 590 ms (446 ± 8i ms),respectively. Slow pathway effective refractoryperiod could be measured in 7, and ranged from 300tO 420 ms (346 ± 59 ms). In the remaining 7 patients,atrioventricular conduction was atrial limited. Slowpathway functional refractory period ranged from400 to 740 ms (554± III ms).
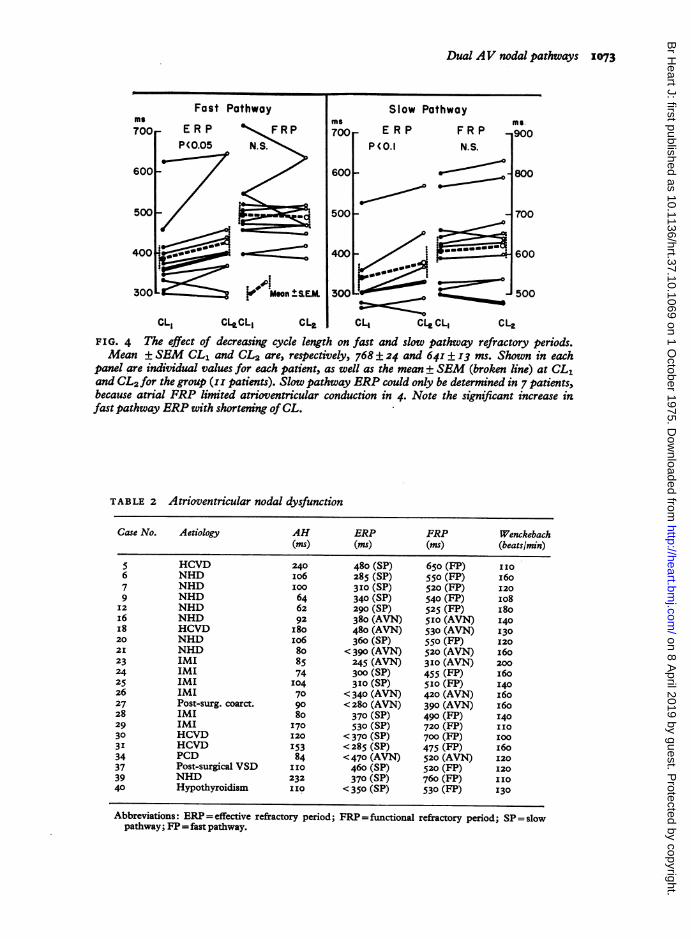
In the II patients in whom dual pathway curveswere obtained at both CL1 and CL2, the effect ofdecrease in CL on the fast and slow pathway re-fractory periods could be determined. Mean ± SDCL1 and CL2 in these II patients were, respect-ively, 768 ± 76 and 64I ± 44 ms. The mean± SEMfast pathway effective refractory period at CL1 andCL2 were, respectively, 39I ± 29 and 428±37 ms(P <o.o5) (Fig. 2A and B, and Fig. 4). The meanfast pathway functional refractory periods at CL1and CL2 were, respectively, 50I ± 28 and 489 ± 20ms (NS). The mean slow pathway effective refrac-tory periods at CL1 and CL2 were, respectively, 341± 36 and 374 ± 46 ms (P < o.I) (Fig. 2A and B, andFig. 4). The mean slow pathway functional refrac-tory periods at CL1 and CL2 were, respectively,6I2 ± 33 and 62I ± 36 ms (NS).
s^_ a
on 8 April 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.10.1069 on 1 October 1975. D
ownloaded from
Dual AV nodal pathways 1073
Fast Pathway
Maamn±t+
E
P(C
Slow Pathwayms.
'RP FRP 900).I N.S.
800
_ 700
/s ammmomt 600*s--5 no
CL1 CL,CL, CL, CL, CLe CL, CL,FIG. 4 The effect of decreasing cycle leWth on fast and slow pathway refractory periods.Mean ± SEM CL1 and CL2 are, respectively, 768 ± 24 and 64I±±I3 ms. Shown in each
panel are individual values for each patient, as well as the mean ± SEM (broken line) at CL1and CL2 for the group (I I patients). Slow pathway ERP could only be determined in 7 patients,because atrial FRP limited atrioventricular conduction in 4. Note the significant increase infast pathway ERP with shortening ofCL.
