Embed Size (px)
Citation preview

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 1/77
Dr S Raju

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 2/77
Asthma is a common disorder◦ It can happen to anybody◦ It is not contagious◦
It produces recurrent attacks of coughwith or without wheeze
◦ It can be effectively treated◦ Between attacks people with asthma
lead normal lives as anyone else◦ In most cases there is some history of
allergy in the family

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 3/77
Most patients with asthma aretreated by primary carephysicians (>60%).
Some asthmatics havemanagement problems that
should be referred to a specialistin asthma.

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 4/77
15 – 20 million asthmatics in India In Delhi prevalence estimated at 12% in
children
Significant cause of school/ workabsence
Increasing morbidity and mortality

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 5/77
More than one of the symptoms e:g : wheeze,cough, difficulty breathing, chest tightnessespecially if ◦ Frequent and recurrent◦ Worse at night and early morning
◦ Occur in response to, or worse after Exercise or other trigger – eg exposure to pets, cold ordamp air, emotions or laughter
◦ Occur apart from colds Personal history of atopic disorder
Family history of atopic disorder and/or asthma Widespread wheeze heard on auscultation History of improvement in symptoms or lung
function in response to adequate therapy

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 6/77
Symptoms with cold only, no interval symptoms Isolated cough in absence of wheeze or
difficulty breathing
History of moist cough Repeatedly normal chest examination whilst
symptomatic Normal PEF or spirometry whilst symptomatic
No response to trial of asthma treatment Clinical features pointing to alternative
diagnosis

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 7/77
Prevention of triggers
Patient education
Pharmacological drugs
PEFR measurement

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 8/77
Minimal (ideally no) chronic symptoms Minimal (infrequent) exacerbations
No emergency visits
Minimal (ideally no) need for "as needed” use of β 2-
agonist No limitations on activities, including exercise
PEF circadian variation of less than 20 percent
(Near) normal PEF/FEV1
Minimal (or no adverse effects from medicine)

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 9/77
"The aim of asthmamanagement should be
control of the disease"

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 10/77

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 11/77
Gain control as quickly as possible; then
decrease treatment to the least medicationnecessary to maintain control. Gainingcontrol may be accomplished by either starting treatment at the step most appropriate to the initial severity of thecondition or starting at a higher level of therapy (e.g., a course of systemiccorticosteroids or higher dose of inhaled corticosteroids) and then stepping down

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 12/77
Review treatment every 1-6 months; agradual stepwise reduction intreatment may be possible.
If control is not maintained, considerstep up.

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 13/77
At each step, patients should control their environment to avoid or control factors
that make their asthma worse (e.g.,allergens, irritants); this requires specificdiagnosis and education.

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 14/77
Step down◦ Review treatment every 1-6 months.
◦ If control is sustained for at least 3 months, agradual stepwise reduction in treatment may be
possible Step up
◦ If control is not achieved, consider step up.
◦ But first, review patient medication technique,adherence and environmental control (avoidance of
allergens or other precipitant factors)

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 15/77
The stepwise approach presents guidelinesto assist clinical decision-making.
Asthma is highly variable; clinicians shouldtailor specific medication plans to the needsand circumstances of individual patients

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 16/77
Asthma management in 2007 is focused on control of the individual patient’s asthma symptoms, aparadigm shift from earlier recommendations of astep-wise increase in therapy based on asthmaseverity;
Patient self-management plans play an important rolein prevention of exacerbations;
Successful asthma interventions lead to increasedmedication costs but decreased costs forhospitalization, and decreased death rates;
Allergen exposure is an important contributory factorin exacerbations of IgE-mediated asthma.

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 17/77
Allergens
Tobacco smokeIndoor pollutants and irritants

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 18/77
Animal dander◦ Remove animal from house / keep animal out of patient’s bedroom
House dust mite◦ Encase mattresses in an allergen-impermeable cover
◦ Wash sheets and blankets in hot water weekly◦ Remove carpets from bedroom / avoid sleeping on upholstered furniture
Cockroaches◦ Poison baits / Do not leave food and garbage exposed
Indoor mould◦ Fix all leaks and eliminate water sources associated with mould growth
◦ Clean moldy surfaces
Pollen◦ Stay indoors esp. in the afternoons◦ Windows closed during the season in which they have problems with outdoor allergens

