Embed Size (px)
Citation preview

Drexel University College of Medicine
Surgery for Inflammatory Bowel Disease
David E. Stein, M.D.
Division of Colorectal Surgery
Department of Surgery
Drexel University College of Medicine

Drexel University College of Medicine
Inflammatory Bowel Disease
• Ulcerative Colitis and Crohn’s Disease
• Different Disease Entities
• Treatment changes based on disease type and pattern of disease

Drexel University College of Medicine
Crohn’s Disease

Drexel University College of Medicine
Crohn’s Disease
• Chronic inflammatory condition of uncertain etiology
• Patients present with a chronic history of GI complaints– Episodic cramping and diarrhea
• May take two years until diagnosis
• Incurable
Drexel University College of Medicine
Disease Sites
Small bowel
Ileocolic (40%)
Colon and/or rectum
Other
• Stomach and/or duodenum
• Anal canal and/or perineum
Drexel University College of Medicine
Operative Incidence
Jejunoileitis: 50% at 5 years; 70% at 10 years
Ileocolitis: 75% at 5 years; 70% at 10 years
Colitis: 50% at 5 years; 70% at 10 years
Whelan 1985
Drexel University College of Medicine
Treatment Caveats
Exclusion of infectious causes
Recognition of disease extent
Presence of complicating disorders

Drexel University College of Medicine
Medications
5-ASA compounds
Anti-microbials
Corticosteroids
Immune-modulating agents

Drexel University College of Medicine
Immune-Modulating Agents
Methotrexate
Azathioprine and 6-MP
Cyclosporine

Drexel University College of Medicine
Mild or Moderate Disease
Outpatient therapy
• 5-ASA compounds (topical or oral)
• Anti-microbials
• Corticosteroids
• Immune-modulating agents

Drexel University College of Medicine
Severe Disease
Inpatient therapy
• Corticosteroids
• Anti-microbials
• 5-ASA compounds (topical or oral)
• Immune-modulating agents

Drexel University College of Medicine
Operative Indications
Disease complications
• Toxic colitis or megacolon
• Perforation
• Hemorrhage
• Cancer risk
• Obstruction/Strictures
Drexel University College of Medicine
Operative Indications
Failure of medical therapy
• Unresponsive disease
• Incomplete response
• Excessive steroid requirements
• Complications due to medications
• Noncompliance with medication

Drexel University College of Medicine
Operative Options
Bypass
Resection with/without anastomosis
Strictureplasty

Drexel University College of Medicine
Operative Considerations
• Crohn’s disease is incurable
• Death most common from operative complications
• Surgery most often for intestinal complications
• Operative options are influenced by a myriad factors

Drexel University College of Medicine
Operative Considerations
• Asymptomatic disease should be ignored
• Non-diseased bowel can be affected
• Mesenteric division can be difficult
• Resection margins should be conservative
• Use effective, long-term drainage of sepsis

Drexel University College of Medicine
Patient Preparation
Counseling
Stoma site marking
Restoration of physiologic deficits
Medication withdrawal
Steroids
Mechanical and antibiotic preparation

Drexel University College of Medicine
Resection

Drexel University College of Medicine
Resection
Procedure of choice
Operative principles
• Adequate mobilization
• Minimal contamination
• Suture ligation of mesenteric pedicles
• Conservative resection margins (<2-5 cm)
Drexel University College of Medicine
Anastomosis
Configuration and technique unrelated to recurrence
Operative principles
• Inspect mesenteric mucosa for ulceration
• Equilibrate lumen size
• Tension- and torsion-free anastomosis
• Close mesenteric defect
Drexel University College of Medicine
Temporary Stoma
Incompletely drained sepsis
Excessive blood loss
Prolonged operation (>4 hours)
Severe hypoalbuminemia (<2.5 g/dL)

Drexel University College of Medicine
Strictureplasty

Drexel University College of Medicine
Strictureplasty
Indications
• Multiple strictures in long segment
• Existing or impending short bowel syndrome
• Non-phlegmonous, fibrotic stricture

