Embed Size (px)
Citation preview

Confidential: For Review OnlyDouble blind randomized controlled trial of postoperative
low molecular weight heparin bridging therapy for patients who are at high risk for arterial thromboembolism
(PERIOP2)
Journal: BMJ
Manuscript ID BMJ-2021-064134
Article Type: Research
BMJ Journal: BMJ
Date Submitted by the Author: 07-Jan-2021
Complete List of Authors: Kovacs, Michael; University of Western Ontario; London Health Sciences Centre, MedicineWells, Philip; Ottawa Health Research Institute; University of Ottawa, MedicineAnderson, David; Dalhousie University, MedicineLazo-Langner, Alejandro; University of Western Ontario, MedicineBates, Shannon; McMaster University, MedicineBlostein, Mark; McGill University, HematologyKahn, Susan; McGill UniversitySchulman, Sam; McMaster University, Division of Hematology and Thromboembolism, Department of MedicineSabri , Elham; Ottawa Hospital Research Institute, Clinical Epidemiology ProgramRamsay, Timothy; Ottawa Health Research InstituteYeo, Erik; University of Toronto, MedicineRodger, Marc; McGill University, Medicine
Keywords: anticoagulation, thromboembolism, bridging
https://mc.manuscriptcentral.com/bmj
BMJ

Confidential: For Review Only
Page | 1
Double blind randomized controlled trial of postoperative low molecular weight heparin bridging
therapy for patients who are at high risk for arterial thromboembolism (PERIOP2)
Authors. 1Michael J. Kovacs, 2Philip S. Wells, 3David R. Anderson, 1Alejandro Lazo-Langner,
4*Clive Kearon, 4Shannon M. Bates, 5Mark Blostein, 5Susan R. Kahn, 4Sam Schulman, 6Elham
Sabri, 5*Susan Solymoss, 6Tim Ramsay, 7Erik Yeo, and 5Marc A. Rodger; for the PERIOP2
Investigators
*These authors are deceased.
Affiliations. 1Department of Medicine, Western University, London, ON, Canada; 2Department
of Medicine, University of Ottawa, Ottawa Hospital Research Institute, Ottawa ON Canada,
3Department of Medicine, Dalhousie University, Halifax NS Canada, 4Department of Medicine,
McMaster University and Thrombosis and Atherosclerosis Research Institute, Hamilton ON,
Canada, 5Department of Medicine, McGill University, Montreal QC Canada, 6Ottawa Hospital
Research Institute, Ottawa ON Canada, and 7Department of Medicine, University of Toronto,
Toronto ON Canada.
Word count (text): 2530
Correspondence: Michael J. Kovacs MD FRCPC, Hematology Division, London Health
Sciences Centre, 800 Commissioners Rd E, Rm E6-214, London ON, N6A 5W9, Canada
Tel: (519) 685-8500 Ext. 52254
Fax: (519) 685-8294
Email: [email protected]
Page 1 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 2
Key Points
It has been uncertain if post-procedure bridging with low molecular weight heparin is necessary
when warfarin is stopped in patients with atrial fibrillation or mechanical valves undergoing a
procedure. This prospective multicentre double-blind placebo-controlled trial in 1471 patients
found rates of major thromboembolism of 1.23% for placebo and 0.98% for dalteparin and major
bleeding rates of 2.00% and 1.34% respectively that were not significantly different. Hence this
study did not find a significant benefit of post-procedure dalteparin bridging to prevent major
thromboembolism in patients with atrial fibrillation or mechanical valves who need warfarin
stopped for a procedure.
Page 2 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review Only
Page | 3
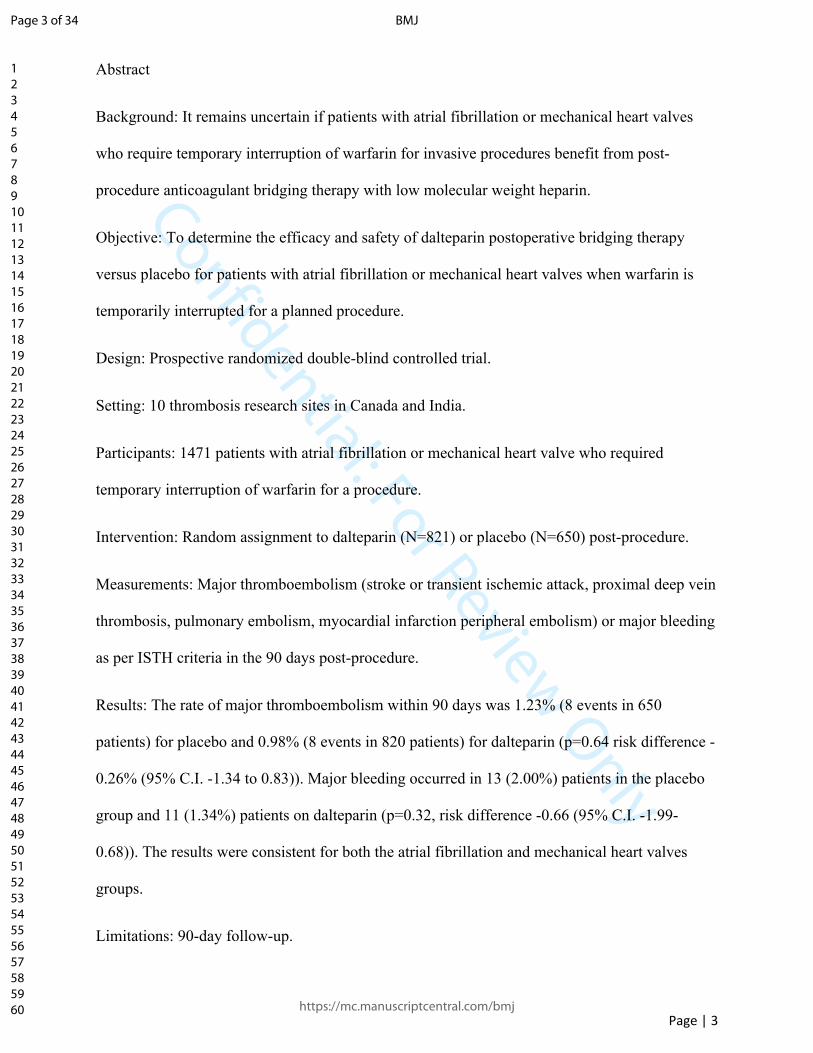
Abstract
Background: It remains uncertain if patients with atrial fibrillation or mechanical heart valves
who require temporary interruption of warfarin for invasive procedures benefit from post-
procedure anticoagulant bridging therapy with low molecular weight heparin.
Objective: To determine the efficacy and safety of dalteparin postoperative bridging therapy
versus placebo for patients with atrial fibrillation or mechanical heart valves when warfarin is
temporarily interrupted for a planned procedure.
Design: Prospective randomized double-blind controlled trial.
Setting: 10 thrombosis research sites in Canada and India.
Participants: 1471 patients with atrial fibrillation or mechanical heart valve who required
temporary interruption of warfarin for a procedure.
Intervention: Random assignment to dalteparin (N=821) or placebo (N=650) post-procedure.
Measurements: Major thromboembolism (stroke or transient ischemic attack, proximal deep vein
thrombosis, pulmonary embolism, myocardial infarction peripheral embolism) or major bleeding
as per ISTH criteria in the 90 days post-procedure.
Results: The rate of major thromboembolism within 90 days was 1.23% (8 events in 650
patients) for placebo and 0.98% (8 events in 820 patients) for dalteparin (p=0.64 risk difference -
0.26% (95% C.I. -1.34 to 0.83)). Major bleeding occurred in 13 (2.00%) patients in the placebo
group and 11 (1.34%) patients on dalteparin (p=0.32, risk difference -0.66 (95% C.I. -1.99-
0.68)). The results were consistent for both the atrial fibrillation and mechanical heart valves
groups.
Limitations: 90-day follow-up.
Page 3 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 4
Conclusions: In patients with atrial fibrillation and/or mechanical valves who had warfarin
interrupted for a procedure there was no significant benefit of post-operative dalteparin bridging
to prevent major thromboembolism.
Primary Funding Source: CIHR (Canadian Institutes of Health Research).
