Embed Size (px)
Citation preview

17-Oct-191
Dr Sadik AL-Ghazawi
MRCP FRCP UK

17-Oct-192

17-Oct-193
Movement Disorder
The control of voluntary movement is affected by
the interaction of the pyramidal , cereballar &
extrapyramidal systems interconnecting with
each other as well as projecting to anterior
horn region or cranial nerve motor nuclei.
.

17-Oct-194
The extrapyramidal system consists of
paired subcortical masses or nuclei of gray matter,
the basal ganglia which consist of, caudate,
butamen, globus pallidus , subthalamic nuclei, and
substantia nigra.
The caudate nucleus & butamen are collectively
referred to as the (striatum)

17-Oct-195

17-Oct-196
Acetylcholine :
Synthesis by small striatal cells.
Greatest information in striatum.
Excitatory effect
Dopamine:
Synthesis by cell substantia nigra and nigral
projection in striatum .
Greatest concentration in substantia nigra
Inhibiting effects.
Note: these two transmitters normally are "in
balance" .
Imbalance –ACH depletion or dopamine excess
results in the movement disorder, chorea.
Dopamine depletion –results in the movement
disorder of Parkinsonism.

17-Oct-197
Gamma aminobutyric acid ( GABA)
synthesis in the striatum & globus pallidus.
It has inhibitory action
Deficiency is associated with
Huntington's chorea.
.

17-Oct-198
Negative features
1- Bradykinesia: a loss or slowness of voluntary
movement, this result in :
• reduced facial expression (mask- like).
• Reduced blinking
• Reduced adjustment of posture when seated
• When agitated , the patient will move swiftly- "
kineasia paradoxical".
.

17-Oct-199
2- Postural disturbance:
Flexion of limbs and trunk is associated with Failure
to make quick postural or " righting" adjustment to
correct balance, patient falls whilst turning or if
pushed

17-Oct-1910
Positive features:
1- Involuntary movement
Tremor
Chorea ( irregular , repetitive, jerky
movement)
Athetosis (irregular , repetitive, writhing
movement).

17-Oct-1911
Dystonia ( slow, sustained abnormal movement).
Ballismus ( explosive, violent movement)
Choreaothetosis : chorea & athetosis may merge
into one another.

17-Oct-1912
2- Rigidity:
stiffness felt by the examiner when passively
moving a limb.
This "resistance is present with the same
degree through out the full range of
movement.
affecting flexor & extensor muscle groups
equally, & is described as lead pipe rigidity.

17-Oct-1913
when tremor is super imposed upon rigidity it
produces " cogwheel" rigidity.
Note: In Parkinson's Disease both positive
features e.g. tremor, & negative features e.g.
bradykinesia occur.
Note: In Huntington's chorea positive features
,e.g. chorea, predominate.

17-Oct-1914
Parkinson's disease:
❖Described by James Parkinson( 1817) in " An
assay on the shaking palsy".
❖ Recognized as an extrapyramidal disorder by
Kenner Wilson 1912.
❖ Annual incidence: 20/ 100000.

17-Oct-1915
❖Prevalence 190/100000
❖ Sex incidence : M:F -3:2
❖ Age of onset : 50 years upward.
❖ Incidence peak in mid – 70s then decline.
❖ Familial incidence occur in 5%.

17-Oct-1916

17-Oct-1917

17-Oct-1918
Risk Factors:
Family history of PD
Head trauma (Concussion)
Exposure to chemicals and pesticides

17-Oct-1919
Features of Parkinson's Disease occur in many
disorders ( Akinetic Rigid syndromes) :
Idiopathic Parkinson's Disease
Secondary Parkinsonism :
a-Drug induced ,e.g. haloperidol
b-Post encephalopathic
c- toxic e.g. CO
d- toxic (endogenous) e.g. Wilson's
Disease

17-Oct-1920
Multiple system atrophy (MSA).
Progressive supraneuclear palsy
Corticobasal degeneration
Diffuse Lewy’s bodies disease
Alzheimer's disease

17-Oct-1921

17-Oct-1922
Pathology of idiopathic Parkinson's Disease:
The substantia nigra contains pigmented cells
( neuromelanin) which gives it a characteristics
black appearance.
These cells are lost in Parkinson's Disease& the
substantia nigra become pale.

