Embed Size (px)
Citation preview

SUPPORTIVE CARE IN PAEDIATRIC ONCOLOGY:
Oncologic Emergencies
Drug Related Side Effects
Late Effects
FRACP course 2017Mandy de Silva
Aims
• Main aim: Pass this exam
• Second aim: Pass this exam with flying colours
• Third aim: To understand how oncology works
Topics
• Oncologic emergencies (and urgencies)• Tumour lysis• Anterior mediastinal mass• Spinal cord compression• Anaphylaxis• Extravasation• Febrile neutropenia / Infections
• Drug related side effects• General• Post bone marrow transplant• Specific drugs
• Late effect (Late effect assessment programme: LEAP)
Oncologic Emergencies (and urgencies)
• Initial presentation of primary disease • Complication/ progression of known disease
• Complication of therapy
• Need to be addressed before therapy can begin or continue
• Aim:• Avoid end‐organ injury• Avoid compromising long‐term Quality Of Life
Tumour Lysis Syndrome (TLS)
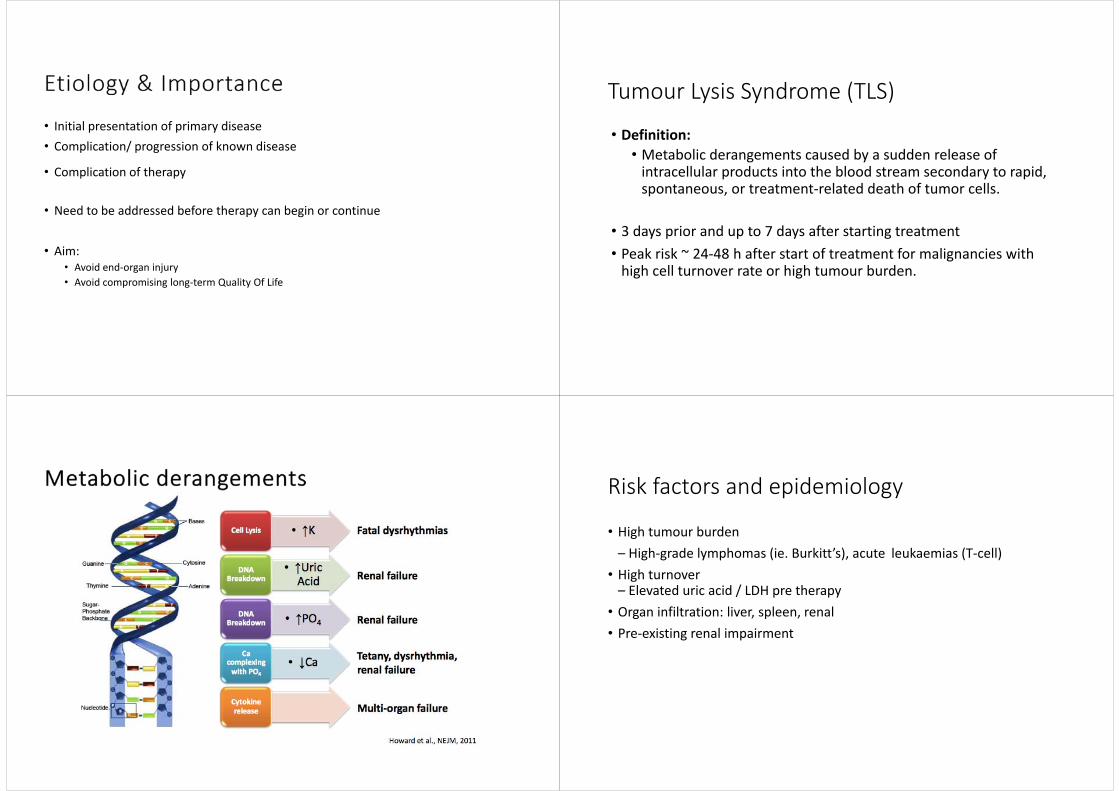
• Definition: • Metabolic derangements caused by a sudden release of intracellular products into the blood stream secondary to rapid, spontaneous, or treatment‐related death of tumor cells.
• 3 days prior and up to 7 days after starting treatment • Peak risk ~ 24‐48 h after start of treatment for malignancies with high cell turnover rate or high tumour burden.
Risk factors and epidemiology
• High tumour burden – High‐grade lymphomas (ie. Burkitt’s), acute leukaemias (T‐cell)
• High turnover– Elevated uric acid / LDH pre therapy
• Organ infiltration: liver, spleen, renal • Pre‐existing renal impairment