Trial Registration Number: NCT00432796
Page 4 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 5
Introduction
It is uncertain whether patients with atrial fibrillation or mechanical heart valves requiring
interruption of vitamin K antagonists for invasive procedures benefit from post procedure
bridging with low molecular weight heparin (LMWH). [1,2] Many published protocols and
guidelines have sought to address this common clinical problem. [3,4]
In the typical bridging strategy, warfarin is held for 4 or 5 days pre-procedure and is resumed
after the procedure either the same day or 1 or 2 days later and [4,5,6,7] LMWH is given once or
twice a day for 3-5 days pre-procedure and for a minimum of 4 days post-procedure until the
international normalized ratio (INR) is therapeutic. [4,5,6,7] The goal of bridging with LMWH is to
reduce the risk of perioperative thromboembolism by minimizing the time without
anticoagulation, while reducing bleeding risks by using a short-acting anticoagulant allowing for
minimal or no anticoagulant effect at the time of interruption. [8]
Bridging has been most studied in patients with atrial fibrillation in multiple observational or
single armed studies [9]. A recently completed double blind placebo trial which suggested that
LMWH bridging is not necessary pre or post procedure for patients on warfarin [10]. However,
mechanical heart valve patients were usually excluded and patients with atrial fibrillation at high
risk of stroke were not well represented. [4,5,6] In a previous single arm multicenter pilot study of
dalteparin bridging for 224 patients with atrial fibrillation or mechanical heart valves we found
that the post procedure rate of thrombosis was 3.1% with 75% of those events occurring in
patients who had anticoagulation held due to a bleeding event post procedure. [6] This suggested
that post-procedure bridging caused harm potentially due to a more prolonged period off of
anticoagulation due to bleeding which then lead to thrombotic events.
Based on this information we performed a randomized double-blind placebo controlled trial to
Page 5 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 6
assess the necessity of post-operative bridging with the LMWH dalteparin for patients with atrial
fibrillation or prosthetic mechanical valves who required warfarin to be held for a procedure. We
hypothesized that patients who would receive placebo post-procedure would have fewer bleeding
events and thus a lower rate of thromboembolism due to the association of thromboembolism
with bleeding in our pilot study. [6]
Page 6 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 7
Methods
Study Design and Oversight
Periop2 was a randomized double-blind placebo controlled trial. The protocol was designed by
the Steering Committee and approved by the Institutional Review Board at each participating
center. The study was funded by the Canadian Institute of Health Research (CIHR-MCT79607)
and had support from Pfizer in the form of study drug. The trial was registered at
ClinicalTrials.gov (NCT00432796). Pfizer did not have any role in the design or conduct of the
study, analysis of the data, or preparation of the manuscript. Study medication (dalteparin or
placebo) was prepared in each local center by a pharmacist not involved in the subject’s care.
Patients
Patients were eligible to participate in the trial if they were 18 years of age or older and had
either a mechanical heart valve (with or without atrial fibrillation), or atrial fibrillation or atrial
flutter and a CHADS2 risk factor (previous TIA or stroke, high blood pressure, diabetes, age
greater than 75, or moderate/severe left ventricular dysfunction) were receiving long term anti-
coagulation with warfarin and required elective non-cardiac surgery or an invasive procedure in
which the physician requested an absence of warfarin effect. Patients were excluded for any of
the following reasons: active bleeding within 30 days prior to stopping warfarin; platelet count
<100 x10⁹/L; spinal or neurosurgery; life expectancy less than 3 months; calculated creatinine
clearance <30ml/min; multiple mechanical valves or a Starr-Edwards valve, mechanical valve
with history of stroke or TIA, or a history of heparin induced thrombocytopenia. All patients
provided written informed consent.
Procedures
Warfarin was discontinued 5 days before the procedure (day 0), that is, 5 doses were held (see
Figure 1) as in our pilot study [6]. All patients were given dalteparin 200 IU per kilogram
subcutaneously 72 and 48 hours prior to the procedure and 100 IU per kilogram 24 hours prior to
Page 7 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 8
the procedure. The maximum dose of dalteparin was 18000 IU. Warfarin was resumed the
evening of the procedure at twice the usual daily dose for the first day and then according to the
INR result. After the procedure, eligibility was reconfirmed for all patients prior to
randomization which occurred either on day 0 or day +1. Patients were randomized to receive
dalteparin or placebo starting the morning of the day after the procedure at least 12 hours post
procedure. Patients considered at high risk for bleeding (cancer surgery (genitourinary, head and
neck, intra-abdominal, breast), orthopedic joint replacement, kidney or liver biopsy, prostate
resection or biopsy, pacemaker insertion, abdominal hysterectomy, hernia repair or vascular
surgery [see Supplementary Appendix S1]) were given dalteparin 5000 IU or placebo
subcutaneously daily for at least 4 doses and until the INR was greater than 1.9. Patients who
underwent procedures considered at low risk for bleeding (non-cancer abdominal surgery,
cholecystectomy, hemorrhoidectomy, node dissection, vaginal hysterectomy, hand surgery, skin
procedures, non-joint replacement orthopedic surgery (shoulder, foot surgery, arthroscopic
surgery), line insertion, endoscopic biopsies [see Supplementary Appendix S1]) received
dalteparin at 200 IU per kilogram (maximum 18000 IU) subcutaneously or placebo for at least 4
days and until the INR was greater than 1.9. The final determination of high or low bleeding risk
was left to the local investigator and attending physician. For patients on aspirin this was
discontinued 7 days pre-procedure and resumed post-procedure at the site investigator’s
discretion. Patients had daily contact with research staff while on study medication and were
subsequently assessed at one week, 4 weeks, and 90 days post-procedure by telephone.
Study outcomes
Study outcomes were assessed from the time of randomization to 90 days which was the
standard at the time this study started in 2007. The primary efficacy outcome was major
thromboembolism which included any of: ischemic stroke, transient ischemic attack, myocardial
infarction, peripheral arterial embolism, valve thrombosis, vascular death, or symptomatic acute
Page 8 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 9
venous thromboembolism. (Supplementary Appendix) Secondary efficacy endpoints included
the individual major thromboembolism outcomes and a composite outcome of major
thromboembolism, and major bleeding (net clinical benefit). The primary safety outcome was
major bleeding as per International Society on Thrombosis and Haemostasis ISTH criteria
(Supplementary Appendix). The secondary safety outcomes were clinically relevant non-major
bleeding and trivial bleeding (Supplementary Appendix). All study outcomes were
independently and blindly adjudicated by an adjudicating committee that included a thrombosis
expert, neurologist and cardiologist.
Statistical Analysis
The primary efficacy outcome was major thromboembolism in the 90 days post-procedure. From
our pilot study (that used the same inclusion/exclusion criteria) we expected 3.1% of patients in
the control arm to have major thromboembolism (post-procedure bridging) [6]. The minimum
clinically important difference was a 2% absolute difference. That is, if there were 2 more
thromboembolic events per 100 patients in one arm compared to the other it would be considered
clinically meaningful. The 2% difference in event rates would translate into a mortality
difference of 0.3% at 90 days assuming that 15% of thromboembolic events were fatal [1,11]. The
null hypothesis was that the experimental intervention (no post-operative bridging) would have
the same primary outcome event rate. We accepted a 5% chance of falsely rejecting the null
hypothesis (i.e. two tailed alpha = 0.05) and a 20% chance of falsely not rejecting the hypothesis
(i.e. power = 80%). To achieve these standards we required a sample size (2N) of 1612. In our
previous study, 8% of patients did not receive the intended therapy (non-compliance, withdrawal
or lost to follow-up) [6] and so to be conservative we assumed that an additional 2% would be lost
to follow-up. Consequently, the sample size was increased by 10% to 1773. The study was
stopped early due to funding limitations and declining enrollment due to the widespread use of
direct oral anticoagulants rather than warfarin for atrial fibrillation.
Page 9 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 10
Data were analyzed by intention to treat. Patients who were lost to follow up were censored from
the time of their last known follow up. The proportion of patients experiencing a primary
outcome event was compared in the placebo and dalteparin groups by an unadjusted Fisher’s
exact test of proportions. A priori we planned to analyze primary and secondary outcomes in the
subgroups prosthetic valves with or without atrial fibrillation and atrial fibrillation only. Two
interim analyses (at 33% and 66% enrollment) were planned.
