Embed Size (px)
Citation preview

450 LEcouRs: INTRA-ABDOMINAL PRESSURES aNov.1946 vol.P~~~~~~~~~~~~~~~~1Nv 96 o.5
tolerance curve was not flattened. A barium seriesshowed: (1) Fragmentation and scattering of the barium.(2) Loss of the normal feathery pattern of the smallbowel mucosa. (3) The appearance of sausage shapedloops of bowel.
The radiologist's report indicated a typical deficiencypattern consistent with the diagnosis of sprue syndrome.*X-rays of the bones showed moderate osteoporosis.Chemical examination of the stools showed: total fat,70% of dried feces; neutral (unsplit fat), 23% oftotal fat; fatty acids (split fat), 77% of total fat.
The chemical findings in the stool indicated thatpancreatic function was adequate, and that the steator-rhcea was the result of deficient absorption rather thanimpaired digestion.
These findings were considered to be diagnostic ofthe sprue syndrome and a treatment plan was outlined,as above, to include diet, liver therapy, vitamins andhydrolyzed protein parenterally.
The results of treatment were satisfactory, withimprovement in the diarrhoea and a gain of 17 lb. withintwo weeks. There was little change in the htumatologicalfindings, which had not been conspicuous at the begin-ning of therapy. We considered that the dramaticclinical response constituted a satisfactory therapeutictest and corroborated the original diagnostic impression.Unfortunately the patient left hospital against advicebefore treatment had been completed, and evaluation ofthe long range results of treatment was impossible.
We believe that this case falls into the groupwhich we would classify as "secondary" sprue.The basic etiology, we consider to be, either (a)disturbance of the anatomical relationships ofthe small bowel or (b) comparable to Hurst'scase of sprue syndrome secondary to mesenterictuberculosis.
Since the above case was studied, we haveobserved another patient in which imperativesurgical interference, occasioned by gangrene ofthe small bowel, resulted in a comparable syn-drome in which the hlematological findings wereoutstanding and the alimentary symptoms sec-ondary. Satisfactory response of both dis-turbances resulted from parenteral liver therapyalone. The latter case, we believe, also supportsthe view that secondary or "mechanical" sprueshould be recognized as an entity.
CONCLUSIONS1. The steatorrheea characteristic of the sprue
syndrome is due to impaired fat absorption fromthe small intestine.
2. The etiological factors should be recognizedas falling into two groups: (a) Deficiency of"extrinsic" and "intrinsic" factors as in per-nicious anaemia. (b) Mechanical factors pre-venting absorption from the small bowel, suchas lymphatic obstruction and operative dis-turbances of anatomical relationships.
3. Deficiencies of ingestion and absorption* We are indebted to Dr. J. W. MacKay, Radiologist,
Montreal General Hospital, for the radiological inter-pretations. Specimen radiographs are shown in Fig. 1.
produce heematopoietic disturbances similar tothose of pernicious anemia.
REFERENCES1. GEE, S.: St. Barth. Hosp. Rep., 24: 17, 1888.2. CASTLE, W. B., RHOADS, C. P., LAWSON, H. A. AND
PAYNE, G. C.: Arch. Int. Med., 56: 628, 1935.3. HURST, A.: Guy's Hosp. Rep., 91: 1, 1942.4. HANES, F. M.: Am. J. M. Sc., 204: 436, 1942.5. MOORE, C. V., VILTER, R., MINNICH, V. AND SPIES, T.
D.: J. Lab. tClin. Med., 29: 1226, 1944.6. DARBY, W. J., JONES, E. AND JOHNSON, H. C.: J. Am.
M. Ass., 130: 12, 1946.
INTRA-ABDOMINAL PRESSURES
By R. Lecours, M.D.St. Jacques (Montcatm), Que.
IN 1930 Livingston' wrote: "In contrast tothe frequency with which this term intra-
abdominal pressure appears in surgical writ-ings, little or no reference to the subject isfound in textbooks of physiology. Thesesource books offer little aid."
