Embed Size (px)
Citation preview

What is PD?
Dr Catherine Dotchin MD MRCP
Consultant Geriatrician

Overview of presentation
• Case history
• Video example pre and post treatment
• Historical review
• PD in the UK
• Epidemiology and aetiology
• Making the diagnosis
• Main clinical features

Case reportThis man was seen, and diagnosed, in 1995, when Richard was
investigating stroke in the Hai district.
At that stage, he was 30 years old and displayed clear signs of
Parkinsonism. He had been unable to afford to visit anyone regarding
his condition and as a result had become increasingly slow and his
mobility had deteriorated markedly. He has left-sided tremor
predominant PD. This has led him to give up work in his ‘shamba’, his
only source of income.
He has many other symptoms, including freezing, difficulty rising from a
chair, drooling of saliva, cramps and pain in his legs and arms, quiet
voice, difficulty communicating, nocturia and frequency and constipation.

Case report cont.
• CD visited him again at the end of 2005 (an annually
since then)
• Now, he is 40 years and is limited to mobilising around
his house and in the small area of yard outside it. He has
tried various treatments from the village traditional healer
who had diagnosed ‘evil spirits’. These have included
oral medication, topical treatment, inhalations and
tattoos, but none of them had benefit. He relies upon
help and financial support from his nephews. Many find
his symptoms distressing, as they believe he is a “young
man who has grown old too soon”.


After 3 months of treatment with
levodopa/carbidopa

James Parkinson

The History of Parkinson’s
Disease
• Parkinson’s Disease (PD) was first described by
James Parkinson in 1817
• He noted
– ‘involuntary tremulous motion’
– ‘a propensity to bend forwards’
– ‘to pass from a walking to running pace’
– ‘the senses and intellect being uninjured’
• 40 years later Charcot named Parkinson’s
Disease

Parkinson’s Disease Defined
• Parkinson’s Disease is:
– A chronic, progressive, neurological
degenerative disease
• The contemporary definition is:
– ‘Multi-system neurological disorder which
affects cognitive processes, emotion and
autonomic function.’ (Playfer 2001)
Pathological findings:
• Progressive loss of dopaminergic cells in the
substantia nigra of the basal ganglia

Epidemiology (UK)
• 1% of population > 65 years have PD.
• A typical GP practice will have no more
than 5 PD patients.
• 6% of NH residents have PD.
• 150,000 NH + 350,000 Res care beds.
• Therefore 30,000 PD pts in care (£300m).
• Complex needs.

Aetiological theory for PD

What causes Parkinson’s?
Parkinson’s disease
Ageing Genes
50
60
70
Possible protective effect: smoking and caffeine
Environment

When do clinical signs of
Parkinson's develop?
Striatal dopamine levels
Reduced by 80%
Cell loss in the substantia nigra
Reaches 50%

Basal Ganglia simplified functions!
• controls the preparation, initiation,
sequencing and timing of well learnt motor
skills
• ‘auto pilot’ facility


The ‘Braak hypothesis’
Stage 1 and 2:
Pathology confined to certain
structures in the brain stem,
not yet the substantia nigra
Stage 3 and 4:
Pathology spreads to the
midbrain and basal ganglia
Stage 5 and 6:
Changes spread to the
cortex
Image adapted from The Professionals Guide to Parkinson’s Disease,
Parkinson'sS