Results
Patients
As shown in Figure 2 1677 patients provided informed consent between February 2007 – March
2016 at 10 sites in Canada and India. Subsequently 1471 patients were randomized post-
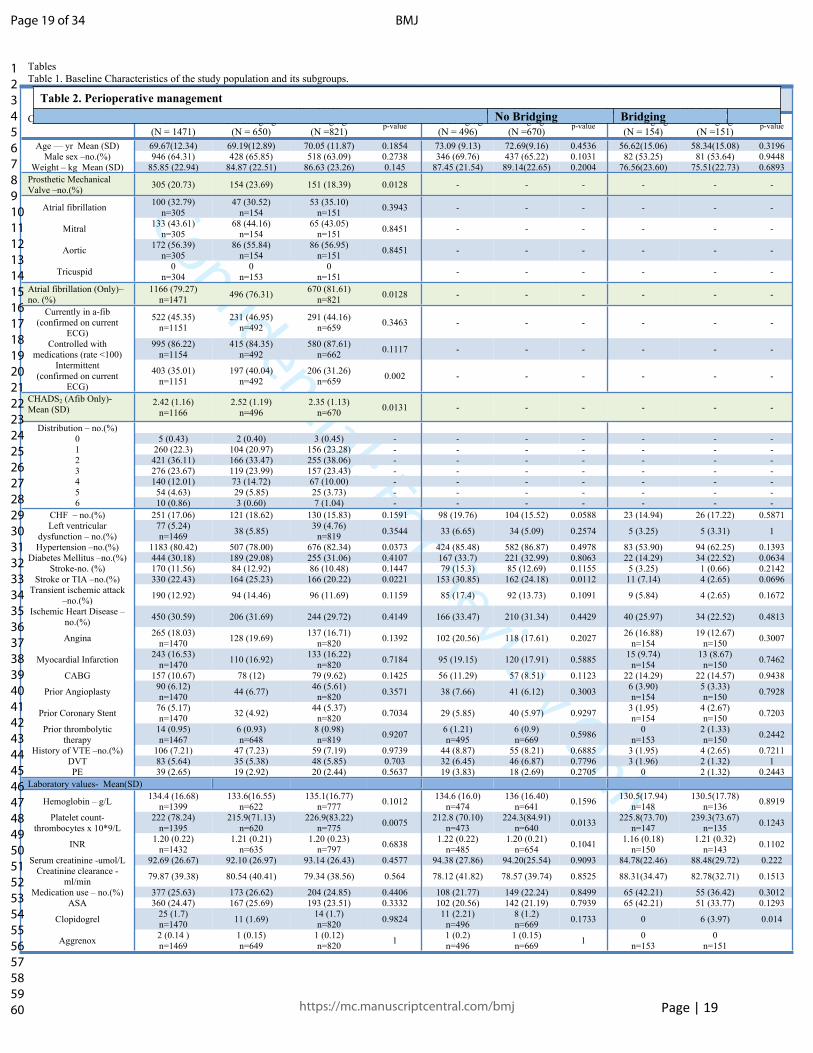
procedure, 821 to dalteparin and 650 to placebo. Baseline patient characteristics were well
balanced (Table 1). The mean age was 69.7 years, 64.3% were male, 79.3% had atrial fibrillation
and 20.7% had mechanical valves (32.8% of the mechanical valve patients also had atrial
fibrillation). One patient with a mechanical valve assigned to dalteparin withdrew their consent
immediately after randomization before receiving study medication. The average CHADS2 score
was 2.42 and 41.2% had a score of 3.0 or higher. ASA was being taken by 24.5% of patients
while 1.7% of patients took other anti-platelet agents. There were a wide range of procedures.
[Supplementary Appendix S2]
At the time of the first scheduled interim analysis it was discovered by the DSMB that there was
an imbalance in randomization. This was due to a programming error that lead to all patients
within the atrial fibrillation and low post-procedure bleeding risk stratum being assigned to post-
procedure dalteparin at the two sites that also were leading in recruitment. After review with the
DSMB, our study methodologists and independent international experts, to correct for this
randomization imbalance the randomization program was amended at these two sites only in that
stratum to subsequently allocate 80% of patients to placebo and 20% to dalteparin in order to
maintain the blind. The investigators were aware that there was an imbalance but remained
Page 10 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 11
blinded to its magnitude and direction.
Post-procedure anticoagulant management
As shown in Table 2, 9 of 650 patients assigned to placebo and 14 of 821 patients assigned to
dalteparin did not receive post-procedure dosing. The mean number of post-procedure doses for
placebo and dalteparin were 5.56 and 5.37. The 287 low bleeding risk patients assigned to
dalteparin had a mean dose of 15256.0 IU per day. The 520 high bleeding risk patients assigned
to dalteparin had a mean dose of 5024.2 IU per day.
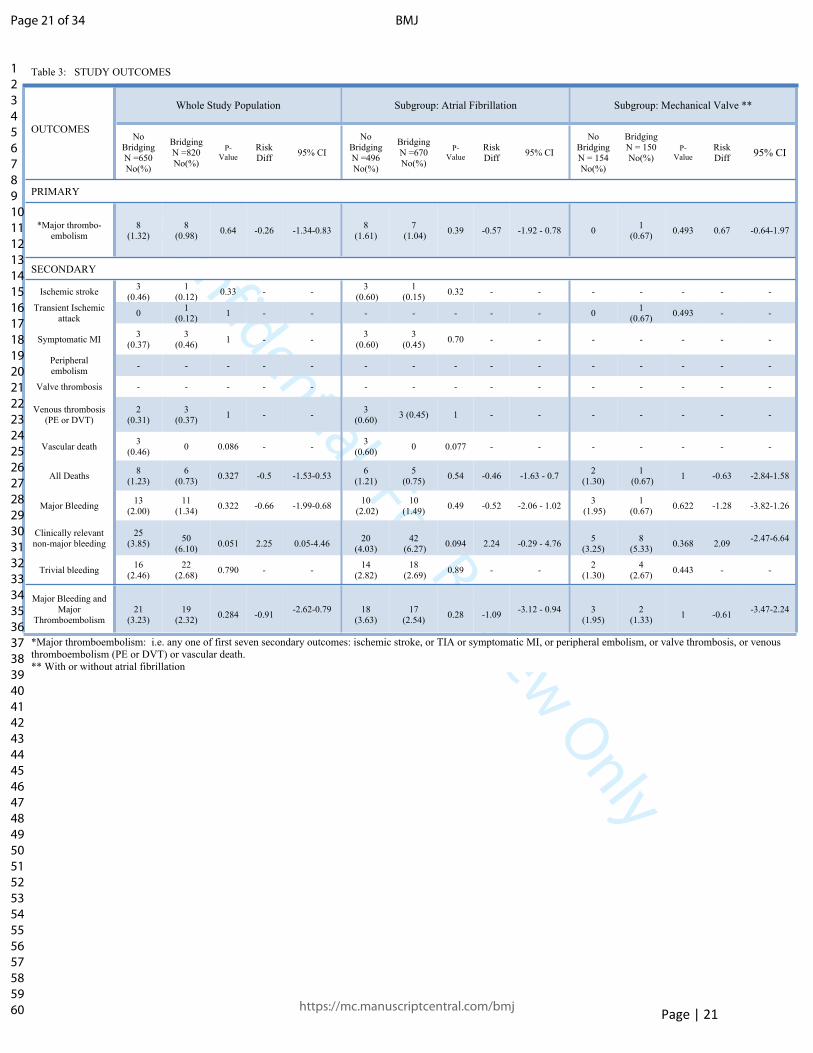
Study Outcomes
As shown in Table 3, the rate of major thromboembolism at 90 days was 1.23% (8 events in 650
patients) for placebo and 0.98% (8 events in 820 patients) for dalteparin (p=0.64 risk difference -
0.26% [95% C.I. interval -1.34 to 0.83]). Major bleeding occurred in 13 (2.00%) patients
assigned to placebo compared to 11 (1.34%) assigned to dalteparin (p=0.32, risk difference -0.66
[95% C.I. -1.99-0.68]).
For the pre-specified secondary end point combining major bleeding and major
thromboembolism there were 21 (3.23%) events in patients assigned to placebo compared to 19
(2.32%) events in patients assigned to dalteparin (p=0.29 risk difference -0.91 [95% C.I. -2.62 –
0.79]). There were no differences for any of the additional secondary outcomes.
In the pre-specified subgroup analyses according to indication for anticoagulation, there were no
significant differences for any of the outcomes among the subgroups of atrial fibrillation and
mechanical valves. Only 1 patient in the mechanical valve group had a major thromboembolism,
and that patient was in the dalteparin arm.