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 19/77
Stop smoking or smoke outside home (patients andothers at home)
Smoking reduces the response to inhaled steroid Daycare providers / workplace smoke
Reduce wood-burning stoves and fire-places Unvented stoves and heaters Reduce perfumes / cleaning agents / sprays
etc.
8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 20/77
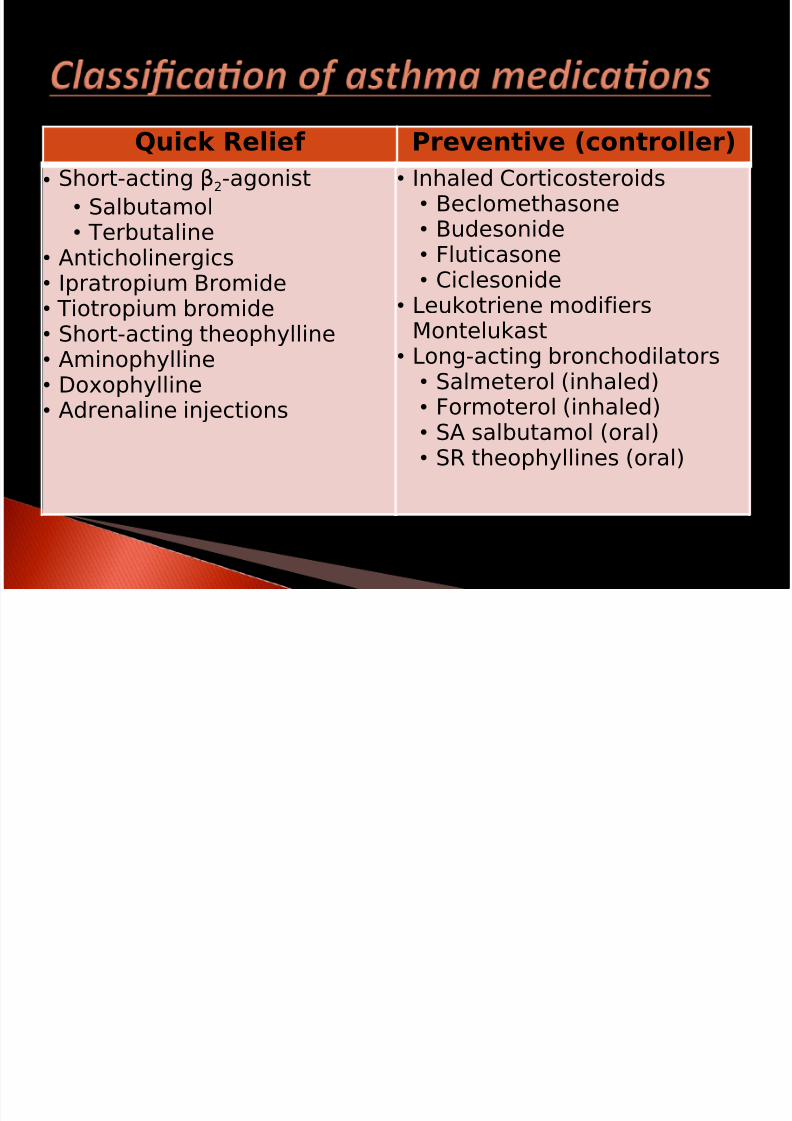
Quick Relief Preventive (controller)• Short-acting β2-agonist
• Salbutamol• Terbutaline
• Anticholinergics• Ipratropium Bromide• Tiotropium bromide• Short-acting theophylline• Aminophylline• Doxophylline•
Adrenaline injections
• Inhaled Corticosteroids• Beclomethasone• Budesonide• Fluticasone
• Ciclesonide• Leukotriene modifiers
Montelukast• Long-acting bronchodilators
• Salmeterol (inhaled)•
Formoterol (inhaled)• SA salbutamol (oral)• SR theophyllines (oral)

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 21/77
GINA Workshop Report,2003

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 22/77
If a patient uses◦ b
2agonists > twice per week in day time,
◦ or awakens > twice per month with nocturnalasthma,
◦ or refills a b2-inhaler > twice in a year, then the patient's asthma is mild
persistent or greater and daily anti-inflammatory therapy is required.

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 23/77
GINA Workshop Report,2003

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 24/77
Inhaled steroid

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 25/77
Inhaled corticosteroids Budesonide/ beclomethasone/
fluticasone/ ciclesonide – use any
Start (400-1000 mcg/day approx. in 2divided doses)
Maintain for 2 to 3 months
Taper slowly Safe for long-term use (years)

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 26/77
Most potent anti-inflammatorymedications for asthma
Prevent decline in lung function
Safer than other equally effectivetreatments
Most cost-effective

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 27/77
Throat infections (gargle/ use spacer)Hoarseness (singers/teachers/ leastwith ciclesonide)
Cataracts?Osteoporosis?

