Embed Size (px)
Citation preview

Drugs in dyslipidaemias
Dr Sanjeewani Fonseka
Department of Pharmacolgy

Atheroma
• Focal disease of intima
• Deposition of C in arterial wall

Atheromatous disease
• myocardial infarction
• Cerebo vascular accidents

Synthesizedby liver
LipidsExo
Endo
TAG
FFA FFA
chy remnant Cleared
byliver
VLDL LDL
(+ cholesterol)Liver - bile
Cell membrane
HDL
chy
Skeletal, cardiac and adipose tissue

Dyslipidaemias
• Hypercholesterolaemia
• Hypertriglyceridaemia
• Mixed dyslipidaemia

Dyslipidaemias
Primary
• Genetically
• Cassify according to
lipoprotein particle
Secondary
• DM• Alcohol• Nephrotic• CRF• Hypothyroidism• Liver disease• Drugs

Drugs in dyslipidaemias
• Statins
• Fibrates
• Bile acid binding resins
• Niacin
• Inhibitors of cholesterol absorption
• Omega-3 fatty acids

Drugs in dyslipidaemias
• Statins
• Fibrates
• Bile acid binding resins
• Niacin
• Inhibitors of cholesterol absorption
• Omega-3 fatty acids

Statins
• Competitive inhibition of HMG CoA reductase
• HMG Co A HMG Co A mevalonic acid
reductase
• Reduced C in the liver
• ↑ Expression of LDL receptor
• Increased LDL clearance

• Activation of sterol regulatory element binding protein 2 (SREBP2)
• ↑ Expression of gene encoding LDL receptor

Other effects of statins
• Improve endothelial function
• Decreased coagulation
• Decreased inflammation
• Improved stability of atherosclerotic plaques
statin cont;

statin cont;
• Well absorbed
• Metabolized in liver
• Extensive pre- systemic metabolism

Statins
• ↓ LDL-cholesterol by 25-55%
• ↑ HDL-cholesterol by 5%
• ↓ triglycerides by 10-35%
• Given once daily (nocte)
statin cont;

Statins
• Lovastatin
• Pravastatin
• Simvastatin
• Fluvastatin
• Atorvastatin
• Rosuvastatin
statin cont;

statin cont;
Clinical use
• Primary prevention
• Secondary prevention

Statins: adverse effects
• Hepatotoxicity
• Myotoxicity
• Dyspepsia, abdominal pain, diarrhoea
• Angioedema
statin cont;

Statins: hepatotoxicity
• Asymptomatic
• ↑ ALT, AST
• First 6 months
• Discontinued if ALT / AST > 3 times the upper limit of normal range
statin cont;

Statins: myotoxicity
• Pain / tenderness, weakness
• ↑ CK > 10 times upper limit of normal
• Reversible
• ↑ risk with concurrent fibrate therapy, hypothyroidism, renal insufficiency
statin cont;

Drugs in dyslipidaemias
• Statins
• Fibrates
• Bile acid binding resins
• Niacin
• Inhibitors of cholesterol absorption
• Omega-3 fatty acids

Fibrates
• Activate peroxisome proliferator-activated receptor-α (PPARα)
• Heterodimer binds to peroxisome proliferator response elements (PPREs) in the promoter regions of specific genes
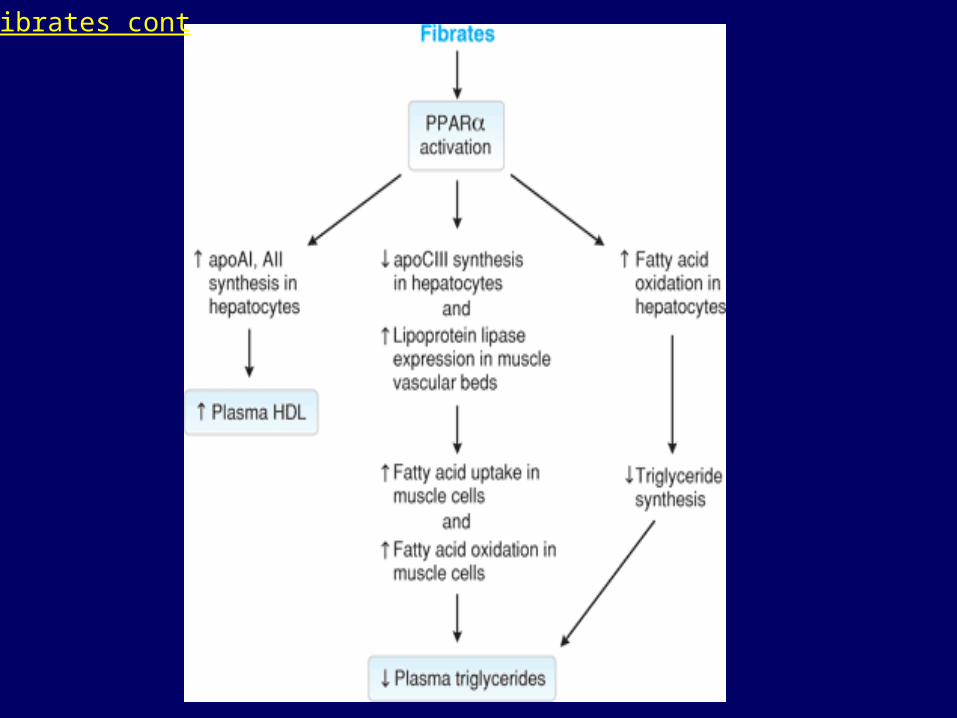
Fibrates cont

Fibrates cont:
• Gemfibrozil, fenofibrate
• ↓ LDL-cholesterol by 5-20%
• ↑ HDL-cholesterol by 10-35%
• ↓ triglycerides by 20-50%

