Embed Size (px)
Citation preview

The Visceral Leishmaniasis (VL) Global R&D & Access Initiative
Drugs for Neglected Diseases initiative (DNDi)
Contact:
Alexandra Heumber

Project title: The Visceral Leishmaniasis (VL) Global R&D & Access Initiative
Project summary:*
This proposal recommends as a candidate demonstration Project the creation of the VL Global R&D &
Access Initiative that will demonstrate that VL R&D projects can be optimized through guiding principles such as cross-regionals collaboration of existing networks (see Annex 3), open-innovation
and sharing knowledge, equitable access to new products, and sustainable funding secured through
existing and new funding mechanisms.
Considering the current VL R&D landscape, the existing drug portfolio (see below) and the current
treatments limitations mentioned above, for this project DNDi will focus on the following strategy over the next five years (see table below summarizing the objectives related to the treatment limitation):
Objective 1: to develop new safe and effective oral treatments as monotherapy and as early as possible as
combination treatment (medical product) to prevent the risk of resistance development for the treatment of VL patients and a very safe, short-course one for asymptomatic carriers once their role in disease
transmission has been better established:
Activity 1: to identify new series of compounds and to select candidates for promising NCEs
from lead-optimization program to pre-clinical (class of Oxaborole; class of Nitromidazole;
Dundee/GSK); Activity 2: to bring from preclinical to POC a new drug candidate (VL2098);
Activity 3: to complete the clinical development of existing candidate up to registration
(Fexinidazole or VL 2098) as monotherapy and as soon as possible as combination treatment.
Objective 2: to develop technology of diagnostic (xenodiagnoses coupled with a quantitative PCR) in
order to evaluate the role in transmission of asymptomatic carriers and PKDL patients:
Activity 1: set-up of sand fly colonies and training on xenodiagnoses and quantitative PCR. Activity 2: small clinical study evaluating the infectivity of asymptomatic careers and PKDL
patients.
Objective 3: to develop treatment for PKDL (medical product): Activity 1: start and complete clinical development of new regimen of treatments that
demonstrate skin penetration for the current treatment of PKDL patient.
Objective 4: the contribution to the development of a shared, open-access data base that will allow
identifying determinants of treatment effectiveness that will be based on existing ones developed for
malaria.
The project is based on an optimization and coordination of already existing initiatives in order to
reduce the time, costs and efficiency necessary to achieve the goal of development new tools for the
treatment of VL.
The guiding principles of the Initiative are defined as:
1. Sharing knowledge and Open innovation Open knowledge platform through the establishment of a Drug Accelerator Consortium -which could be supported by the Innovative Medicines Initiative (IMI)/Horizon 2020 - will be a key asset to speed up
upstream research, avoid duplication of research and decrease cost of R&D development: partners within
the Drug Accelerator platform will agree to screen their libraries together increasing chance to identify
good hits for later optimization. Other institutions and researchers from different Initiatives and networks (listed in Annex 3) would agree
ensuring open knowledge sharing, similar to the Open Source Drug Discovery (OSDD) set up in India3
part of the Council of Scientific and Industrial Research (CSIR).
2. Sustainable funding In addition to existing resources involved in the support of VL, new funding mechanisms would be
needed to increase resources such as the European and Developing Countries Clinical Trials Partnership
(EDCTP 2), Innovative Medicines Initiative (IMI), contributions from emerging economies countries
affected by the disease (Brazil, India, Middle-East and North Africa) and Prizes.
3. Equitable access To ensure affordable access replicate the industrial model based on agreement signed with pharmaceutical company for one project for example contract signed with Sanofi for fexinidazole. It makes new
therapeutic and diagnostic tools developed as public goods and ultimately available at affordable prices.
4. Coordination through collaborative approach Setting up the VL Global R&D & Access Initiative in partnership with the current VL consortia and
research platforms from the different relevant regions (see Annex 3).
Details about the functioning of the Initiative:
The Initiative for VL would be composed of a steering committee selected among the representatives of the scientific community, key governments, main R&D partners, relevant regional WHO offices (SEARO,
PAHO, EURO, AFRO), DNDi, and the existing VL Initiatives (LEAP; Consortium for VL treatment in
India and Bangladesh; Consortium on HIV/VL in East Africa; Consortium on PKDL) supported by a
secretariat housed in an existing institution.
The Initiative would also work in partnership with relevant partners such as the EDCTP, IMI, the Council
of Scientific and Industrial Research (CSIR) including OSDD. The Secretariat will need to be committed to minimizing overhead costs and achieving value for money.
The responsibilities of the Initiative would be to: • Review and validate R&D priorities for VL disease
• Define priority treatment candidates
• Development and implementation of equitable access policy • Review and validate funding needs
• Identify potential funding mechanisms at country, regional, and international levels
• Review and validate proposals for innovative incentive mechanisms such as prizes • Review and propose regulatory, financial, and procurement policies to facilitate access to final products
• Monitor project implementation and results
• Review and validate financial reports
• Facilitate information sharing with national programs and regional initiatives • Appoint and have oversight of delegated activities of the Secretariat
*As taken from original proposal template, question 5.

Page 1 of 26
1.* Title of the project: The Visceral Leishmaniasis (VL) Global1 R&D & Access Initiative 2.* Submitted by: 3.* Target disease or health condition: (Focus on type II and III diseases and special R&D needs of developing Countries in type I disease where there is an identified health technology gap.)
Visceral Leishmaniasis (VL) occurs on five continents with endemic transmission reported in 98 countries. VL is one of the most neglected tropical diseases despite the fact that it is the most deadly parasitic disease after malaria. It comprises a complex vector-borne disease, caused by several species of the protozoan genus Leishmania and ranging from localised skin ulcers (then resulting in Cutaneous Leishmaniasis – not addressed here) to lethal systemic disease. This visceral form of the disease is the most severe and is lethal if left untreated2. VL disproportionately affects poor patients living in the poorest areas of the world such as the Bihar State in India, Bangladesh, remote areas of Sudan, Ethiopia, Kenya, Uganda, Latin American countries and to a lesser degree, other regions as the European and Mediterranean region (see map below). VL is transmitted by bites of a sandfly and is endemic in the regions, but can also occur in forms of epidemics (see section 6). The reservoir of the parasite is human (anthropoonotic) in Asia and Africa, but could be transmitted from vertebrate animals to humans (zoonotic) in Europe, Latin America and also Africa. In addition, recent scientific data has hypothesised on the additional possible role of asymptomatic patients (“carriers”) throughout the world, as well as of the role of patients presenting with a particular form of the disease present in Sudan and Asia (Post Kala Azar Dermal Leishmaniasis or PKDL). It is critical to understand all context of VL as if the hypothesis was confirmed, this means that alternative treatment options will be needed for these sub-groups of patients that are fuelling silent transmission of the disease. In patients who develop symptoms, presentation is insidious with development of splenomegaly, irregular fevers, anaemia, pancytopaenia, weight loss and weakness occurring progressively over a period of weeks or even months. Untreated, the disease is lethal. Current treatments have serious drawbacks in terms of safety, drug resistance, stability and cost and vary in specificity according to geographical region, as well as to clinical
1 For example in Spain, Leishmaniasis is hypoendemic (0.41 cases every 100,000 inhabitants) and is caused by Leishmania infantum. The dog is the main reservoir host. Between February 1982, when leishmaniasis was declared a notifiable disease, and December 1995 a total of 1,574 accumulated cases of leishmaniasis were reported. 2 Siqueira-Neto JL, Moon S, Jang J, Yang G, Lee C, et al. (2012) An Image-Based High-Content Screening Assay for Compounds Targeting Intracellular Leishmania donovaniAmastigotes in Human Macrophages. PLoSNegl Trop Dis 6(6): e1671. doi:10.1371/journal.pntd.0001671
Page 2 of 26
presentation of the disease (see Section 5). So it remains a challenging public health need in the endemic regions, and an increasingly health burden in the other regions such as In Europe (as Spain) where it seems to be re-emerging. East Africa pays a particular tribute as for instance the efficacy of the liposomal amphotericin B is below what it is in the Indian sub-continent for the same dosage, and to date, the only treatment option remains the association of 2 injectables ones limiting their large field use and also associated with some side effects. In addition severe PKDL is present in Sudan and HIV-VL co-infection in Ethiopia.
(Note that the role of animal and the control of transmission via animal reservoir is also of critical importance but not directly the scope of this project). This proposal as a candidate demonstration project recommends developing a coordinated strategy to cover the current R&D gaps of treatment and control of the human transmission of visceral Leishmaniasis through innovative mechanisms.
Complexity of treatment approaches for Visceral Leishmaniasis
1. Outside of the typical VL clinical patient, other clinical forms exist: a. asymptomatic patients – currently neither detected nor treated b. PKDL patients – another treatment is needed. Currently receiving long courses of
antimonials or high doses of liposomal amphotericin B – note that to date no VL treatment actually prevents the occurrence of PKDL but it is hoped that this would be the case of the NCEs
c. HIV co-infected patients – Experienced severe VL relapsed. Project on-going (AfricoLeish EU FP7)
2. Existing treatments options vary according to: a. Geographical region - response to drug treatment has been shown to vary between and
within regions: higher doses (of Ambisome® and paromomycin) are required to achieve efficacy in the East Africa and Latin America as opposed to South Asia foci. Geographical variation has also been shown within East Africa
b. Clinical forms as shown above. 3. Current treatment limitations: Lack of effective, safe and field-adapted 1st line oral treatments for
East Africa, Latin America and for the Indian sub-continent 4. Lack of understanding of the role of asymptomatic and PKDL patients in the transmission of the
disease – if confirmed, new approaches to control transmission will be required 5. Lack of global tools to identify determinants of treatment effectiveness and be used to also
monitor the development of resistance to existing treatments

Page 3 of 26
Geographical distribution of visceral leishmaniasis in the Old and New world
4. * The suggested health technology that project seeks to develop: (Eg. Medicine; diagnostic test: medical device; vaccine etc.)
The project aims, to cover some of the critical R&D gaps in order to provide supporting tools towards WHO elimination goals which focus on the Indian sub-continent (work on asymptomatic and PKDL patients) as well as to cover the urgent treatment needs for East Africa and Latin America (new treatment options).
- Objective 1: To develop new safe and effective oral treatments as monotherapy and as early as possible as combination treatment (medical product) to prevent the risk of resistance development and a very safe, short-course one for asymptomatic careers once their role in disease transmission has been better established.
- Objective 2: To develop technology of diagnostic (xenodiagnoses coupled with a quantitative PCR) in order to evaluate the role in transmission of asymptomatic careers and PKDL patients.
- Objective 3: To develop a treatment for PKDL (medical product). - Objective 4: To support development of a shared, open-access data base to identify
determinants of treatment effectiveness.
Page 4 of 26
5. * Project summary:
This proposal recommends as a candidate demonstration Project the creation of the VL Global R&D & Access Initiative that will demonstrate that VL R&D projects can be optimized through guiding principles such as cross-regionals collaboration of existing networks (see Annex 3), open-innovation and sharing knowledge, equitable access to new products, and sustainable funding secured through existing and new funding mechanisms. Considering the current VL R&D landscape, the existing drug portfolio (see below) and the current treatments limitations mentioned above, for this project DNDi will focus on the following strategy over the next five years (see table below summarizing the objectives related to the treatment limitation): Objective 1: to develop new safe and effective oral treatments as monotherapy and as early as possible as combination treatment (medical product) to prevent the risk of resistance development for the treatment of VL patients and a very safe, short-course one for asymptomatic carriers once their role in disease transmission has been better established:
Activity 1: to identify new series of compounds and to select candidates for promising NCEs from lead-optimization program to pre-clinical (class of Oxaborole; class of Nitromidazole; Dundee/GSK);
Activity 2: to bring from preclinical to POC a new drug candidate (VL2098); Activity 3: to complete the clinical development of existing candidate up to registration (Fexinidazole or VL 2098) as monotherapy and as soon as possible as combination treatment.