• Risk of xanthine nephropathy• Hyperhydration (double maintenance or 125ml/m2/hour)• Allopurinol
• xanthine oxidase inhibitor• To halt production of uric acid
• Rasburicase (0.2 mg/kg) • Urate oxidase to transform uric acid to excretable product• Contraindicated in G6PD deficiency
• Can be fatal • Need ECG and cardiac monitoring • Frequent laboratory assessment • Beware of pseudohyperkalemia during hyperleukocytosis
• Double check with blood gas machine• Calcium gluconate, insulin infusion, salbutamol, calcium resonium +/‐dialysis
Management ‐ Hyperphosphataemia
• Regular biochemistry• Fluids• Phosphate binders• May need dialysis
• Only treat if symptomatic • Fatigue, cramping, tetany, laryngospasm, weakness, paresthesia, Seizure, ECG changes (long QTc)
•Calcium Gluconate •Avoid calcium replacement while phosphate is rising, as Ca‐Po4 complex can worsen renal damage.
•complete and updated guideline on National Child Cancer Network (NCCN) website.
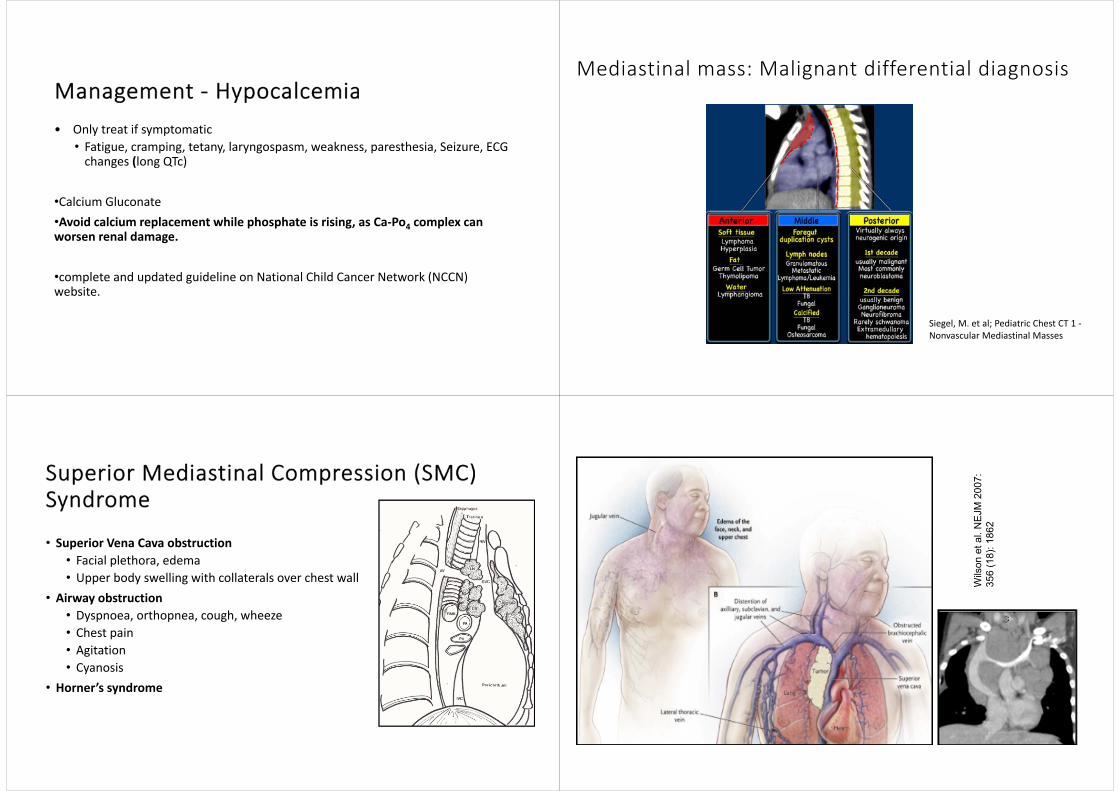
Mediastinal mass: Malignant differential diagnosis
Siegel, M. et al; Pediatric Chest CT 1 ‐Nonvascular Mediastinal Masses
• Superior Vena Cava obstruction• Facial plethora, edema• Upper body swelling with collaterals over chest wall
• Airway obstruction• Dyspnoea, orthopnea, cough, wheeze • Chest pain• Agitation• Cyanosis
• Horner’s syndrome
Wils
on e
t al.
NE
JM 2
007:
35
6 (1
8): 1
862

• 80% of mediastinal masses are malignant.
• ~10% tumours in the anterior‐superior mediastinum compress the SVC and / or proximal tracheal or main bronchus.
• St. Jude’s Experience (n= ~3700) Seth & Bhat, Ind J Pediatr, 2011 • NHL: 70% with mediastinal mass • Hodgkin’s: 30%• Respiratory compromise in up to 75%
Management
• Avoid sedation as can cause complete airway obstruction • Don’t lie flat• Call a friend– anaesthetist / ICU / cardiologist / radiologist etc (ie MDT involvement)
• CT scan and echo
• Full management can be found in NCCN website under Superior Mediastinal Compression (SMC) syndrome
• Neuroblastoma• Metastatic Brain Tumour• Primary Spinal Tumour• Ewing Sarcoma • Osteosarcoma • Soft tissue sarcoma eg Rhadbomyosarcoma• Lymphoma/Leukaemia (chloromas)
• Acute cord compression• 3‐5% of children at diagnosis – tumour of spinal or para‐spinal in origin
• Local or radicular pain > 80% – may be present for weeks • Weakness / sensory loss / paresis
• Motor weakness often present at diagnosis • Incontinence (cauda lesions) • Paraplegia / quadriplegia can progress rapidly & can be irreversible