This statement still keeps all its freshnessin 1946, for even the most recent treatises onphysiology have not yet found a place in theirindex for the term " intra-abdominal pressure ".The number of special articles on it publishedin the U.S.A. in the last 30 or 35 years wouldHGt be over 12.2 to 10
PHYSIOLOGICAL AND PATHOLOGICAL ASPECTSAmono the nuimerous phenomena which are
likely to influence the intra-abdominal pressures(I.A.P.) or to be influenced by them, pulmonaryrespiration deserves an important rank. Respi-ration, even of the most quiet type, would notpermit complete rest in the abdominal cavityunless this thoroughly changed its form, itsdimensions, and, consequently, its internal pres-sures at least 30 times in a minute. Althoughwe read in Best and Taylorll that " thediaphragm is the chief muscle of respiration,its movements being responsible during deepbreathing for 60%o of the total amount of airbreathed ", we still cannot forget that thediaphragm constitutes one of the great muscu-lar segments of the abdomen. This being so,I cannot but think that a significant proportionof the respiratory act until now attributed tothis important muscle should really be ascribedto the physiological play of I.A.P. This shouldespecially be so when, in considering coughing,we realize that this abdomino-thoracic partitionhas no great respiratory value except inasmuchas, supporting itself against the closed glottisand the thoracic contents, it participates in the

Canad. M. A. J. 1Nov. 1946, vol. 55 1 LECOURS: INTRA-ABDOMINAL PRESSURES
"mise-en-tension" of the abdomen with theother muscles of the abdominal periphery.The lung specialist has certainly done well
not to wait for a more thorough knowledge ofI.A.P. physiology before carrying out the injec-tion of large quantities of air into the peri-toneal cavity, as have Banyai,12' 13 Rilance,14LaRue-Henderson'5 and many others. Thisprocedure, however, should modify the statusof abdominal pressures for a long while. Whenthe same specialist, by direct surgical actionupon the phrenic nerve, obtains a pulmonarycollapse, he will probably admit with us thatthe desirable effects of the rise of the paralyzedhemidiaphragm can be explained, at leastpartially, by the effects of the repeated eleva-tion of I.A.P. It is indeed my opinion that,even after phrenic nerve surgery, coughing,straining at stool, or any other severe physicalefforts are still able to produce very high peaksof pressure inside the abdomen, which directlyreact on the denervated hemidiaphragm. A
third example of the lung specialist being ableto modify profitably the I.A.P. is when, withAlexander and Kountz,'6 he treats serious cases
of pulmonary emphysema by the wearing of a
special belt "in order to maintain an adequateintra-abdominal pressure''.The gastro-enterologist is regularly consulted
by those thin and elongated patients who sufferfrom various symptoms and, among many othertherapeutic measures, he often prescribes tothem the wearing for a long time of an indi-vidually -designed corset, thus trying to bringabout permanent relief of their symptoms bythe use of a permanent artificial abdominal wallwhich would raise their I.A.P. to a comfortablelevel. He may recognize too that some cases ofgastric ulcer in man do not fit their psycho-neurotic etiology (that dernier cri!) and, then,if he reads A. C. Vietor,17 he will find many
good reasons to consider splanchnkoptosis as "a
potential anatomical path to gastric and duo-denal ulcers". Where then is the explanationof splanchnoptosis if not in the physiopath-ology of the I.A.P.?The cardiologist does not forget that the
variations, respiratory or others, of the I.A.P.may constitute one of the most importantfactors in the blood circulation. As early as
1926, A. E. Fossier'u considers essential hypo-tension as a symptom of splanchnoptosis; itmust be our aim to increase the abdominal pres-sure, "thus raising the diaphragm and thereby
giving a better support to the heart". In 1940,W. S. McCann19 attributes some cases of ortho-static hypertension to visceroptosis. Also in
1940, N. C. Gilbert et al.20 have tried with some
success to demonstrate the action of gastricdistension pressures on the circulation in thecoronary arteries.Though, generally speaking, it might be said