Page 11 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review Only
Page | 12
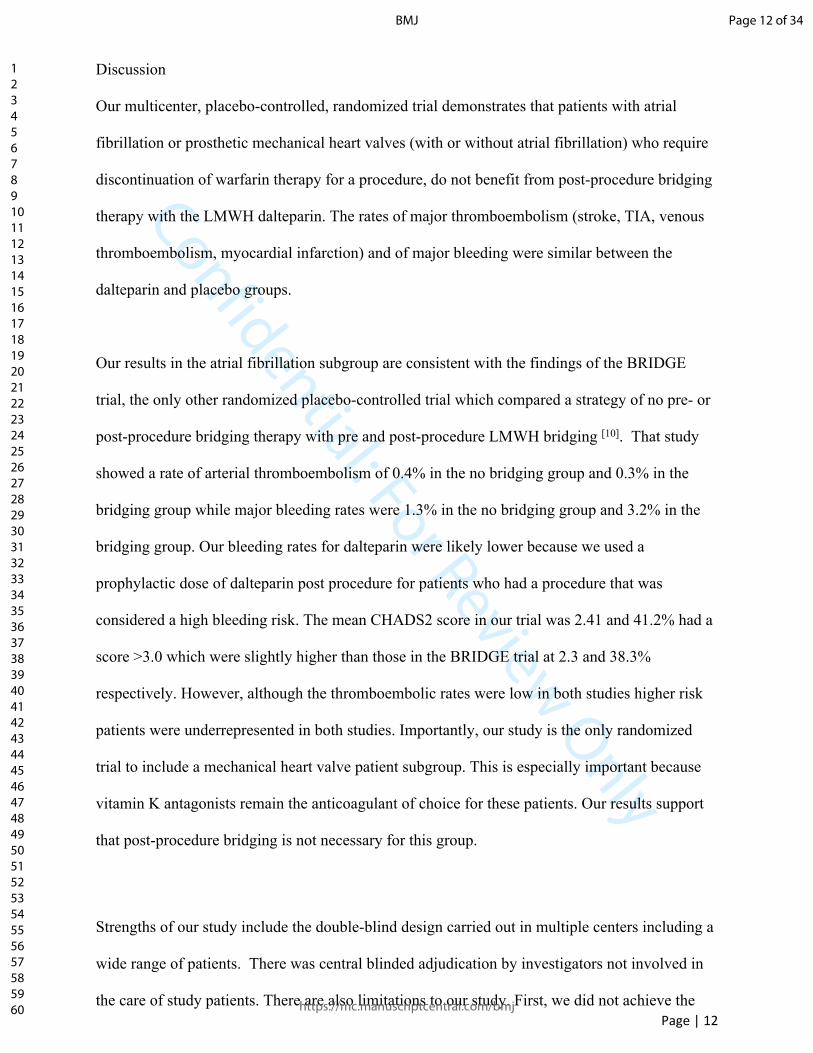
Discussion
Our multicenter, placebo-controlled, randomized trial demonstrates that patients with atrial
fibrillation or prosthetic mechanical heart valves (with or without atrial fibrillation) who require
discontinuation of warfarin therapy for a procedure, do not benefit from post-procedure bridging
therapy with the LMWH dalteparin. The rates of major thromboembolism (stroke, TIA, venous
thromboembolism, myocardial infarction) and of major bleeding were similar between the
dalteparin and placebo groups.
Our results in the atrial fibrillation subgroup are consistent with the findings of the BRIDGE
trial, the only other randomized placebo-controlled trial which compared a strategy of no pre- or
post-procedure bridging therapy with pre and post-procedure LMWH bridging [10]. That study
showed a rate of arterial thromboembolism of 0.4% in the no bridging group and 0.3% in the
bridging group while major bleeding rates were 1.3% in the no bridging group and 3.2% in the
bridging group. Our bleeding rates for dalteparin were likely lower because we used a
prophylactic dose of dalteparin post procedure for patients who had a procedure that was
considered a high bleeding risk. The mean CHADS2 score in our trial was 2.41 and 41.2% had a
score >3.0 which were slightly higher than those in the BRIDGE trial at 2.3 and 38.3%
respectively. However, although the thromboembolic rates were low in both studies higher risk
patients were underrepresented in both studies. Importantly, our study is the only randomized
trial to include a mechanical heart valve patient subgroup. This is especially important because
vitamin K antagonists remain the anticoagulant of choice for these patients. Our results support
that post-procedure bridging is not necessary for this group.
Strengths of our study include the double-blind design carried out in multiple centers including a
wide range of patients. There was central blinded adjudication by investigators not involved in
the care of study patients. There are also limitations to our study. First, we did not achieve the
Page 12 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 13
full sample size due to the decreased availability of patients with atrial fibrillation on warfarin
because of the introduction of direct oral anticoagulant therapy [4]. Second, the total number of
patients with mechanical heart valves was relatively low, although to our knowledge this is the
largest population and the only randomized trial in this group of patients to date. Also, the rate of
major thromboembolism in this subgroup was very low with only 1 event and that patient was in
the bridging arm. Further randomized studies in this group would be ideal however are likely to
be logistically difficult as was our experience. Third, all of our patients had pre-procedure
bridging with dalteparin. Given the results of the BRIDGE trial pre-procedure LMWH bridging
for atrial fibrillation patients is likely not necessary [10]. Moreover, a recent trial strongly suggests
that pre and post procedure bridging therapy is not necessary for patients receiving direct oral
anticoagulants for atrial fibrillation [12]. We cannot make any conclusions about pre-procedure
bridging for mechanical heart valves and high-risk AF from our study given that all patients
received it, thus this requires further study. Finally, given that we excluded mechanical heart
valve patients with a history of stroke or TIA, or those with multiple mechanical valves, results
from this study should not be applied to those patients.
In conclusion, for patients with atrial fibrillation or mechanical heart valves (with or without
atrial fibrillation) who are managed with warfarin, post-procedure bridging with dalteparin is not
beneficial in preventing major thromboembolism. We did not find a difference in major bleeding
between groups with our protocol. Although warfarin is being used less frequently in patients
with atrial fibrillation, it is still the long-term anticoagulant of choice for patients with
mechanical heart valves and in other populations such as dialysis patients, those with limited
drug coverage for DOACs and resource constrained settings. Our results are important for those
patients. Further studies to determine the need for pre-procedure bridging for patients with
mechanical heart valves are necessary.
Page 13 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 14
Acknowledgements. The authors wish to dedicate this work in memory of Drs. Clive Kearon,
Linda Vickars and Susan Solymoss, accomplished researchers and dear friends.
Susan Kahn holds a Tier 1 Canada Research Chair in venous thromboembolism. Shannon M
Bates holds the Eli Lilly Canada/May Cohen Chair in Women’s Health at McMaster University.
Michael J. Kovacs, Philip S. Wells P, David R Anderson, Alejandro Lazo-Langner, Clive
Kearon, Shannon M. Bates, Mark Blostein, Susan R. Kahn, Sam Schulman, Susan Solymoss,
Tim Ramsay, Erik Yeo, and Marc A. Rodger are investigators of the CanVECTOR Network; the
Network receives grant funding from the Canadian Institutes of Health Research (CDT-142654).
Page 14 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 15
References
1. Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med 1997; 336(21):1506-1511
2. Baron TH, Kamath PS, McBane RD. Management of antithrombotic therapy in patients undergoing invasive procedures. N Engl J Med 2013;368:2113-24.
3. Douketis JD, Spyropoulos AC, Spence FA, et al. Perioperative management of antithrombotic therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. [published correction appears in Chest. 2012;141(4):1129]. Chest. 2012;141(2)(suppl):e326S-e350S.doi:10.1778/chest.11-2298
4. Spyropoulos AC, Al-Badri A, Sherwood MW, et al. Periprocedural management of patients receiving a vitamin k antagonist or a direct oral anticoagulant requiring an elective procedure or surgery. J Thromb Haemost. 2016;14(5):875-885. doi:10.1111/jth.13305
5. Dunn AS, Spyropoulos AC, Turpie AG. Bridging therapy in patients on long-term oral anticoagulants who require surgery: The Prospective Peri-operative Enoxaparin Cohort Trial (PROSPECT). J Thromb Haemost. 2007;5(11):2211-2218. doi:10.111/j.1538-7836.2007.02729.x
6. Kovacs MJ, Kearon C, Rodger M, et.al. A Single Arm Study of Bridging Therapy with Low Molecular Weight Heparin for Patients at Risk for Arterial Embolism Who Require Temporary Interruption of Warfarin. Circulation 2004;110:1658-1663.
7. Douketis JD, Johnson JA, Turpie AG. Low-molecular-weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen. Arch Intern Med 2004;164:1319-26.
8. Spyropoulos AC, Douketis JD, Gerotziafas G, et al. Subcommittee on Control of Anticoagulation of the SSC of the ISTH. Periprocedural antithrombotic and bridging therapy: recommendations for standardized reporting in patients with arterial indications for chronic oral anticoagulant therapy. J Thromb Haemost. 2012;10(4):692-694. doi:10.1111/j.1538-7836.2012.04630.x
9. Siegal D, Yudin J, Kaatz S, et al. Periprocedural heparin bridging in patients receiving vitamin K antagonists: systematic review and meta-analysis of bleeding and thromboembolic rates. Circulation. 2012 Sep 25;126(13):1630-9. Doi: 10.1161/CIRCULATIONAHA.112.105221.