17-Oct-1923
Remaining cells contain esonophilic inclusions in
the cytoplasm –Lewy’s bodies- although these are
not specific to Parkinson's Disease .
Lewy's bodies may be found in the cerebral cortex
especially when dementia is present (diffuse Lewy’s
body disease).
Minor changes are seen in other basal nuclei-
striatum & globus pallidus.

17-Oct-1924
Clinical features:
Initial symptoms are vague, the patient often\
complains of aches & pain .
1- coarse tremor:
➢ Coarse at a rate 4/ second , usually develops
early in the disease.
➢It begins unilaterally in the upper limbs &
eventually spread to all 4 limbs.

17-Oct-1925
➢The tremor is often " pill-rolling”, the thumb
➢moving rhythmically back & forward on the
palm.
➢It occurs at rest , improve with movement &
➢ disappears during sleep.

17-Oct-1926
2- Rigidity:
oPredominant in flexor muscles of the neck,
trunk, & limbs.
oResults in the typical " flexed posture".

17-Oct-1927
3- Bradykinesia :
Slowness or paucity of movement affects
facial muscles of expression ( mask- like
appearance) as well as muscles of
mastication, speech, voluntary swallowing &
muscles of the trunk & limbs.
Dysartheria , dysphagia & slow deliprate gait
with little associated movement ( arm
swinging).
17-Oct-1928
Notes:
Tremor, rigidity & bradykinesia deteriorate
simultaneously, affecting every aspect of the
patient's life :
hand writing reduced in size (micrographia),
the gait become shuffling & festinant (small,
rapid steps to " keep up with" with the center of
gravity) and the posture more flexed.

17-Oct-1929
Rising from a chair becomes laborious with
progressive difficulty in initiating lower limb
movement from a stationary position .
Eye movement may be affected with loss of
ocular convergence & upward gaze.
Excessive sweating & greasy skin (seborrhea )
can be trouble some.

17-Oct-1930
Depression, drug- induced confusional state &
dementia occur in 30% of patients.
Occasionally autonomic features occur –
postural hypotension.
Note: Post-encephalictic Parkinson's disease
( encephalitis lethargica) now rarely encountered, is
characterize by an earlier age of onset & oculogyric
crisis ( acute ocular deviation) .

17-Oct-1931
•Cognitive dysfunction.
•Psychosis.
•Mood disorders (depression, anxiety, apathy/abulia).
•Sleep disturbances.
•Fatigue.
•Autonomic dysfunction (urinary urgency/frequency,
constipation, orthostasis, erectile dysfunction).
•Olfactory dysfunction.
•Pain and sensory disturbances.
•Dermatologic findings (seborrhea).

17-Oct-1932
Features of Parkinson disease
1-Bradykinesia2-Rigidity
3-Resting tremor
4-Postural Instability

