Embed Size (px)
Citation preview

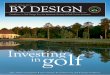
W H A T I S A M E D I C A L G O L F E V A L U A T I O N ?= Video Swing Analysis + Functional Movement Physical + Corrective Strategies
Video Swing Analysis: Identify swing faults and correlate with performance and/or health ramifications
1. S-Posture: can be caused by the player creating too much arch in their lower back by sticking their tail bone out too much in the setup position. This excessive curvature in the lower back or S-Posture puts abnormally high stress on the lower back and causes the abdominal muscles to relax. This deactivation of the core muscles can cause a loss of posture or reverse spine angle during the backswing. This in turn puts the lower body out of position on the downswing and will affect the sequence of motion in the golf swing.
2. C-Posture: occurs when the shoulders are slumped forward at address and there is a definitive roundness to the back from the tailbone to the back of the neck. If the player fails to keep the backswing short and wide he will find it difficult to maintain posture as he swings the club back. The majority of C-Postures are caused by a series of muscle imbalances and joint restrictions that are developed over many years.
3. Loss of Posture: any significant alteration from the body’s original set up angles during the golf swing. Loss of posture can affect all aspects of the swing namely timing, balance, and rhythm. Losing spine angle or altering posture usually causes two typical mishits, the block the right and a hook to the left. As the body angles change, the player is put in a position to have to rely on their hand action to square the face. This becomes a timing-driven swing that can be inconsistent.
4. Flat Shoulder Plane: the angle of the shoulders at the top of the backswing. At address, the spine is tilted due to the forward bend of the hips to allow the correct setup position. In the ideal swing the shoulders would move perpendicular to the tilt of the spine on the backswing A flat shoulder plane is when the shoulders turn on a more horizontal plane than the axis of the original spine angle. The flat shoulder plane can cause the club to be out of position on the backswing that creates a shift in swing planes and a change in the original spine angles on the downswing which reduces the efficiency of the motion. As a result, the player will usually make compensations on the downswing with the body or hands to square the club face. This can also cause a loss of power in the swing as well as inconsistent ball striking.
5. Early Extension: occurs when the hips and spine of a golfer start to go into extension or straighten up too early on the downswing. This can be seen when the hips and pelvis move closer to the ball on the downswing. Early extension causes the upper body to lift up, allowing the golfer to maintain their balance. The lower body does not easily rotate through impact, instead it pushes forward and the person stands up. Players will often complain of being stuck or trapped with their arms on the downswing. This is because the lower body has moved into the space where the arms need to go. The result can be a block or hook as the hands and arms desperately try to deliver the club to the ball. Because of Early Extension if golfers don’t do anything with their hands through impact they may actually shank some shots because they are closer to the ball than they were at address.
6. Over-the-Top: perhaps the most common swing characteristic among high handicap golfers. It usually occurs because of overuse or over-dominance of the upper body during the downswing. As a result the club is thrown outside of the intended swing plane, with the club head approaching the ball in an out-to-in motion. This creates a pull if the clubface is square or a slice if the clubface is open. Over-the-Top can rob a golfer of power and limit their ability to control the ball flight as he adds or decreases loft to the club and additional spin to the ball though impact. By changing the swing plane or swing path, he will create a more solid strike and increase their distance and accuracy.