that hernia is probably one of the most easilydiagnosed and most adequately treated humandiseases, the pathogenesis of this so well-defined syndrome is still a subject of debate.In 1945, Minty and Minty21 say: "The weightof medical opinion in regard to the cause ofhernias is that they are a result of a congenitalweakness in the individual"; but in 1917Pitzman-Marsh22 said: "The theory of con-
genital malformations as the cause of herniareached the height of its popularity about 20years ago". We turn then to the opinion ofM. Cherner23 who, in 1940, wrote: "In spite ofall discussions, both written and oral, upon thesubject of hernia, the problem seems to be ofas much interest and importance today as itwas fifty years ago". Once more we ask thequestion: where is the explanation of herniaand its recurrence or re-recurrence if not inthe physiopathology of the I.A.P.? We couldcontinue in this vein for a long time. Forinstance, in accord with recent articles pub-lished, we could put forward the importance ofI.A.P. studies to the gynaecologist, the urologist,the obstetrician, and other specialists. Let itbe sufficient to sum it up by pointing outprosaically, that you cannot sit down or getup, you cannot lift burdens, walk, cough or
sneeze, expel any foreign body from one endor the other of your alimentary tract, laugh,sing, speak loudly or even breathe deeplybefore you have created, consciously or not,the necessary amount of pressure in your
abdomen.
TERMINOLOGY
Some definition of the principal terms to beused is necessary.
1. The abdominal cavity.-This is the spacelimited by the diaphragm above and themusculo-aponeurQtic perineum below, by thelumbo-sacral column posteriorly and the walls
of the abdomen antero-laterally. We considerthe pelvic cavity as a purely conventionaldivision of the abdominal cavity. From the
point of view of I.A.P. studies, it does not exist.
451

IJECOURS: INTRA-ABDOMINAL PRESSU'ES [eCanad. M. A. J.XL Nov. 1946,VO. 55
2. The abdominal contents. 'The abdoniinalcavity contains the whole of the digestivesystem, less the cesophagus; the whole of the*genitourinary system, less part of the urethraand vagna-; many important blood vess.els andlymphatic organs; and, moreover, a serous
membrane, the peritoneum, which has oftenmisled and sometimes completely mystifiedexperimentors on I.A.P.One has to take the peritoneum for what it
is. Indeed, if the peritoneum, considered inall its anatomical details, virtually takes up a
large space submitted to the laws of I.A.P. as
are the rest of the abdominal contents, it alsoforms, by the numerous folds of its perivisceralsheets, many ligaments and mesenteries- whosefunctions are to support afferent and efferentcirculation and innervation and, also, to opposetheir action to that of gravity upon severalabdominal organs.
3. The intra-abdominal pressures.-Under this
term we wish to include all pressure phenom-ena that may possibly take place within thelimits of the abdominal cavity.
Personally, I do not like this prefix "intra"which is so persistently added to the term"abdominal pressure". Whilst there can beabdominal pressures due to extra-abdominalcauses, I think there is too much chance of thisnot very useful prefix making the term "intra-abdominal pressures" into a misnomer. Never-theless, I shall continue to use the word"intra" throughout this article, but only for-tradition's sake.
4. The modalities of intra-abdominal pressure.-1In principle, all parts of the abdominal con-
tents are capable of being influenced by I.A.P.In practice, however, one cannot conceive thepossibility of.measuring the I.A.P. everywherein the abdomen. For example, it would not befeasible to measure the pressure that. existsat a certain moment in the middle of thehepati parenchyma. Practically as well as
theoretically one may say that I.A.P. can bemeasred wherever an intra-abdomina fluid,natural or artificial, can transmit the pressuresexerted upon it to an extra-abdominal mano-
meter. As8the abdomen is, 1fter ally a greathollow muscle, it may therefore be said thatall these pressures, fall under two groups ofmodalities.'"A" modalities.-The I.A.P. can be studied
either inside the hollow vilsera of the abdomen
-intestine, bladder, stomach, etc.,9 or outsidethese same organs. There are therefore twomodalities of the I.A.P., namely, the intra- orendo-visceral pressures; and the intra-peri-toneal pressures.