10. Douketis JD, Spyropoulos AC, Kaatz S, et al: BRIDGE Investigators. Perioperative bridging anticoagulation in patients with atrial fibrillation. N Engl J Med.
Page 15 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 16
2015;373(9):823-833. doi:10.1056/NEJMoa1501035
11. Rodger M, Bredseon C, Wells PS, et al. Cost-effectiveness of low-molecular-weight heparin and unfractionated heparin in treatment of deep vein thrombosis. CMAJ 1998; 159(8):931-938.
12. Douketis JD, Spyropoulos AC, Duncan J, et al. Perioperative management of patient with atrial fibrillation receiving a direct oral anticoagulant. JAMA Intern Med. 2019;179(11):1469-1478. Doi:10.1001/jamaintermed.2019.2431
Page 16 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 17
Figures
Figure 1
Page 17 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 18
Figure 2
Page 18 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review Only
Page | 19
TablesTable 1. Baseline Characteristics of the study population and its subgroups.
Whole Study Population(N = 1471)
Atrial Fibrillation (AFIB)(N= 1166)
Mechanical Valve ±AFIB(N=305)
Characteristics Total(N = 1471)
No Bridging(N = 650)
Bridging(N =821) p-value No Bridging
(N = 496)Bridging(N =670) p-value No Bridging
(N = 154)Bridging(N =151) p-value
Age — yr Mean (SD) 69.67(12.34) 69.19(12.89) 70.05 (11.87) 0.1854 73.09 (9.13) 72.69(9.16) 0.4536 56.62(15.06) 58.34(15.08) 0.3196Male sex –no.(%) 946 (64.31) 428 (65.85) 518 (63.09) 0.2738 346 (69.76) 437 (65.22) 0.1031 82 (53.25) 81 (53.64) 0.9448
Weight – kg Mean (SD) 85.85 (22.94) 84.87 (22.51) 86.63 (23.26) 0.145 87.45 (21.54) 89.14(22.65) 0.2004 76.56(23.60) 75.51(22.73) 0.6893Prosthetic Mechanical Valve –no.(%) 305 (20.73) 154 (23.69) 151 (18.39) 0.0128 - - - - - -
Atrial fibrillation 100 (32.79) n=305
47 (30.52) n=154
53 (35.10) n=151 0.3943 - - - - - -
Mitral 133 (43.61) n=305
68 (44.16) n=154
65 (43.05) n=151 0.8451 - - - - - -
Aortic 172 (56.39) n=305
86 (55.84) n=154
86 (56.95) n=151 0.8451 - - - - - -
Tricuspid 0 n=304
0n=153
0n=151 - - - - - -
Atrial fibrillation (Only)– no. (%)
1166 (79.27) n=1471 496 (76.31) 670 (81.61)
n=821 0.0128 - - - - - -
Currently in a-fib (confirmed on current
ECG)
522 (45.35) n=1151
231 (46.95) n=492
291 (44.16) n=659 0.3463 - - - - - -
Controlled with medications (rate <100)
995 (86.22) n=1154
415 (84.35) n=492
580 (87.61) n=662 0.1117 - - - - - -
Intermittent (confirmed on current
ECG)
403 (35.01) n=1151
197 (40.04) n=492
206 (31.26) n=659 0.002 - - - - - -
CHADS2 (Afib Only)- Mean (SD)
2.42 (1.16) n=1166
2.52 (1.19) n=496
2.35 (1.13) n=670 0.0131 - - - - - -
Distribution – no.(%)0 5 (0.43) 2 (0.40) 3 (0.45) - - - - - - -1 260 (22.3) 104 (20.97) 156 (23.28) - - - - - - -2 421 (36.11) 166 (33.47) 255 (38.06) - - - - - - -3 276 (23.67) 119 (23.99) 157 (23.43) - - - - - - -4 140 (12.01) 73 (14.72) 67 (10.00) - - - - - - -5 54 (4.63) 29 (5.85) 25 (3.73) - - - - - - -6 10 (0.86) 3 (0.60) 7 (1.04) - - - - - - -
CHF – no.(%) 251 (17.06) 121 (18.62) 130 (15.83) 0.1591 98 (19.76) 104 (15.52) 0.0588 23 (14.94) 26 (17.22) 0.5871Left ventricular
dysfunction – no.(%)77 (5.24) n=1469 38 (5.85) 39 (4.76)
n=819 0.3544 33 (6.65) 34 (5.09) 0.2574 5 (3.25) 5 (3.31) 1
Hypertension –no.(%) 1183 (80.42) 507 (78.00) 676 (82.34) 0.0373 424 (85.48) 582 (86.87) 0.4978 83 (53.90) 94 (62.25) 0.1393Diabetes Mellitus –no.(%) 444 (30.18) 189 (29.08) 255 (31.06) 0.4107 167 (33.7) 221 (32.99) 0.8063 22 (14.29) 34 (22.52) 0.0634
Stroke-no. (%) 170 (11.56) 84 (12.92) 86 (10.48) 0.1447 79 (15.3) 85 (12.69) 0.1155 5 (3.25) 1 (0.66) 0.2142Stroke or TIA –no.(%) 330 (22.43) 164 (25.23) 166 (20.22) 0.0221 153 (30.85) 162 (24.18) 0.0112 11 (7.14) 4 (2.65) 0.0696
Transient ischemic attack –no.(%) 190 (12.92) 94 (14.46) 96 (11.69) 0.1159 85 (17.4) 92 (13.73) 0.1091 9 (5.84) 4 (2.65) 0.1672
Ischemic Heart Disease –no.(%) 450 (30.59) 206 (31.69) 244 (29.72) 0.4149 166 (33.47) 210 (31.34) 0.4429 40 (25.97) 34 (22.52) 0.4813
Angina 265 (18.03) n=1470 128 (19.69) 137 (16.71)
n=820 0.1392 102 (20.56) 118 (17.61) 0.2027 26 (16.88)n=154
19 (12.67) n=150 0.3007
Myocardial Infarction 243 (16.53) n=1470 110 (16.92) 133 (16.22)
n=820 0.7184 95 (19.15) 120 (17.91) 0.5885 15 (9.74)n=154
13 (8.67) n=150 0.7462
CABG 157 (10.67) 78 (12) 79 (9.62) 0.1425 56 (11.29) 57 (8.51) 0.1123 22 (14.29) 22 (14.57) 0.9438
Prior Angioplasty 90 (6.12) n=1470 44 (6.77) 46 (5.61)
n=820 0.3571 38 (7.66) 41 (6.12) 0.3003 6 (3.90)n=154
5 (3.33) n=150 0.7928
Prior Coronary Stent 76 (5.17) n=1470 32 (4.92) 44 (5.37)
n=820 0.7034 29 (5.85) 40 (5.97) 0.9297 3 (1.95)n=154
4 (2.67) n=150 0.7203
Prior thrombolytic therapy
14 (0.95) n=1467
6 (0.93) n=648
8 (0.98) n=819 0.9207 6 (1.21)
n=4956 (0.9) n=669 0.5986 0
n=1532 (1.33) n=150 0.2442
History of VTE –no.(%) 106 (7.21) 47 (7.23) 59 (7.19) 0.9739 44 (8.87) 55 (8.21) 0.6885 3 (1.95) 4 (2.65) 0.7211DVT 83 (5.64) 35 (5.38) 48 (5.85) 0.703 32 (6.45) 46 (6.87) 0.7796 3 (1.96) 2 (1.32) 1PE 39 (2.65) 19 (2.92) 20 (2.44) 0.5637 19 (3.83) 18 (2.69) 0.2705 0 2 (1.32) 0.2443
Laboratory values- Mean(SD)
Hemoglobin – g/L 134.4 (16.68) n=1399
133.6(16.55) n=622
135.1(16.77) n=777 0.1012 134.6 (16.0)
n=474136 (16.40)
n=641 0.1596 130.5(17.94) n=148
130.5(17.78) n=136 0.8919
Platelet count-thrombocytes x 10*9/L
222 (78.24) n=1395
215.9(71.13) n=620
226.9(83.22) n=775 0.0075 212.8 (70.10)
n=473224.3(84.91)
n=640 0.0133 225.8(73.70) n=147
239.3(73.67) n=135 0.1243
INR 1.20 (0.22) n=1432
1.21 (0.21) n=635
1.20 (0.23) n=797 0.6838 1.22 (0.22)
n=4851.20 (0.21)
n=654 0.1041 1.16 (0.18) n=150
1.21 (0.32) n=143 0.1102
Serum creatinine -umol/L 92.69 (26.67) 92.10 (26.97) 93.14 (26.43) 0.4577 94.38 (27.86) 94.20(25.54) 0.9093 84.78(22.46) 88.48(29.72) 0.222Creatinine clearance -
ml/min 79.87 (39.38) 80.54 (40.41) 79.34 (38.56) 0.564 78.12 (41.82) 78.57 (39.74) 0.8525 88.31(34.47) 82.78(32.71) 0.1513
Medication use – no.(%) 377 (25.63) 173 (26.62) 204 (24.85) 0.4406 108 (21.77) 149 (22.24) 0.8499 65 (42.21) 55 (36.42) 0.3012ASA 360 (24.47) 167 (25.69) 193 (23.51) 0.3332 102 (20.56) 142 (21.19) 0.7939 65 (42.21) 51 (33.77) 0.1293
Clopidogrel 25 (1.7) n=1470 11 (1.69) 14 (1.7)
