Drugs and the Kidney 1.Drugs and the normal kidney 2.Drugs
toxic to the kidney 3.Prescribing in kidney disease 4.Case
presentation
Slide 3
Normal Kidney Function 1 Extra Cellular Fluid Volume control 2
Electrolyte balance 3 Waste product excretion 4 Drug and hormone
elimination/metabolism 5 Blood pressure regulation 6 Regulation of
haematocrit 7 regulation of calcium/phosphate balance (vitamin D3
metabolism)
Slide 4
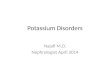
Pharmacokinetics Absorption Distribution Metabolism Elimination
filtration secretion
Slide 5
Drugs and normal kidney
Slide 6
Slide 7
Slide 8
Effects of renal disease on drugs
Slide 9
Slide 10
Patient related risk factors for drug-induced nephrotoxicity
Absolute or effective intravascular depletion Age older than 60
years Diabetes Exposure to multiple nephrotoxins Heart failure
Sepsis Underlying renal insufficiency (glumerular filtration
rate
Effect of dialysis on drugs Drugs with MW >500 daltons
poorly cleared by conventional HD membranes. Protein or tissue
binding or lipid soluble are not dialyzed properly. For drugs not
removed by HD, it is unusual to be removed by peritoneal dialysis.
High-flux membranes (porous) are more permeable to drugs.
Slide 47
Acetaminophen Angiotensin-converting enzyme inhibitors
Angiotensin receptor blockers Adriamycin Allopurinol Amiodarone
Amoxapine Azathioprine Benzodiazepines -Blockers Bupropion
Buspirone TABLE 57-2 -- Drugs That Have Active or Toxic Metabolites
in Dialysis Patients Cardiac glycosides Clorazepate Cephalosporins
Chloral hydrate Clofibrate Desipramine Diltiazem Encainide Esmolol
H 2 -blockers Hydroxyzine Imipramine
Slide 48
Isosorbide Levodopa Lorcainide Meperidine Metronidazole
Methyldopa Miglitol Minoxidil Morphine Nitrofurantoin Nitroprusside
Procainamide Primidone TABLE 57-2-- Drugs That Have Active or Toxic
Metabolites in Dialysis Patients cont.. Propoxyphene Pyrimethamine
Quinidine Serotonin reuptake inhibitors Spironolactone
Sulfonylureas Sulindac Thiazolidinediones Triamterene Trimethadione
Verapamil Vidarabine
Slide 49
Slide 50
B & C- ACEIs and ARB Angiotensin converting enzyme
inhibitors (ACEI) and angiotensin receptor blocker (ARB) are
inhibiting Renin system and decrease the blood hemodynamic: It
produces VD and decrease perfusion pressure and decreases GF At the
start of the treatment a decrease of urine volume and increase of
creatinine by 30% indicates Damage is reversible Rehydration of
patient is advisable Initiate treatment with short acting
(captopril) and titrate later with long acting
Prescribing in Kidney Disease Patients with renal impairment
Patients on Dialysis Patients with renal transplants
Slide 54
Dosing in renal impairment Loading dose does not change
(usually) Maintenance dose or dosing interval does T often
prolonged Reduce dose OR Increase dosing interval Some drugs have
active metabolites that are themselves excreted renally Warfarin,
diazepam
Slide 55
References Clinical Pharmacology: Melmon and Morrelli,
McGraw-Hill, 2000 Taber SS and Pasko, Epidemiology of drug- induced
disorders: the kidney; Exper.Opin.Drug Saf. 7(6):679-690, 2008
Hanbook of dialysis therapy: Nissenson and Fine, Sunders Elsevier,
philadelphia, 4 th edition, 2008, (83): 1089-1195 The Kidney at a
glance: Ocallaghan and Brenner, blackwell Science,2000:38-39 Burton
Rose, drug-induced nephrotoxicity, Uptodate 20.1 2012
Slide 56
case1 A 54 y/o female with resistant ALL received IV
Methotraxate for 3 days. After 3-4 days she developed nausea,
vomiting and azotemia was diagnosed. She had hypocalcemia,
hyperphosphatemia hyperuricemia and hyperkalemia. In lab exam also
severe keukopenia and pancytopenia was found. She received G-CSF,
leukoverin, Hemodialysis and Antibiotics. Dx?
Slide 57
case2 A 65 y/o female with chronic hypertension developed fever
39 c and dysuria, flank pain. In U/A and U/C pyuria and E-Coli
100000 cc was reported. She received 500 mg amikacin stat and 250
mg tid IM. Her serum Cr was 1.5 mg/dl and BUN 26, her body weight
was 50 kg. What is your opinion about this prescription?
Slide 58
Case2 Cr Clearance= (140-age)x BW (kg)/85 x serum Cr Cr
Clearance= 75 x 50/85 x 1.5 Cr Clearance= 3750 / 127.5 Cr
Clearance= 30 ml/min What is your prescription?
Slide 59
Case3 A 38 y/o man with uncontroled hypertension and serum Cr =
2 mg/dl and BUN 28 mg/dl is candidate for renal artery MRA with
gadolinium, his BW is 72 kg. What is your opinion? Could he do the
MRA? What is his estimated GFR?
Slide 60
Case3 Cr Clearance= (140-age)x BW (kg)/85 x serum Cr Cr
Clearance= 140 38 x 72/72 x 2 Cr Clearance= 102x 72/ 144 Cr
Clearance= 51ml/min
Slide 61
case4 A 47 y/o diabetic male with IHD and Chest pain is
candidate for coronary angiography; his serum Cr is 2.5 mg/dl and
BW is 85kg. He is consulted for using contrast. What is your
suggestion? Can he use contrast? Does he need prophylctic
dialysis?