Here, again, the particle "intra" appears as
a useless prefix to the term "visceral" and"p.ritoneal pressures". In fact, if one isthinking about intra-visceral pressures he willeasily refer to all other abdominal pressures as
being extra-visceral, i.e., intra-peritoneal. Onthe other Jiand, if one is thinking about intra-peritoneal pressures one will easily refer allother abdominal pressures as being extra-peritoneal. i.e., intra-visceral.
Until now ttle terms intra-peritoneal andintra-abdominal pressure have often been lakenas synonymous in the medical literature. Thevhave even been very freely exchanged in the samearticle. For example, it has been written:"There is always a variable amount of pressure
in the peritoneal cavity, known as intra-abdominal pressure "' ;4 or "Briefly stated,intra-abdominal pressure, or more specially,intra-peritoneal pressure, is the ,.resultant of
24 or "That intra-abdominal pressureis normally negative is satisfactorily demon-strated by clinical observations and laboratoryexperiments" ;6 or even, "The intra-abdominalpressure is not intra-peritoneal but rather endo-visceral in its manifestations and, under normalcircumstances, is made to equa} the atmosphericpressure by the degree of tone of the abdominalmusculature"25 C. R. Lam10 has made laud-able efforts to bring to an end this' confusionof ideas and concepts, but, unfort'unately, hecontinues to classify the I.A.P. under the threeold headings, the intra-abdominal pressure, theintra-peritoneal, and the intra-visceral pres-
sures > thus failing to note that the second andthird of these terms cannot indicate more thanmodalities of the I.A.P. -Intra-visceral pressureis to be regarded as the variable amount ofpressure developed in a hollow abdominal viscus
by the actual tonus of its own parietal muscu-
lar fibres or by distension of ingestive, secretory
or excretqry origin.From the point of view of general physi-
ology, our division of the I.A.P. into these two
modalities would probably appear more didac-'tic than practical. This we concede, but it is
obvious that the study of some pgrticular intra-
452

Canad. M. A. J. 1Nov. 1946, vol. 55j LECOURS: INTRA-ABDOMINAL PRESSURES
visceral pressure can afford much information.A number of recently published articles on thesubject of cystometry has already proved theimportance of measuring intra-vesical pres-sures. Intra-gastric minute variations of pres-sures have also recently been studied byThornton et at.26 as a means of emphasizingthe value of the section of vagus nervebranches-in the treatment of gastric ulcer."B" modalities.-The I.A.P. can be studied
either during the conscious or unconscious restphase of the abdomen's muscular walls, orduring their total or segmentary active phase,whence we have two other important forms ofthe I.A.P., namely: the static intra-abdominalpressure (S.I.A.P.), and the dynamic intra-abdominal pressure (D.I.A.P.).The S.I.A.P. is to a large extent, a relation
between the weight and volume of the abdominal
contents and the capacity of the abdominalcavity, which capacity also depends on the stateof tonicity of the abdominal muscle. As will beproved later on, posture is the most direct factorin causing variations of these pressures.The D.I.A.P. is the pressure exerted on the
abdominal contents by any voluntary or auto-matic contraction of one or a group of abdominalmuscles. As will be seen later on, when theabdominal cavity has reduced its potentialcapacity by assuming its most spherical form,that is after a deep inspiration and closure ofthe glottis, and when the entire abdominalmuscle energetically contracts, very high pres-sures are created and transmitted to and throughall parts of the abdominal contents. Only underthese conditions do the abdominal coLitents be-have like a true hydrostatic medium in a rigidcontainer.