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 28/77
Same dose for at least 3 months Then, gradual stepwise reduction intreatment (25% - 50% every 1 - 3
months)Use peak flow meter – very imp

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 29/77
New EU scale

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 30/77
No symptomsAsymptomatic during exercise andplay
Sleep undisturbedMinimal / no use of ‘relief’medication

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 31/77
~ 400 mcg/day (budesonide) Over 9 years of continuous use No growth retardation Uncontrolled asthma causes growthretardation
Pedersen and Agertoft NEJM 2000;343:1064-69

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 32/77
Non-compliance / non-adherenceHabitual b2-agonist overuseGE refluxSinusitisHyperventilationOthers:
◦ Bronchiectasis /PE◦ OSA /Cardiac disease

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 33/77
first reconfirm diagnosis
Check Inhaler Technique /
Check RegularUse
Add LABA
Formoterol /
Salmeterol
Increase doseof inhaled
steroid
AddLeukotriene
modifier
Add SR Theophylline

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 34/77
First-line add-on therapy at Step 3(BTS)
But over a 4-fold dosage range (200-
800 mcg BDP/BUD)So the dilemma is at what dose toadd the LABA ?

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 35/77
80-90 % of the maximum therapeuticbenefit of ICS is achieved at daily doseof 200mcg FP or 400mcg BUD
200 mcg FP or equivalent shouldbe the preferred dose at which toconsider adding LABA if control is
inadequate Masoli M et al, Thorax 2005;60:730-734

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 36/77
PrednisoloneAcute severe episodesDispense preferablySteroid-dependent asthma (regularneed)

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 37/77
Montelukast 10mg/day (5mg/4mg forchildren)
Oral anti-inflammatory
Not as effective as inhaled steroid First-line option for 2 to 5 yr. olds in
mild persistent asthma
All your ‘regular’ bronchodilator users

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 38/77
As an add-on agent at every step of persistent asthma
As an option particularly in children < 5years with mild persistent asthma
When patients strongly resist takinginhalation medication in spite of adequatetraining and counseling
Exercise-induced asthma Aspirin-sensitive asthma Allergic rhinitis and asthma

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 39/77
Sustained release for regular use Inexpensive , but toxicNot more than 400 mg per day
(serum levels 1 – 5 mcg/ml)Anti-inflammatory effects
8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 40/77
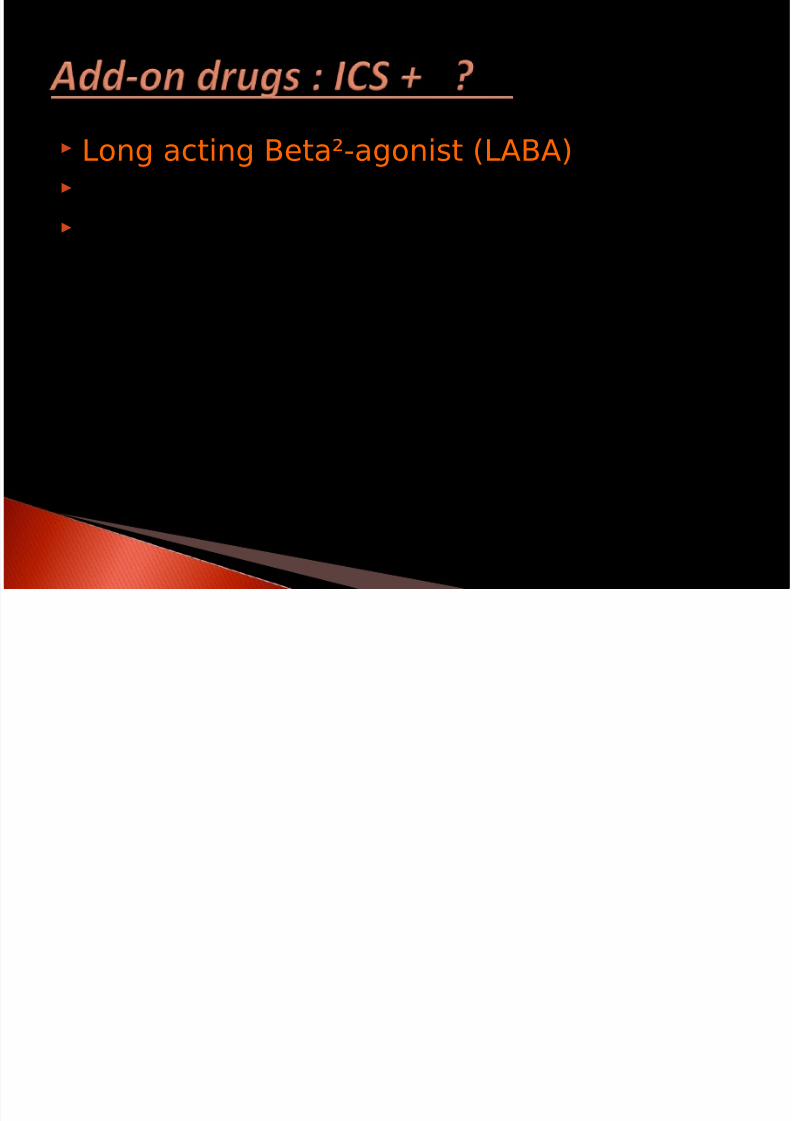
Long acting Beta²-agonist (LABA) Montelukast SR Theophylline

