Embed Size (px)
Citation preview

Drugs Used For Affective Drugs Used For Affective DisordersDisorders
By By
Prof. Abdulqader AlhaiderProf. Abdulqader Alhaider

Definition of Affected DisordersDefinition of Affected Disorders Either Depresion or maniaEither Depresion or mania
Incidence: Depression is a chronic and Incidence: Depression is a chronic and recurrent illness that can affect at recurrent illness that can affect at least 20% of the population at some least 20% of the population at some period in their lifetime. An estimated period in their lifetime. An estimated 35-40 million Americans living today 35-40 million Americans living today will suffer from major Depressive will suffer from major Depressive Illness during their lives. Illness during their lives.

For each person directly suffering, For each person directly suffering, three or four times that number of three or four times that number of their relatives, employees, their relatives, employees, associates, and friends will also be associates, and friends will also be adversely affected.adversely affected.
Cost: 15-35 billions $/years in USA Cost: 15-35 billions $/years in USA
onlyonly. .

Symptoms of DepressionSymptoms of Depression The symptoms of Depressive Illness are highly The symptoms of Depressive Illness are highly
recognizable, both to those affected and to those recognizable, both to those affected and to those closest to them, once they are told what to look for. closest to them, once they are told what to look for.
Here is a checklist of symptoms of Depressive Here is a checklist of symptoms of Depressive illness: illness: – Loss of energy and interestLoss of energy and interest. . – Diminished ability to enjoy oneself. Diminished ability to enjoy oneself. – Decreased -- or increased -- sleeping or appetite. Decreased -- or increased -- sleeping or appetite. – Difficulty in concentrating; indecisiveness; Difficulty in concentrating; indecisiveness;
slowed or fuzzy thinking. slowed or fuzzy thinking. – Exaggerated feelings of sadness, hopelessness, Exaggerated feelings of sadness, hopelessness,
or anxiety. or anxiety. – Feelings of worthlessnessFeelings of worthlessness. . – Recurring thoughts about death and Recurring thoughts about death and suicidesuicide. . – If most of these symptoms last for two weeks or If most of these symptoms last for two weeks or
more, you probably have Depressive Illness. more, you probably have Depressive Illness. Sometimes depression alternates with "mania" Sometimes depression alternates with "mania" and is called and is called Manic-Depressive Illness Manic-Depressive Illness (Bipolar)(Bipolar). .

Symptoms of ManiaSymptoms of Mania causes mood swings creating periods causes mood swings creating periods
with the following symptoms: with the following symptoms: – A high energy level with A high energy level with decreased decreased
need for sleep. need for sleep. – Unwarranted or Unwarranted or exaggerated beliefexaggerated belief in in
one's own ability. one's own ability. – Extreme irritability. Extreme irritability.
– Rapid, Rapid, unpredictable emotional unpredictable emotional changechange. .
– Impulsive, thoughtless activity, with a Impulsive, thoughtless activity, with a high risk of damaging consequences high risk of damaging consequences (i.e., stock speculations, sudden love (i.e., stock speculations, sudden love affairs, etc.). affairs, etc.).

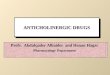
Affective DisordersAffective Disorders SerotoninSerotonin
NENE NE NE
ManiaMania Depression Depression
Rx Rx Drugs that decrease NEDrugs that decrease NE Drugs that increase NEDrugs that increase NE
What is the evidence to support this theory ?What is the evidence to support this theory ?Amphetamine and mania while Clonidine and methyldopa produce Amphetamine and mania while Clonidine and methyldopa produce
depression.depression.
Figure 1:Biochemical Theory of Affective Disorders.

What are the features of drugs that What are the features of drugs that are to be used for Rx of Depression?are to be used for Rx of Depression?

Classification of Antidepressants Classification of Antidepressants Based on Site of Action (see Fig 29-2)Based on Site of Action (see Fig 29-2) A ) A ) Drugs that Block the RE-uptake of NE and Drugs that Block the RE-uptake of NE and
5- 5- HT HT ( e.g.:Most tricyclics)( e.g.:Most tricyclics)
B)B) Drugs that Selectively Block Re-Uptake of Drugs that Selectively Block Re-Uptake of 5-5- HT (SSRIs) HT (SSRIs) (Fluoxetine; Paroxetine; (Fluoxetine; Paroxetine; Sertraline; Sertraline; Citalopram)Citalopram)
C)C) Drugs that Block Presynaptic Drugs that Block Presynaptic αα22--adrenoceptors adrenoceptors (e.g.: Mirtazapine, Mianserin).(e.g.: Mirtazapine, Mianserin).
D)D) Drugs that Inhibit MonoAminoOxidase Drugs that Inhibit MonoAminoOxidase (MAOIs, (MAOIs, Phenelzine, Tranylcypraine, Phenelzine, Tranylcypraine, MoclobemideMoclobemide))