Clinical use
• Mixed dyslipidaemia
• Low HDL
Fibrates cont

• Well absorbed
• Elimination renal
Fibrates cont

Fibrates: adverse effects
• Gastrointestinal discomfort
• Myopathy
• ↑ liver transaminases
• Gallstone formation (Gemfibrozil)
• Displace warfarin from albumin binding sites
Fibrates cont

Drugs in dyslipidaemias
• Statins
• Fibrates
• Bile acid binding resins
• Niacin
• Inhibitors of cholesterol absorption
• Omega-3 fatty acids

Bile acid binding resins
• Cationic polymer resins that bind
non-covalently to negatively-charged bile acids in small intestine
• Enterohepatic circulation of bile acids interrupted causing up-regulation of 7α-hydroxylase in hepatocytes

Bile acid binding resins cont;

Bile acid binding resins cont
• Increased expression of the LDL receptor
• Concurrent up-regulation of hepatic cholesterol and triglyceride synthesis

Bile acid binding resins cont
• Cholestyramine, colestipol
• ↓ LDL-cholesterol by 15-30%
• ↑ HDL-cholesterol by 3-5%
• Triglycerides: no effect or ↑

• Not absorbed from GIT
• Bloating & dyspepsia
• Decreased absorption of digoxin, warfarin, fat-soluble vitamins
• Take one hour before or 4 h after colestyramine
Bile acid binding resins cont
Drugs in dyslipidaemias
• Statins
• Fibrates
• Bile acid binding resins
• Niacin
• Inhibitors of cholesterol absorption
• Omega-3 fatty acids

Niacin
• Also known as nicotinic acid
• ↓ LDL-cholesterol by 5 – 25%
• ↑ HDL-cholesterol 15 – 35%
• ↓ Triglycerides by 20 – 50%
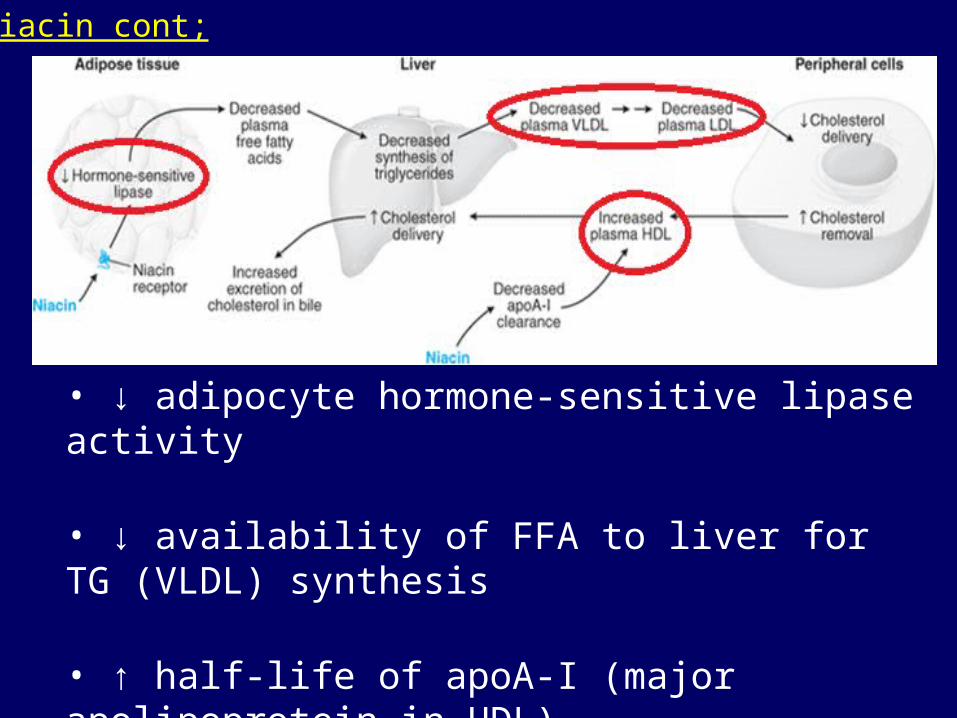
• ↓ adipocyte hormone-sensitive lipase activity
• ↓ availability of FFA to liver for TG (VLDL) synthesis
• ↑ half-life of apoA-I (major apolipoprotein in HDL)
Niacin cont;

adverse effects
• Cutaneous flushing & pruritus
• Release of prostaglandins D2 & E2
• Prevented by aspirin
• Extended-release formulations associated with less flushing
• hyperuricaemia, impaired insulin sensitivity, myopathy
Niacin cont;

Drugs in dyslipidaemias
• Statins
• Fibrates
• Bile acid binding resins
• Niacin
• Inhibitors of cholesterol absorption
• Omega-3 fatty acids

Inhibitors of cholesterol absorption
• Ezetimibe
• Decreases cholesterol transport from micelles into enterocytes by inhibiting brush border protein NPC1L1
• Reduces cholesterol incorporation into VLDL in liver

Inhibitors of cholesterol absorption
• rapidly absorbed by enterocytes
• Eliminated in bile
• Undergoes enterohepatic circulation
• Clinical benefit uncertain

Drugs in dyslipidaemias
• Statins
• Fibrates
• Bile acid binding resins
• Niacin
• Inhibitors of cholesterol absorption
• Omega-3 fatty acids

Omega-3 fatty acids
• Eicosapentaenoic acid (EPA)
• Docosahexaenoic acid (DHA)

• Reduce triglycerides
• Increase C
• Benefit - uncertain

Summary
• Most important hyperlipidaemia is hypercholesterolaemia
• Most effective drug – statin
• Drugs reduce risk of MI