Management
• Any compromise of the spinal cord, conus medullaris, or cauda equina requires emergent attention
• Imaging– X‐ray can miss up to 50% of cases–Emergency MRI if non‐ambulatory or significant deficits
• Emergency surgery, radiation, chemotherapy • Dexamethasone in some situations • Prognosis: children regain better function if treatment started within 10 days of onset
Anaphylaxis: Question
Which of the following is most commonly associated with Anaphylaxis?
(A) L’Asparaginase(B) Vincristine(C) Carboplatin(D) Doxorubin(E) None has significant risk of anaphylaxis
Answer
(A) L’Asparaginase(B) Vincristine(C) Carboplatin(D) Doxorubin(E) None has significant risk of anaphylaxis
Anaphylaxis
• Most commonly with
• L’Asparaginase, erwinia asparaginase and PEG asparaginase• Etoposide/Tenoposide• Carboplatin• ATG
• Less severe but marked allergic reactions with newer monoclonal antibodies

Extravasation: Question
Which of the above is associated significant risk of extravasation?
(A) Vincristine(B) Vinblastine(C) Dactinomycin(D) Carmustine(E) All of the above.
Answer
(A) Vincristine(B) Vinblastine(C) Dactinomycin(D) Carmustine(E) All of the above
Extravasation
• Significant risk associated with:
• Amsacrine, Carmustine, Dactinomycin, Daunorubicin, Doxorubicin, Epirubicin, Idarubicin, Vinblastine, Vincristine.
Question
A 12 yr old Girl with ALL undergoing consolidation therapy with High dose (20g) methotrexate complains of swelling around port with yellow fluid leaking out. Her parents are doctor and lawyer. What do you do????
(A) Do nothing(B) Aspirate and observe(C) Aspirate and arrange theatre for acute debridement by plastic surgeon(D) Stop infusion and observe(E) Contact your Lawyer and ensure defence insurance up to date.

Answer
(A) Do nothing(B) Aspirate and observe(C) Aspirate and arrange theatre for acute debridement by plastic surgeon(D) Stop infusion and observe(E) Contact your Lawyer and ensure defence insurance up to date.
Doxorubicin Extravasation
Febrile neutropenia / infections: Question
2 year old AML, has had High dose Cytarabine (AraC). Has HickmanLine in situ. Current febrile neutropenia. Clinically appeared shocked. What is the likely microorganism?
A. Coagulase negative staphB. Alpha Haemolytic StrepC. EnterococcusD. Staph aureus
Answer
A. Coagulase negative staph
B. Alpha Haemolytic Strep
C. Enterococcus
D. Staph aureus

Febrile Neutropenia
• >38˚C on 2 occasions or >38.5˚C on one occasion AND ANC of <0.5 x 109/L, or expected neutropenia from recent chemo
• Every cancer child with new onset fever needs urgent review because:• Chemotherapy causing decreased number and function of immune cells
• Radiation complication• Surgeries • Breakdown of mucocutaneous barriers • Foreign bodies (CVL, grafts etc.)
Febrile neutropenia
• Most common culprits are staph epi, streps, gram negative rods. But most rapidly lethal are gram negatives (E. Coli, Pseudomonas, Kliebsiella)
• Microbiological diagnosis only made in 10‐30%• Antibiotics should be started within the first hour
• Tazocin (Piperacillin / Tazobactam) monotherapy • HD araC exposure / AML / BMT – add Vancomycin• Known ESBL – add Amikacin• If shocked – add Amikacin and Vancomycin• If shocked, but cisplat exposure or risk of renal damage – use Meropenem• If low risk – consider Ceftriaxone as outpatient
Infection prevention• PCP: Cotrimoxazole/Pentamidine/Dapsone
• Candidiasis: Nystatin / fluconazole• Aspergillus /Mucormycosis: Ambisome• Black moulds: Voriconazole
• HSV / VZV: Acyclovir
• GCSF (eg interval compression)
Question12 yr old with osteosarcoma presents with high fever 40˚C, neutrophils of 0.1, platelets of 50. Rigors. Moderately tachycardic but alert and well perfused, BP ok. No localising signs. Has Hickman line in place. What is /are your antibiotic(s) of choice?
A. Amikacin, timentinB. Ceftazidime or Cefepime aloneC. Regular Gentamicin, timentin and vancomycinD. Meropenem

Answer
A. Amikacin and timentinB. Ceftazidime or Cefepime aloneC. Regular gentamicin, timentin and vancomycinD. Meropenem
Question
In regards to chickenpox exposure, which statement is NOT correct?
A. recent evidence suggests the previous 96hr cut off for ZIG is no longer valid and can be given at any time. Isolate day 7 to 28B. If day 5 could give acyclovir for 7‐10 days C. Viraemia can occur from day 6 but can be delayed until day 28D. Monthly IVIG is not protective
Answer
A. Recent evidence suggests the previous 96hr cut off for ZIG is no longer valid and can be given up tp 10 days. Need to be isolated day 7 to 28
B. If day 5 could give acyclovir for 7‐10 days
C. Viraemia can occur from day 6 but can be delayed until day 28
D. Monthly IVIG is not protective
Drug related side effects