Objective 2: to develop technology of diagnostic (xenodiagnoses coupled with a quantitative PCR) in order to evaluate the role in transmission of asymptomatic carriers and PKDL patients:
Activity 1: set-up of sand fly colonies and training on xenodiagnoses and quantitative PCR. Activity 2: small clinical study evaluating the infectivity of asymptomatic careers and PKDL patients.
Objective 3: to develop treatment for PKDL (medical product):
Activity 1: start and complete clinical development of new regimen of treatments that demonstrate skin penetration for the current treatment of PKDL patient.
Objective 4: the contribution to the development of a shared, open-access data base that will allow identifying determinants of treatment effectiveness that will be based on existing ones developed for malaria. The project is based on an optimization and coordination of already existing initiatives in order to reduce the time, costs and efficiency necessary to achieve the goal of development new tools for the treatment of VL.
Page 5 of 26
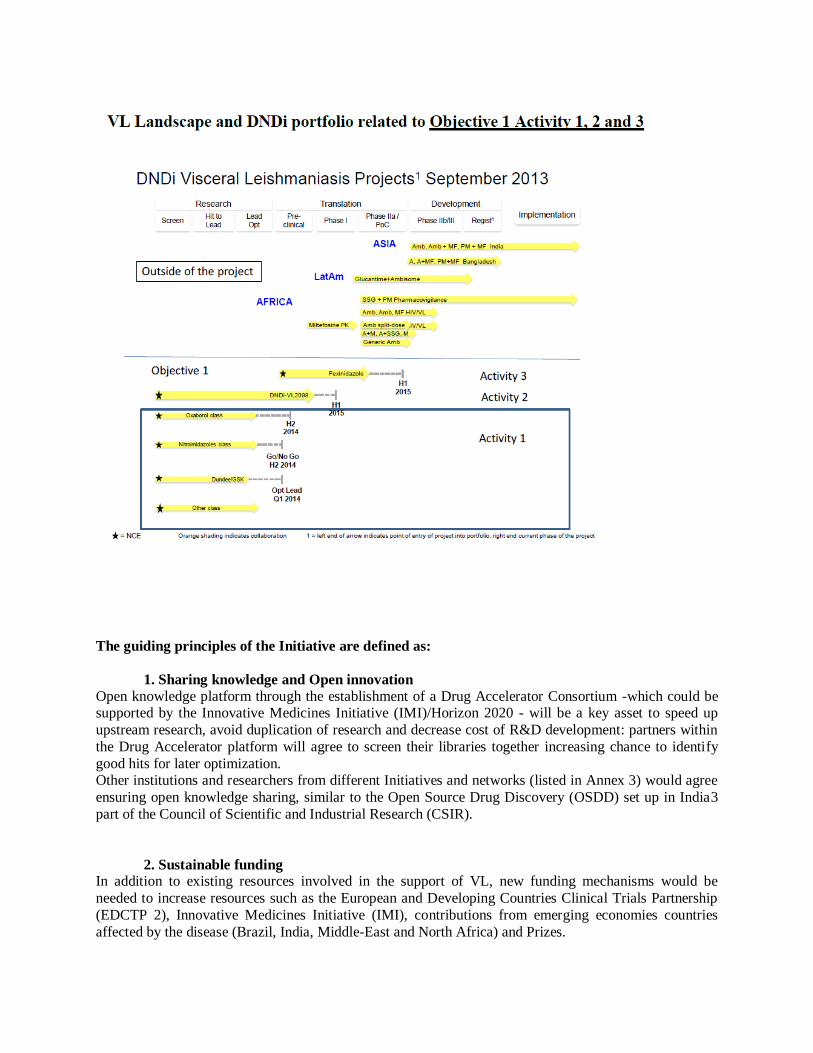
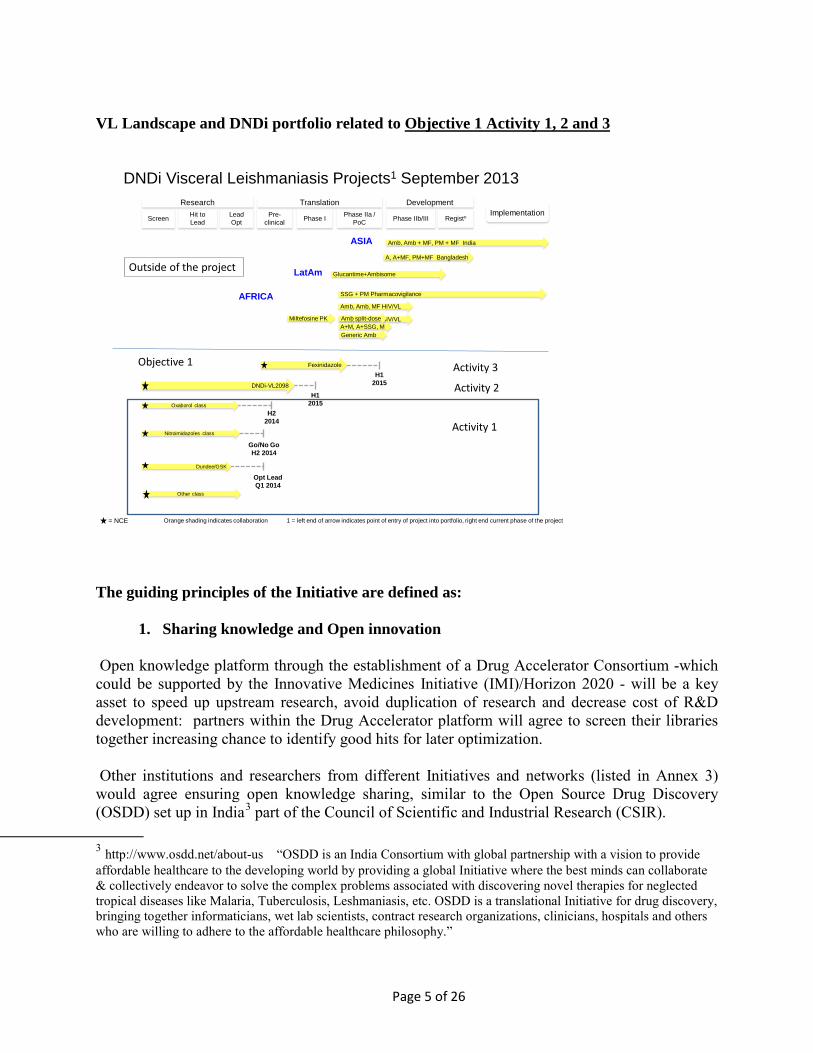
VL Landscape and DNDi portfolio related to Objective 1 Activity 1, 2 and 3
DNDi Visceral Leishmaniasis Projects1 September 2013
Amb, Amb, MF HIV/VLA+M, A+SSG, M
Screen Hit to Lead
Lead Opt
Pre-clinical Phase I Phase IIa /
PoC Phase IIb/III Registn
Research Translation DevelopmentImplementation
SSG + PM Pharmacovigilance
Amb, Amb + MF, PM + MF India
Glucantime+Ambisome
A, A+MF, PM+MF Bangladesh
ASIA
AFRICA
LatAm
= NCE 1 = left end of arrow indicates point of entry of project into portfolio, right end current phase of the projectOrange shading indicates collaboration
Amb, Amb, MF HIV/VL
Miltefosine PK Amb split-dose
DNDi-VL2098H1
2015Oxaborol class H2
2014Nitroimidazoles class
Go/No GoH2 2014
Dundee/GSK
Opt LeadQ1 2014
Generic Amb
Fexinidazole
H12015
Other class
Activity 1
Activity 3
Activity 2
Outside of the project
Objective 1
The guiding principles of the Initiative are defined as:
1. Sharing knowledge and Open innovation
Open knowledge platform through the establishment of a Drug Accelerator Consortium -which could be supported by the Innovative Medicines Initiative (IMI)/Horizon 2020 - will be a key asset to speed up upstream research, avoid duplication of research and decrease cost of R&D development: partners within the Drug Accelerator platform will agree to screen their libraries together increasing chance to identify good hits for later optimization.
Other institutions and researchers from different Initiatives and networks (listed in Annex 3) would agree ensuring open knowledge sharing, similar to the Open Source Drug Discovery (OSDD) set up in India3 part of the Council of Scientific and Industrial Research (CSIR).
3 http://www.osdd.net/about-us “OSDD is an India Consortium with global partnership with a vision to provide affordable healthcare to the developing world by providing a global Initiative where the best minds can collaborate & collectively endeavor to solve the complex problems associated with discovering novel therapies for neglected tropical diseases like Malaria, Tuberculosis, Leshmaniasis, etc. OSDD is a translational Initiative for drug discovery, bringing together informaticians, wet lab scientists, contract research organizations, clinicians, hospitals and others who are willing to adhere to the affordable healthcare philosophy.”

Page 6 of 26
2. Sustainable funding
In addition to existing resources involved in the support of VL, new funding mechanisms would be needed to increase resources such as the European and Developing Countries Clinical Trials Partnership (EDCTP 2), Innovative Medicines Initiative (IMI), contributions from emerging economies countries affected by the disease (Brazil, India, Middle-East and North Africa) and Prizes.
3. Equitable access
To ensure affordable access replicate the industrial model based on agreement signed with pharmaceutical company for one project for example contract signed with Sanofi for fexinidazole. It makes new therapeutic and diagnostic tools developed as public goods and ultimately available at affordable prices.
4. Coordination through collaborative approach
Setting up the VL Global R&D & Access Initiative in partnership with the current VL consortia and research platforms from the different relevant regions (see Annex 3). Details about the functioning of the Initiative: The Initiative for VL would be composed of a steering committee selected among the representatives of the scientific community, key governments, main R&D partners, relevant regional WHO offices (SEARO, PAHO, EURO, AFRO), DNDi, and the existing VL Initiatives (LEAP; Consortium for VL treatment in India and Bangladesh; Consortium on HIV/VL in East Africa; Consortium on PKDL) supported by a secretariat housed in an existing institution. The Initiative would also work in partnership with relevant partners such as the EDCTP, IMI, the Council of Scientific and Industrial Research (CSIR) including OSDD. The Secretariat will need to be committed to minimizing overhead costs and achieving value for money. The responsibilities of the Initiative would be to:
• Review and validate R&D priorities for VL disease • Define priority treatment candidates • Development and implementation of equitable access policy • Review and validate funding needs • Identify potential funding mechanisms at country, regional, and international levels • Review and validate proposals for innovative incentive mechanisms such as prizes • Review and propose regulatory, financial, and procurement policies to facilitate access to
final products • Monitor project implementation and results • Review and validate financial reports • Facilitate information sharing with national programs and regional initiatives • Appoint and have oversight of delegated activities of the Secretariat
Page 7 of 26
6.* Public health that the proposed project aims to address:
(Explain the public health need in terms of burden of disease; prevalence; incidence; fatality rate; geographical spread; current interventions and their limitations; and what proposed new technology would change in terms of disease prevention, control, diagnosis, treatment etc. If detailed information is not possible at present then please provide some basic level information)
The annual incidence is estimated at approximately 0.15 to 0.34million VL cases, with a case-fatality rate of 10% for visceral leishmaniasis per year4. Although a total of 98 countries reported endemic Leishmaniasis transmission, 90% of global VL cases occur in just six countries: India, Bangladesh, Sudan, South Sudan, Brazil and Ethiopia. It is estimated that 350 million people are at risk of the disease, most of them are children.
Furthermore, numbers rise sharply during an epidemic. As recently as 2012, South Sudan faced an epidemic which recorded more than 28,000 cases; 70% of patients were children aged under 15 who were already suffering from malnutrition during a drought.