n=820 0.9824 11 (2.21)n=496
8 (1.2) n=669 0.1733 0 6 (3.97) 0.014
Aggrenox 2 (0.14 ) n=1469
1 (0.15) n=649
1 (0.12) n=820 1 1 (0.2)
n=4961 (0.15) n=669 1 0
n=1530
n=151
Table 2. Perioperative management No Bridging Bridging
Page 19 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 20
Variable (N =650) (N =821) P ValueWarfarin treatment
Pre-procedure time not taking warfarin No. of patients with data 650 821 No. of days, Mean (SD) 5.13 (0.66) 5.11 (0.55) 0.6095Pre-procedure INR INR > 1.7 (Day -1)-no.(%) 11 (1.70) n=648 9 (1.10) n=817 0.3289Vitamin K 2 mg given -no.(%) 7 (1.08) n=650 7 (0.85) n=819 0.6633INR 1.5 - 1.7 (Day -1)-no.(%) 34 (5.25) n=648 43 (5.26) n=817 0.989Vitamin K 1 mg given -no.(%) 32 (4.92) n=650 42 (5.13) n=819 0.8583Different dose of Vitamin K given (Day-1)-no.(%) 5 (0.77) n=650 2 (0.24) n=818 0.252INR repeated on the day of procedure (Day 0)-no.(%) 131 (20.15) 128 (15.59) 0.0225
Post-procedure dose No. of patients for whom warfarin was resumed 645 (99.23) 814 (99.15) 0.8598
No. of patients for whom warfarin was resumed on post-op day (Day 0) 564/645 (87.44) 752/814 (92.38)No. of patients for whom warfarin was resumed the next post-op day (Day ≥1) 81/645 (12.56) 62/814 (7.62) 0.0016
Mean no. dose (for patients resumed on Day 0) 8.68 (3.54) n=564 8.62 (3.80) n=752 0.7678Mean no. dose (for patients resumed on Day ≥1) 7.51 (2.94) n=81 7.84 (2.79) n=62 0.4946
Low-molecular-weight heparin or placebo Pre-procedure dose
No. of patients with data 648 819 Average dose received over the three days- Mean (SD) 13508.95 (4896.02) 13484.27 (4136.75) 0.9183Receive LMWH dose Day -3 no. (%) 640 814 Dose for Day -3, Mean (SD) 16288.90 (10026.09) 15979.85 (6361.39) 0.4968Receive LMWH dose Day -2 no. (%) 646 815 Dose for Day -2, Mean (SD) 15919.90 (7471.38) 16028.91 (8076.44) 0.7894Receive LMWH dose Day -1 no. (%) 643 817 Dose for Day -1, Mean (SD) 8342.88 (2211.01) 8458.54 (4088.84) 0.4901Post-OP LMWH, N (%) Patients who started LMWH post op on Day +1 630 (96.92) 789 (96.10)Patients who started LMWH post op on day +2 or later 11 (1.69) 18 (2.19)Patients who did not receive LMWH 9 (1.38) 14 (1.71)
0.6962
Post-procedure dose No. of patients with dose given 641 807 No. of doses, Mean (SD) 5.56 (2.11) 5.37 (1.96) 0.0819Average Dose per day, Mean (SD) 9523.51 (5479.98) 8663.02 (5271.28) 0.0025No. of patients when LMWH started post-op Day +1 630 789 No. of doses when LMWH started post-op Day +1, Mean (SD) 5.57 (2.11) 5.38 (1.94) 0.0778Average dose per day when LMWH started post-op Day +1, Mean (SD) 9433.13 (5462.90) 8688.34 (5277.13) 0.0094No. of patients when LMWH started post-op Day ≥ 2 11 18 No. of doses when LMWH started post op Day ≥ 2, Mean (SD) 4.91 (1.70) 5.11 (2.85) 0.8334Average dose per day when LMWH started post op Day ≥ 2, Mean (SD) 14700.00 (3755.38) 7553.33 (5022.53) 0.0004
Low Risk patients who received post-op LMWH dose 284 287 No. of doses- Low bleeding risk, Mean (SD) 5.52 (1.99) 5.49 (2.15) 0.8399Average dose per day- Low bleeding risk, Mean (SD) 15142.15 (3223.94) 15255.99 (3166.79) 0.6012Patients had >5000 per day, N (%) (Fisher’s Exact Test) 281 (98.60) 283 (98.61) 1
High Risk patients who received post-op LMWH dose 356 520 No. of doses- High bleeding risk, Mean (SD) 5.54 (2.19) 5.31 (1.85) 0.0494Average dose per day- High bleeding risk, Mean (SD) 5046.64 (684.82) 5024.21 (567.77) 0.6106Patients had >5000 per day, N (%) (Fisher’s Exact Test) 2 (0.56) 3 (0.58) 1Aspirin treatment – no./total no.(%) 167 (25.69) 193 (23.51) 0.3332Anti-platelet medication 173 (26.62) 204 (24.85) 0.4406No. of patients have stop day reported for anti-platelet medication 149 190 Interruption ≥ 7 days before procedure 122 (81.88) 163 (85.79)Interruption < 7 days before procedure 27 (18.12) 27 (14.21) 0.3288
ASA Restarted post procedure 123 (86.01) n=143 150 (85.23) n=176 0.8423Total days until ASA resumed, Mean (SD) 9.08 (2.86) n=123 10.13 (5.69) n=150 0.049
Page 20 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review Only
Page | 21
Table 3: STUDY OUTCOMES
Whole Study Population Subgroup: Atrial Fibrillation Subgroup: Mechanical Valve **
OUTCOMESNo
BridgingN =650No(%)
BridgingN =820No(%)
P-Value
Risk Diff 95% CI
No BridgingN =496No(%)
BridgingN =670No(%)
P-Value
Risk Diff 95% CI
No BridgingN = 154No(%)
BridgingN = 150No(%)
P-Value
Risk Diff 95% CI
PRIMARY
*Major thrombo-embolism
8 (1.32)
8(0.98) 0.64 -0.26 -1.34-0.83 8
(1.61)7
(1.04) 0.39 -0.57 -1.92 - 0.78 0 1 (0.67) 0.493 0.67 -0.64-1.97
SECONDARY
Ischemic stroke 3 (0.46)
1(0.12) 0.33 - - 3
(0.60)1
(0.15) 0.32 - - - - - - -
Transient Ischemic attack 0 1
(0.12) 1 - - - - - - - 0 1 (0.67) 0.493 - -
Symptomatic MI 3 (0.37)
3(0.46) 1 - - 3
(0.60)3
(0.45) 0.70 - - - - - - -
Peripheral embolism - - - - - - - - - - - - - - -
Valve thrombosis - - - - - - - - - - - - - - -
Venous thrombosis (PE or DVT)
2 (0.31)
3(0.37) 1 - - 3
(0.60) 3 (0.45) 1 - - - - - - -
Vascular death 3(0.46) 0 0.086 - - 3
(0.60) 0 0.077 - - - - - - -
All Deaths 8 (1.23)
6(0.73) 0.327 -0.5 -1.53-0.53 6
(1.21)5
(0.75) 0.54 -0.46 -1.63 - 0.7 2 (1.30)
1 (0.67) 1 -0.63 -2.84-1.58
Major Bleeding 13 (2.00)
11(1.34) 0.322 -0.66 -1.99-0.68 10
(2.02)10
(1.49) 0.49 -0.52 -2.06 - 1.02 3 (1.95)
1 (0.67) 0.622 -1.28 -3.82-1.26
Clinically relevant non-major bleeding
25 (3.85) 50
(6.10) 0.051 2.25 0.05-4.46 20 (4.03)
42 (6.27) 0.094 2.24 -0.29 - 4.76 5
(3.25)8
(5.33) 0.368 2.09 -2.47-6.64
Trivial bleeding 16 (2.46)
22 (2.68) 0.790 - - 14
(2.82)18
(2.69) 0.89 - - 2 (1.30)
4 (2.67) 0.443 - -
Major Bleeding and Major
Thromboembolism21
(3.23)19
(2.32) 0.284 -0.91 -2.62-0.79 18 (3.63)
17 (2.54) 0.28 -1.09 -3.12 - 0.94 3
(1.95)2
(1.33) 1 -0.61 -3.47-2.24
*Major thromboembolism: i.e. any one of first seven secondary outcomes: ischemic stroke, or TIA or symptomatic MI, or peripheral embolism, or valve thrombosis, or venous thromboembolism (PE or DVT) or vascular death.** With or without atrial fibrillation
Page 21 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 22
SUPPLEMENTARY APPENDIX
This appendix has been provided by the authors to give readers additional information about their work.