Nail changes
A FungusB BacterialC Hand and Nail diseaseD chemotherapy effect
ANSWER: D
Inflammation of mucous membranes
• Mucositis: Chemo drugs• Stomatitis: Candida/ Herpes• Oesophagitis: Candida• Typhlitis = neutropenic colitis
• GVHD of gut• Can involve the whole of the alimentary tract ie. Mouth anus
Question
Which of the below are associated with mucositis
(A) Bleomycin(B) Methotrexate(C) Thioguanine(D) Doxorubicin(E) All of the above.
Answer
(A) Bleomycin(B) Methotrexate(C) Thioguanine(D) Doxorubicin(E) All of the above
Mucositis
Drugs associated with Mucositis:
• Bleomycin, Daunomycin, Methotrexate, Mitozantrone, Thioguanine, Thiotepa, Vinblastine, Idarubicin, Mercaptopurine, Melphalan, 5‐Fluorouracil, Hydroxyurea, Doxorubicin.
Prevention/treatment of mucositis /stomatitis
Prevention • Hyperhydration• Folinic acid• Oral Health (dental care, mouth washes)
• Nutrition• Antifungals • Delay dose of chemotherapy• Glutamine
Treatment• Analgesia• Mouthwashes• IV antifungals• IV antivirals if HSV suspected/not yet ruled out
• Keratinocyte growth factor stimulant
Nausea and vomiting in cancer can be multifactorial
Vomiting centre
Vestibular Apparatus
Cardiovascular and Abdominal afferents (vagal)
Chemoreceptor Trigger Zone
Limbic cortex
Peripheral pain pathways
Vomiting
mass

Vomiting centre
Vestibular Apparatus
Cardiovascular and Abdominal afferents (vagal)
Chemoreceptor Trigger Zone
Limbic cortex
Peripheral pain pathways
Vomiting
mass
Nausea and Vomiting• 5HT3 receptor antagonists– Ondansetron (Zofran)• Corticosteroids – Dexamethasone• NK1 antagonists –Aprepitant• Anti cholinergic ‐‐ Hyoscione (Scopoderm TTS)• Antihistamines – Cyclizine (vestibular centres)• Dopaminergic ‐‐Metoclopramide/Domperidone• Phenothiazines ‐ Chlorpromazine• Benzodiazepines ‐ Lorazepam/ Diazepam• Cannabinoids – Nabilone, THC but with warning re aspergillosis
• Non Pharmacological interventions (psychologist, play therapist, accupressure randomised trial underway etc).
Myelosuppression / Bone marrow failure
• Bone marrow infiltration by disease• Infective agents esp viral (parvovirus)• Chemotherapy• Anti infective: Gancyclovir / Aciclovir / Cotrimoxazole• Radiotherapy (esp. pelvis and spine)• Nutrient deficiencies: B12/folic acid• Renal/ Hepatic dysfunction causing increased toxicity
• Supportive with transfusions (know thresholds), GCSF, EPO/iron in selected cases, thrombopoietin (romiplostim)
Altered body image impacting on psychological well being• ALOPECIA• Portacath /CVL line insertion sites• Surgical Scars/Amputations
• Weight loss / gain• Cushingoid features
• LOSS OF CONTROL.
Most of the common chemotherapeutic agents we use cause alopecia• Frequent/Severe
• Anthracyclines• Taxol• Ifosphamide• Cyclophosphamide• Vindesine• Bleomycin• Actinomycin C
• Moderate/Dose Dependent
• 5‐FU• Mitoxantrone• Etopside• Methotrexate• Vincristine• Vinblastine• Carmustine• Hydroxyurea• Rare/ Less common /dose
dependant• Cisplatin• Asparginase• Dacarbazine• Procarbazine• mercaptopurine
The image part with relationship ID rId3 was not found in the file.
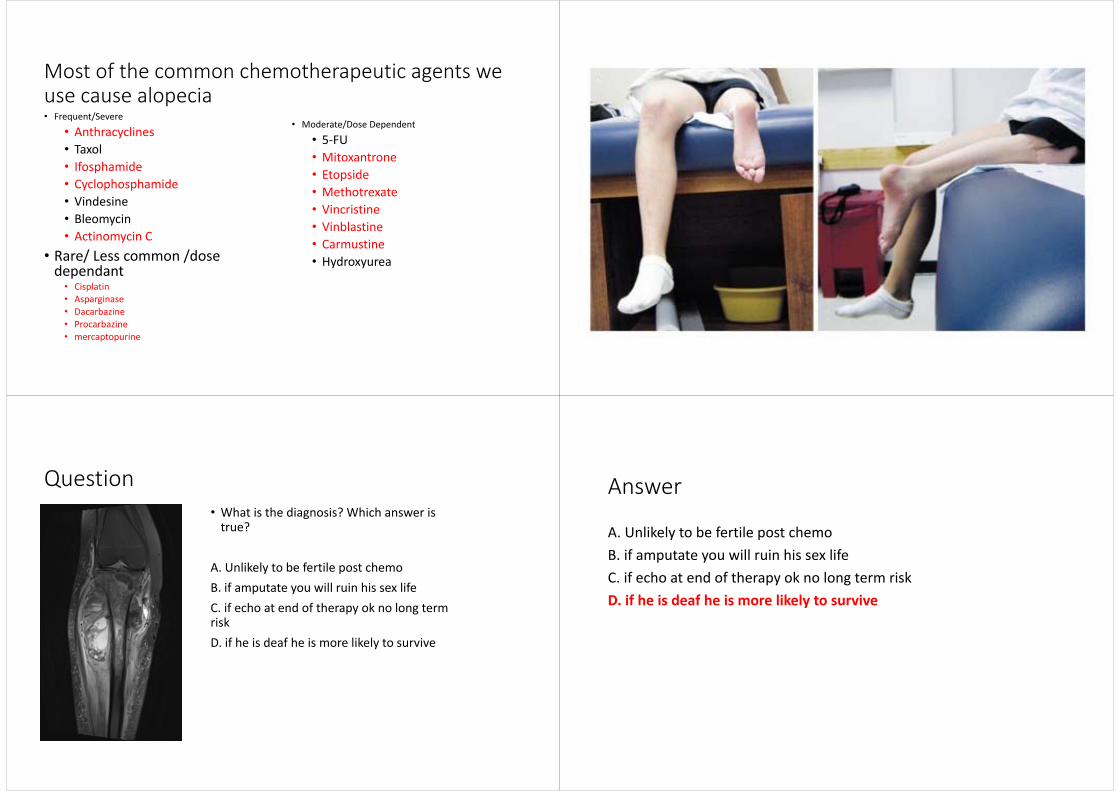
Question• What is the diagnosis? Which answer is true?
A. Unlikely to be fertile post chemoB. if amputate you will ruin his sex lifeC. if echo at end of therapy ok no long term riskD. if he is deaf he is more likely to survive
Answer
A. Unlikely to be fertile post chemoB. if amputate you will ruin his sex lifeC. if echo at end of therapy ok no long term riskD. if he is deaf he is more likely to survive