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 41/77
Non-pharmacological methods-insufficient evidence (Acupuncture,Homeopathy, Immunotherapy)
Breast feeding, smoking cessation,weight control for obesityrecommended
Role of non-static spacersAction plans

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 42/77
Monotherapy with cromones is nolonger given as an alternative tomonotherapy with a low dose of ICS
in adults. Long-acting beta-2-agonists likebambuterol are no longer
recommended as add-on agents insevere asthma.

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 43/77

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 44/77
Patients still suffer poor asthma control despite beingprescribed regular ICS or ICS/LABA treatment
Patients recognize impending worsening and managethese spontaneously by increasing their medication, butin a sub-optimal way
The time from early warning signs and the peak of aworsening provides a window of opportunity for betterself-management to reduce and prevent symptoms andexacerbations
There is a clear need of awareness at the level of both thephysician and patient to effectively control asthma

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 45/77

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 46/77
Base: all respondents (n=3,415)
Patients (%)
0 10 20 30 40
9+
5-8
3-4
1-2
None
Number
ofinhala t
ions/day

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 47/77
Proportion of patients reporting disease ‘relatively good’ in thepast week:
Relatively good
96%96%
87%87%
55%55%
Well-controlled by
ACQ
Not well-controlled by ACQ
Uncontrolled by ACQ
Relativel
y good
Relatively good
Patridge MR et al,BMC Pulmonary Medicine 2006,

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 48/77
Respiratory Medicine Vol 96 (2002) 835-840

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 49/77
Respir Med 2002; 96: 835-40

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 50/77
Fear about steroids Do not like public labeling as asthmatic Fear of addiction
Feel pumps reserved for serious orsevere attacks or will fail to act
Misconception that costly Prefer oral medications Physicians lack of knowledge and time

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 51/77
A new approach to asthma management

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 52/77
ICS plus LABA for prophylaxis and relief Simple one device treatment strategy Improves daily control
Prevents severe exacerbations moreeffectively than higher dose ICS plusSABA or maintenance ICS/LABA plusSABA reliever
Recommended in recent GINAguidelines

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 53/77
Control-drivenmanagement
“to achieve and maintaincontrol”
“Treating to target”
Not wellcontrolled
Partly controlled
Controlled

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 54/77
The goal of management is CONTROL of asthma
Current Clinical Control and controlling
Future Risk Addressing OBSTACLES to asthma
control Better use of CURRENT TREATMENTS

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 55/77
Develop a doctor / patient partnership
Doctor-directed patient self-Doctor-directed patient self-
managementmanagement

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 56/77
Single inhaler for relief andmaintenance
Regular maintenance dose (usually
twice daily) with additional inhalation(s)as needed Patients do not require a separate SABA Use of reliever is always accompanied
by an extra dose of anti-inflammatoryICS

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 57/77
Single maintenance and relief therapy For better informed and less compliant
patients Not for poor perceivers of worsening Home PEFR use preferred Patient directed rather than physician
controlled (now proven to be effective in
over 6 studies)

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 58/77
A highly effective way of stepping up anti-inflammatory therapy in line with disease activity
If a combination inhaler containing formoterol and budesonide is selected, it may be used for
both rescue and maintenance. This approach hasbeen shown to result in reductions inexacerbations and improvements in asthmacontrol in adults and adolescents at relatively lowdoses of treatment (Evidence A )

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 59/77
Emphasizes Asthma management on◦ Clinical control rather than classification of
patient by severity
Exacerbation◦ One of the important criteria in assessing
asthma control
This important shift reflects in
pharmacological care asthma includingnew treatment approach

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 60/77
Treats the underlying inflammation with
every inhalation
Reduces exacerbations
Improves daily asthma control
Reduces overall steroid load
Is simple to use with only one inhaler formaintenance and relief
1O’Byrne PM, et al. Am J Respir Crit Care Med 2005;171:129–136; 2Rabe KF, et al. Lancet2006;368:744–753;
3Vogelmeier C, et al. Eur Respir J 2005;26:819–828; 4Rabe KF, et al. Chest2006;129:246–256;
5Scicchitano R, et al. Curr Med Res Opin 2004;20:1403–1418; 6Kuna P, et al. Int J ClinPract 2007;In Press.