17-Oct-1933
Diagnosis:
When tremor, rigidity & bradykinesia
co-exist ,distinguish Parkinson's
disease from secondary Parkinsonism by the
absence of relevant drug history.
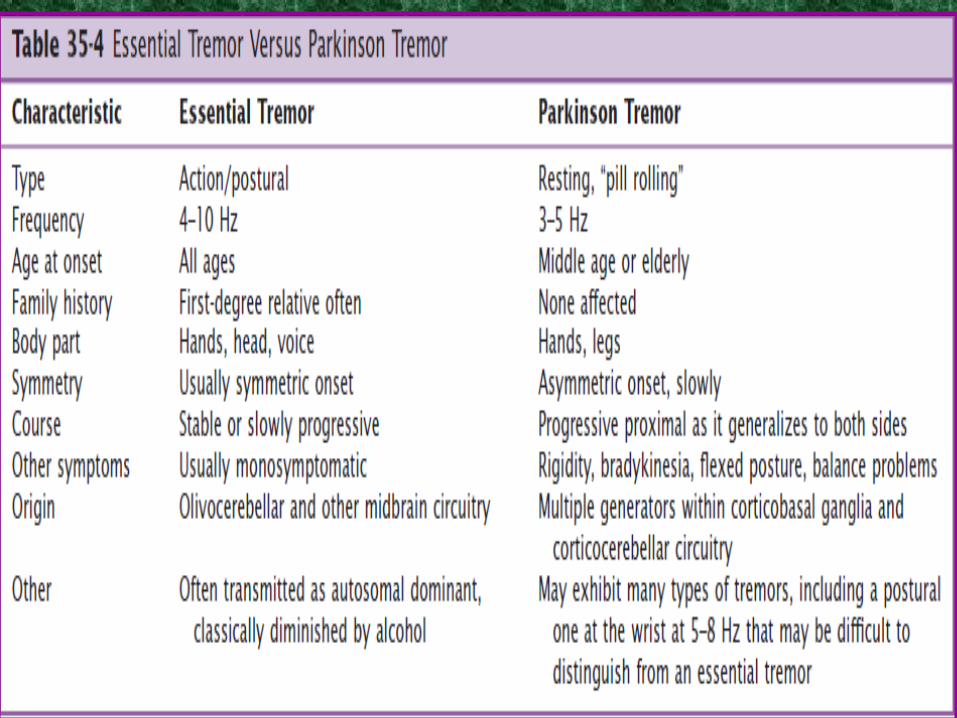
Tremor should be distinguished from :
senile tremor, essential tremor & metabolic
tremor; which are all absent at rest & more
pronounce on voluntary movement.
.

17-Oct-1934

17-Oct-1935
Parkinson disease medical treatment (motor symptoms)
Levodopa
Dopamine Agonists
Monoamine Oxidase B inhibitors (e.g. Selegiline)
Anticholinergic Agents (e.g. Benztropine, Trihexyphenidyl).
Amantidine.
Catechol-O-Methyl transferase inhibitors (COMT) (e.g.
Entacapone).

17-Oct-1936

17-Oct-1937
Levodopa or Dopamine Agonists shouldn’t be stopped
abruptly
Risk of Parkinsonism Hyperpyrexia Syndrome

17-Oct-1938
Exogenous dopa:
-Given as;
1-levodopa or
2- levodopa + decarboxylase inhibitor, which
prevents peripheral brake down of levadopa in
the liver allowing a higher concentration of dopa
to reach the blood-brain barrier; also the
peripheral side effects of levodopa ( nausea,
vomiting, hypotension) are diminished.

17-Oct-1939
Central side effects:
confusion, depression,
dyskinetic movements and following
long- treatment- " on /off" phenomenon.
Controlled –release or long acting preparations
produce constant plasma levels & a more even
clinical response.

17-Oct-1940
Exogenous dopa improve bradykinesia, rigidity,
& to a lesser extent, tremor, but in 20% the
response is poor.
The "good" responders often develop central side
effects later – especially the
" on/off " phenomenon.

17-Oct-1941
Dopamine Agonist:
When levodopa responsiveness is low , dopamine
agonist are used.
-Bromorciptine .

17-Oct-1942
-Apomorphine
given by continuous infusion or intermittent
injection & is affected in shortening periods of
prolong immobility (freezing).
Dopamine agonist may produce postural
hypotension & confusion.

17-Oct-1943
Selegililine:
The enzymes monoxidase (MAO) A & B play a key
role in the break down of Dopamine.
This drug is an MAO –B inhibitor, its usage
results in increased dopamine levels.

17-Oct-1944
Amantidine,
an antiviral drug, may help rigidity, the mode of
action is not known.

17-Oct-1945
Surgical treatent of parkinson disease:
•1-Deep brain stimulation (STN, Gpi).
•2-Ablative surgery: (Thalamotomy, Pallidotomy &
Subthalamotomy).