TABLE 2 Atrioventricular nodal dysfunction
Case No. Aetiology AH ERP FRP Wenckebach(ms) (mis) (ms) (beats/lmn)
5 HCVD 240 480 (SP) 650 (FP) IIo6 NHD Io6 285 (SP) 550 (FP) i6o7 NHD I00 3I0 (Sp) 520 (FP) I209 NHD 64 340 (SP) 540 (FP) 108I2 NHD 62 290 (SP) 525 (FP) I80I6 NHD 92 380 (AVN) 5io (AVN) 140I8 HCVD I80 480 (AVN) 530 (AVN) I3020 NHD I06 360 (SP) 550 (FP) 1202I NHD 8o <390 (AVN) 520 (AVN) I6023 IMI 85 245 (AVN) 310 (AVN) 20024 IMI 74 300 (SP) 455 (FP) i6025 IMI I04 310 (SP) 5I0 (FP) I4026 IMI 70 < 340 (AVN) 420 (AVN) I6027 Post-surg. coarct. 90 <280 (AVN) 390 (AVN) 16028 IMI 80 370 (SP) 490 (FP) I4029 IMI I70 530 (SP) 720 (FP) II030 HCVD I20 < 370 (SP) 700 (FP) I003I HCVD I53 <285 (SP) 475 (FP) I6034 PCD 84 <470 (AVN) 520 (AVN) I2037 Post-surgical VSD 110 460 (SP) 520 (FP) I2039 NHD 232 370 (SP) 760 (FP) I1040 Hypothyroidism II0 < 350 (SP) 530 (FP) 130
Abbreviations: ERP=effective refractory period; FRP=functional refractory period; SP=slowpathway; FP= fast pathway.
ms
on 8 April 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.10.1069 on 1 October 1975. D
ownloaded from
1074 Denes, Wu, Dhingra, Amat-y-Leon, Wyndham, and Rosen
Relation of dual pathways to presence ofatrioventricular nodal dysfunction (Table 2)Twenty-two patients (54%) had either an aetio-logical factor strongly associated with atrioven-tricular nodal dysfunction or one or more electro-physiological abnormalities suggesting depressedatrioventricular nodal function. Six patients (I5%)had old inferior wall myocardial infarction (DeSoyza et al., 1974), and 2 patients (5%) had pre-vious surgery for correction of congenitalanomalies.
Electrophysiological evidence for atrioventricularnodal dysfunction was considered to be present on
the basis of one or more of the following: I) pro-longed AH interval (> I30 ms) during sinus rhythm(Dhingra et al., I973) which was found in 5 patients(I2%). 2) Prolonged atrioventricular nodal effectiverefractory period or slow pathway effective refrac-tory period ( > 380 ms) at CL1 (Denes et al., 1974a),which was found in 4 patients (Io%). 3) Prolongedatrioventricular nodal functional refractory periodor fast pathway functional refractory period (> 507ms) at CL1 (Denes et al., I974a), which was found ini6 patients (39%). 4) Atrial pacing rates of IIo or
less inducing atrioventricular nodal Wenckebachperiods (Dhingra et al., I973), which was found in 5patients (I2%). Seventeen patients (41%) had one
or more electrophysiological abnormalities of atrio-ventricular nodal function.
Relation to paroxysmal supraventriculartachycardiaSeventeen patients had electrocardiographic docu-mentation of spontaneous paroxysmal supraven-tricular tachycardia (group i), 8 patients had re-
current paroxysmal palpitation without documenta-tion of spontaneous paroxysmal supraventriculartachycardia (group 2), and i6 patients had neitherpalpitation nor documented paroxysmal supraven-tricular tachycardia (group 3).
In I5 of the I7 patients (88%) in group i, atrio-ventricular nodal re-entrance with echo zones couldbe demonstrated during electrophysiological studies.Single echoes were demonstrated in 5 patients andsustained paroxysmal supraventricular tachycardiawas induced in I0 patients.
In 4 of the 8 patients in group 2, spontaneousarrhythmias other than paroxysmal supraventriculartachycardia were documented (paroxysmal ven-
tricular tachycardia in 2 patients and paroxysmalatrial flutter in 2 patients). No arrhythmias were
documented in the remaining 4 patients. Atrio-ventricular nodal re-entrance with atrial echoes or
paroxysmal supraventricular tachycardia could not
be induced in any of these 8 patients during electro-physiological studies.