Post BMT complications: Question
At day 10 post bone marrow transplant: painful hepatomegaly, ascites, increased weight gain, and jaundice. Ultrasound does not show reverse flow in portal system
A. GVHD pulse of 2mg/kg steroidsB. Viral hepatitisC. Veno‐occlusive disease start defibrotide immediatelyD. cholangitis add antibiotics
Answer
A. GVHD pulse of 2mg/kg steroidsB. Viral hepatitisC. Veno‐occlusive disease start defibrotide immediatelyD. cholangitis add antibiotics
Veno‐occlusive disease (VOD or SOS)
• Risk factors:• cyclosporin, busulphan, cyclophosphamide, antibiotics/antifungals
• Urso / Defibrotide protective• Signs:
• Weight gain, increased bili, tender hepatomegaly, platelet refractory• Micro thrombosis within the hepatic system• Biopsy is gold standard but doppler U/S of use although changes are often late
Graft Vs host Disease (GVHD)
The image part with relationship ID rId3 was not found in the file.

GVHD• Post transplant • Acute / chronic • Single or multiple organs
• Skin, liver and gut are the main sites but can involve others
• One of leading causes of death in MUD transplants• mortality in non‐steroid responsive > 50%
• Prevention : T cell depletion infusion / ATG / Cyclosporin / campath / cyclophosphamide
• Treatment : adequate Cyclosporin levels / steroids / newer anti‐TNF IL2 egInfliximab & Dacluzimab, Etanercept, PUVA
Engraftment syndrome
• Earlier, precedes count recovery• Rash, fever, capillary leak, pulmonary oedema • Can be independent of GVHD • Unclear cytokine triggers • Higher risk in high cell dose• Treatment: steroids with rapid wean
Question
Day 80 post BMT. Severe GVHD on immunosuppresive treatment.
What does the CT scan show?
What is your next step?
A. Bronchoscopy +/‐ lavage
B. Lobar/segmental excision
C. Fine needle Biopsy
D. increase immunosuppression/steroids
Answer
A. Bronchoscopy +/‐ lavage
B. Lobar/segmental excision
C. Fine needle Biopsy
D. increase immunosuppression/steroids
Fungal therapy
• Fluconazole shown to reduce candida and increase survival• Itraconazole (vs fluconazole) in high risk patients can increase fungal free survival
• Liposomal Amphoterecin B expensive• Voriconizole (vs amphotericin B) superior for treatment of invasive aspergillosis infections but multiple interactions (P450) esp vincristine
• Caspofungin for resistant strains • Combination therapy often advocated but minimal evidence
Lymphoproliferative Disorder • Post transplant (solid organ and BMT) complication due to the lack of T cells
• Usually accompanied by increasing plasma EBV viral load • Can present in multiple or isolated organs
• Bowel / lung / plasma / CSF
• Management:• Reduction in immunosuppression • In resistant cases, add rituximab and cyclophosphamide +/‐ antiviral
Specific drug related side effects

Haemorrhagic cystitis• Culprit:
• Alkylating agents: Cyclophosphamide / Ifosfamide• Management:
• Hyperhydration• MESNA
• Need to rule out BK virus
• Late effects: bladder scarring
Cardiotoxicity ‐ cardiomyopathy• Culprits:
• Anthracyclines (Doxorubicin/Daunorubicin) >250‐300mg/m2 cumulative dose)
• Mitoxantrone• HD Cyclophosphamide • TBI
• Echo: LVFS and LVEF decreases, increased afterload• Usually seen in
• pubertal growth• cardiac deaths in runners• pregnancy/childbirth girls
Cardiotoxicity
• Electrolytes especially potassium, magnesium and trace elements
• Dietary likely important but hard to prove • Worst cases: malnourished girls
• Hypertension predictive of CHF
• Long term cardiac deaths increased in survivors, worse with as little as 5Gy radiation, and also worse with combination of Vinka‐akaloids
• Early intervention with ACEI modifies onset in adult randomised trial
Dezrazoxane
• Cardioprotectant agent
• Latest studies in paediatrics T‐ALL, NHL have shown:• Cardioprotective effect (better LV function)• No compromise in antitumour efficacy• No increase in toxicities• No increase in second malignancies
• Beneficial for >300mg/m2 anthracyclines (eg: Osteosarcoma).