Mechanism of Action of AntidepressantsMechanism of Action of Antidepressants1) Inhibition of reuptake of NE and or 5-HT ?? or 1) Inhibition of reuptake of NE and or 5-HT ?? or increases the release of NE or 5-HT. ???increases the release of NE or 5-HT. ???
2) Desensitization (down-regulation) of 2) Desensitization (down-regulation) of ββ- - adrenoceptors (decrease c-AMP). (very adrenoceptors (decrease c-AMP). (very important and related to clinical response). important and related to clinical response).
How do SSRIs desensitize How do SSRIs desensitize ββ-adrenoceptors?-adrenoceptors? Hint: Remember Raphe nuclei!!Hint: Remember Raphe nuclei!!

Tricyclic Antidepressants (TCAs)Tricyclic Antidepressants (TCAs)
e.g.: Imipramine; Amitriptyline ; Desipramine; e.g.: Imipramine; Amitriptyline ; Desipramine; Doxepin (see Table 1). Doxepin (see Table 1).

Pharmacological Actions of TCAs:Pharmacological Actions of TCAs:
Monoamineuptake (see Table 1)Monoamineuptake (see Table 1)Which one of them selectively blocks NE?Which one of them selectively blocks NE?
Side effects of TCA (see table 2 )Side effects of TCA (see table 2 ) Note:Note: They are drugs with broad spectrum of They are drugs with broad spectrum of
pharmacological effects at many receptors (e.g. pharmacological effects at many receptors (e.g. Histamine ; ACH therefore, they are also associated Histamine ; ACH therefore, they are also associated with many side effects) (see table 2).with many side effects) (see table 2).– Sedation Why? Sedation Why? – Cardiovascular effects (Tachycardia and hypotension) Cardiovascular effects (Tachycardia and hypotension)
How? How? – Anticholinergic effectsAnticholinergic effects– Weight gain.Weight gain.– SeizureSeizure– HypomaniaHypomania

Table 1: Effects of tricyclic antidepressants on Table 1: Effects of tricyclic antidepressants on Reuptake and 5-HTReuptake and 5-HT22
Tricyclic antidepressantsTricyclic antidepressants 5-HT reuptake5-HT reuptake Noradrenaline Noradrenaline reuptakereuptake
5-HT2 antagonism5-HT2 antagonism
Tricyclic antidepressantsTricyclic antidepressantsAmitriptylineAmitriptyline
ClomipramineClomipramine
DesipramineDesipramineDothiepinDothiepin
DoxepinDoxepin
Imiprmine Imiprmine
LofipramineLofipramine
Nortriptyline Nortriptyline
+ + + +
++
??
--
++
++
--
++
--
++++
++
++
++
++
++
++
??
--
--
++
--
--
++
Which one of the tricyclics is more selective on inhibiting reuptake of NE?Which one of the tricyclics is more selective on inhibiting reuptake of 5-HT?

Table 2: Side Effects of Tricyclic antidepressantsTable 2: Side Effects of Tricyclic antidepressants
Relative Side effectsRelative Side effects Reuptake inhibitionReuptake inhibition
SedationSedation Cardio-Cardio-toxicitytoxicity
HypotensionHypotension Anti-Anti-CholinnergicCholinnergic
NENE 5-HT5-HT
AmitriptylineAmitriptyline
AmoxapineAmoxapine
ClomipramineClomipramine
DesipramineDesipramine
DothiepinDothiepin
DoxepinDoxepin
ImipramineImipramine
LofepramineLofepramine
NortriptylineNortriptyline
ProtriptylineProtriptyline
TrimipramineTrimipramine
++++++
++++
++++
++
++++++
++++++
++++
++
++
--
++++++
++++++
++
++++++
++++++
++++++
++++
++++++
++
++++
++++++
++++++
++++++
++
++++
++
++++
++++
++++++
++
0/+0/+
++
++++
++++++
++++
++++
++++
++++
++++
++++++
++
++++
++++
++++
++++
++++++
+/-+/-
++++++++
++
++
++
++++++++
++++++
++++++++
++
++++++
++
++++++
+/-+/-
++
++
++++++
++
++
++
++

•Pharmacokinetics:Pharmacokinetics:• Lipophilic Lipophilic with High protein binding; basic in nature, with High protein binding; basic in nature, metabolized in livermetabolized in liver. .
• Nowadays, this group of antidepressants became less Nowadays, this group of antidepressants became less popular than it was, due to the unwanted effects.popular than it was, due to the unwanted effects.
•Treatment of overdose of Tricyclic AntidepressantsTreatment of overdose of Tricyclic Antidepressants
Why hemodialysis is not effective for Rx of TCA Why hemodialysis is not effective for Rx of TCA toxicity?. toxicity?.