Leishmaniasis is normally a disease of rural transmission but urbanization is a fact due to the increasing proximity of human new habitats with endemic areas where transmission occurs5 due to proximity of sylvatic infected reservoirs to the peri-domestic environment in which stray dogs bridge transmission to humans. In the new context where population is immunologically naive, epidemics are frequent. Currently various epidemics are on-going in major capitals like Asunción in Paraguay, Madrid in Spain or Tblisi in Georgia6. One of the major threats to controlling VL is its interaction with HIV infection. VL has emerged as an important opportunistic infection associated with HIV. In areas where VL is endemic, many people have asymptomatic infection. A concomitant HIV infection increases the risk of developing active VL by 100–2320 times. In southern Europe, up to 70% of cases of VL in adults are associated with HIV infection.
4 Leishmaniasis Worldwide and Global Estimates of Its Incidence. Alvar J. et al. (2012) PLoS ONE 7(5): e35671. doi:10.1371/journal.pone.0035671 5 Desjeux P.Trans R Soc Trop Med Hyg. 2001 May-Jun;95(3):239-43 6 Alvar J, Vélez ID, Bern C, Herrero M, Desjeux P, Cano J, Jannin J, den Boer M. Leishmaniasis Worldwide and Global Estimates of Its Incidence. PLoS ONE 2012, 7(5): e35671 Gil-Prieto R, Walter S, Alvar J, de Miguel AG. Epidemiology of leishmaniasis in Spain based on hospitalization records (1997-2008). Am J Trop Med Hyg. 2011 Nov;85:820-5.

Page 8 of 26
Epidemiological considerations • VL is fatal disease: patients need life-saving treatment to be cured. • 150,000-300,000 cases/y, with around 90% focused in a few countries (India, Sudan,
Brazil, Bangladesh, Ethiopia). • In southern Europe, up to 70% of cases of VL in adults are associated with HIV infection. • India is an important endemic country: 60% of all cases in Bihar state. • Around 20,000 cases are estimated in the East Africa region which is prone to
devastating outbreaks. • In Soudan more half of the patients develop PKDL in Soudan7 • VL is poverty related and leads to economic devastation to already poor households; this
is partly due to lack of cheap effective treatments at the lowest health care level. • 50-70% of patients are children.
VL is of a complex nature comprising various elements fuelling transmission including: Poverty. Leishmaniasis has strong but complex links with poverty; under nutrition has been shown to increase the risk of infected patients progressing to clinically manifested VL. HIV/VL co-infection. Both HIV and Leishmaniasis contribute to the impairment of the immune response – together, they exert a synergistic deleterious effect on host cells, increasing both virus replication and parasite multiplication8. Anthroponotic reservoirs. It has been proven that there are 26 more chances to have a second case in a house where there is an active VL case than in a house with no patient, and only 50 meters far the chances decrease to 3 times due to the short distance that the sand flies can fly. To prove if the patient contacts could prevent the disease by taken chemoprophylaxis is of paramount importance in the prevention of VL. If an oral, safe and cheap drug would be available, a new concept in the control strategy should include the contacts. Also a large number of individuals in endemic areas are infected with Leishmania spp but do not develop clinical signs of the disease. In various longitudinal studies it has been shown that every 1 active VL case there are 4 asymptomatics (Kenya or Bangladesh) up to 1.50 (Spain)9. If these asymptomatic
7 Desjeux et al. Parasites & Vectors 2013, 6:196 http://www.parasitesandvectors.com/content/6/1/196 8 Prognosis of HIV/VL co-infection is poor with very common relapses, and an additional drawback is the increased toxicity of VL treatments (especially pentavalent antimonials) in HIV co-infected patients. Thirty-five countries around the world report HIV/VL co-infection, with the highest incidence being reported in Ethiopa with up to 40% of all VL cases in Humera in the northwest. In southern Europe, up to 70% of cases of VL in adults are associated with HIV infection. 9 Among seropositive individuals, PCR positivity was found in 12% (Iran) and even in seronegative individuals PCR was positive in 8 out of 365 individuals in India. Moreover, living promastigotes have been isolated in 3 blood bags out of 30 seropositive in a blood bank in a major hospital in Ibiza, Spain9.
Page 9 of 26
carriers are indeed infective to sand flies, they could act as a reservoir of parasites and control programmes should therefore take them into account.
PKDL. It is a skin condition that usually develops after VL treatment. PKDL occurs in 1 to 40% of normally treated VL cases. The drug used for VL treatment is thought to influence PKDL incidence, but more evidence is needed to support this assumption. PKDL patients could play an important role as a reservoir, maintaining transmission during inter-epidemic periods.
Although the number of treatment options for VL has increased in the past decade, the existing therapies for VL, have serious drawbacks in terms of safety, resistance, stability, and cost10 and low tolerability, long treatment duration, and are difficult to administer (see table in annex 3). Therefore, there is an urgent need for safe, short-course oral treatments that cover all species of the parasite for the visceral forms of the disease and that would be efficacious in all geographic regions – as well as for Post-Kala Azar Dermal Leishmaniasis (PKDL), eventually used in HIV-VL co-infected patients and one that can be administered to asymptomatic infective cases- and “contacts”. 7.* Explain which new and innovative approaches and mechanisms to supporting financing and coordination of R&D this project would demonstrate?
(This is a very important part to be filled. The idea of these demonstrations projects is “to address identified gaps that disproportionately affect developing countries’ particularly the poor, and for which immediate action can be taken” (WHA66.22). 66th WHA considered these demonstration projects as part of the efforts to “take forward action in relation to monitoring, coordination and financing for health research and development”. The assembly decided to identify such projects that :”(a) address identified research and development gaps related to discovery, development and/or delivery, including promising product pipelines, for diseases that disproportionally affect developing countries, particularly the poor, and for which immediate action can be taken; (b) utilize collaborative approaches, including open knowledge approaches, for research and development coordination; (c) promote the de-linkage of the cost of research and development from product price; and (d) propose and foster financing mechanisms including innovative, sustainable and pooled funding; (2) The demonstration projects should provide evidence for long-term sustainable solutions.”)
The overall project, which addresses the identified gaps of VL R&D (see question 4 and 5) and with the guiding principles developed under question 5, requires different innovative incentive
10 Structures, Targets and Recent Approaches in Anti-Leishmanial Drug Discovery and Development. Seifert K., Open Med Chem J. 2011; 5:31–39. doi: 10.2174/1874104501105010031

Page 10 of 26
mechanisms to fill R&D gaps to increase knowledge, decrease the risk of failure, raises down the resources needed, capitalize on existing resources and develop drug at affordable cost using the principle of delinkage.
The delinkage of the cost of R&D from product price can only be ensured when the cost of R&D is paid for (or “recouped”) through mechanisms other than the sales revenues of the product. This can be done through a range of mechanisms - such as prize, grant with access clauses, patent pool - with contractual commitments to access, affordability and non-exclusive licensing provisions. It would necessarily entail transparency related to the costs of R&D, manufacturing and delivery of the final products.
The VL Initiative will consider, following the guiding principles, the following appropriate mechanisms according to the R&D gaps targeted and the related treatment limitation.
Objectives Topic Incentives mechanisms Partners (pending until
discussion and aggreementfrom suggested partners)
Region
Objectives 1: effective, safe and field-adapted 1st line treatments for East Africa and Latin America (and 2nd
line for the Indian sub-continent),
Activity 1 : Identifying new compounds fromlead optimisation to pre-clinical phase(class of Oxaborole, Dundee/GSK, class of Nitromidazole)
Activity 2:Moving a NCE from pre-clinical phase to POC (VL 2098)
Open knowledge, Drug Accelerator and Open source
Grant with access clause
OSDD/ CDRI, Drug Accelerator partners, IMI
Global
Activity 3:Developmentduring clinical trials(Fexinidazole and Combinaison)
Capacity building, Collaborative coordination,Innovative Regulatorypathways
LEAP, EDCTP, Fiocruz, ICMR, East Africa, Latin America, India
Objectives 2: understanding of the role of asymptomatic and PKDL patients in the transmission of the disease
Xenodiagnosis andquantitative PCR
Capacity building, Collaborative coordination, data sharing, Milestones Prizes
University Utrecht, Institute of EndemicDiseases, University of Caracas, Ferrer Group, Salpêtrière Hospital, StiefelGSK, SGS
Soudan, Bangladesh, India
Objectives 3: safe, effective and field-adapted 1st line treatment for PKDL patients
Research on skin penetration of existing drugs –clinicaldevelopment
Open knowledge, Drug Accelerator and Open source
LEAP, EDCTP, ICCDRB, PATH, IMI
Sudan, Bangladesh, possibly later India
Objectives 4: tools to monitor the development of resistance to existing
Build up databaseand tools
Open source , data sharing WARRN, MoHs , ITM,EDCTP(www leishrisk net)
Global
Incentives for Objective 1 (see graphic below) Activity 1: to identify and to select candidates for promising NCEs from lead-optimization program to pre-clinical in order to respond to an important attrition rate inherent to R&D activities. Establishing innovative partnerships with the private and public sector based on open knowledge and open innovation principles in order to accelerate research and optimize the limited funding resources available. Despite improvements over the last years the resources invested in drug discovery and development for neglected tropical diseases such as

Page 11 of 26
Leishmaniasis is still fails to meet the huge and pressing need for new medicines. In order to increase the scale of this work, increase the number of new chemical entities (NCEs) for VL in the development pipeline and accelerate the provision of new ingredients for future treatments it is needed to synergise several important advances in NTD science and collaborations with and between large pharmaceutical companies. Then the establishment of a drug accelerator consortium in partnerships with pharmaceutical companies to provide access to state of the art, compound profiling assays and drug discovery expertise also connected with other leading groups in lead optimization for NTDs such as Drug Discovery Unit of Dundee University will build a capacity able to meet the demands of an increased R&D pipeline. This combination of DNDi’s expertise in parasitology and kinetoplastid diseases coupled with industry leading drug discovery and development capabilities and collaborations with leading academic drug discovery groups will provide excellent capabilities to identify a large number of top quality preclinical candidates through pooling of resources, sharing knowledge and avoiding duplication of effort. Mechanisms such as Innovative Medicines Initiative (IMI) within the Horizon 2020 program could help to promote game-changing activities and ensure that various pharmaceutical companies collaborate in an integrated manner with academic partners, SMEs and a product development partnership to foster innovation . The drug Accelerator’s specific purpose is to pool resources by searching and screening multiple libraries simultaneously and capabilities of pharmaceutical companies to identify more rapidly expanded hit series and quickly establish Structure-Activity Relationships (SARs) that the initiative may then take through lead optimization (LO) and the full spectrum of pharmaceutical research, development and implementation for NTDs. The discoveries will be put into the public domain exploiting developments such as the EU Open PHACTS Discovery Platform to catalyze further research and enhance collaboration. Incentive for Objective 1 activity 2: Moving NCE from pre-clinical phase to clinical development (POC) through Grant funding with access clauses. (VL 2098) The principle of delinkage of R&D cost from product price mentioned above can also be implemented with any type of grant through provisions/clauses in grant contracts to ensure access and affordability of the final products. Incentives for Objective 1 activity 3: To complete the clinical development of existing candidate up to registration (Fexinidazole / VL 2098) as monotherapy and as soon as possible as combination treatment through collaborative coordination with EDCTP and the consortiums and platforms in endemic countries: - DNDi has in its portfolio fexinidazole for VL that is progressing into preclinical phase and
clinical phases.

Page 12 of 26
- This project will allow the involvement of the various platforms (see Annex 3) in the progression of those molecules into clinical phases using clinical research platforms set up in endemic areas. Considering the wide range of disease strains, the project will also allow to perform at the same time clinical trials following GCP standards in different geographical areas reflecting the complexity of the disease and the various geographical immune responses.