SNP’s prediction of anthracycline‐induced cardiotoxicity (ACT)
• Retrospective study • Identified genetic variants associated with ACT
• 96% accurately predicted to have no acute cardiac toxicity in low risk group
• 75% accurate predicted to have ACT 36% in high risk group
Methotrexate• Antimetabolites• Competes with folic acid for protein binding folic acid deficiency tumour cell death
• Cotrimoxazole/ Penicillin based drugs interfere with urine excretion
• Third spacing
• Mucositis, transient liver function derangement
• Folinic Acid (Leukovorin) prevents / reduces side effects.
Cytosine Arabinoside (Ara‐c, cytarabine)
• Risk of conjunctivitis if high dose• Rx Steroid eye drops
• Low dose fevers 12 hr post dose• Rash
• Neurotoxicity• Peripheral neuropathy• Cerebellar ataxia• Seizures
Platinum (Cisplatin > Carboplatin)Nephrotoxicity• Cr EDTA GFR baseline / regular repeats
• Cystatin C on top of Creatinine• Hyperhydration• Mannitol rather than frusemide(worse nephrotoxicity)
Ototoxicity• High frequency sensorineural hearing loss (HFHL)
• More so with Cisplatin• Audiology as baseline / regular follow upsBrock Grading system (>2 years old)
• Brock et al, Hospitals for Sick Children, 1991
• Synergistic toxicity : Aminoglycosides & RT CNS

Common audiology findings for children who have had Cisplatin using Brock grading HFHL• <40dB at all frequencies Grade 0• >40db at 8000Hz only Grade 1• >40db at 4000Hz and above Grade 2• >40db at 2000Hz and above Grade 3• >40db at 1000Hz and above Grade 4
Grade 1‐2 hearing loss
Neurological side effects
Peripheral Neuropathy• Vincristine• Vinblastine• Cisplatin• Ifosfamide
Leuko Encephalopathy• HD Methotrexate • +/‐ intrathecals in combination• Radiotherapy• Seizures• MRI changes
Try and remember where in the Cell Cycle does a drug act on – good luck!!!
Do you need to stand up and stretch????

Late effects (LEAP)
Improved survival rate in the last 3‐4 decades
http://www.cancerresearchuk.org/cancer-info/cancerstats/childhoodcancer/
If you are interested, read this:
Nature Reviews Cancer14,61–70(2014)doi:10.1038/nrc363405 December 2013
Wake up and Guess The Diagnosis!!!
• 4 yr old • Abdo mass• Elevated BP
High Risk Neuroblastoma – at least stage 3

Late effects: Question
Which statement is false?
A. Hearing impairment can be due to cisplatinB. Short stature is multifactorialC. Infertility risk is due to vincristine D. Renal insufficiency can be due to radiationE. Second malignancies can be due to radiation, akylator, and topoisomerase II inhibitors F. Pulmonary fibrosis risk increases with Busulphan
Answer
A. Hearing impairment risk due to cisplatinB. Short stature is multifactorialC. Infertility risk is due to vincristine D. Renal insufficiency due to radiationE. Second malignancies radiation, akylator, and topoisomerase II inhibitors F. Pulmonary fibrosis risk with Busulphan
HFHL
• 16 month old girl with hepatoblastoma, treated with Cisplatin alone at total dose 480mg/m2. Moderate(Grade 2‐3) HFHL bilaterally. Fitted with hearing aids.
• Can be permanent hence the need for hearing aids (30%, but ranges from 25‐100% depends on testing methods)
• Increasing risk with increasing cumulative dose of platinum agents• Considerable individual susceptibility (pharmacogenomics)• Recent phase 3 trial (SIOPEL 6) report seems encouraging about otoprotective outcome with Sodium Thiosulphate (STS)
Audiology
6 July 2004 - Baseline
29 December 2004 – Post Cisplatin #3
21 June 2005 – Follow up
10 November 2004 - Post Cisplatin #2
16 February 2005 – Post Cisplatin #4

Hearing: Posterior fossa radiation fields
Protons Photons (Standard)
Lin et al, Int J Rad Onc Biol Phys, 2002
Pulmonary Fibrosis
• Bleomycin• Lomustine• Busulphan• Lung irradiation
• Pulmonary function test• Respiratory team involvement
Question: Post leukaemia therapy ‐ which is false?A. Teens most at riskB. Boys worse than GirlsC. Dexamethasone is worse than prednisone although cure rates are higher with dex.D. Steroid reduction, use of Statins and bisphosphonates are being trialled for prevention
Answer
A. Teens most at riskB. Boys worse than GirlsC. Dexamethasone is worse than prednisone although cure rates are higher with dex.D. Steroid reduction, use of statins and bisphosphonates are being trialled for prevention