17-Oct-1946
Advances in drug treatment in recent years have
reduced the need for stereotactic surgery, but in
patients with intractable tremor this is still of
benefit, a steriostactic lesion is made in the
globus pallidus or ventrolateral nucleus of the
thalamus ( contralateral to the tremor).
17-Oct-1947
Essential tremor
•1-Worsens with age and may eventually significantly interfere with
normal activities.
•4-10 Hz
•2-50% AD, LINGO1 gene.
•3-Mild parkinsonian features (i.e., rest tremor, cog wheeling, and
breakdown in rapid alternating movements) may also be present.
•Improves with alcohol intake.

17-Oct-1948
17-Oct-1949

17-Oct-1950
Physiologic tremor
▪1-Normally present in healthy individuals.
▪8-12 Hz
▪2-Factors Enhanced physiological tremor:
▪
Stress, fatigue, emotions, hypoglycemia, hypothermia, thyrotoxicosis,
▪
pheochromocytoma, drug withdrawal, and alcohol intoxication and Beta
receptor agonists.

17-Oct-1951
Chorea

17-Oct-1952
➢Rapid unpredictable nonrhythmic
involuntary contractions affecting mostly distal limbs, trunk,
neck and face which rapidly flip from region to region in an
irregular pattern.
➢DD ,Athetosis and ballism are sometimes confused with
chorea.

17-Oct-1953
Ballismus:
✓Movement of the proximal limb muscles with
a larger amplitudes and more rotatory or flinging
quality than chorea.
✓Hemiballismus
Athetosis:
✓Slow flowing writhing involuntary movement

17-Oct-1954
Pathophysiology Of Chorea
✓Loss of inhibition in the indirect pathway>> excessive
dopaminergic activity.
✓Putamen, Globus pallidus and subthalamic nuclei and
caudate in Huntington disease.
17-Oct-1955
Chorea:
❑Uninvoluntary, irregular, jerking movement
❑affecting limb & axial muscle groups.
❑These movements are suppressed with
difficulty and are incorporated into voluntary
gestures resulting in a "semi purposeful“
appearance e.g. crossing & uncrossing of legs.

17-Oct-1956

17-Oct-1957
Causes :
❖ Hereditary)(Huntington's disease), benign chorea.
❖
❖ Drugs: Antiparkinsonian drugs, oral
❖contraceptive.
❖ Toxins: alcohol, CO poisoning.
❖ Infections: Sydenham's chorea, encephalitis.
❖ Metabolic: hyperthyroidism, hypocalcemia.
❖ Immunological: SLE, PAN
❖ Miscellaneous: Chorea gravidarum, polycythemia
rubra vera .

17-Oct-1958
Treatment
•Monoamine inhibitors: (depletes dopamine)Tetrabenazine, Reserpine
•Antipsychotics : (dopamine receptor antagonists)Haloperidol, risperidone
•Anticonvulsants:Clonazepam, valproic acid (chorea?)

17-Oct-1959
Huntington's disease :
Autosomal disorder
Onset in middle life & progression to death within
10-12 yrs .
It may occur in young person (juvenile) ; here
chorea less apparent & negative symptoms
( rigidity) predominate.

17-Oct-1960
Pathology:
Neuronal loss in the striatum is associated with
reduction in projections to other basal ganglia
structure.
.The neurochemical basis of this disorder
involves deficiency off GABA & Ach

17-Oct-1961
Clinical features:
1-Chorea:
- may be the initial symptom.
gross involuntary movements which
interrupt involuntary movement & make feeding
& walking impossible.
2- Dementia

17-Oct-1962

17-Oct-1963
3- Behavioral disturbance:
1- Personality change.
2- Affective disorder & psychosis occurs.
4- Hypotonicity often accompanies choreiform
movement.
5- Primitive reflexes : grasp,
6- Eye movements are disturbed with impersistence
of gaze.
17-Oct-1964
Diagnosis:
On clinical ground
• Family history ( although true
• parents may be unknown or
•knowledge of illness suppressed.
• Distinguish from benign hereditary chorea in
which intellect is preserved.