Graphic highlighting the new incentives related to Objective 1 activity 1, 2 and 3
DNDi Visceral Leishmaniasis Projects1 September 2013
Amb, Amb, MF HIV/VLA+M, A+SSG, M
Screen Hit to Lead
Lead Opt
Pre-clinical Phase I Phase IIa /
PoC Phase IIb/III Registn
Research Translation DevelopmentImplementation
SSG + PM Pharmacovigilance
Amb, Amb + MF, PM + MF India
Glucantime+Ambisome
A, A+MF, PM+MF Bangladesh
ASIA
AFRICA
LatAm
= NCE 1 = left end of arrow indicates point of entry of project into portfolio, right end current phase of the projectOrange shading indicates collaboration
Amb, Amb, MF HIV/VL
Miltefosine PK Amb split-dose
DNDi-VL2098H1
2015Oxaborol class H2
2014Nitroimidazoles class
Go/No GoH2 2014
Dundee/GSK
Opt LeadQ1 2014
Generic Amb
Fexinidazole
H12015
Other class
Activity 1
Activity 3Activity 2
Outside of the project
Incentives for Objective 1
Open knowledgeDrug Accelerator
Open source
Grant with Access clauses
Collaborative coordination with consortiums and clinical platforms Innovative regulatory pathways
Incentives for Objective 2: to develop technology of diagnostic (xenodiagnoses coupled with a quantitative PCR) in order to evaluate the role in transmission of asymptomatic carriers and PKDL patients through milestone prizes that could be awarded to projects that achieve pre- determined milestone thresholds throughout the development of the diagnostic.
Incentives for Objective 3: to start and complete clinical development of new regimen of
treatments that demonstrates skin penetration for the current treatment of PKDL patient, with the same incentives as clinical development of NCEs (objective 1).
Innovative mechanism for Objective 4: the contribution to the development of a shared, open-
access data base that will allow identifying determinants of treatment effectiveness that will be based on existing ones developed for malaria. The initiative will work with existing initiatives such as WWARN, to start building up under the same principles a clinical and
Page 13 of 26
possibly biological shared data base where data can be accessed to elucidate scientific questions that could not be answered in single studies.
Overall, interactions and collaborations among the different partners -through the Initiative- with a focused coordination of promising R&D projects are needed to accelerate their completion. In addition, equitable access policy and pool funding are also essential: Ensuring equitable access policy The Initiative will implement a policy of equitable access to new therapeutic and diagnostic tools, based on agreed-upon principles ensuring that the products developed via the coordinated funding are done so as public goods, with affordable pricing, thus supporting de-linkage of R&D costs from final product prices. To ensure sustainable access, the Initiative will regularly review and propose enabling regulatory, financial, and procurement policies with involvement of endemic countries regulators in the platform to accelerate the registration. Funding The VL Initiative would pull public and private funding into a fund to support the project. To ensure sustainable funding, members of the steering committee, namely governments, would need to commit the necessary funding for identified R&D priorities. Some funding sources already exist that could be leveraged and targeted in this way, including from cooperation agencies, regional philanthropic foundations and mechanisms such as European & Developing Countries Clinical Trials Partnership (EDCTP 2) which will extend its scope to Neglected tropical diseases for supporting clinical trials in Africa and contributions from emerging economies countries affecting by the diseases. 8.* Evidence of market failure/research landscape
(Explain why there has been no investment in this technology or why investment has not resulted in access to the health care product.)
Most cases (>90%) occur in just six countries: Bangladesh, India, Nepal, Sudan, Ethiopia and Brazil. Half of patients worldwide live in the Indian state of Bihar, one of the poorest states of India. . The second largest focus is East Africa, which is also an epidemic-prone region. Those affected people do not represent an attractive market for the pharmaceutical industry. There are three major barriers to the elimination of VL, one is lack of knowledge in the natural history of VL, the other one is the attrition rate in getting an appropriate drug, moreover if it is for preventive therapy and finally the unaffordability and lack of access to treatments.

Page 14 of 26
The last decade has seen improvements in the treatment, diagnosis, and prevention of leishmaniasis in South Asia, notably through the development of liposomal amphotericin B, paromomycin, and miltefosine.
While the progress achieved has led to a clearer notion of how to treat patients across different continents, existing treatments are not ideal: potential of resistance development, low tolerability, long treatment duration and difficulty in administration, as well as high cost are still major drawbacks as explained above under Question 6. The main causes of the weaknesses in the VL R&D pipeline are:
• High attrition rate for the selection of clinical candidates Drug discovery for Leishmaniasis has been challenging. This is partly because the Leishmania parasite resides in an intracellular compartment in macrophages. A limited number of molecular targets have been validated; hence phenotonic screening against intracellular parasites is the main approach. Several optimised leads from different chemicals series have been advanced but failed to show significant in vivo activity. For assessing PK/PD parameters, a suitable animal model does not exist. Further, in vitro potency assays have significant intra-lab variations, making cross lab comparison difficult requiring more time and effort for optimisation and selection of clinical candidates.
• Lack of affordable treatment
The need for affordable treatments is today the most important drawbacks of existing therapies as mentioned above. A recent study evaluated the cost-effectiveness of various monotherapies and combination VL treatment strategies in the Indian subcontinent which led to the main conclusion that although cost-effective treatments are available, most afflicted patients cannot afford them, and strategies including relatively expensive drugs such as AmBisome® are not accessible to most individuals unless governments, manufacturers and donors are willing to subsidize these treatments. 11 Moreover, keeping in mind the goal of elimination by 2020 for the Indian subcontinent, it is required to understand the different elements fuelling transmission inter- and during epidemics and to develop the appropriate drugs that certainly differ according to the targeted population. For instance, if the case is to put under chemoprophylaxis asymptomatic infective carriers and “patient contacts”, the TPP has to be very strict: oral drug, extremely safe, not interfering with other oral drugs taken routinely in other programs, not need to be administered more than twice per year, etc. New treatments that address these issues and address geographical variations and local realities are essential (i.e. East Africa reality)
11 Meheus F., Balasegaram M., Olliaro P., Sundar S., Rijal S., Faiz A., Boelaert M. Cost-effectiveness of combination therapies for the treatment of Visceral Leishmaniasis in the Indian Subcontinent, Poster presented at ASTMH, 2009.
Page 15 of 26
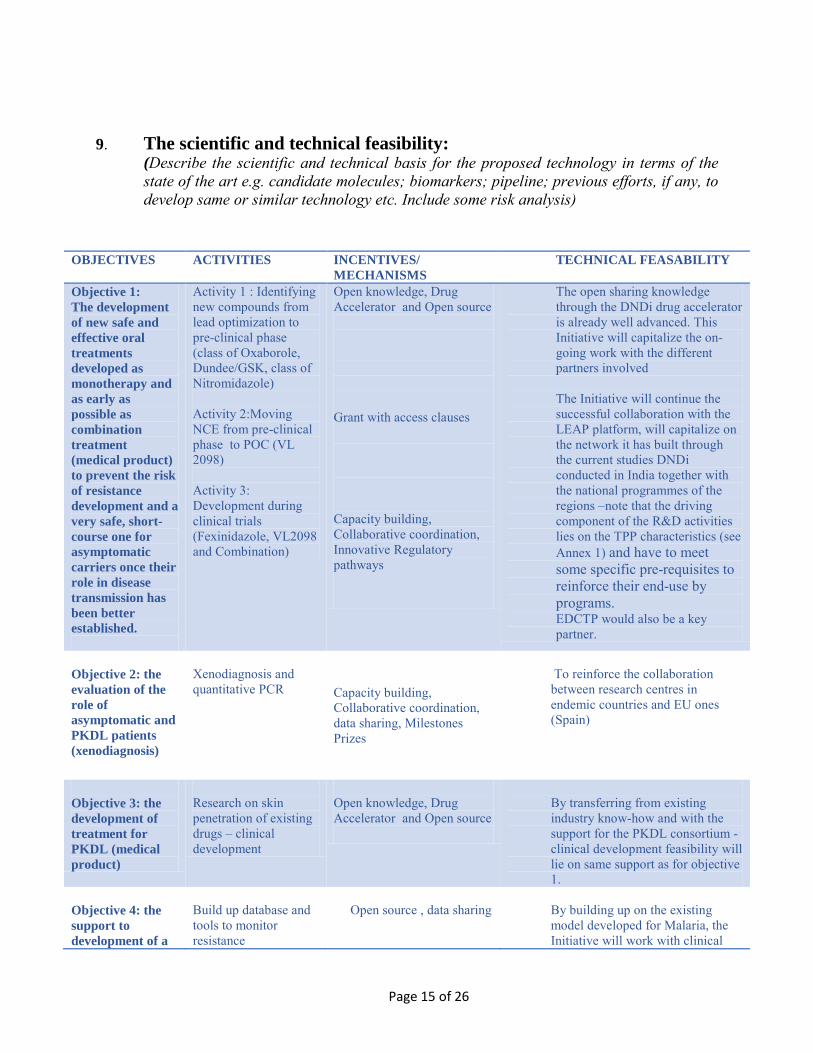
9. The scientific and technical feasibility:
(Describe the scientific and technical basis for the proposed technology in terms of the state of the art e.g. candidate molecules; biomarkers; pipeline; previous efforts, if any, to develop same or similar technology etc. Include some risk analysis)
OBJECTIVES ACTIVITIES INCENTIVES/ MECHANISMS
TECHNICAL FEASABILITY
Objective 1: The development of new safe and effective oral treatments developed as monotherapy and as early as possible as combination treatment (medical product) to prevent the risk of resistance development and a very safe, short-course one for asymptomatic carriers once their role in disease transmission has been better established.
Activity 1 : Identifying new compounds from lead optimization to pre-clinical phase (class of Oxaborole, Dundee/GSK, class of Nitromidazole) Activity 2:Moving NCE from pre-clinical phase to POC (VL 2098) Activity 3: Development during clinical trials (Fexinidazole, VL2098 and Combination)
Open knowledge, Drug Accelerator and Open source
Grant with access clauses
Capacity building, Collaborative coordination, Innovative Regulatory pathways
The open sharing knowledge through the DNDi drug accelerator is already well advanced. This Initiative will capitalize the on-going work with the different partners involved The Initiative will continue the successful collaboration with the LEAP platform, will capitalize on the network it has built through the current studies DNDi conducted in India together with the national programmes of the regions –note that the driving component of the R&D activities lies on the TPP characteristics (see Annex 1) and have to meet some specific pre-requisites to reinforce their end-use by programs. EDCTP would also be a key partner.
Objective 2: the evaluation of the role of asymptomatic and PKDL patients (xenodiagnosis)
Xenodiagnosis and
quantitative PCR
Capacity building, Collaborative coordination, data sharing, Milestones Prizes
To reinforce the collaboration between research centres in endemic countries and EU ones (Spain)
Objective 3: the development of treatment for PKDL (medical product)
Research on skin penetration of existing drugs – clinical development
Open knowledge, Drug Accelerator and Open source
By transferring from existing industry know-how and with the support for the PKDL consortium - clinical development feasibility will lie on same support as for objective 1.
Objective 4: the support to development of a
Build up database and tools to monitor resistance
Open source , data sharing
By building up on the existing model developed for Malaria, the Initiative will work with clinical

Page 16 of 26
10. Reasons for proposing:
(Provide details if any priority setting and/or selection criteria that has underpinned the consideration to take up this area of technology for development.)