Drexel University College of Medicine
Strictureplasty
Contraindications
• Multiple strictures in short segment
• Phlegmonous or fistula-related stricture
• Free or contained perforation
• Hypoalbuminemia (<2.0 g/dL)
• Colonic strictures
Drexel University College of Medicine
Strictureplasty
Short (<10 cm) segments
• Heineke-Mikulicz
Long segments
• Finney
• Side-to side isoperistaltic
Michelassi 1996

Drexel University College of Medicine
Specific Disease Sites
Stomach and/or duodenum
Small bowel
Ileocecal
Colon
Rectum
Anal canal and/or perineum

Drexel University College of Medicine
Anoperineal Disease

Drexel University College of Medicine
Anoperineal Disease
Frequency of lesions: 40-80%
Influence of intestinal disease site:
• Colonic disease: 47-92%
• Small bowel disease: 26-74%
Fielding 1972, Rankin 1979

Drexel University College of Medicine
Anoperineal Disease
Classification
• Skin lesions
• Anal canal lesions
• Fistulae/abscesses
Buchmann and Alexander-Williams 1980

Drexel University College of Medicine
Anoperineal Disease
Skin lesions• Maceration• Erosion• Ulceration• Skin tags
Anal canal lesions• Fissure• Ulcer• Stenosis
Fistulae/abscesses

Drexel University College of Medicine
Hemorrhoids and Skin Tags
Conservative approach
Excision
• Poor healing: 12-25%
• Proctectomy: 30%
Jeffery 1977, Wolkomir 1993

Drexel University College of Medicine
Anal Ulcer
Asymptomatic
Painful
• Control sepsis, antibiotics
• Sitz baths
• Regulation of bowel movements
• Cortisone suppository or injection

Drexel University College of Medicine
Fistulae
Operative options
• Non-cutting seton
• Fistulotomy
• Rectal mucosal advancement flap
• Cutaneous advancement flap
• Fecal diversion (temporary or permanent)

Drexel University College of Medicine
Abscesses
High index of suspicion
Consider EUA
Incision and drainage
Avoid primary fistulotomy
Adjuvant antibiotics
Solomon 1993

Drexel University College of Medicine
Specific Problems
Abdominal abscess
Fistulae
Free perforation
Hemorrhage
Colonic stricture
Ileal pouch

Drexel University College of Medicine
Conclusions
The treatment of Crohn’s disease focuses on ameli-oration of symptoms while minimizing morbidity and maintaining intestinal continuity through the joint efforts of gastroenterologists and surgeons.
Operative therapy for Crohn’s disease is based upon symptoms, disease extent, and clinical presentation.

Drexel University College of Medicine
Ulcerative Colitis

Drexel University College of Medicine
Ulcerative Colitis
• Disease is more common in Caucasians
• Incidence is 4/100,000
• 3rd decade of life
• 35% incidence in First degree relatives (HLA-B27)
• Etiology Unknown
• UC is a disorder of the colorectal mucosa

Drexel University College of Medicine
Ulcerative Colitis

Drexel University College of Medicine
Disease Distribution
Proctitis/proctosigmoiditis: 44-49%
Left-sided colitis: 36-41%
Pan-colitis: 14-37%
Hendriksen 1985, Farmer 1993, Langholz 1994, Langholz 1996
Drexel University College of Medicine
Disease Severity
Mild colitis: 20%
Moderate colitis: 71%
Severe colitis: 9%
Langholz 1991
Drexel University College of Medicine
Disease Course
Proctitis:• 50% pan-colitis; 12% colectomy
Left-sided colitis:• 9% pan-colitis; 23% colectomy
Pan-colitis:• 40% colectomy
Langholz 1996

Drexel University College of Medicine
Medications
Routes of delivery• Topical• Oral• Intravenous

Drexel University College of Medicine
Medications
5-ASA compounds
Corticosteroids
Immune-modulating agents