17-Oct-1965
• Exclude senile chorea by older age of onset &
absence of dementia .
• CT scan may demonstrate atrophy of the
caudate nucleus.
MRI shows an increased in the T2 signal in the
caudate nucleus.
17-Oct-1966
Treatment :
Phenothiazine, haloperidol, or tetrabenazine may
control the movements in the preliminary stages.

17-Oct-1967
Sydenham's chorea
•Group A beta hemolytic streptococcus
•Age (5-15 years)
•Rheumatic fever
•Few weeks after onset.
•Associated with psychiatric symptoms.
•Self limited.
•Recurrence (20%)

17-Oct-1968
Sydenham's chorea:
Acute onset.
Associated with streptococcal infection.
Remits in weeks.
Necrotizing arteritis in thalamus, caudate
nucleus & potamin.
Diagnosis is confirmed by elevated ESR &
antistreptolycine ( ASL) titer.

17-Oct-1969
Treatment:
sedation, phenothiazines.
The condition may become recurrent – during
pregnancy, intercurrent infection.

17-Oct-1970
Chorea Gravidarum:
❖Acute onset in pregnancy, usually the first
trimester.
❖Restricted to face or generalized.
❖Perhaps caused by reactivation of
Sydenham's chorea.
❖Pathology unknown.
❖Treatment: Haloperidol.

17-Oct-1971
Benign chorea:
Dominant inheritance with incomplete
penetration.
Onset in childhood.
The movements are mild, occasionally
aggravated by physical exercise .
Rarely progressive.

17-Oct-1972
Dystonia
17-Oct-1973
DYSTONIA
Sustained contraction of agonist and antagonist muscles,
leading to abnormal postures with repetitive twisting
movements.
• Focal
Blephrospasm
Cervical dystonia
• Segmental
• Generalized
• Multifocal

17-Oct-1974
Cervical dystonia• The most common focal dystonia.• Manifests with involuntary head posture, neck pain and a tremor
Task-specific dystonia• Only with specific activities• The most common task-specific dystonia is writer’s cramp

17-Oct-1975
✓Treatment ✓
Botulinum injection (focal)✓Anticholinergics ✓Dopamine-depleting ( Tetrabenazine)✓Muscle relaxants (GABA agonists)✓Levodopa✓Surgical (DBS of the Gpi)

17-Oct-1976
Spasmodic torticollis ( Wry neck):
Unilateral deviation of the head .
Etiology is unknown.
Dystonic contraction of the left
sternomastoid produces head turning to the
right.

17-Oct-1977
Treatment:
Anticholenergic & phenothiazines produce
some benefit in 50% of patients.
Injection off botulinum toxin into the
sternomastoid muscle gives variable
systematic relieve so requires regular
repetition.

17-Oct-1978
Writer's Cramp:
❖Variable age of onset.
❖Muscles of the hand & forearm tighten on
attempting to right and pain may occur in the
forearm muscles.
❖Previously regarded as an " occupational
neurosis" but now is classified as a partial
dystonia.
❖May be precursor of Parkinson's Disease.

17-Oct-1979
Treatment :
❖Benzodiazipine & anticholenrgic are of limited
value.

17-Oct-1980
Drug induced dystonia:
❖Acute adoption of abnormal dystonic posture
❖ – usually head & neck or oculogyric crisis
( upward deviation of eyes)- caused by
phenothiazine & metaclopramide.
❖Treatment
Anticholenergic, benztropine -24-48 hrs help
symptom settle.

17-Oct-1981
Progressive supranuclear palsy:
A condition characterize by gaze palsy,
extrapyramidal features, axial dystonia (
truncal) .
Progressive psudobulbar palsy.
Onset in the 5th – 6th decade.
Etiology unknown.

17-Oct-1982
Down eye movement is initially impaired
followed by all other voluntary eye movement,
lid retraction is common.
Psudobulbar signs develop.
The head then hyperextend & rigidity ensues in
the limbs.

17-Oct-1983
Treatment:
Levodopa & anticholenergics give disappointing
results.
The coarse is relentless with progression & death
in 2-5 yrs.