References: - Urgent public health need as described under question 6. - World Health Assembly resolution WHA60.13, May 20007 - Control of the Leishmaniasis, WHO 2010 - WHO Roadmap 2020, Sustaining the drive to overcome the global impact of the neglected
diseases
11. Who could potentially develop the technology/carry out the research? (Provide known details : individual researcher? Group of researchers? Research/coordination organization including PDPs? Group of research organizations working together? Combination of these; What would be the process of selection of developers?) DNDi a PDP has developed the competence to coordinate and work with a variety of actors from different background: from university, to CROs, to biotech, pharmaceutical, researchers from endemic countries, to conduct clinical trials, involving endemic countries regulators, donors and WHO.
12. Who could potentially manufacture the final product?
Multinational company? Local production? Joint venture? How the decision will be made about the producer? Industrial partners such as pharmaceutical companies involved in neglected diseases. DNDi has already examples of contractual relation with industry partners such as SANOFI in the context of Fexinidazole for sleeping sickness /Human African trypanosiomasis, with the possibility to develop technology transfer with generic companies in endemic regions
shared, open-access data base that will allow to identify determinants of treatment effectiveness
partners, notably EDCTP, towards a similar tool acknowledging that technical (database) and legal (anonymisation, access, conflict of interest …) aspects were addressed by for the Malaria database and will not be different
Page 17 of 26
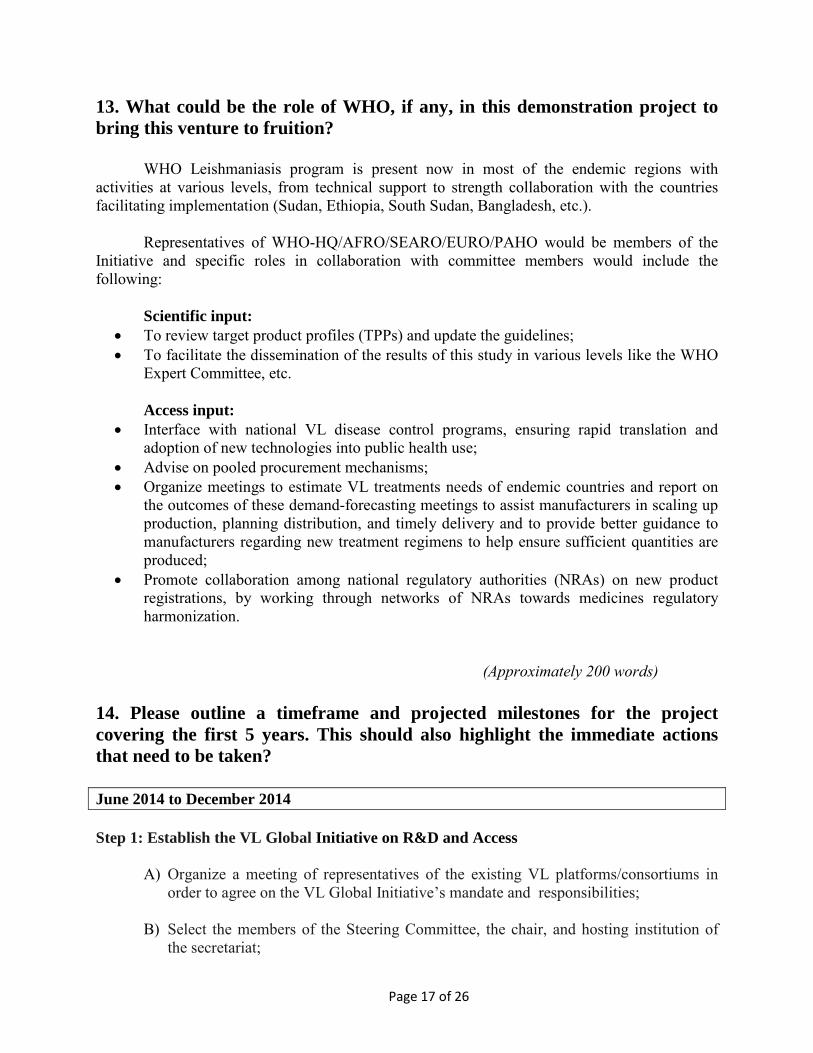
13. What could be the role of WHO, if any, in this demonstration project to bring this venture to fruition? WHO Leishmaniasis program is present now in most of the endemic regions with activities at various levels, from technical support to strength collaboration with the countries facilitating implementation (Sudan, Ethiopia, South Sudan, Bangladesh, etc.). Representatives of WHO-HQ/AFRO/SEARO/EURO/PAHO would be members of the Initiative and specific roles in collaboration with committee members would include the following:
Scientific input: • To review target product profiles (TPPs) and update the guidelines; • To facilitate the dissemination of the results of this study in various levels like the WHO
Expert Committee, etc. Access input:
• Interface with national VL disease control programs, ensuring rapid translation and adoption of new technologies into public health use;
• Advise on pooled procurement mechanisms; • Organize meetings to estimate VL treatments needs of endemic countries and report on
the outcomes of these demand-forecasting meetings to assist manufacturers in scaling up production, planning distribution, and timely delivery and to provide better guidance to manufacturers regarding new treatment regimens to help ensure sufficient quantities are produced;
• Promote collaboration among national regulatory authorities (NRAs) on new product registrations, by working through networks of NRAs towards medicines regulatory harmonization.
(Approximately 200 words) 14. Please outline a timeframe and projected milestones for the project covering the first 5 years. This should also highlight the immediate actions that need to be taken? June 2014 to December 2014 Step 1: Establish the VL Global Initiative on R&D and Access
A) Organize a meeting of representatives of the existing VL platforms/consortiums in order to agree on the VL Global Initiative’s mandate and responsibilities;
B) Select the members of the Steering Committee, the chair, and hosting institution of the secretariat;
Page 18 of 26
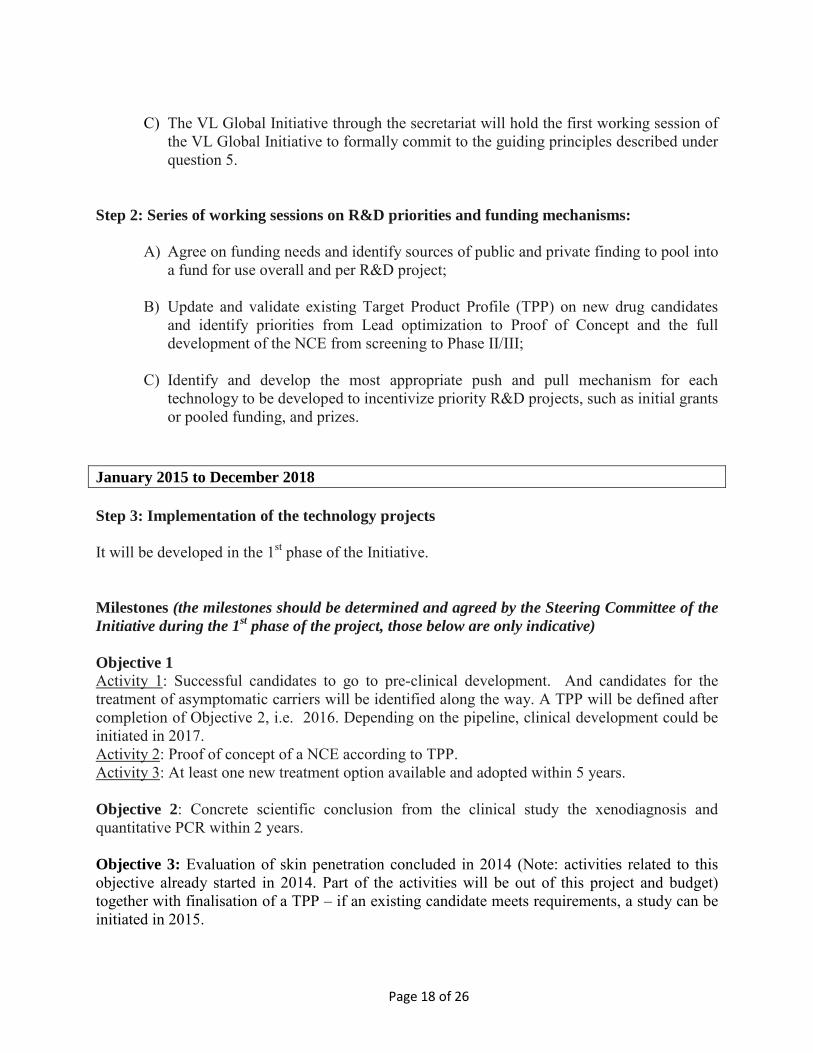
C) The VL Global Initiative through the secretariat will hold the first working session of
the VL Global Initiative to formally commit to the guiding principles described under question 5.
Step 2: Series of working sessions on R&D priorities and funding mechanisms: A) Agree on funding needs and identify sources of public and private finding to pool into
a fund for use overall and per R&D project;
B) Update and validate existing Target Product Profile (TPP) on new drug candidates and identify priorities from Lead optimization to Proof of Concept and the full development of the NCE from screening to Phase II/III;
C) Identify and develop the most appropriate push and pull mechanism for each technology to be developed to incentivize priority R&D projects, such as initial grants or pooled funding, and prizes.
January 2015 to December 2018 Step 3: Implementation of the technology projects It will be developed in the 1st phase of the Initiative. Milestones (the milestones should be determined and agreed by the Steering Committee of the Initiative during the 1st phase of the project, those below are only indicative) Objective 1 Activity 1: Successful candidates to go to pre-clinical development. And candidates for the treatment of asymptomatic carriers will be identified along the way. A TPP will be defined after completion of Objective 2, i.e. 2016. Depending on the pipeline, clinical development could be initiated in 2017. Activity 2: Proof of concept of a NCE according to TPP. Activity 3: At least one new treatment option available and adopted within 5 years. Objective 2: Concrete scientific conclusion from the clinical study the xenodiagnosis and quantitative PCR within 2 years. Objective 3: Evaluation of skin penetration concluded in 2014 (Note: activities related to this objective already started in 2014. Part of the activities will be out of this project and budget) together with finalisation of a TPP – if an existing candidate meets requirements, a study can be initiated in 2015.
Page 19 of 26
Objective 4: Database running within 1 year. 15. What is the intellectual property (IP) landscape relative to this project? Is there any IP, e.g. patents that need to be licensed in to be able to develop and market the product in developing countries? How would IP and related intellectual assets, including knowhow, proposed to be managed in this project? With regards to the development of new technologies, the equitable access policy established by the VL Global Initiative would include an IP policy that would be applied to all funded projects based on the following principles:
• Ensure ability to undertake further research based on the research findings in development of new tools or treatments
• Ensure treatments are ultimately affordable to the patients who need them and that access to these treatments is equitable
• Develop new drugs and tests as public goods 16.* What would be the strategy to ensure access to the product once it is developed? (Access is an important dimension of these demonstration projects, it is important for the projects to begin with the end in mind, explain how this project would deliver the technologies to the needy patients i.e. Price and affordability; modes of supply; storage; prescription; dispensing; and compliance; WHO will develop guiding principles for ensuring access to any products coming out of the demonstration projects)
The early involvement and collaborative work of the Initiative with active participation of VL control programs, SEARO, AFRO, PAHO, EURO and WHO-HQ together with key research institutions, PDPs, and manufacturers, are seen as key components to minimise the time for translation and adoption of developed technologies. In order to ensure equitable access the VL Initiative would develop an access policy for funded projects requiring that new therapeutic and diagnostic tools be developed as public goods and ultimately available at affordable prices. Financial incentives, such as advance purchase commitments, and pooled procurement may be required to scale up manufacturing of these treatments, ensure their affordability, and facilitate their delivery to developing country patients. The coordinating body can act as a forum to assess such needs and propose incentives and seek funding for them.