M e d i c a l G o l f E v a l u a t i o n
D r . S c o t t M . Wacker PT, DPT, OCS, CSCS, CGFI i s a C o l o r a d o n a t i v e a n d r e c e i v e d h i s D o c t o r o f P h y s i c a l T h e r a py d e g r e e f ro m R e g i s U n i v e r s i t y i n 2 0 0 4 . H i s c r e d e n t i a l s p u t h i m i n t h e t o p 1 % o f l i c e n s e d p hy s i c a l t h e r a p i s t s i n t h e c o u n t r y. F o r t h e l a s t d e c a d e , h e h a s s p e c i a l i z e d i n o u t p a t i e n t c a r e o f r e c r e a t i o n a l , c o l l e g e , a n d p ro f e s s i o n a l a t h l e t e s i n t h e m o u n t a i n s o f C o l o r a d o . S c o t t fi r s t i n t ro d u c e d t h e Va i l Va l l e y t o t h e s p e c i a l i z e d t e c h n i q u e o f Tr i g g e r Po i n t D r y N e e d l i n g ( T D N ) n e a r l y f o u r y e a r s a g o a n d n o w t e a c h e s t h e t e c h n i q u e b o t h l o c a l l y a n d i n t e r n a t i o n a l l y. P r e v i o u s t o t e a c h i n g T D N w i t h K i n e t a c o r e , S c o t t w a s a n a f fi l i a t e f a c u l t y m e m b e r a t R e g i s U n i v e r s i t y w h e r e h e i n s t r u c t e d g r a d u a t e l e v e l s t u d e n t s . H e i s a C e r t i fi e d S t r e n g t h a n d C o n d i t i o n i n g S p e c i a l i s t ( C S C S ) a n d i s b o a r d - c e r t i fi e d C l i n i c a l S p e c i a l i s t i n O r t h o p e d i c P h y s i c a l T h e r a p y ( O C S ) . H e r e c e n t l y b e c a m e t h e fi r s t a n d o n l y p hy s i c a l t h e r a p i s t i n t h e Va i l Va l l e y c e r t i fi e d a n d w i t h a d v a n c e d -l e v e l t r a i n i n g i n t h e F u n c t i o n a l M o v e m e n t S c r e e n a n d t h e S e l e c t i v e F u n c t i o n a l M o v e m e n t A s s e s s m e n t - -s y s t e m s c u r r e n t l y u s e d i n t h e N a t i o n a l F o o t b a l l L e a g u e a n d o t h e r p ro f e s s i o n a l s p o r t s . H e i s a l s o t h e o n l y t h e r a p i s t i n t h e Va l l e y t h a t i s a T i t l e i s t P e r f o r m a n c e I n s t i t u t e C e r t i fi e d G o l f F i t n e s s I n s t r u c t o r ( C G F I ) .

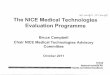
W H A T I S A M E D I C A L G O L F E V A L U A T I O N ?= Video Swing Analysis + Functional Movement Physical + Corrective Strategies
Video Swing Analysis: Identify swing faults and correlate with performance and/or health ramifications
7. Sway: any excessive lower body lateral movement away from the target during the backswing that forces the weight to the outside of the back foot. This swing characteristic makes it very difficult to develop a proper weight shift during transition and the downswing. Imagine a baseball batter digging in at the plate with their back foot. This simple routine allows them to load around their back leg and drive their weight from their back let to their front leg in a very efficient manner. If there is no stable platform to drive their weight off of during transition, golfers will lose power and inadvertently to develop speed in an inefficient sequence.
8. Slide: any excessive lower body lateral movement toward the target during the downswing. This swing characteristic makes it very difficult to stabilize your lower body during the downswing, which will eventually rob power and speed from the upper body through impact. The upper body needs a stable lower body to insure acceleration during the downswing. Once the lower body starts its forward shift into the downswing, it should transfer energy to the upper body and provide a stable base for the extreme rotary forces created by the torso, arms, and club. If there is no stable platform, players will lose power and try to develop speed in an inefficient sequence.
9. Reverse Spine Angle: excessive upper body backward bend or excessive left lateral upper body bend during the backswing. This makes it difficult to start the downswing in the proper sequence, because the lower body is in a position that usually limits its ability to initiate the downswing. This swing characteristic is also one of the prime causes of lower back pain. The upper body tends to dominate the swing when the lower body can’t start the downswing or has a limited ability to initiate the movement. The upper body domination will eventually create path problems and limited power output. This swing characteristic also puts excessive tension on the lower back due to forced inhibition of the abdominal musculature during the backswing.