17-Oct-1984
Hemiballismus:
Unilateral, violent, flinging of the limbs.
Occusionally severe enough to throw the patient
of balance or even from his bed.
Lesion of subthalamic nuclei .

17-Oct-1985
It usually results from vascular disease
( posterior cerebral artery).
Occasionally occur in MS.
Drug treatment is ineffective.
The condition often settled spontaneously.

17-Oct-1986
Athetosis:
Present in childhood
Slow writhing movement, the rate of movement
between chorea or dystonia.
Involve the digits , hands & face on each side.
Associated with hypoxic neonatal brain
damage, kirnicterus, lipid storage disease.
Response to anticholenergic is variable &
occasionally dramatic.

17-Oct-1987
Tradive Dyskinesia(TDs)
are involuntary movements of the tongue, lips, face, trunk, and extremities that occur in patients treated with long-term dopaminergic antagonist medications
• May occur during therapy with dopamine-receptorantagonists or even years after the medication is
discontinued

17-Oct-1988
• Oro-bucco-lingual movements ,restlessness), dystonia , tremor, parkinsonism, orcombination of these
Treatment:
Discontinue neuroleptic. If not possible, continue on
lowest possible dose.

17-Oct-1989
Tics
17-Oct-1990
Sudden, relatively quick, stereotyped movements (motor tics) or sounds (phonic tics) which are repeated at irregular intervals.

17-Oct-1991

17-Oct-1992
Wilson's Disease:
Autosomal recessive disorder of copper metabolism.
Neuronal loss within potamine & globus pallidus .
Copper accumulate in descemet membrane in the
eyes, nail bed, liver & kidney.
Deficiency of alpha 2 globuline – ceruloplasim – which
normally binds 98% of copper in the plasma.
Increased in loosely bound copper- albumine &
deposition occur in all organs.
Urinary copper is increased.

17-Oct-1993
Clinical features:
Two clinical forms:
•Acute (Children): characterized by ,
•bradykinesia, behavioral changes,
•
involuntary movement, liver involvement is
common,
•untreated , death in 2 yrs from hepatic & renal
failure.

17-Oct-1994
•Chronic ( young adult): marked proximal
tremor, dysartheria, dystonia,
•rigidity, choreoathetosis, psychosis,
•
behavioral disorders, dementia,
•
liver involvement less severe,
• untreated , death in 10 yrs.

17-Oct-1995

17-Oct-1996
Diagnosis:
Slitlamp (Kayser-Fleischer ring).
Low Ceruloplasmine < 20mg/dl.
Elevated unbound serum copper.
High urinary copper excretion.
Liver biopsy & copper metabolism test with
radioactive CU 64.
MRI

17-Oct-1997
In families, biochemical test identify low
ceruloplasmine in carriers and presymptomatic
patients.

17-Oct-1998
Treatment:
Low copper diet ,
pencillamine 1gm daily.
Treatment for the patient life, adequate treatment
is compatible with normal life.

17-Oct-1999
Clinical presentation:
- Childhood.
- Motor before vocal tics.
- (85%) experience reduction in tics during and after
adolescence.
- Psychiatric manifestations:
Depression and mood disorders.
Tourette’s syndrome

17-Oct-19100
Myoclonus
➢sudden, brief and shock-like involuntary
movements.
➢Types:
Physiologic: , Anxiety, Hiccups
Epileptic.
Symptomatic.
➢Treatment
Clonazepam, Sodium valproate, Levetricetam.

17-Oct-19101
Dr Sadik Sharief
MRCP, FRCP Edinburgh
Lecture





![arXiv:1710.00317v1 [q-bio.PE] 1 Oct 20171 arXiv:1710.00317v1 [q-bio.PE] 1 Oct 2017 2 is not considered particularly relevant in malarial disease studies given the rela-tively low mortality](https://img.dokumen.tips/doc/110x75/604651c63779285f9f300e34/arxiv171000317v1-q-biope-1-oct-2017-1-arxiv171000317v1-q-biope-1-oct-2017.jpg)