Selective Serotonin Uptake Blockers Selective Serotonin Uptake Blockers (SSRI)(SSRI)
e.g. Fluoxetine; Fluvoxamine; Paroxetine; e.g. Fluoxetine; Fluvoxamine; Paroxetine; Sertraline; Citalopram (see table 3).Sertraline; Citalopram (see table 3).
Pharmacological Activities:Pharmacological Activities:
MOA : Selective uptake of 5-HT in the MOA : Selective uptake of 5-HT in the presynaptic cleft. presynaptic cleft.
Why they are better choice as comparedWhy they are better choice as compared to to TCA?TCA?

Table 3: Effect of SSRIs on Reuptake and 5-HT2Table 3: Effect of SSRIs on Reuptake and 5-HT2
5-HT reuptake5-HT reuptake Noradrenaline Noradrenaline reuptakereuptake
5-HT2 5-HT2 antagonistsantagonists
Selective serotonin reuptake Selective serotonin reuptake inhibitorsinhibitors
CitalopramCitalopram
FluoxetineFluoxetine
FluvxamineFluvxamine
ParoxetineParoxetine
SertralineSertraline
++
++
++
++
++
--
--
--
--
--
--
--
--
--
--
What is the clinical significant of the antagonistic effect on 5-HT2 receptors?

Side Effects of SSRI (see Table 4)Side Effects of SSRI (see Table 4) Almost have no cardiovascular manifestations as Almost have no cardiovascular manifestations as
compared to TCA.compared to TCA. Nausea and vomiting and decrease appetite How?Nausea and vomiting and decrease appetite How?
Insomnia and anxiety (with Fluoxetine ; Citalopram; but Insomnia and anxiety (with Fluoxetine ; Citalopram; but not with Paroxetine. So What? not with Paroxetine. So What?
Impotence and sexual dysfunction (in male and female) Impotence and sexual dysfunction (in male and female)
How these occur and what are their clinical significant How these occur and what are their clinical significant ??
Decrease weight. How?Decrease weight. How?

Side effects of SSRIs cont’dSide effects of SSRIs cont’d
Nausea; vomiting and anorexia. How Nausea; vomiting and anorexia. How ?? Can SSRIs be used together with TCA Can SSRIs be used together with TCA ??
Drugs interactions due to their significant inhibitory Drugs interactions due to their significant inhibitory action at CYP450 (Except Citalopram.) action at CYP450 (Except Citalopram.)
Which one of SSRIs does produce active metaboliteWhich one of SSRIs does produce active metabolite??
Which one has the longest tWhich one has the longest t1/21/2 ??

Drug Cardiotoxicty Nausea Anticholinergic SedationDrug Cardiotoxicty Nausea Anticholinergic Sedation
effectseffects
Citalopram Citalopram ? ++ _ _ ? ++ _ _
FluoxetineFluoxetine - ++ _ _ - ++ _ _
FluvoxamineFluvoxamine _ +++ _ + _ +++ _ +
Paroxetine Paroxetine _ ++ + + _ ++ + +
SertralineSertraline _ ++ _ _ _ ++ _ _
Table 4: Side effects of SSRIs

αα22 – adrenoceptors antagonists – adrenoceptors antagonists
e.g. Mirtazepine (Romeron ®); Mianserine.g. Mirtazepine (Romeron ®); Mianserin
act by increasing the release of 5-HT and NEact by increasing the release of 5-HT and NE
Via………Via………
Differ from SSIR in Differ from SSIR in
Increase appetite (good for patients taking Increase appetite (good for patients taking cancer chemotherapy) NO N/V why? No cancer chemotherapy) NO N/V why? No Sexual dysfunction Why ? ; sedation. Also, Sexual dysfunction Why ? ; sedation. Also, produces constipation and rarely leads to produces constipation and rarely leads to agranulocytosis agranulocytosis

Other non classified AntidepressantsOther non classified Antidepressants
Venlavaxine (Venlavaxine (EffexorEffexorRR)): Act by blocking 5-: Act by blocking 5-HT and NE uptake but it has side effects HT and NE uptake but it has side effects profile similar to SSRI. However, it may profile similar to SSRI. However, it may produce seizure and constipation. Why?produce seizure and constipation. Why?
Desvenlafaxine Desvenlafaxine PristiqR PristiqR (metabolite of Venlavaxine)(metabolite of Venlavaxine)
Trazodone: Selective blocker of 5-HT uptake Trazodone: Selective blocker of 5-HT uptake but has significant but has significant αα- blocking effect - blocking effect (hypotension and sedation); Blocks 5-HT2 (hypotension and sedation); Blocks 5-HT2 receptors receptors (Priapism(Priapism))