10. Hanging Back: when a golfer does not shift their weight correctly back onto the lead side on the downswing. golfers tend to hang back on their trailing leg and spine through impact. This usually results in a lack of power and the inability to create a consistent strike on the golf ball. Hanging back can also be caused by other swing characteristics such as a reverse pivot or sway. Hanging back will usually result in premature release of the wrist angles as the player is trying to advance the club with their arms rather than with the correct weight shift and pivot.
11. Casting, Early Release and Scooping: refers to any premature release of the wrist angles during the downswing and though impact. The angle loss results in a weakened impact position with the lead wrist being cupped at ball strike. The angle loss adds lost to the face of the club and as a result we see a loss of power and consistency. It is termed “casting” or “early release” when the club head and left forearm are in a straight line prior to making contact with the ball. The term is “scooping” when the club head passes the hands through impact and the student is trying to lift the ball into the air. We should see the shaft leaning slightly toward the target (hands leading the club head). At impact this helps to compress the golf ball and creates a more powerful impact position.
12. Chicken Winging: a loss of extension or breakdown of the lead elbow through the impact area. This swing characteristic makes it difficult to develop speed or power and tends to put excessive force on the outside of the elbow joint. If the golfers suffering from high weak shots or they tend to develop tennis elbow on the lead side, they probably have a chicken wing.
M e d i c a l G o l f E v a l u a t i o n
D r . S c o t t M . Wacker PT, DPT, OCS, CSCS, CGFI i s a C o l o r a d o n a t i v e a n d r e c e i v e d h i s D o c t o r o f P h y s i c a l T h e r a py d e g r e e f ro m R e g i s U n i v e r s i t y i n 2 0 0 4 . H i s c r e d e n t i a l s p u t h i m i n t h e t o p 1 % o f l i c e n s e d p hy s i c a l t h e r a p i s t s i n t h e c o u n t r y. F o r t h e l a s t d e c a d e , h e h a s s p e c i a l i z e d i n o u t p a t i e n t c a r e o f r e c r e a t i o n a l , c o l l e g e , a n d p ro f e s s i o n a l a t h l e t e s i n t h e m o u n t a i n s o f C o l o r a d o . S c o t t fi r s t i n t ro d u c e d t h e Va i l Va l l e y t o t h e s p e c i a l i z e d t e c h n i q u e o f Tr i g g e r Po i n t D r y N e e d l i n g ( T D N ) n e a r l y f o u r y e a r s a g o a n d n o w t e a c h e s t h e t e c h n i q u e b o t h l o c a l l y a n d i n t e r n a t i o n a l l y. P r e v i o u s t o t e a c h i n g T D N w i t h K i n e t a c o r e , S c o t t w a s a n a f fi l i a t e f a c u l t y m e m b e r a t R e g i s U n i v e r s i t y w h e r e h e i n s t r u c t e d g r a d u a t e l e v e l s t u d e n t s . H e i s a C e r t i fi e d S t r e n g t h a n d C o n d i t i o n i n g S p e c i a l i s t ( C S C S ) a n d i s b o a r d - c e r t i fi e d C l i n i c a l S p e c i a l i s t i n O r t h o p e d i c P h y s i c a l T h e r a p y ( O C S ) . H e r e c e n t l y b e c a m e t h e fi r s t a n d o n l y p hy s i c a l t h e r a p i s t i n t h e Va i l Va l l e y c e r t i fi e d a n d w i t h a d v a n c e d -l e v e l t r a i n i n g i n t h e F u n c t i o n a l M o v e m e n t S c r e e n a n d t h e S e l e c t i v e F u n c t i o n a l M o v e m e n t A s s e s s m e n t - -s y s t e m s c u r r e n t l y u s e d i n t h e N a t i o n a l F o o t b a l l L e a g u e a n d o t h e r p ro f e s s i o n a l s p o r t s . H e i s a l s o t h e o n l y t h e r a p i s t i n t h e Va l l e y t h a t i s a T i t l e i s t P e r f o r m a n c e I n s t i t u t e C e r t i fi e d G o l f F i t n e s s I n s t r u c t o r ( C G F I ) .