Drexel University College of Medicine
Immune-Modulating Agents
Azathioprine and 6-MP
Cyclosporine

Drexel University College of Medicine
Mild - Moderate Disease
Distal colitis• 5-ASA compounds (topical or oral)• Corticosteroids (topical)
Extensive colitis• 5-ASA compounds (oral)

Drexel University College of Medicine
Moderate - Severe Disease
Distal colitis• 5-ASA compounds (topical or oral)• Corticosteroids (topical or oral)
Extensive colitis• Corticosteroids (oral)

Drexel University College of Medicine
Severe - Fulminant Disease
Distal or extensive colitis• Corticosteroids (intravenous)• Cyclosporine (intravenous)

Drexel University College of Medicine
Maintenance Therapy
Distal colitis• 5-ASA compounds (topical or oral)• Immune-modulating agents
Extensive colitis• 5-ASA compounds (oral)• Immune-modulating agents

Drexel University College of Medicine
Operative Indications
Acute disease complications• Toxic colitis or megacolon• Perforation• Hemorrhage

Drexel University College of Medicine
Operative Indications
Chronic disease complications• Cancer risk• Obstruction• Growth retardation• Extra-intestinal manifestations

Drexel University College of Medicine
Operative Indications
Failure of medical therapy• Unresponsive disease• Incomplete response• Excessive steroid requirements• Complications due to medications• Noncompliance with medication

Drexel University College of Medicine
Toxic Colitis
Subjective appearance
Objective criteria:• Fever• Tachycardia• Leukocytosis• Hypoalbuminemia

Drexel University College of Medicine
Toxic Megacolon

Drexel University College of Medicine
Toxic Megacolon
Toxic colitis
Objective criteria:
• Colonic diameter greater than 5 cm
• Persistent colonic gas pattern

Drexel University College of Medicine
Toxic Colitis and Megacolon
Operative technique• Identify and quarantine perforations• Decompress colon• Minimize handling of bowel• Maintain named vessels• Resect omentum• Plan for definitive resection

Drexel University College of Medicine
Cancer Risk
Risk after 10 years• 0.5-1.0% per year
Uncertain affect on risk• Age of disease onset
Increased risk• Disease duration• Extent of disease
No affect on risk• Severity of disease
Drexel University College of Medicine
Dysplasia
Dysplasia associated lesion or mass (DALM)• 40-60% concomitant cancer
High-grade dysplasia• 30-43% concomitant cancer
Low-grade dysplasia• 10-19% concomitant cancer

Drexel University College of Medicine
Emergent Operative Options
• Blow-hole colostomy and loop ileostomy• Subtotal colectomy (STC) and end ileostomy• Total proctocolectomy (TPC) and end ileostomy

Drexel University College of Medicine
STC and Ileostomy
Contraindications• Rectal hemorrhage or perforation• Micro-perforation• Co-morbidity• Pregnancy

Drexel University College of Medicine
TPC and Ileostomy
Indications• Rectal hemorrhage or perforation
Contraindictations• Micro-perforation• Co-morbidity

Drexel University College of Medicine
Elective Operative Options
• Subtotal colectomy (STC) or total abdominal colectomy (TAC) and end ileostomy
• Total proctocolectomy (TPC) and end ileostomy• Total proctocolectomy and ileal pouch-anal
anastomosis (IPAA)

Drexel University College of Medicine
STC or TAC and End Ileostomy
Indications• Significant co-morbidity• Obesity• Immune-modulating agents• High-dose prednisone (>20 mg/day)• Severe hypoalbuminemia• Severe anemia