In 2 of the i6 patients (I3%) in group 3, singleatrioventricular nodal re-entrant echoes withoutsustained paroxysmal supraventricular tachycardiawere induced during electrophysiological studies.
DiscussionRosenblueth (I958) and Moe et al. (I956), usingextrastimulus technique, suggested that the atrio-ventricular node might undergo longitudinal dis-sociation into two pathways. Rosen et al. (1974)recently reported a patient with two PR intervalsand dual atrioventricular nodal conduction timesand refractory periods, findings strongly suggestiveof dual atrioventricular nodal pathways. Denes et al.(I973), and Wu et al. (I974) reported atrioventric-ular nodal conduction curves (A1-A2, H1-H2) inpatients with atrioventricular nodal re-entrantparoxysmal supraventricular tachycardia and normalPR intervals, suggesting dual atrioventricular nodalpathways. In these previous studies, the demonstra-tion of dual atrioventricular nodal pathways wasdirectly relevant to the patients' clinical or electro-cardiographic findings.The present study suggests that dual atrioventricu-
lar nodal pathways are a relatively common electro-physiological finding, being found in approximatelyio per cent of the patients undergoing extrastimulustesting in our laboratory. Though the patientsstudied in our laboratory frequently have conduc-tion disease, the demonstration of dual pathwayswas frequently not anticipated and not always rele-vant to the patients' clinical or electrocardiographicfindings.
In a patient with dual pathways, the ability todemonstrate these pathways depends upon theproperties of the two pathways. The following con-ditions are necessary for the demonstration of dualpathways with atrial extrastimulus technique. i) Afast pathway effective refractory period which islonger than the slow pathway effective refractoryperiod; if the fast pathway had a shorter effectiverefractory period than the slow pathway, the slowpathway would be concealed. 2) An atrial functionalrefractory period which is shorter than the slowpathway effective refractory period; if the atria hada longer functional refractory period than the slowpathway effective refractory period, the slow path-way would be concealed.The inability to demonstrate dual pathways
during sinus rhythm in I4 patients of the presentseries may be explained by the above conditions.Shortening of cycle length decreased the atrialfunctional refractory period (Denes etal., I974a), and
on 8 April 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.10.1069 on 1 October 1975. D
ownloaded from
Dual AV nodal pathways 1075
as demonstrated in the present study, prolongedfast pathway effective refractory period. Both ofthese effects could allow unmasking of a slow path-way with atrial pacing, which was concealed at CL1.This could account for demonstration of dual path-ways only at CL2 in some or all of these I4 patients.However, another factor must be considered. Italso is possible that dual pathways were not presentat longer cycle lengths (sinus rhythm) in thesepatients, and that non-homogeneity of atrioventric-ular conduction related to shortening of cyclelengths was a necessary prerequisite for functionaldissociation of the atrioventricular node.We have assumed that the slow pathway is intra-
nodal. Whether the fast pathway is intranodal orextranodal (James tract or other bypass) is not yetclear (Denes, Wu, and Rosen, I974b). The follow-ing fast pathway properties are consistent with anintranodal location. i) An AH during sinus rhythm(fast pathway conduction time) which is within orgreater than the normal range of AH intervals. 2) Afast pathway functional refractory period whichis within or greater than the normal range foratrioventricular nodal functional refractory period.3) A fast pathway effective refractory period whichis within or greater than the normal range for atrio-ventricular nodal effective refractory period. 4) Anincrease in fast pathway effective refractory periodwith decrease in cycle length, the normal cyclelength-refractory period relation of the atrioventric-ular node (Denes et al., I974a). Fast pathways in thepresent series conformed to the properties describedabove.