Page 22 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 23
Inclusion/Exclusion Criteria
Inclusion/Exclusion Criteria
Inclusion Criteria
Informed consent, Patients aged >18 Patients with a prosthetic mechanical heart valve
or Patients with atrial fibrillation or atrial flutter and a major risk factor (previous TIA or
stroke, high blood pressure, diabetes, aged >75, moderate/severe left ventricle dysfunction)
Who are receiving long-term oral anticoagulation and require elective non-cardiac surgery or an invasive procedure with reversal of their anticoagulant therapy.
Exclusion Criteria
Evidence of active bleeding within last 30 days prior to stopping warfarin. Platelet count <100 x 109/L. Spinal or neurosurgery. Life expectancy less than 3 months. Calculated creatinine clearance <30 ml/min Patients requiring cardiac surgery. Multiple prosthetic (mechanical)valves or Starr-Edwards valve or
prosthetic(mechanical) valve with a history of stroke or TIA History of heparin induced thrombocytopenia (HIT)
Page 23 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 24
Primary Efficacy Endpoint
Primary Efficacy Endpoint
Description of the Endpoint Characteristics
Ischemic Stroke Sudden onset of a neurological deficit that persists for more than 24 hours and involves one or more of the following: Hemiparesis: involving the face, arm and/or leg unilaterally Hemisensory loss; involving face, arm and/or leg unilaterally Speech impairment; (i.e. Aphasia) Visuo-spatial impairment Visual loss (monocular or binocular) Two or more of the following symptoms which suggest
vertebrobasilar involvement:o (a) incoordination/ataxia, o (b) cranial nerve abnormality, o (c) dysarthria,o (d) dysphagia, o (e) vertigo, o (f) reduction/loss of consciousness, o (g) diplopia
Objective and persistent (more than one week) worsening of a previous deficit or worsening associated with an appropriate new finding on CT scan or MRI.
Transient Ischemic Attack (TIA)
A transient ischemic attack is defined for the purposes of this trial as a sudden onset of a neurological deficit lasting at least one minute but less than 24 hours. Isolated syncope was not considered a TIA unless this occurs with one or more of the following neurological symptoms suggesting vertebrobasilar involvement. Hemiparesis; involving face, arm and/or leg unilaterally Hemisensory loss; involving face, arm and/or leg unilaterally Speech impairment; (i.e. Aphasia) Visuo-spatial impairment Visual Loss (monocular or binocular) Two or more of the following symptoms:
o Incoordination/ataxia, o Cranial nerve abnormality, o Dysarthria, o Dysphasia,o Vertigo, o Reduction/loss of consciousness, o Diplopia
Myocardial Infarction At least two of:i) Ischemic chest pain,ii) EKG changes compatible with a MI (hyperacute T wave, elevated ST segment,
T wave inversion, presence of new bundle branch block, loss of R wave height, development of Q waves) OR
iii) elevation of cardiac enzymes (troponin, CK, CKMB isoenzyme, or other cardiac enzymes) to at least 2X the upper limit of the normal reference range or 3X the upper limit of normal within 48 hours after percutaneous coronary intervention (or if markers are already elevated, greater than 50% of the lowest recovery level from the index infarction
Peripheral embolism The occurrence of acute ischaemia documented by angiography or at surgical removal.
Page 24 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 25
Valve Thrombosis Thrombus deposition on the valve resulting in valve dysfunction requiring reoperation or thrombolytic therapy.
Vascular Death Cardiac, cerebrovascular death excluding subarachnoid or primary intracranial haemorrhage or fatal pulmonary embolism.
Venous Thromboembolism Symptomatic deep vein thrombosis or pulmonary embolism confirmed objectively by any of compression ultrasound, ascending venogram, ventilation/perfusion lung scan, spiral CT or pulmonary angiogram.
Primary outcome events were ascertained from the time of randomisation to 90 days. The time of randomization coincided with the time of administration of the first post-operative dose of study drug (+/- 1 hour). All thromboembolic events from the time of randomisation to 90 days were similarly ascertained. All outcome events were blindly and independently adjudicated by an adjudication committee (a cardiologist, a neurologist and a specialist in thromboembolism).
Page 25 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 26
Primary Bleeding Endpoint
The primary bleeding endpoint is major bleeding, defined by one or more of the events defined by the International Society on Thrombosis and Hemostasis.
Primary Bleeding Endpoint
Major Bleeding: All major bleed must be clinically overt and satisfies one of the following criteria: a fall in hemoglobin of 20g/L within a 24-hour period; results in transfusion of 2 units of blood within a 24-hour period; Death One of the following sites (see below)Clinically overt bleeding at a critical anatomic site Intracranial Intraspinal Intraocular Retroperitoneal, Pericardial
Fatal bleeding Bleeding that directly contributes to death (e.g. intracranial bleed) or causes clinical
deterioration leading to death (e.g. bleed associated with major organ failure or sepsis)Note: Bleeding that was asymptomatic, such as a small retroperitoneal bleed identified as an incidental
finding on computed tomography, would not qualify as a major bleed Intra-operative bleeding that is expected due to the type of surgical procedure and requires blood
transfusion of ≥ 2 units of packed red blood cells would not qualify as a major bleed
Page 26 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 27
Secondary Bleeding Endpoint
Clinically Relevant Non-Major Bleeding is defined as overt bleeding that does not meet the
criteria for major bleeding but is associated with medical intervention, unscheduled contact (visit
or telephone call) with a physician, (temporary) cessation of study treatment, or associated with
any other discomfort such as pain, or impairment of activities of daily life. Examples of this
category of bleeding are; 1) epistaxis if it lasts for more than 5 minutes, if it is repetitive (i.e., 2
or more episodes of true bleeding, i.e. not spots on a handkerchief, within 24 hours), or leads to
an intervention (packing, electrocoagulation etc), 2) gingival bleeding if it occurs spontaneously
(i.e. unrelated to tooth brushing or eating), or if it lasts for more than 5 minutes, 3) hematuria if it
is macroscopic, and either spontaneous or lasts for more than 24 hours after instrumentation
(e.g., catheter placement or surgery) or the urogenital tract, 4) macroscopic gastro-intestinal
hemorrhage: at least one episode of melena/hematemesis, if clinically apparent, 5) rectal blood
loss, if more than a few spots, 6) hemoptysis, if more than a few speckles in the sputum, 7)
intramuscular hematoma, 8) subcutaneous hematoma if the size is larger than 25 cm2, or larger
than 100 cm2 if provoked, 9) multiple source bleeding, 10) surgical site (e.g. bleeding involving
the surgical wound or the surgical bed).
All other overt bleeding episodes not meeting the criteria for clinically relevant bleeding are
classified as Trivial Bleeding.