Bone density / osteoporosis
• Steroids toxicity • Randomised trial shows exercise can correct
Question
5 year old boy diagnosed with high risk B cell leukaemia. Four weeks into induction therapy, he has difficulty walking especially upstairs. On examination he has gained 4kg since diagnosis, has depressed reflexes in all limbs and is weak proximally > distally. Which two are false?
A. He most likely had a white cell >50 at diagnosis to be high riskB. Most likely cause for his weakness is vincristine induced neuropathyC. It is likely that an echo will show a reduction in ejection fraction/fractional shortening D. At 28 days of therapy there is approximately a 95% or better chance he is already in remission morphologically
AnswerA. He most likely had a white cell >50 at diagnosis to be high riskB. Most likely cause for his weakness is vincristine induced neuropathyC. It is likely that an echo will show a reduction in ejection fraction/fractional shortening D. At 28 days of therapy there is approximately a 95% or better chance he is already in remission morphologically
Steroid induced myopathy
METABOLIC SYNDROME IN CHILDHOOD CANCER SURVIVORS

Long‐term Endocrine Complications• Hypothalamic‐Pituitary Dysfunction
• GH deficiency• Early puberty• LH/FSH, TSH, ACTH deficiencies• Hyperprolactinemia• Obesity
• Thyroid abnormalities• Primary hypothyroidism• Hyperthyroidism• Thyroid neoplasms
• Gonadal dysfunction• Males
• Infertility• Leydig cell failure
• Females• Acute ovarian failure• Premature menopause
• Bone disease• Osteoporosis• Osteonecrosis• Rickets
• Metabolic abnormalities• Insulin insufficiency• Insulin resistance/metabolic syndrome
MSKCC, n=115Number of patients
0 10 20 30 40 50 60
GH def
TSH def
ACTH def
Primary Hypothyroid
LH/FSH def
DI
Prec Puberty
Ovarian Failure
≥1 endocrine conditions reported by 43% of survivors in CCSS (n=1,607)
Gurney et al, Cancer 2003
Growth failure is multifactorial
Medulloblastoma Radiotherapy Dosimetry – Radiation to pituitary and hypothalamus Spinal Radiotherapy
Laughton SJ et al. JCO 2008
Second malignancy
• Rates around 2% above expected on average • Worst groups are
• Radiation exposure: AML, sarcomas• Etoposide exposure: AML, sarcomas• Hodgkins: mantle field irradiation • Genetic predispositons: retinoblastoma, fanconi anaemia, TP53 etc
Moskowitz C S et al. JCO 2014;32:2217-2223
Cumulative risk of breast cancer
Neuropsychological impairment
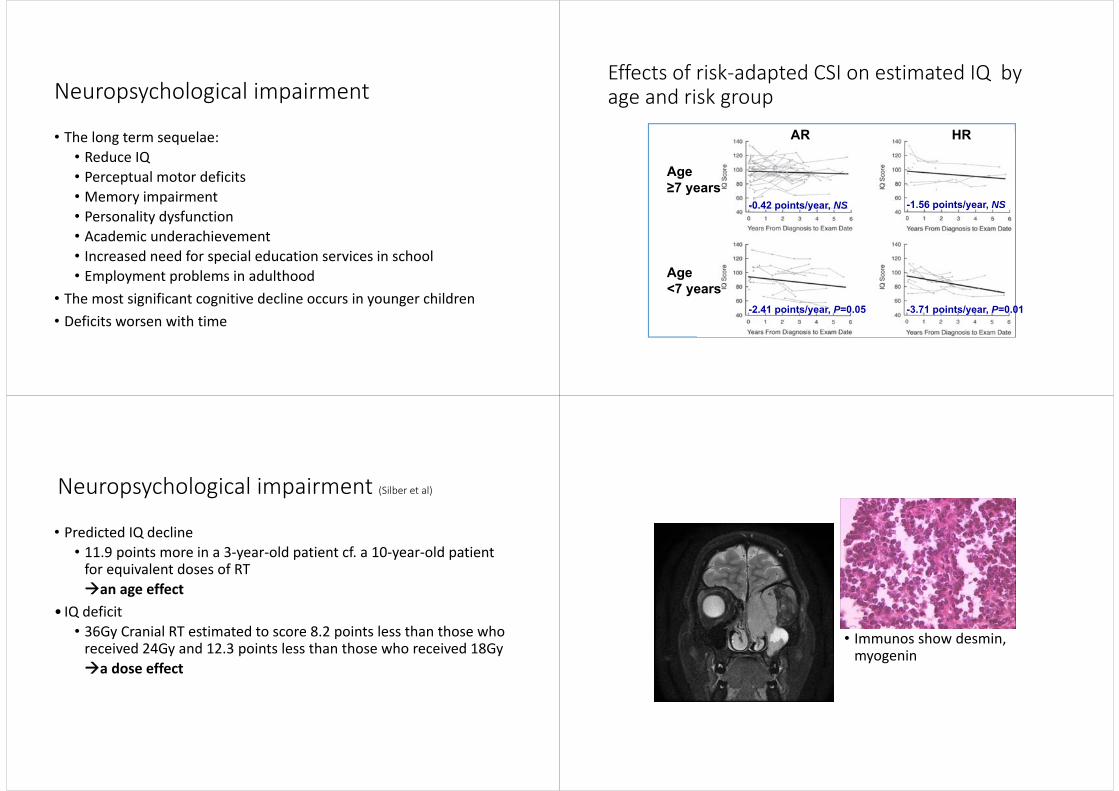
• The long term sequelae:• Reduce IQ• Perceptual motor deficits• Memory impairment• Personality dysfunction• Academic underachievement• Increased need for special education services in school• Employment problems in adulthood
• The most significant cognitive decline occurs in younger children • Deficits worsen with time
Mulhern, R et al. Journal of Clinical Oncology 2005, 23:5511-5519
Effects of risk‐adapted CSI on estimated IQ by age and risk group
-1.56 points/year, NS-0.42 points/year, NS
-2.41 points/year, P=0.05 -3.71 points/year, P=0.01
AR HR
Age ≥7 years
Age <7 years
Neuropsychological impairment (Silber et al)
• Predicted IQ decline• 11.9 points more in a 3‐year‐old patient cf. a 10‐year‐old patient for equivalent doses of RTan age effect
• IQ deficit• 36Gy Cranial RT estimated to score 8.2 points less than those who received 24Gy and 12.3 points less than those who received 18Gya dose effect
• Immunos show desmin, myogenin