Page 20 of 26
The Initiative would also explore and facilitate innovative regulatory pathways to strengthen collaboration and mutual recognition between regulatory authorities. One of the issues to scale up treatment is the need for more operational resources to deliver treatments in the field. The VL Global Initiative would have regular contact with national programs and regional initiatives to discuss how new tools could be integrated into their national strategy and advocate to national governments that the appropriate resources are committed in order to scale up treatment. (Approximately 400 words)
Page 21 of 26
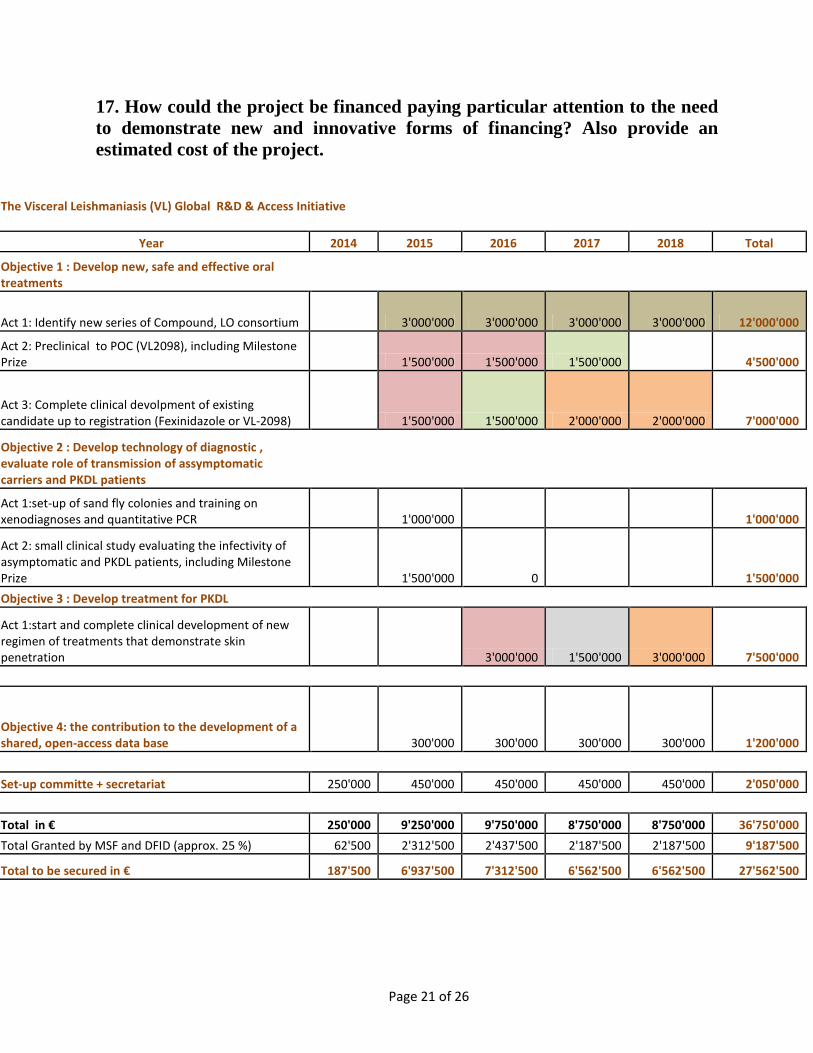
17. How could the project be financed paying particular attention to the need to demonstrate new and innovative forms of financing? Also provide an estimated cost of the project.
The Visceral Leishmaniasis (VL) Global R&D & Access Initiative
Year 2014 2015 2016 2017 2018 Total
Objective 1 : Develop new, safe and effective oral treatments
Act 1: Identify new series of Compound, LO consortium 3'000'000 3'000'000 3'000'000 3'000'000 12'000'000
Act 2: Preclinical to POC (VL2098), including Milestone Prize 1'500'000 1'500'000 1'500'000 4'500'000
Act 3: Complete clinical devolpment of existing candidate up to registration (Fexinidazole or VL-2098) 1'500'000 1'500'000 2'000'000 2'000'000 7'000'000
Objective 2 : Develop technology of diagnostic , evaluate role of transmission of assymptomatic carriers and PKDL patients
Act 1:set-up of sand fly colonies and training on xenodiagnoses and quantitative PCR 1'000'000 1'000'000
Act 2: small clinical study evaluating the infectivity of asymptomatic and PKDL patients, including Milestone Prize 1'500'000 0 1'500'000 Objective 3 : Develop treatment for PKDL
Act 1:start and complete clinical development of new regimen of treatments that demonstrate skin penetration 3'000'000 1'500'000 3'000'000 7'500'000
Objective 4: the contribution to the development of a shared, open-access data base 300'000 300'000 300'000 300'000 1'200'000 Set-up committe + secretariat 250'000 450'000 450'000 450'000 450'000 2'050'000 Total in € 250'000 9'250'000 9'750'000 8'750'000 8'750'000 36'750'000 Total Granted by MSF and DFID (approx. 25 %) 62'500 2'312'500 2'437'500 2'187'500 2'187'500 9'187'500
Total to be secured in € 187'500 6'937'500 7'312'500 6'562'500 6'562'500 27'562'500
Page 22 of 26
Resources are already devoted to this project and could be leveraged in order to finance the total amount needed: among the 37 M needed, currently about 9 M is already financed. DNDi existing financiers includes core funding donors:
- MSF - DFID
18. How could the project be governed and coordinated paying particular attention to the need to demonstrate better way of coordination? One of the main objectives of the Initiative for VL Global is to demonstrate that R&D projects can be optimised and deliver through strengthening coordination with multidisciplinary partners and through innovative mechanisms to finance and to coordinate R&D. To this end, the Initiative would be composed of a steering committee selected among the representatives of the scientific community, key governments, main R&D partners), relevant regional WHO offices (SEARO, PAHO, EURO, AFRO), DNDi, and the existing VL Initiatives (LEAP; Consortium for VL treatment in India and Bangladesh; Consortium on HIV/VL in East Africa; Consortium on PKDL) supported by a secretariat housed in an existing institution. The development of the partnership with relevant partners such as the EDCTP, IMI, the Council of Scientific and Industrial Research (CSIR) including OSDD, will be a fundamental function of the Initiative in order to maximize the conduct of VL R&D projects. The Initiative would also enhance DNDi on-going partnerships with pharmaceutical partners such as Sanofi, GSK etc., as well as with academics such as University of Dundee. The Initiative based on a strong coordination with relevant partnerships and through the steering committee elected among multidisciplinary partners, would catalyse the existing and future expertise and networks in VL R&D area, in order to accelerate the delivery of tools to treat VL patients and to prevent VL transmission. 19. Have any donor agencies/governments already indicated interest in supporting the project? For EURO region: France, Spain, Switzerland. These countries are supporting DNDi since several years. For EMRO region: Sudan. Discussions are currently on-going with the potential partners mentioned in the proposal and with Member States notably from endemic regions.
Page 23 of 26
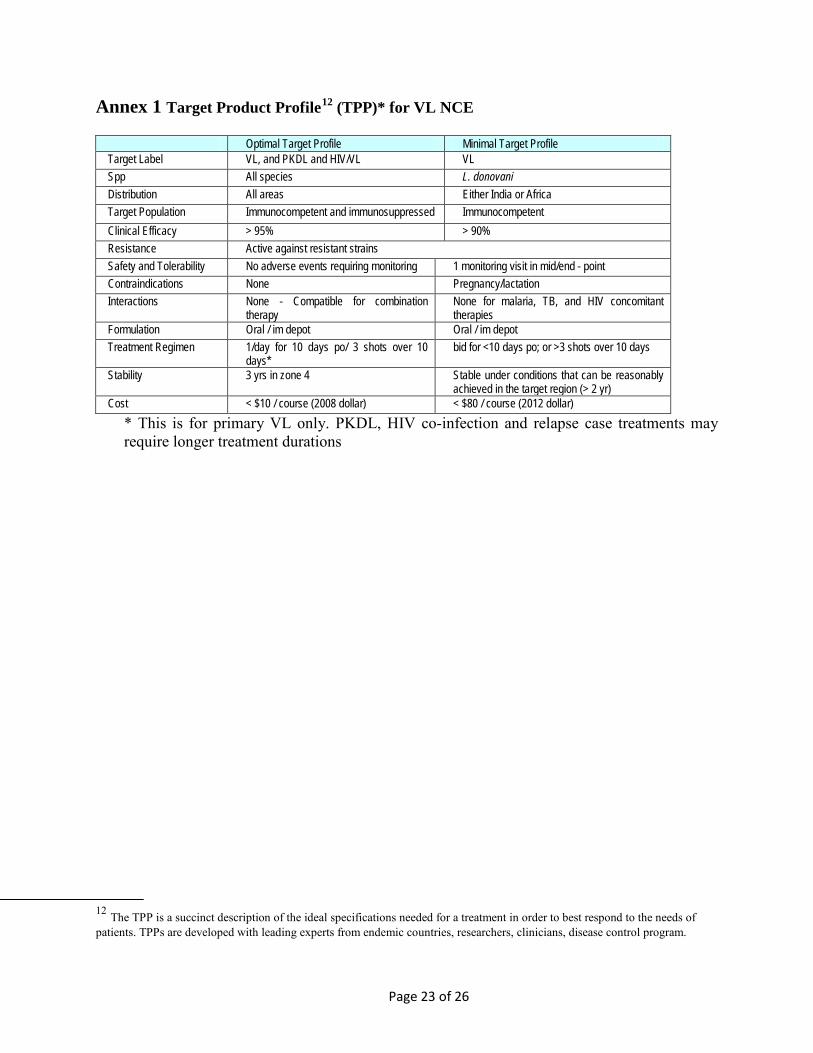
Annex 1 Target Product Profile12 (TPP)* for VL NCE
Optimal Target Profile Minimal Target Profile Target Label VL, and PKDL and HIV/VL VL Spp All species L. donovani Distribution All areas Either India or Africa Target Population Immunocompetent and immunosuppressed Immunocompetent Clinical Efficacy > 95% > 90% Resistance Active against resistant strains Safety and Tolerability No adverse events requiring monitoring 1 monitoring visit in mid/end - point Contraindications None Pregnancy/lactation Interactions None - Compatible for combination
therapy None for malaria, TB, and HIV concomitant therapies
Formulation Oral / im depot Oral / im depot Treatment Regimen 1/day for 10 days po/ 3 shots over 10
days* bid for <10 days po; or >3 shots over 10 days
Stability 3 yrs in zone 4 Stable under conditions that can be reasonably achieved in the target region (> 2 yr)
Cost < $10 / course (2008 dollar) < $80 / course (2012 dollar) * This is for primary VL only. PKDL, HIV co-infection and relapse case treatments may require longer treatment durations
12 The TPP is a succinct description of the ideal specifications needed for a treatment in order to best respond to the needs of patients. TPPs are developed with leading experts from endemic countries, researchers, clinicians, disease control program.