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 61/77
One or more present:◦ Use of accessory muscles of respiration
◦ Pulses' paradoxicas >25 mm Hg
◦
Pulse > 110 pm◦ Inability to speak sentences
◦ Respiratory rate >25 - 30 breaths/min
◦ PEFR or FEV1 < 50% predicted
◦ SaO2 < 91- 92%
McFadden Am J Respir Crit CareMed 2003

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 62/77
Tachypnea Tachycardia Wheeze Hyperinflation Accessory muscle use Pulses paradoxicus Diaphoresis (profuse sweating)
Cyanosis Obtundation (altered mental state)
Brenner, Tyndall and Crain In: Emergency Asthma. MarcelDekker 1999

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 63/77
Previous episode of near-fatal asthma Multiple prior ER visits or hospitalizations Poor compliance with medical treatments Adolescents or inner city asthmatics Recent use of oral corticosteroid (OCS) Inadequate therapy:
◦ Excessive use of β-agonists
◦
No inhaled corticosteroid (ICS)◦ Concomitant β-blockers
Ramirez and Lockey In: Asthma, American College of
Physicians, 2002

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 64/77
Lower or upper respiratory infections Cessation or reduction of medication Concomitant medication, e.g. β-blocker Allergen or pollutant exposure
8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 65/77

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 66/77
Respiratory frequency: (count)◦ Speech: sentences, single words
Auxiliary respiratory muscle use Posture: sitting, can patient lie down? Airway patency: rhonchi, silent chest (PEF) Respiration: cyanosis (SaO2, blood gases) General appearance, effort of breathing:
activity level (pulse rate)

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 67/77
Oral corticosteroids are the most powerfulmedications available to reduce airwayinflammation
Use until attack has completely abated:◦ PEFR and FEV1 at baseline levels
◦ Symptoms gone
Taper to QOD and determine if patient canremain well if corticosteroids are withdrawncompletely

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 68/77
Treat the condition symptomatically Determine what caused the exacerbation:
◦ inhalant allergen
◦ food allergen
◦ drug reaction (ASA, vaccination, etc)◦ infection
◦ worsening of a chronic condition:
◦ poor therapy compliance
Treatment needs adjustment

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 69/77
Use antibiotics if any suspicion of bacterial infection
If antibiotics are prescribed,recommendation is for broad spectrummacrolide antibiotics that cover atypicalbacteria (chlamydia, mycoplasma), eg,azithromycin, clarithromycin,
erythromycin, roxithromycin,dirithromycin, amoxicillin + clavulan;moxifloxacin, cefuroxin

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 70/77
IS A RESPIRATORY ATTACK! Consider improved prophylaxis:
◦ Treat, Monitor and Follow-up allergen avoidance
allergen vaccination
pharmacological treatment update
stop smoking
enhance compliance to recommendations
teaching and monitoring
8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 71/77
Seasonal asthma◦ Use same stepwise approach as for the long-term
management of asthma.
◦ Begin anti-inflammatory agents two weeks prior
to the anticipated onset of the season andcontinue through the season.

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 72/77
Seen more in young children. Use same stepwise approach as for the
long-term management of asthma.
Chronic use of anticholinergics for thisdisorder is not recommended

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 73/77
Poorly controlled asthma duringpregnancy results in increasedperinatal mortality; increasedprematurity and low birth weight
Controlling the mother's asthma withthe use of bronchodilators and anti-inflammatory medication is best for the
baby and mother
8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 74/77
Surgical patients receiving systemiccorticosteroids during the last 6 months
Give 100 mg hydrocortisone q 8 h i.v.
during the surgical period and reducedose rapidly 24 h following surgery

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 75/77
Missing cardiac asthma and treating itas bronchial asthma
Missing near fatal asthma cases
Misdiagnosing the severity of asthma Not giving inhaled steroid to patients
with persistent asthma Not differentiating between asthma and
COPD

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 76/77
Buying a Peak Flow Meter (severity of asthma,diagnosis of asthma, drug titration, aggravatingfactors, diagnosing exercise induced asthma,personal best parameter: chargeable test)
FEV1 test: small machine gives the FEV1 and canbe billed as mini spirometry
Asthma group counseling sessions can be charged

8/8/2019 Dr Raju Final- Bhandup
http://slidepdf.com/reader/full/dr-raju-final-bhandup 77/77