Fig. 1.-A: Man, aged 21, abdominal circumference 33", height 68", weight 153 lb.B: Woman, aged 29, abdominal circumference 36", height 63", weight 175 lb.a-Ib: Initial supine posture.b - c: Knee-chest.c - d: Erect.d - e: Second supine posture in A and prone-horizontal in B.
Every point marked with a letter indicates either a change in posture, or a stop varying from 15 to 60seconds in the unrolling of the kymograph paper.
Every marked rise has been produced by violent coughing.
453
Boo.
aC
6t....5417qn*W$ *
... . . .. ... .. - .. . . .. . . . . . .. . ... - . ... ... ... . . ...
c A. .... ... . . - . .. .. Z-
LECOURS: INTRA-ABDOMINAL PRESSURES [ Canad. M. A. J.L Nov. 1946, vol. 55
THE PRACTICAL MEASUREMENT OF HUmAANINTRA-ABDOMINAL PRESSURE
As I am aware that I.A.P. and its variableshave been one of the most neglected subjects inthe field of general physiology, and, as I believethat no further progress can be made in thephysiopathology of these pressures so long as
physicians are without an accurate and easy
method of measuring them, I have evolved a
method which seems to enable us to register anyvariation of the I.A.P. This method has been
qualified by a friend as "discouragingly"simple, but I present it as it is, h9ping that itwill be improved on if found inadequate.
Small rubber balloons of 10 c.c. capacity weremade from hand-sealed surgical drains and fixedat the end of convenient rubber tubings. Theseballoons were then introduced into differentparts of the abdominal ecavity and inflated with8 e.c. of air. The tubes were subsequently con-
nected to not too sensitive but sturdy enoughmetallic tambours whose excursions under pres-
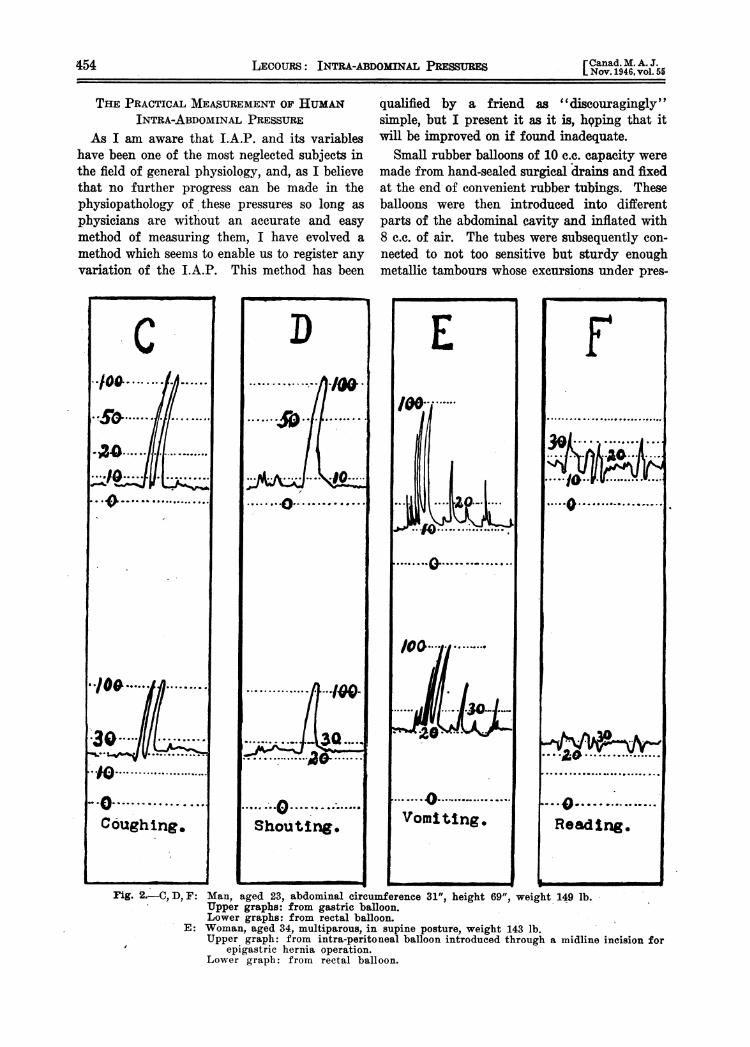
Fig. 2.-C, D, F: Man, aged 23, abdominal circumference 31", height 69", weight 149 lb.Upper graphs: from gastric balloon.Lower graphs: from rectal balloon.