Table 5: Effects of atypical antidepressants on Table 5: Effects of atypical antidepressants on Reuptake and 5-HT2Reuptake and 5-HT2
5-Ht reuptake5-Ht reuptake Noradrenaline Noradrenaline reuptakereuptake
5-HT2 antagonism5-HT2 antagonism
AmoxapineAmoxapine
BuproprionBuproprion
MaprotilineMaprotiline
MianserinMianserin
NafazodoneNafazodone
NomifensineNomifensine
TrazodoneTrazodone
VenlafaxineVenlafaxine
--
--
--
--
-/+-/+
--
++++
++
++
--
++
--
--
++
--
++
++
--
--
++
++
--
++
--

Nefazodone:Nefazodone: Structurally related to trazodone Structurally related to trazodone but does not has the sedative effect and does but does not has the sedative effect and does not block not block αα- adrenoceptors , however; it likes - adrenoceptors , however; it likes most SSRI inhibit P450 3A4 isoenzyme.most SSRI inhibit P450 3A4 isoenzyme.

3. Monoamine Oxidase Inhibitors:3. Monoamine Oxidase Inhibitors: History: The anti TB Iproniazide exhibited History: The anti TB Iproniazide exhibited mood elevating properties and latter found to mood elevating properties and latter found to inhibit MOA.inhibit MOA.

Table 6: Side effects of atypical Table 6: Side effects of atypical antidepressantsantidepressants
DrugDrug Toxicity Toxicity SedationSedation HypotensionHypotension Anticholinergic Anticholinergic effectseffects
MianserinMianserin
MirtazepineMirtazepine
NefazodoneNefazodone
TrazodoneTrazodone
VenlafaxineVenlafaxine
--
--
--
++
++
++++
++++
++
++++++
++++
--
--
++
++++++
--
++
++
--
--
++

Classifications of MAOIsClassifications of MAOIs
Either:Either:
Hydralazine Derivatives (Hydralazine Derivatives (PhenelzinePhenelzine (Nardil®) (Nardil®)
Non –hydralazine DER.(Non –hydralazine DER.(TranylcypramineTranylcypramine (Parnate®) (Parnate®)
Or as Or as irreversibleirreversible non –selective (Phelzine and non –selective (Phelzine and Tranylcypramine) vs Tranylcypramine) vs reversible selective reversible selective ( Mclobemide)( Mclobemide)
Side EffectsSide Effects::↑ ↑ appetite appetite (Phenelzine like) (Phenelzine like) ↓ ↓ appetite appetite (Tranylcypramine; hepatotoxicity; SLE like;(Tranylcypramine; hepatotoxicity; SLE like;
Drug and Food interactions (very important).Drug and Food interactions (very important).

DrugDrug SedationSedation Anticholinergic Anticholinergic effectseffects
HypotensinHypotensin
Non-selective Non-selective irreversibleirreversible
IsocarboxazidIsocarboxazid
PhenelzinePhenelzine
TranylcypromineTranylcypromine
++
++
--
--
++++
++++
++
--
++
++
++
--Selective Selective reversiblereversible MoclobemideMoclobemide

Clinical uses of Antidepressant Drugs.Clinical uses of Antidepressant Drugs.
A.A. Endogenous Depression ( SSRIs (first Choice) Tricyclics.Endogenous Depression ( SSRIs (first Choice) Tricyclics.
B.B. Panic Disorders ( Imipramine or SSRIs)Panic Disorders ( Imipramine or SSRIs)
C.C. Obsessive Compulsive Disorders (SSRIs Clomipramine),Migraine; Obsessive Compulsive Disorders (SSRIs Clomipramine),Migraine; Chronic pain, IBS and Anxiety (Amityiptyline)Chronic pain, IBS and Anxiety (Amityiptyline)
D.D. Anorexia nervosa and Bulemia (SSRIs)Anorexia nervosa and Bulemia (SSRIs)
E.E. Schizo-Afective Disorders (Amoxapine or SSRI + Haloperidol)Schizo-Afective Disorders (Amoxapine or SSRI + Haloperidol)
F.F. Premature ejaculationPremature ejaculation
G.G. Anxiety disordersAnxiety disordersH.H. Migraine Migraine I.I. Nocturnal Enuresis in children e.g. Imipramine Nocturnal Enuresis in children e.g. Imipramine