Page 24 of 26
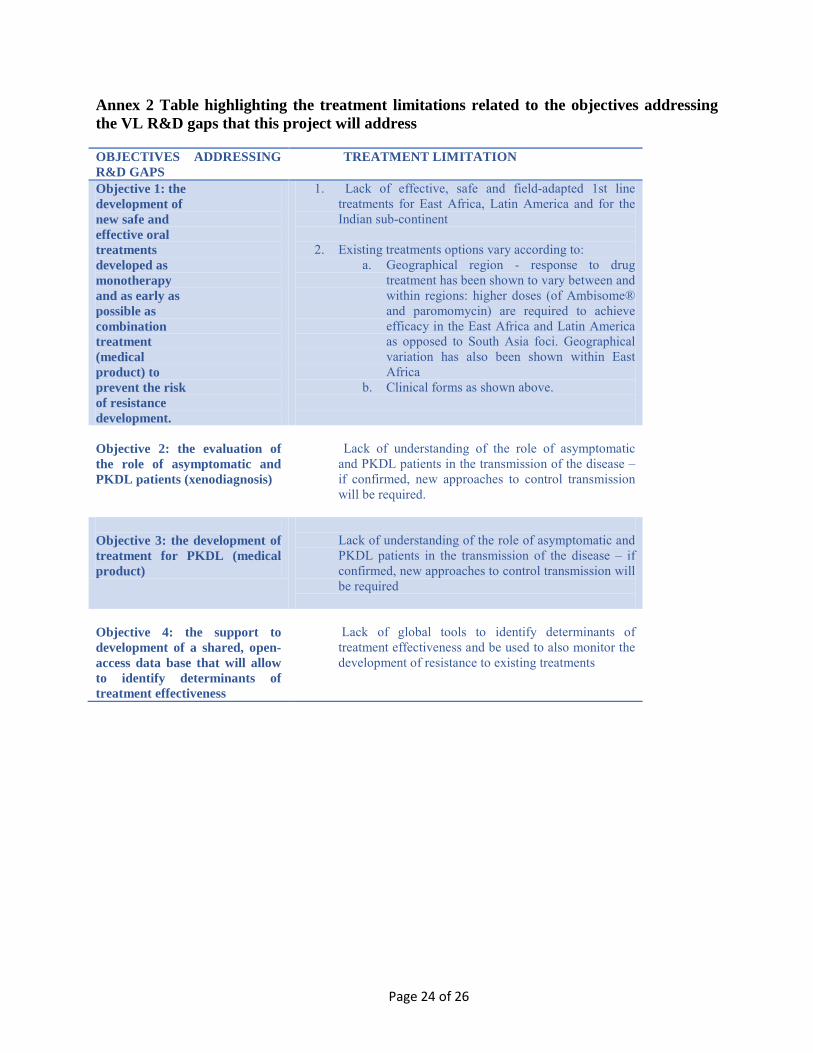
Annex 2 Table highlighting the treatment limitations related to the objectives addressing the VL R&D gaps that this project will address OBJECTIVES ADDRESSING R&D GAPS
TREATMENT LIMITATION
Objective 1: the development of new safe and effective oral treatments developed as monotherapy and as early as possible as combination treatment (medical product) to prevent the risk of resistance development.
1. Lack of effective, safe and field-adapted 1st line treatments for East Africa, Latin America and for the Indian sub-continent
2. Existing treatments options vary according to:
a. Geographical region - response to drug treatment has been shown to vary between and within regions: higher doses (of Ambisome® and paromomycin) are required to achieve efficacy in the East Africa and Latin America as opposed to South Asia foci. Geographical variation has also been shown within East Africa
b. Clinical forms as shown above.
Objective 2: the evaluation of the role of asymptomatic and PKDL patients (xenodiagnosis)
Lack of understanding of the role of asymptomatic and PKDL patients in the transmission of the disease – if confirmed, new approaches to control transmission will be required.
Objective 3: the development of treatment for PKDL (medical product)
Lack of understanding of the role of asymptomatic and PKDL patients in the transmission of the disease – if confirmed, new approaches to control transmission will be required
Objective 4: the support to development of a shared, open-access data base that will allow to identify determinants of treatment effectiveness
Lack of global tools to identify determinants of treatment effectiveness and be used to also monitor the development of resistance to existing treatments

Page 25 of 26
Annex 3: Summary of current VL treatments (based on WHO expert committee, 2010)1. Only the drug price is considered not the cost of hospitalisation
Regimen* Manufacturer Cost USD Efficacy Comments AmBisome IV 10mg/kg single dose Gilead 126 95% (P3) India subcontinent, poor
efficacy in Africa; requires cold chain
AmBisome 20mg/kg over 4 doses Gilead 252 98% (P4) India subcontinent, poor efficacy in Africa; requires cold chain
Amphotericin B 1mg/kg over 30 days
Multiple 20 95% (P3) Toxicity is main barrier to use
Miltefosine (MF) 100mg/ day oral for 28 days
Paladin 65-150 94% (P3) 82% (P4)
Low compliance and teratogenicity
Paromomycin base (PM) 11mg/kg/ day IM for 21 days
Gland Pharma 15 94% (P3) India subcontinent, poor efficacy in Africa
SSG 20mg/kg/ day for 30 days Albert David 55.8 65-95% (P3) Some toxicity; resistance in Bihar, but not elsewhere
Glucantime 20mg/kg/ day for 30 days Sanofi-Aventis 59.3 90% + Some toxicity; mainly used in Latin America
AmBisome 5mg/kg + MF 100mg/kg/ day for 7 days
Gilead Paladin
88.2-109.5 97.5% (P3) India subcontinent; requires cold chain; teratogenicity of MF
AmBisome 5mg/kg + PM 11mg/kg/ day for 7 days
Gilead Gland Pharma
79 97.5% (P3) India subcontinent; requires cold chain
MF 100mg/kg + PM 11mg/kg both for 10 days
Paladin Gland Pharma
30.2-60.7 98.5% (P3) India subcontinent; teratogenicty of MF; effectiveness?
SSG 20mg/kg + PM 11mg/kg both given IM for 17 days
Albert David Gland Pharma
44 91% (P3) Africa only; used in a wide field setting by MSF
*Assuming 35Kg patient Annex 4 List of VL consortiums and relevant platforms
• The Leishmaniasis East Africa Initiative (LEAP): coordinated by DNDi and gathers more than 60 individuals representing over 20 institutions. The overall aim of LEAP is to strengthen clinical research capacity, which is lacking in part due to the remoteness and geographic spread of the patients, most of whom live in the most impoverished regions of Africa. This Initiative also serves as a base for on-going educational cooperation between the countries in the East African region and standardization of procedures and practices within the region, as far as is possible within the confines of local regulations. LEAP evaluates, validates, and registers new treatments that address regional needs for VL.
• Consortium for VL treatment in India and Bangladesh: an international consortium formed in November 2011 to support control and elimination strategies in both countries, where the concentration of disease burden is among the world’s highest. DNDi, together with OneWorld Health (OWH) and the Special Programme for Research and Training in Tropical Diseases (TDR) collaborate with the National Control Programmes of India and Bangladesh, Médecins Sans Frontières (MSF), the Bihar State Health Society, and the Indian Council for Medical Research to carry out the consortium’s projects. The projects

Page 26 of 26
aims to generate the data necessary for Indian and Bangladeshi Ministries of Health to select adopt and implement the best management strategies to support control and elimination VL.
• Consortium on VL and HIV/VL in East Africa: the AfriCoLeish project, ‘Care Package for Treatment and Control of Visceral Leishmaniasis in East Africa’, aims to develop and deliver a shorter combination treatment for kala-azar patients that is equally as safe and effective as the current WHO-recommended first-line treatment for the disease (sodium stibogluconate and paromomycin, SSG&PM) in East Africa. The project aims to determine appropriate treatment strategies for kala-azar in patients that are also HIV positive, in order to treat and also prevent repetitive relapses that are common in co-infected patients. AfriCoLeish bring together six partners from Europe and East Africa with vast experience in R&D and treatment of HIV and kala-azar, namely the Drugs for Neglected Diseases initiative (DNDi); the Institute of Tropical Medicine in Antwerp (ITM-Antwerp); the London School of Hygiene and Tropical Medicine (LSHTM); Médecins Sans Frontieres (MSF, The Netherlands); the Institute of Endemic Diseases, University of Khartoum (IEND), Sudan; and the University of Gondar (UoG), Ethiopia.
• Consortium on PKDL: the PKDL Consortium is committed to promote and facilitate activities that lead to better understanding of all aspects of PKDL that are needed for improved clinical management and to achieve control of PKDL and VL. Fifty clinicians, scientists, policy makers, and advocates came together to discuss issues relating to PKDL epidemiology, diagnosis, pathogenesis, clinical presentation, treatment, and control.
• The OSDD consortium part of the CSIR: an India Consortium with global partnership with a vision to provide affordable healthcare to the developing world by providing a global Initiative where the best minds can collaborate & collectively endeavour to solve the complex problems associated with discovering novel therapies for neglected tropical diseases like Malaria, Tuberculosis, Leishmaniasis, etc. Launched in September 2008 has more than 7500 registered users from more than 130 countries around the world, and has emerged as the largest collaborative effort in drug discovery. Launched on the three cardinal principals of Collaborate, Discover & Share, it is a community driven open innovation Initiative to address the unmet need of research and development of drugs for diseases that affect the developing world.

1
ADDENDUM- CEWG Demonstration Projects
The Visceral Leishmaniasis Global R&D and Access Initiative
“Authors must send an addendum to their project which describes, where relevant, how the project:
1. Intends to delink the price of the final product from the cost of the R&D.
2. Utilizes collaborative approaches, including open knowledge innovation approaches.
3. Utilizes licensing approaches that secure access to your research outputs and final products.
4. Proposes and fosters financing mechanisms including innovative, sustainable and pooled funding.
5. Fosters effective and efficient coordination mechanisms amongst existing organizations/initiatives.
6. Strengthens capacity for research, development and production, including through technology transfer, in developing countries. “
Submitted by DNDi to the WHO PHI Secretariat on January 15th, 2014
How the project : ADDENDUM- The Visceral Leishmaniasis Global R&D & Access Initiative (1583 words)
1. Intends to de-link the price of the final product from the cost of the R&D
To address identified VL R&D gaps (cf. proposal Questions 4 and 5), the VL Global Initiative (hereafter ‘Initiative’) requires innovative incentive mechanisms that de-link R&D costs from product price. De-linkage particularly applies to activities of moving a new chemical entity from product pre-clinical to clinical development (Objective 1, Activity 2); completing clinical development of an existing candidate up to registration (Objective 1, Activity 3); and developing a new treatment for PKDL (Objective 3). De-linkage is ensured through:
1. DNDi’s intellectual property (IP) policy adopted in 2004, based on two criteria: ensuring that drugs are affordable and accessible in an equitable manner to patients who need them; and developing drugs as public goods whenever possible. This is the basis of contract negotiations with pharmaceutical partners to guarantee patient access to end products, in line with the Target Product Profile, which defines the ideal characteristics of the end product. Research and operations are not financed through IP rent revenues.
2. Contractual provisions with pharmaceutical partners. In practice, DNDi aims at securing licensing terms which ensure research and its outputs are considered public goods that advance public health. After ten years of experience, DNDi developed 6 new treatments and established ‘Gold standard’ licensing terms:
- Perpetual royalty-free, non-exclusive, sub-licensable licenses - Worldwide research and manufacturing rights; - Commitment to make the final product available at manufacturing
cost, plus minimal margin, in all endemic countries, regardless of
2
income level; - Non-exclusivity, enabling technology transfer and local production to
multiply sources of production and decrease cost of product. As an example of de-linkage, ASAQ-FDC for malaria, developed by DNDi and Sanofi (2007), is available at-cost plus a small margin (under USD 1 for adults; under USD 0.5 for children). 3. PDPs as push mechanisms: The last decade, with new public and private donor commitments, has seen new push mechanisms, including PDPs, to finance R&D and pull mechanisms to attract new stakeholders. PDPs, with a model such as DNDi’s, by seeking diverse funding from private and public donors (cash donations, in-kind contributions, R&D grants), inherently de-link R&D expenditures from product price, financing R&D by sources other than IP rent revenues. For the Initiative, DNDi has already secured EUR 9 million of the EUR 36 million needed. To develop a diagnostic tool based on quantitative PCR (qPCR) (Objective 2) a milestone or small end-stage prize is a suitable incentive for partners to better evaluate VL transmission via asymptomatic carriers and PKDL patients. Because R&D incentives are weakened by insufficient market potential, they fail to stimulate innovation. A milestone or small end-stage prize would stimulate investments to rapidly adapt the existing qPCRs to specific transmission risk-assessment needs for the Initiative. The qPCR technique could help correlate parasite load with transmission risk in asymptomatic and PKDL patients. It detects and quantifies parasite DNA. Similar methodologies exist but show varying levels of sensitivity and specificity in clinical VL, CL, MCL and PKDL. Additional investments are needed to develop more accurate qPCRs adapted to the regional VL variations, sensitive enough to detect very low parasite DNA in asymptomatic, antibody-positive carriers. The VL prize would notably reward a group already invested in qPCR and stimulate developing countries’ research orientations and researchers, thus strengthening capacities. A small prize, up to EUR 500 thousands would attract small organizations, and shift some costs of failure to the prize-funder rather than researchers. As highlighted by the CEWG report, the success of the prize will depend on the suitability of its design, including targeted cost and technical requirements (e.g. sensitivity) for the intended purpose. The Initiative steering committee and scientific advisory committee will define the design and rules for the prize following key principles of de-linkage (i.e. availability and affordable access) and compliance with the initiative’s IP and licensing rules (including open source publication of findings).