If both fast and slow pathways were intranodal,they could reflect either functional longitudinaldissociation, or anatomical septation of the node.Of the 4I patients reported in this study, 22 hadatrioventricular nodal dysfunction as manifested byabnormal electrophysiological findings (prolongedconduction times or refractory periods) and/oraetiological factors directly associated with atrio-ventricular nodal injury (previous diaphragmaticinfarction or intracardiac surgery) (De Soyza et al.,1974). It is possible that in some of the patients,pathological lesions might be responsible for ana-tomical division of the node into two pathways. Inthe 3 patients with hypothyroidism, one couldpostulate myxoedematous infiltration of the atrio-ventricular node as a possible cause of dual path-ways.The presence of dual atrioventricular nodal path-
ways predisposes to the occurrence of atrioven-tricular nodal re-entrant paroxysmal supraventriculartachycardia (Denes et al., I973; Wu et al., I974). Anatrial premature impulse blocked in the fast path-way may conduct antegradely via the slow pathway,
and return to the atria via the fast pathway. Thus,it is not surprising that I7 of the 4I patients withdual pathways had documented episodes of parox-ysmal supraventricular tachycardia. In I5 of these I7patients, atrioventricular nodal re-entrance with theecho phenomenon was induced during atrial pre-mature stimulation. In IO of these i5, sustainedatrioventricular nodal re-entrant paroxysmal supra-ventricular tachycardia could be induced duringelectrophysiological study.The following conditions seem to be necessary for
the induction of single atrial echoes (due to atrio-ventricular re-entrance) in a patient with dual path-ways. i) An antegrade fast pathway effective refrac-tory period longer than the slow pathway antegraderefractory period. 2) A slow pathway anterogradeconduction time long enough for the pathway to re-cover for retrograde conduction. 3) A final commonpathway distal to the fast and slow pathways, so thatthe impulse can re-enter the fast pathway. 4) Abilityfor the fast pathway to conduct in retrograde direc-tion. For sustained atrioventricular nodal re-entrantparoxysmal supraventricular tachycardia to developin these patients, conditions i) to 4) must be met.In addition, there must be a proximal commonpathway so that the retrograde fast pathway im-pulse can re-enter the slow pathway in an ante-grade direction. There must also be critical relationsbetween fast and slow pathway conduction timesand refractory periods, so that the circus movementis not extinguished.
Atrioventricular nodal conduction is much in-fluenced by autonomic nervous influences. Since thenecessary relation between fast and slow pathwayconduction time and refractory periods appear to berelatively critical for the development of sustainedre-entrance, the lack of induction of sustained re-entry in the patients with known documentedparoxysmal supraventricular tachycardia is not sur-prising. One has only to postulate that autonomicinfluences have critically changed refractoriness orconduction time in one or both pathways, and theability for sustained re-entrance could be lost. Thedemonstration of dual pathways in 8 patients withparoxysmal palpitation without documented parox-ysmal supraventricular tachycardia is intriguing.Though in 4 of the patients, other arrhythmias(ventricular tachycardia and atrial flutter) appeared torelate to palpitation, in the remaining 4, dual path-ways were the most striking abnormality of con-duction demonstrated. It is our opinion that thedemonstration of dual pathways in these 4 suggeststhat sporadic episodes of atrioventricular nodal re-entrant paroxysmal supraventricular tachycardiamay account for the history of palpitation. Sixteenof the patients had neither palpitation nor docu-
on 8 April 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.10.1069 on 1 October 1975. D
ownloaded from

1076 Denes, Wu, Dhingra, Amat-y-Leon, Wyndham, and Rosen
mented paroxysmal supraventricular tachycardia.It is not known whether these i6 patients are at riskfor development of clinically significant spontaneousparoxysmal supraventricular tachycardia in thefuture.The present study sheds little light on one of the
most intriguing questions concerning dual atrio-ventricular nodal pathways in man: 'Are dualatrioventricular nodal pathways a property ofthe normal atrioventricular node in a healthy heart ?'Our data in patients without organic heart diseaseand without paroxysmal supraventricular tachy-cardia are too limited to answer this question. Ourcurrent data suggest that patients with recurrentparoxysmal supraventricular tachycardia withoutother cardiac abnormality frequently have dualatrioventricular nodal pathways. However, in thesepatients, it is possible that either congenital oracquired abnormality of atrioventricular nodalfunction predisposes to longitudinal dissociation ofthe atrioventricular node into dual pathways.
ReferencesDenes, P., Wu, D., Dhingra, R. C., Chuquimia, R., and Rosen,
K. M. (I973). Demonstration of dual A-V nodal pathwaysin patients with paroxysmal supraventricular tachycardia.Circulation, 48, 549.