E: Woman, aged 34, multiparous, in supine posture, weight 143 lb.Upper graph: from intra-peritoneal balloon introduced through a midline incision for
epigastric hernia operation.Lower graph: from rectal balloon.
454

Canad. M. A. J. 1Nov. 1946, vol. 55 ] LECOURS: INTRA-ABDOMINAL PRESSURES
sure were transmitted through ordinary multi-plying devices and registered upon an electrickymograph at any desired speed.
Fig. 1 shows 2 abdominographs taken frommy own series. I shall not discuss the truesignificance of every fluctuation in these graphs,neither shall I compare them with each other,because I feel that no valuable scientific datacan be gained from such comparisons unless onehas at least many hundreds of identical recordsto compare. My purpose in presenting thesegraphs is to prove the ease with which a goodnumber of S.I.A.P. and D.I.A.P. variations can
Gc
.V
- '---~:*. 0
c
be registered in the same short session-about15 minutes -by introducing a small rubberballoon just above the anal sphincters. Tinywaves seen on graph A, between b and d, arelocal respiratory I.A.P. variations. As can beobserved on Fig. 3-G, these variations mayeventually be of greater absolute value. Amongthe interesting features of graph B, are the threelong waves of peristaltic rectal contraction whichcan be noticed between d and e, and, if myreasoning is correct, the height of these wavesis the true measure of this intra-visceral pressure.
455
I
~.6. ........ . ...........,

LECOURS: INTRA-ABDOMINAL PRESSURES [Canad. M. A.J.L Nov. 1946, vol.55
Fig. 2 presents 4 metrogram of D.I.A.P. vari-ations registered simultaneously at two distantpoints of the abdominal contents. Azty one ofthe graphs' C, D or E, is the picture of a par-
ticular strong abdominal muscle contraction.The ensemble of these 3 graphs makes it obviousthat a strong muscular contraction of the totalabdominal periphery will bring about the same
peak of high pressure at any point of the ab-dominal contents where, prior to this contrac-tion, the initial static pressure was 5, 10, 20,30 or even 40 mm. Hg. Henice, it is suggestedthat the most generalized and active I.A.P. vari-ations can be measured with as much accuracy
at a single point of the abdominal contents as
by simultaneous measurements at several distantpoints. This would give extra value to the inter-pretation of Fig. 1 graphs which were registeredfrom a single balloon introduced into the mostaccessible abdominal viscus. Graph F gives an
example of moderate D.I.A.P. variations. Itshows an overall correspondence of the pressure
waves registered at two distant points in theabdomen while these points were submitted tothe same cause of variation in local pressure,
but, as the physical exercise involved in thisexperiment did not require a complete andviolent participation of the entire abdommialmuscle, it does not show identical summits ofhigh pressure in both waves.
All 4 graphs of Fig. 3 have also been recordedthrough reetal balloons. I think these graphswill give some idea of the S.I.A.P. pathologicalvariations one may expect to encounter whenthe observed subjects are asked to assume theknee-chest posture. G probably tells the simplestory of a normal uterine retroposition. H illus-trates the poor mobilization of the pelvic viscera
in a case of chronic parametritis and left chronicsalpinx. Both I and J are chapters of thegastroenteroptotic romance, but J, objectively,and subjectively, is much more pathetic.