Drexel University College of Medicine
STC or TAC and End Ileostomy
Drexel University College of Medicine
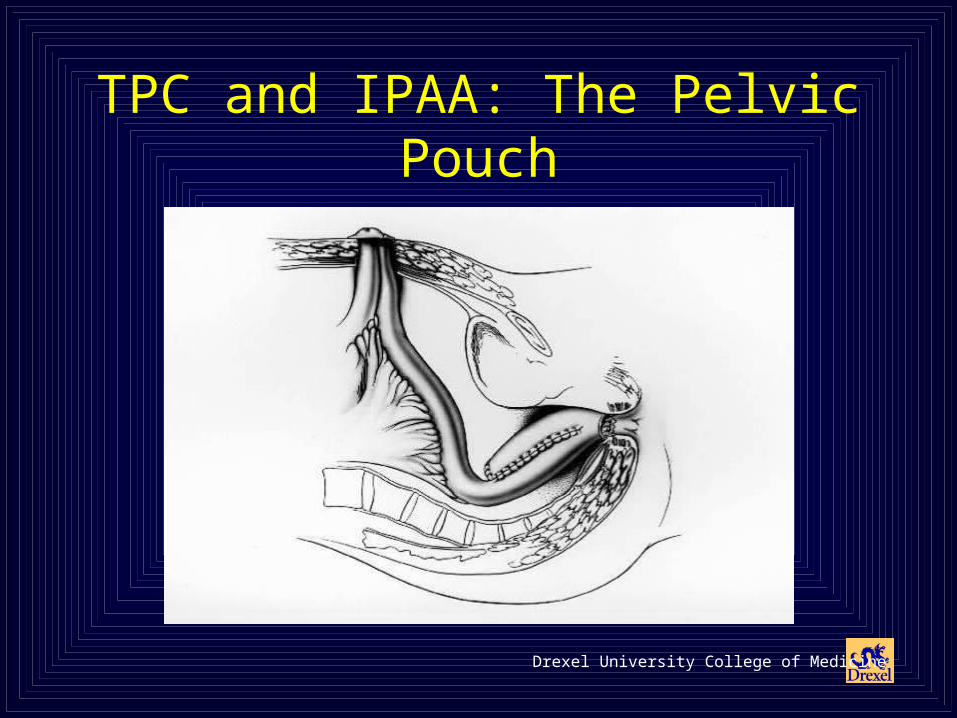
TPC and IPAA: The Pelvic Pouch

Drexel University College of Medicine
TPC and IPAA: The Pelvic Pouch
Drexel University College of Medicine
TPC and IPAA
Contraindications• Significant co-morbidity• Obesity• Marginal or poor sphincter strength• Stage II-IV upper or middle rectal cancer• Stage I-III low rectal cancer• Stage IV colon cancer
Drexel University College of Medicine
TPC and IPAA
Early complications• Small bowel obstruction: 13%• Pelvic sepsis: 5%• Wound infection: 3%• Sexual dysfunction: 2%
Pemberton 1991, Fazio 1995

Drexel University College of Medicine
TPC and IPAA
Late complications• Small bowel obstruction: 9%• Anastomotic leak: 2%• Anastomotic stricture: 5%• Pouchitis: 31%
Pemberton 1991, Fazio 1995

Drexel University College of Medicine
TPC and IPAA
Functional outcome• Frequency: 5-7 stools/day• Nocturnal seepage: 20-30%• Medication: 30%• Pouch loss: 9% (10 years)
Meagher 1998

Drexel University College of Medicine
TPC and IPAA
Quality of Life• SF 36: Comparable to general population• HRQOL: Comparable to patients in remission
with mild disease• HRQOL: Comparable to general population
Fazio 1998, Martin 1998, Thirlby 1998
Drexel University College of Medicine
Conclusions
The treatment of ulcerative colitis focuses on eradication of disease while minimizing morbidity and maintaining intestinal continuity through the combined efforts of gastroenterologists and surgeons.
The operative treatment of ulcerative colitis is based upon clinical presentation, sphincter function, and patient motivation.

Drexel University College of Medicine
Surgery for Inflammatory Bowel Disease
David E. Stein, M.D.Division of Colorectal Surgery
Department of SurgeryDrexel University College of Medicine





