Denes, P., Wu, D., Dhingra, R., Pietras, R. J., and Rosen,K. M. (1974a). The effect of cycle length on cardiac re-fractory periods in man. Circulation, 49, 32.
Denes, P., Wu, D., and.Rosen, K. M. (I974b). Demonstra-tion of dual A-V pathways in a patient with Lown-Ganong-Levine syndrome. Chest, 65, 343.
De Soyza, N. D. B., Bissett, J. K., Kane, J. J., and Murphy,M. L. (I974). Latent defects of atrio-ventricular conduc-tion in right coronary artery disease. American HeartJournal, 87, I64.
Dhingra, R. C., Rosen, K. M., and Rahimtoola, S. H. (I973).Normal conduction intervals and responses in 6I patientsusing His bundle recording and atrial pacing. Chest, 64, 55.
Ferrier, G. R., and Dresel, P. E. (I973). Role of the atrium indetermining the functional and effective refractory periodsand the conductivity of the atrioventricular transmissionsystem. Circulation Research, 33, 375.
Ferrier, G. R., and Dresel, P. E. (1974). Relationship of thefunctional refractory period to conduction in the atrio-ventricular node. Circulation Research, 35, 204.
Goldreyer, B. N. (1972). Intracardiac electrocardiography inthe analysis and understanding of cardiac arrhythmias.Annals of Internal Medicine, 77, I17.
Hoffman, B. F., Moore, E. N., Stuckey, J. H., and Cranefield,P. F. (I963). Functional properties of the atrioventricularconduction system. Circulation Research, 13, 308.
Katz, L., and Pick, A. (I956). Clinical Electrocardiography,Part I, The Arrhythmias. Lea and Febiger, Philadelphia.
Krayer, 0., Mandoki, J., and Mendez, C. (19si). Studies onveratrum alkaloids: XVI. Action of epinephrine and ofveratramine on the functional refractory period of theauriculo-ventricular transmission in the heart-lung pre-paration of the dog. Journal of Pharmacology and Experi-mental Therapeutics, 103, 412.
Lipman, B., and Massie, E. (I965). Clinical Scalar Electro-cardiography, sth ed. Year Book Medical Publishers,Chicago.
Mendez, C., Gruhzit, C. C., and Moe, G. K. (I956). Influenceof cycle length upon refractory period of auricles, ven-tricles, and A-V node in the dog. American Journal ofPhysiology, 184, 287.
Mendez, C., Han, J., Garcia de Jalon, P. D., and Moe, G. K.(I965). Some characteristics of ventricular echoes. Circula-tion Research, I6, 562.
Moe, G. K., Preston, J. B., and Burlington, H. (I956). Physio-logic evidence for a dual A-V transmission system. Circula-tion Research, 4, 35I.
Rosen, K. M., Mehta, A., and Miller, R. A. (I974). Demon-stration of dual atrioventricular nodal pathways in man.American Journal of Cardiology, 33, 291.
Rosenblueth, A. (1958). Ventricular 'echoes'. AmericanJ'ournal of Physiology, 195, 53.
Schuilenburg, R., and Durrer, D. (I969). Ventricular echobeats in the human heart elicited by induced ventricularpremature beats. Circulation, 40, 337.
Van Cappelle, F. J. L., Du Perron, J. C., and Durrer, D.(197I). Atrioventricular conduction in the isolated ratheart. Americanjournal of Physiology, 221, 284.
Wit, A. L., Weiss, M. B., Berkowitz, W. D., Rosen, K. M.,Steiner, C., and Damato, A. N. (I970). Patterns of atrio-ventricular conduction in the human heart. CirculationResearch, 27, 345.
Wu, D., Denes, P., Dhingra, R., Khan, A., and Rosen, K. M.(I974). The effect of propranolol on induction of A-Vnodal re-entrant paroxysmal tachycardia. Circulation, 50,665.
Requests for reprints to Dr. Pablo Denes, Section ofCardiology, University of Illinois Hospital, P.O. Box6998, Chicago, Illinois 6o68o, U.S.A.
on 8 April 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.10.1069 on 1 October 1975. D
ownloaded from





