2. Utilizes collaborative approach: including open knowledge innovation approaches
Neglected diseases, where traditional market mechanisms do not attract investments and with limited funding resources, require open models for sharing knowledge and research data, particularly for upstream research, to identify promising new technologies/compounds.
The Drug Accelerator Consortium (hereafter ‘Accelerator’) proposed, based on current DNDi negotiations with several pharmaceutical companies, will be launched in 2014. It transcends existing approaches of bilateral agreements, and will pool resources, compounds, and expertise across companies,
3
expediting identification and selection of candidates for promising new chemical entities from lead optimization to pre-clinical research (Objective 1, Activity 1). The Accelerator would collectively adhere to the licensing practices described above, and reduce costs and time of the discovery phase of R&D. Outcomes would be placed into the public domain (e.g. through the EU Open PHACTS Discovery Platform) to catalyse further research. Specifically, the Accelerator’s activity would comprise searching and screening multiple libraries simultaneously and pooling capabilities of companies to identify more rapidly expanded hit series to quickly establish Structure-Activity Relationships that the Initiative could take through lead optimization and the full spectrum of R&D to implementation. It would provide access to state-of-the-art compound profiling assays and expertise with other leaders in NTD lead optimization (e.g. Drug Discovery Unit of Dundee University) to increase the capacity to identify a large number of top quality preclinical candidates and avoid duplication. The Innovative Medicines Initiative (IMI), a public-private partnership between the European Union and the European Pharmaceutical Industries and Associations with a EUR 2 billion budget, within the Horizon 2020 (EU Framework Program) would be an adequate mechanism to promote collaboration among pharmaceutical companies, academic groups, SMEs, and a PDP. Additional funding could be sought through this mechanism (see below).
The Initiative will implement a Data Sharing Platform to identify determinants of treatment efficacy and effectiveness (Objective 4). Working with WWARN, it will develop, under the principles described above, an open clinical and biological database (including pharmacology, in vitro and molecular parameters) to resolve scientific questions emanating from single studies. This requires technical expertise and a legal-ethical framework to pool anonymized patient data for research. Such expertise has been extensively developed by WWARN and malaria partners.
3. Utilizes licensing approaches that secure access to research outputs, and access to final products
The Initiative will secure innovative licensing terms (see Question 1) to make research outputs global public goods. Timely access to newly-generated knowledge and data is crucial to neglected diseases with high mortality rates (e.g. VL). The Initiative will provide open access to knowledge generated, including that of the Accelerator. Data from the Initiative will be presented and published in open access journals and publicly accessible databases (e.g. ChEMBL; WIPO Re:Search). The Initiative will apply an equitable access policy to all new therapeutic and diagnostic tools, based on agreed-upon principles that ensure affordable pricing, sustainable production, and de-linkage (see Objective 1 Activity 2). To ensure sustainable access, the Initiative will regularly review and propose enabling regulatory, financial, and procurement policies by engaging endemic-country regulators in to accelerate the registration.
4. Proposes and fosters financing mechanisms including innovative, sustainable and pooled funding
Leveraging the EUR 9 million already secured by DNDi for the Initiative, other appropriate pooled mechanisms will be approached:
- European & Developing Countries Clinical Trials Partnership (EDCTP-2), which expanded its scope to clinical trials in Africa for all Neglected Infectious Diseases (global budget: EUR 248 million, 2014-2015) (for clinical-trial activities).
4
- Innovative Medicines Initiative (IMI) co-funded by the European Commission and the pharmaceutical industry (in-kind contributions; to support the Accelerator).
- Global Health Initiative Technology Fund, initiated in 2013, co-financed by the Japanese government, the Japanese pharmaceutical industry and the Bill and Melinda Gates Foundation (global budget: USD 100 million, 5 years) for infectious disease R&D.
- Member States’ dedicated funding (including emerging economies that are endemic for VL, e.g. Brazil, India) for demonstration projects, managed as pooled funding for example via TDR.
New innovative funding sources (e.g. UNITAID; FTT), which require Member State decisions, protect long-term product development from shifting individual donor circumstances and priorities. The Initiative aims to constructively feed, by example, ongoing Member State discussions on such mechanisms.
5. Fosters effective and efficient coordination mechanisms amongst existing organizations/initiatives
The Initiative aims to demonstrate that R&D projects can be effective while strengthening coordination among multidisciplinary partners and through innovative R&D financing and coordination mechanisms, notably as VL affects EURO, SEARO, EMRO, AFRO, and PAHO. Seeking rapid health impact and a sustainable public health solution necessitates an integrated model for North-South and South-South collaboration. Constant strong involvement of endemic countries to define priorities and facilitate implementation of new tools, and innovative alliances with pharmaceutical and biotechnology companies and academia, are vital. DNDi, with no laboratories or manufacturing facilities, functions thanks to engagement of public and private partners (academia; public research institutions, particularly in endemic countries; pharmaceutical and biotechnology companies; NGOs; PDPs; and governments) by leveraging their assets, capacities, and expertise. The Initiative will partner with the LEAP clinical platform in Africa, EDCTP, IMI, CSIR and OSDD, in addition to DNDi’s pharmaceutical and academic partners. A steering committee elected among multidisciplinary partners, would embody these sectors.
6. Strengthens capacity for research, development and production, technology transfer in developing countries
- Technology transfer: Development of a new diagnostic technology for diagnosis of asymptomatics and PKDL patients by xenodiagnoses (Objective 2): Two steps: training courses and set-up of colony and infectivity experiments in Bangladesh, Sudan, India (2-year duration).
- Capacity Strengthening via the Prize for qPCR to evaluate the role of transmission in asymptomatics and PKDL. A pre-requisite for receiving the qPCR diagnosis Prize would be capacity-building.
- Clinical development of an existing drug candidate up to registration (Fexinidazole/VL2098) (Objective 1, Activity 3) with potential support of EDCTP and endemic countries, will enhance clinical trial capacity (including GCP, GLP, ethics, case management, regulatory capacity) in Asia, Africa, and Latin America, through DNDi’s platforms and other research networks. Fexinidazole for VL is now in clinical trial, driven by LEAP. With wide-range disease strains, the same GCP-standard clinical trials in different regions will differentiate geographical immune responses.
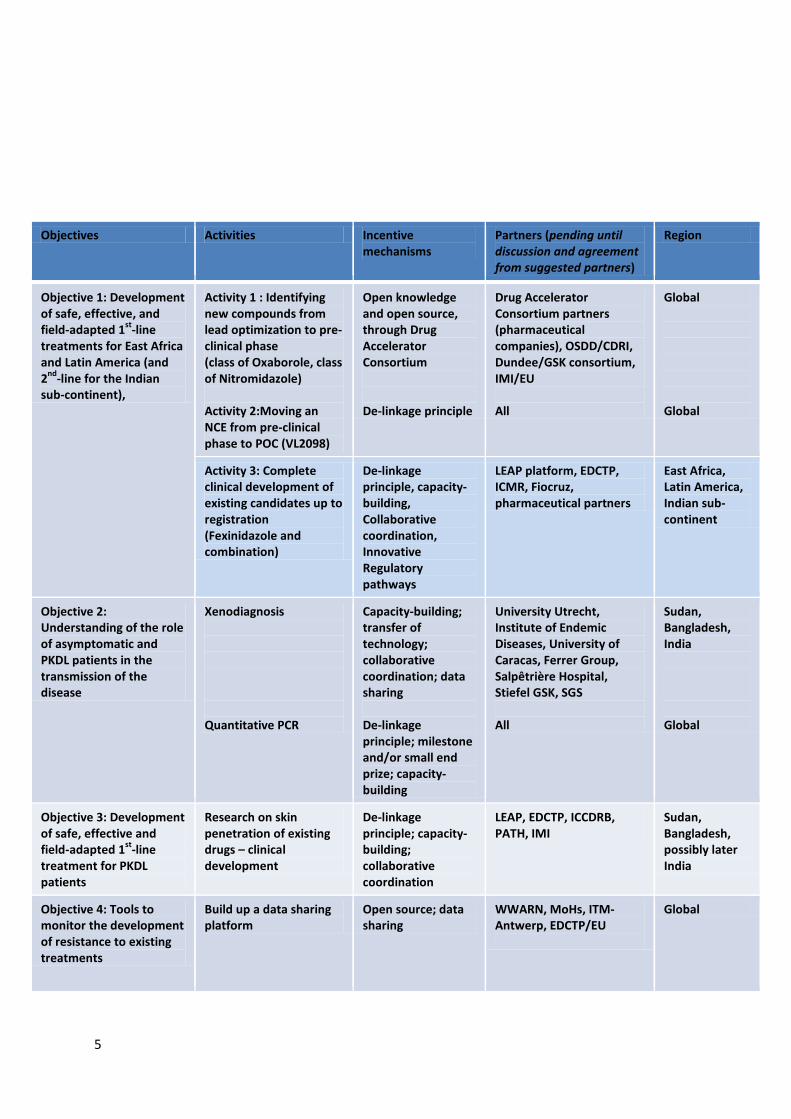
5
Objectives Activities Incentive mechanisms
Partners (pending until discussion and agreement from suggested partners)
Region
Objective 1: Development of safe, effective, and field-adapted 1st-line treatments for East Africa and Latin America (and 2nd-line for the Indian sub-continent),
Activity 1 : Identifying new compounds from lead optimization to pre-clinical phase (class of Oxaborole, class of Nitromidazole) Activity 2:Moving an NCE from pre-clinical phase to POC (VL2098)
Open knowledge and open source, through Drug Accelerator Consortium De-linkage principle
Drug Accelerator Consortium partners (pharmaceutical companies), OSDD/CDRI, Dundee/GSK consortium, IMI/EU All
Global Global
Activity 3: Complete clinical development of existing candidates up to registration (Fexinidazole and combination)
De-linkage principle, capacity-building, Collaborative coordination, Innovative Regulatory pathways
LEAP platform, EDCTP, ICMR, Fiocruz, pharmaceutical partners
East Africa, Latin America, Indian sub-continent
Objective 2: Understanding of the role of asymptomatic and PKDL patients in the transmission of the disease
Xenodiagnosis Quantitative PCR
Capacity-building; transfer of technology; collaborative coordination; data sharing De-linkage principle; milestone and/or small end prize; capacity-building
University Utrecht, Institute of Endemic Diseases, University of Caracas, Ferrer Group, Salpêtrière Hospital, Stiefel GSK, SGS All
Sudan, Bangladesh, India Global
Objective 3: Development of safe, effective and field-adapted 1st-line treatment for PKDL patients
Research on skin penetration of existing drugs – clinical development
De-linkage principle; capacity-building; collaborative coordination
LEAP, EDCTP, ICCDRB, PATH, IMI
Sudan, Bangladesh, possibly later India
Objective 4: Tools to monitor the development of resistance to existing treatments
Build up a data sharing platform
Open source; data sharing
WWARN, MoHs, ITM-Antwerp, EDCTP/EU
Global