Negative intra-peritoneal pressures under thediaphragmatic dome have often been reportedby experimenters. "$ecause of the locationof the abdomen", writes Livingstonl, "sepa-rated from the pleural cavities only by a thinmusculo-fibrous membrane, the upper portionsof the peritoneal cavity display a slight reflectednegativity, subatmospheric or tension pheno-menon showing the presence of an upwardpulling force". I am ready to endorse thisgenerally approved concept of the subdiaphrag-
matic peritoneal negativity and. will even agreeto give up the knee-chest "garrulitis vulv&'to the physiology 'of the pleura if it can beproved that these two negative-pressuredserous membranes can, by their sole existence,increase the abdominal capacity. Fig. 4 -K
I
Fig. 4
K: Gastric negative pressure induced by bulging outthe thorax and abdomen after a deep expiration(a - b).
L: Example of regular pelvic negative pressure in-duced by assuming the knee-chest posture (b -c).
shows what happens within the stomach when,after a deep expiratory movement, the erectman bulges out his thorax and abdomen while,his glottis remains closed. As can be noted,this procedure develops an important negativ-ation of the I.A.P. in the stomach, as itprobably induces a strongly negative intra-pleural pressure, but there seems to be no gQodreason to believe that the subdiaphragmaticperitoneal space would not participate in thisgastric negativity, at least as much as it par-ticipates in the pleural negativity. As shownin Fig. 4 - L, the I.A.P. measured in the rectumis often found to be negative when the subjectassumes the knee-chest posture, and we thinkthis phenomenon presents a close analogy withthe subdiaphragmatic peritoneal. negativity in
the erect posture. Both of these negativitiesprobably come from a normal disproportionbetween the abdominal. capacity, which is oftengreater, and the volume of the abdominalcontents, which is often less.
COMMPNTThe suspended solution of so many clinical
problems more or less intimately connectedwith the I.A.P. appear to us as a stimulant to
456 X
i

Nov.1946vol. 1 FRASER: ULTRAVIOLET RADIATION 457
a fair study of the normal and pathologicvariations of these pressures. The few graphshereby reproduced merely lift a corner of theveil which conceals the laws of I.A.P. variationsin man. The relative inadequacy of our ownmeasuring equipment and, also, the lack ofpublication space, prevent us from trying justnow to unveil more of these laws. For instance,static I.A.P. variations have been studied onhuman subjects lying on a tilting device andrecords have been made while the tilting boardwas slowly moved from a 75 degree head-up to a75 degree head-down position. Two or threegraphs obtained through this procedure wouldgive weight to the opinion that the static pres-sures in the upper abdomen might not increasein the same proportion as they decrease in thepelvis when the subject, prone or supine, is pro-gressively brought from the horizontal to thehead-down position. In other words, the staticpressures encountered in and around such im-portant abdominal viscera as the stomach, theduodenum, the transverse colon, the liver, thegall-bladder, the pancreas, the spleen and eventhe kidneys, are lower in the erect posture thanthe corresponding static pressures in the pelvis,but, though such extreme attitudes as the head-down position or the knee-chest posture wouldsubstantially diminish the static pressures in thelower portion of the abdominal cavity, theywould not increase to the same degree the cor-responding static pressures in the above men-tioned viscera. If this theory. happens to beconfirmed by further experiments, it wouldestablish the fact that, whatever may be theliabitual posture of the subject, the easy bloodirrigation of the aforesaid organs and, -con-sequently, their comparatively high secretoryand peristaltic activities, are not interfered with.
SUMMARY
1. The importance of I.A.P. studies is stressed.2. A new concept of I.A.P. definitions and
classifications is formulated.3. A personal method for registering the
I.A.P. variations is described.4. Preliminary statements are made regarding
the general laws of I.A.P.
It is a pleasure to thank Dr. Eugene Robillard, chiefof the laboratory of general physiology at the Universityof Montreal, for his continued counsel and interest dur-ing the course of this work.