Late effects which one not at risk?
• A. Hearing• B. Cataracts• C. Facial asymmetry• D. Infertility• E. Second malignancy
FERTILITY AFTER CANCER TREATMENT
Boys: Most effective and established means of preserving fertility is sperm
cryopreservation prior to treatment.
• < Tanner stage 3 (~ 14 yrs): • Unlikely to have viable sperm, so no means of collecting / storage in NZ. • Experimental means being looked at internationally
• > Tanner stage 3: • Spermache should have been achieved. Can be tested for by doing urine samples and checking for sperm
• Sample via ejaculation is best (approx 20million sperm)• Second choice is testicular biopsy or aspiration under GA / sedation.
Timing
• Needs to be prior to chemotherapy or >3 months off therapy as sperm have no DNA repair mechanisms
• Store prior to initiation of therapy only• Still worthwhile storing after treatment just in case relapse• Storage is funded in NZ

Girls:Most effective and established means of preserving fertility
is embryo and oocyte cryopreservation prior to cancer treatment
• Hormonal egg maturation stimulation• Ovarian stimulation and oocyte retrieval Requires 10‐17 days (before chemotherapy)
• Transvaginal collection• 200+ babies worldwide• Not for hormonal dependant tumours • No age restriction on ethics approval• No risk of disease transmission
In Vitro Maturation
• Collection of immature oocytes from small follicles• Ovarian stimulation not compulsory • In vitro maturation of harvested eggs or ovarian tissue• Newer technology and avoids one month waiting time• Can be used from frozen• Still end up with having to fertilise egg for storage• Currently experimental
• Protocol is currently open at Starship• New diagnosis or relapsed cancer (not leukaemia / ovarian ca)• >50% risk of ovarian failure• </= 18 years old • Realistic chance of >/= 5 years survival • Whole ovary or portion of an ovary
OVARIAN TISSUE FREEZING
• Risks:• Surgical and anaesthetic risks• May compromise remaining ovarian function• No guarantee of future fertility• Delay in treatment commencement• Tumour cell transmission during reimplantation.
• 70+ babies born worldwide (compared with >5 million IVF babies)• Cost: funded for 5 years, and self‐funded thereafter
OVARIAN TISSUE FREEZING

Management
• Elevated LH, FSH, low estradiol suggest ovarian insufficiency• Earlier testing with Antimullerian hormone (AMH) and/or follicle count (requires trans vaginal ultrasound)
• Therapy with OCP or HRT or replacement slice of ovary (if stored)
Childhood Cancer Survivor Study (CCSS)
Resource designed to investigate long‐term effects among five‐year survivors of childhood and adolescent cancerData‐base ‐ cohort 16,000 , (NOW >30 000)diagnosed < age 21 between 1970‐1986 & SIBLINGScommon cancers‐ leukaemia, lymphoma, brain tumours, neuroblastoma, wilmstumour, bone tumours and soft tissue sarcomasHundreds of publications all freely available
Need Advancement in therapies to minimize short and long term side effects while maintaining survival rate.
PROTONS AND OTHER IMPROVEMENTS TO XRT
Less dose to non target organs Expensive and not available locallyIn retrospective data less second malignancies.IMRT technology also improving secondary organ damage

GD2 receptor antibody Ch14.18 – “Biggest advance in NBL in decade”
• Chimeric • Anti GD2 • Given alone it is
less effective
NEJM Sept 2010 Yu et al
Other new therapy
Tyrosine Kinase inhibitorsImatinibCrizotinibDasatinib
Monoclonal antibodiesRituximab anti CD20 B cellsAlemtuzumab anti CD52 both B and T cellGemtuzumab anti CD33 myeloid cellsPembrolizumab anti-PD1
Cancer genomic profiling – Personalized medicine
• http://www.pedsoncologyeducation.com/
• www.fertilehope.org
• http://atlasgeneticsoncology.org/
• http://www.anzchog.org/
• http://www.survivorshipguidelines.org/• St Judes life time cohort studies

Thank Goodness This is THE END!!
Any Questions?





