DIAGNOSIS

Different Doctors do Different
Diagnoses
• Pathologist - Brainstem Lewy Bodies – PM
findings
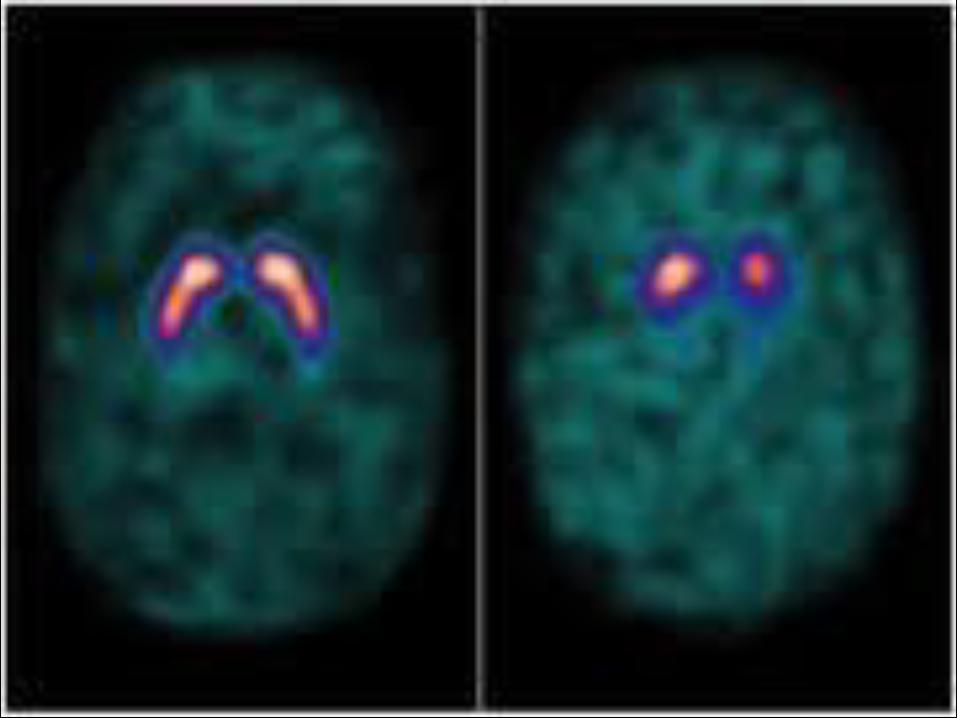
• Radiologists - Fluorodopa PET scans
• Clinicians - Varying clinical criteria

Diagnostic Accuracy
• Clinical diagnosis
• Typically only 90% in specialist hands
• Several differential diagnoses
• 70% of parkinsonism will be PD

Differential Diagnoses
• Drug induced parkinsonism
• Cerebrovascular parkinsonism
• Lewy body dementia
• Alzheimers disease
• Multi system atrophy
• Progressive supranuclear palsy
• Benign essential tremor

Probable most important
diagnostic criteria
• Asymmetrical onset
• Progressive condition
• Responsive to levodopa

Motor symptoms of Parkinson’s
Freezing
Postural
instability
Bradykinesia
Rigidity
Tremor
Motor
symptoms
of Parkinson's
Speech
Arising from
a chair
Posture
Reduced arm
swing
Hypomimia
Shuffling gait
Gait festination
Turning
Turning in bed
Micrographia
Falls

Motor symptoms
• Tremor
– Absent in up to 30% of people with PD
• Bradykinesia
• Rigidity
• Postural instability
– Usually later presentation

Non motor symptoms of
Parkinson’s Disease• Cognitive deficiencies
• Depression
• Raised anxiety levels
• Balance and falls
• Sleep disturbance
• Fatigue
• Pain
• Bowel and bladder problems
• Sexual dysfunction
• Weight loss
• Skin

Clinical Diagnosis
• “Neurological signs that improve on
Ldopa”
• Often not apparent on first assessment
• The use of time as a diagnostic tool
• Interdisciplinary assessments
• No straightforward test

Investigations
• Routine blood investigations
• DAT Scan – normal in essential tremor and drug-induced Parkinsonism
• +/- MRI Scan
• ?Dopamine challenge – reasonable dose for reasonable length of time
• “Sniffin sticks” – objective change in sense of smell at diagnosis in over 70%
Conclusion
• Progressive, chronic, multisystem
neurological condition
• Clinical criteria used to make diagnosis by
physicians
• Risk factors – age, family history, genetics,
environment
• Good symptomatic treatment is available
which will improve quality of life





