REFERENCEs1. LIVINGSTON, E. M.: AM J SUrg., 8: 1930.2. EMERSON, H.: Arch. Imt. Med., 7: 755, 1911.3. NOB, Ga H.: Burg., (Gln. & Obst., 20: 45, 1915.4. Comrn, R. C.: J. Am. M. Ass., 69: 683, 1917.5. COOMB, H. C.: Am. J. Physiol., 61: 159, 1922.6. WAGoNE, R. H.: Am. J. M. Sc., 171: 697, 1926.7. OVERHOLT, R. H.: Arch. Burg., 22: 691, 1931.8. MURPHY, D. P. AND MENGERT, W. F.: Burg., Gyn.
Obat., 57: 487, 1933; Ibid.: 57: 745, 1933.9. SALEIN, D.: Am. Rev. Tubero., 30: 436, 1934.
10. LAm, C. R.: Arch. Surg., 39: 1006, 1939.11. BEST, H. C. AND TATYOR, N. B.: The Physiological
Basis of Medical Practice, The Williams & WilkinsCo., Baltimore, p. 505, 1943.
12. BANYAI, L. A.: AM. Rev. Tuber¢., 29: 603, 1934.13. Idem: Radiology, 31: 48, 1937.14. RILANCE, A. B. AND WARRING, F. C.: Am. Rev. Tuberc.,
44: 323, 1941.15. LARUE-HENDERSON, N. AND WINN, W. D.: Am. Rev.
Tuberc., 52: 380, 1945.16. ALEXANDER, H. L. AND KOUNTZ, W. B.: Am. J. M. So.,
187: 687, 1934.17. VIETOR, A. C.: Rev. Gastroenterol, 7: 203, 1940.18. FossisR, A. E.: Am. J. M. BS., 177: 496, 1926.19. MCCANN, W. S. AND ROMANSKY, LM J.: J. Am. M.
Ase., 115: 8, 1940.20. GLBERT, N. C., ENN, G. K. AND LEROY, G. V.: J. Am.
M. Ass., 115: 1962, 1940.21. MINTY, E. W. AND MINTY, F. W.: M4fm Med., 28: 723,
1945.22. PITZMAN-MARSH: J. Am. M. Ass., 69: 766, 1917.23. CHERNER, M.: Am.J.. Burg., 48: 641, 1940.24. STURMDORF, A.: Gynoplastic Technology, F. A. Davis
& Co., Philadelphia, 2nd ed., 1923.25. WILENSKY,, A. 0. AND KAUFMANN, P. A.: A* Surg.,
106: 373, 1937.26. THORNTON, T. P., STORER, E. H. AND DRAGSTEDT, L. H.:
J. Am. M. Ass., 130: 764, 1946.
FURTEER STUDIES ON ULTRAVIOLETRADIATION IN SURGERYBy Roy Fraser, M.A., F.R.M.S.
Professor of Bacteriology,Mount Allison University, Sackville, N.B.
IT has been stated recently that there are now1,500 hospitals and 300 schools in the United
States which are provided with ultravioletgermicidal equipment for air purification. Theinstallations are in various parts of the hospi-tal, including in some cases the operatingrooms. The extensive and increasing adoptionof such protective equipment seems to be dueto the recognition by hospital authorities offour facts:
1. The development of aerobiological studiesand the consequent understanding of the im-portance of air-borne micro-organisms in medi-cine, surgery, and public health.
2. The efficiency of ultraviolet germicidalradiation as demonstrated both experimentallyand in widespread practical use.
3. The safety of such radiation when testedby experimental methods and clinical experi-ence, provided the proper precautions are ob-served at all times.
4. The acceptance of the Council on PhysicalMedicine of the American Medical Associationof standard ultraviolet equipment for the uses





