Drugs for maniaDrugs for mania e.g. Lithium carbonate; Valproic Acid; e.g. Lithium carbonate; Valproic Acid;
Lamotrigine; Carbamazipine; GabapentinLamotrigine; Carbamazipine; Gabapentin
LITHIUM :LITHIUM : MOA : Remember its similarity to sodium MOA : Remember its similarity to sodium
thus it:thus it:-- inhibits the release of NEinhibits the release of NE-- Increases re-uptake of NEIncreases re-uptake of NE
-- Decreases second messenger in Decreases second messenger in postsynaptic postsynaptic neurons (decrease c-AMP; neurons (decrease c-AMP; IP3 and DAG))IP3 and DAG))

Side effectsSide effects
1) Endocrine side effects1) Endocrine side effects-- Nephrogenic Diabetes insipidus (antagonize the activity of ADH Nephrogenic Diabetes insipidus (antagonize the activity of ADH via via inhibition of c-AMP).inhibition of c-AMP).-- HypothyroidismHypothyroidism
2) Other Side effects:2) Other Side effects:-- Irreversible renal damage (very important) N/V; Mental Irreversible renal damage (very important) N/V; Mental confusion; confusion; leucocytosis; and congenital cardiac anomalies (Ebsteins leucocytosis; and congenital cardiac anomalies (Ebsteins
Malformation)Malformation)
Clinical UsesClinical Uses::
- Rx of mania; Bipolar depression - Rx of mania; Bipolar depression - SIADH ; Hyperthyroidism ?- SIADH ; Hyperthyroidism ?
- Schizophrenia - Schizophrenia - Leucopenia - Leucopenia

– Plasma level :Plasma level : Therapeutic level 1.2 – 1.4 mg/lTherapeutic level 1.2 – 1.4 mg/l Prophylactic level = 0.5-0.8 mg /lProphylactic level = 0.5-0.8 mg /l Lithium takes 3-4 days to act, thus sedative and calming Lithium takes 3-4 days to act, thus sedative and calming
drugs like haloperidol I.V should be given at ER.drugs like haloperidol I.V should be given at ER.
Drug interactions:Drug interactions: Plasma level of Lithium and toxicity, increase in: Plasma level of Lithium and toxicity, increase in:
– Lithium + low salt dietLithium + low salt diet– Lithium + diureticsLithium + diuretics- Lithium + NSAIDs- Lithium + NSAIDs– PostpartumPostpartum

Why lithium is not popular as before?Why lithium is not popular as before?
What are the alternatives of lithium? What are the alternatives of lithium?
Why?Why?
Lithium and pregnancy?Lithium and pregnancy?

Signs and symptoms of Lithium Signs and symptoms of Lithium Toxicity Toxicity
Mild to moderate intoxication ( lithium livel 1.5 -2 Mild to moderate intoxication ( lithium livel 1.5 -2 mEq/l)mEq/l)
Gastrointestinal:Gastrointestinal: -- VomitnigVomitnig
-- Abdominal painAbdominal pain -- Dryness of mouthDryness of mouth Neurological :Neurological :
-- AtaxiaAtaxia -- DizzinessDizziness -- Slurred speechSlurred speech -- NystagmusNystagmus
-- Lethargy or excitementLethargy or excitement-- Muscle weaknessMuscle weakness

Moderate to severe Moderate to severe intoxicationintoxication
(Lithium level 2.0-2.5 mEq /l)(Lithium level 2.0-2.5 mEq /l) Gatrointestinal:Gatrointestinal:
-- Anorexia nervosaAnorexia nervosa-- Persistent nausea and vomitingPersistent nausea and vomiting
Neurological :Neurological :-- Blurred visionBlurred vision-- Muscle fasciculationsMuscle fasciculations-- Clonic limb movementsClonic limb movements-- Hyperactive deep tendon reflexesHyperactive deep tendon reflexes-- Choreoathetoid movementsChoreoathetoid movements-- convulsionsconvulsions-- DeliriumDelirium-- SyncopeSyncope-- Electroencephalographic changesElectroencephalographic changes-- StuperStuper-- ComaComa

Circulatory failure ( lowered blood pressure, Circulatory failure ( lowered blood pressure, cardiac arrhythmias, and conduction cardiac arrhythmias, and conduction abnormalities.abnormalities.
Severe intoxicationSevere intoxication
(Litium level < 2.5 mEq /l)(Litium level < 2.5 mEq /l)
-- Generalized convulsions Generalized convulsions
-- Oliguria and renal failure Oliguria and renal failure
-- DeathDeath