Page 27 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 28
Study Personnel
Study PersonnelPrincipal Investigators:Michael J Kovacs, Lawson Health Research Institute-London Health Science Centre (Clinical Coordinating Center), and Marc A Rodger, Ottawa Hospital Research Institute (Data Coordinating Centre)Data Safety Monitoring Board (DSMB)Mary Cushman (chair, College of Medicine Laboratory for Clinical Biochemistry Research).Kenneth Bauer (Beth Israel Deaconess Medical Center), Chris E. Holmes (University of Vermont and Fletcher Allen Health Care), George Howard (Dept. of Biostatistics School of Public Health University of Alabama at Birmingham)
Steering CommitteeMichael J. Kovacs, Marc A. Rodger, David R. Anderson, Phil S. Wells, Clive Kearon, Shannon M. Bates, Susan Kahn, Linda Vickars, Alejandro Lazo-Langner, Tim Ramsay
Lawson Health Research Institute-London Health Science Centre: Project ManagementData Management: Tim Ramsey, Michael Henley, Dong Vo (OHRI)Clinical Trial Management: Mike Henley, Dong Vo (OHRI)Clinical Trial Statistics: Tim Ramsey and Elham Sabri (OHRI)Clinical Operations: Luljeta Pallaveshi (Lead CRA), Judy Kovacs, Holly VanSpronsen, Melinda Robbins, Roweena Corpuz, Tammy Kraushaar, Anne Marie Clement, Melisa Spero, Judy Richard, Rebekah Conlon, Lisa Grey, Blaine Gallant, Naomi Bedek, Pamela Stevens, Terry Schnurr, Laurie A. Sardo, Diane Donovan, Lisa Rudd-Scott , Shannon Dodds, Michelle Zondag, Montreal Vivian Pananis, Susan Finkenbine, Barb St. Jacques, Maria Dzyuba, Martha Lenis, Sheila Kelly, India (Libie Jose, Nayan Ramesh, Anudeep Ratanala, Sunil Swamy, Sital Pawar) Research Ethics Boards (REB): HSREB Western University, Ottawa Hospital Research Ethics Boards, Hamilton Integrated Ethics Board (HIREB), Biomedical D. Research Ethics Board MUHC-Montreal General Hospital, University Health Network Research Ethics Board, Regina Qu’Appelle Research Ethic Board, India: Canara Research Ethical Committee Bendoorwell Mangalore; Institutional Ethics Committees: Care Foundation Care Convergence Centre, Deenanath Mangeshkar Hospital & Research Centre; Poona Medical Research FoundationMonitoring & Safety: Lawson Research Health Institution-LHSC (for Canada sites) and iProcess Coordinator Network (for India sites). Data cleaning and entry: Jennie Cote.Central Adjudication Committee: David Massel, Michael Nicolle and Alejandro Lazo-LangnerStudy Drug Management Pharmacy: Teresa Longfield, Sherry Weir, Tony Gyapong, Patti Gallant, Deborh Snow, Kim Bruce Payne, Diane Lourenco, Maya Biljan, Gita Sobhi, Armanda Marechal, Julie Roy, Muhammad Zyber, Jie Meng, India (S. Bagwan, Anuja N Chougule)
Enrolling Site Investigators:Canada sites:Ottawa site (518): Marc A Rodger, Phil S. Wells, Allan J. Karotovitch, Marc Carrier, LDM Duffett, Lana A. Castelluci, E Gandara, G. Le Gal, D Scarvellis, MA Forgie, CL. Conslaves, CC. Code (OHRI: Ottawa Hospital-General Campus, Ottawa Hospital); Halifax Site (439): David R Anderson, Andrea Kew, Sudeep Shivakumar, Wanda Hasegawa, Sue Robinson, Darrell White, Stephen Couban, Mary Margaret Keating (QEII Health Science Centre);
Page 28 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 29
London Site (140): Michael J Kovacs, Alejandro Lazo-Langner, Martha Louzada, Kang Howson-Jan, Cyrus Hsia, Joy E Mangel, Anargyros Xenocostas, Brian Larocque (London Health Sciences Centre,140); Hamilton Site (159): Shannon M. Bates, Sam Schulman, Clive Kearon, John WA Eikelboom, Sonia Savitri Anand, Kerstin Elisabeth de Wit, Jeffrey I. Weltz, Peter L. Gross, Agnes YY Lee, Lori-Anne Linkins, Jeffrey S. Ginsberg, Frederick A. Spenser, MA Patel (Hamilton HSC – McMaster University, 89; Hamilton General Hospital,46; Hamilton HSC-Henderson,24)Montreal Site (67): Mark Blostein, Susan Solymoss, Susan Kahn (Jewish General Hospital, 56; Montreal General Hospital, 11)Toronto Site (6): Erik Yeo, William F. Brien, Anne McLeod (UHN -Toronto General Hospital,6)Regina Site (5): Patrick Duffy (Regina General Hospital, 5)
India Sites: Mangalore Site (84): Mukund Kumbla, Anoop Nambiar, KP Shabnam, Abdul Khadar kasim, (Omega Hospitals, 84)Hyderabad Site (49): Guntuboina Usha Rani, Mukund Karmalkar, Sharada Kalavakolanu (CARE Hospital Hyderabad, 49) Pune Site (4): Purvez.K Grant, Nirmala Castellino, Nita Murshi, Desai Bhagyashtri Shripatrao; Shireesh Prabhakar Sathe, Bhingare Kishor Laxman (Ruby Hall Clinic, 2; Deenanath Mangeshkar Hospital, 2)
Page 29 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 30
S1. Suggested Classification of Type of Surgery or Procedure
Classification of Type of Surgery or Procedure*
Minor or low-bleeding risk surgery/procedure
Non-cancer Abdominal Surgery (e.g. bowel or visceral organ resection) Cholecystectomy Hernia repair (inguinal, umbilical) Node dissection Vaginal hysterectomy Hand Surgery Skin procedure (dermatologic surgery or any other dermatologic procedure) Non-joint replacement orthopedic Line insertion (cardiac catheterization, angiogram) Dental procedure (tooth extraction) Endoscopic procedure (e.g. colonoscopy, gastroscopy, esophagoscopy, bronchoscopy without
biopsy)
Major or high-bleeding risk surgery/procedure
Cancer surgery:o GU o Head and Neck o Chest (Lung lobectomy) o Abdominal (mass removal, colectomy, etc.)o Breast (mastoidectomy, reconstruction, etc.) o Extremities
Arthroplasty Kidney biopsy Urologic Surgery Liver biopsy Prostate biopsy TURP Pacemaker Insertion/internal defibrillator insertion Abdominal hysterectomy Vascular surgery (e.g. vascular bypass, abdominal aortic aneurysm repair) Colonic polyp resection Major orthopedic surgery (e.g. hip or knee replacement)
*Note: Patients who satisfied the trial eligibility criteria were classified according to this suggested classification, although the final destination as minor/major /high bleeding risk was left to the discretion of the site investigator.
Page 30 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 31
S2. Surgeries or Procedures by Category and Type
A. Major or high-bleeding risk surgery/procedure
Major or high-bleeding risk surgery/procedure(n=890)
Placebo(n=359)
Dalteparin(n=531)
Cancer Surgery 48 87 -GU 8 23 -Head and Neck 14 12 -Abdomen 14 27 -Breast 8 20 -Chest 2 3 -Extremities 2 2Arthroplasty 33 54Kidney Biopsy 1 3Liver Biopsy 1 2Prostate Biopsy 24 23TURP 13 7Pacemaker 5 29Abdominal Hysterectomy 13 12Vascular Surgery 19 13Cholecystectomy 4 9Cystoscopy 3 5Endoscopic Procedure 129 132Dental Procedure 1 2Hernia Repair 21 54Line Insertion 8 17Kidney Lithotripsy 1 7Wound 2 5Non-Cancer Head and Neck Surgery
4 7
Eye Surgery 5 14Non-Cancer Abdominal Surgery
4 2
Non-Cancer GU Surgery 4 12Hand Surgery 2 6Orthopedic 0 5Non-Joint Replacement Orthopedic
4 7
Skin Procedure 2 8Other 8 9
Page 31 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 32
B. Minor or low-bleeding risk surgery/procedure
Minor or low-bleeding risk surgery/procedure(n=581)
Placebo(n=290)
Dalteparin(n=291)
Non-cancer Abdominal Surgery
5 11
Cholecystectomy 4 9Hernia Repair 8 11Skin Procedure 19 29Non-Joint Replacement Orthopedic
15 9
Endoscopic Procedure 108 80Line Insertion 33 31Dental Procedure 63 55Vaginal Hysterectomy 1 0Hand Surgery 4 14Eye Surgery 3 11Kidney Lithotripsy 6 3Cardiac Ablation 6 7Breast Procedure 4 4Pacemaker 1 3Other 10 14
Page 32 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Page | 33
S3. Times to Death
Study arm Adjudicated cause of death(SAE coded term)
No. of days to death
Dalteparin Pancreatic cancer *93Dalteparin NSSCL 85Dalteparin Lung carcinoma *98Dalteparin Mass lesion in medulla 63Dalteparin Congestive heart failure (CHF) 32Dalteparin Metastatic adenocarcinoma 14
Placebo Metastatic esophageal cancer 86Placebo Myocardial Infarction 3Placebo Metastatic cancer 86Placebo VT Storm- Lung cancer 84Placebo Myocardial Infarction 75Placebo Unknown 87Placebo Stroke 24Placebo Unknown *97Note: The number of days of surgery is computed from the day of the procedure/ randomization to 90 days follow up. *Three of the death events occurred after the 90 days of follow up.
Page 33 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Conflict of Interest
Manuscript Title:
Double blind randomized controlled trial of postoperative low molecular weight heparin bridging therapy for patients who are at high risk for arterial thromboembolism (PERIOP2)
Authors:
Michael J. Kovacs, Philip S. Wells, David R. Anderson, Alejandro Lazo-Langner, *Clive Kearon, Shannon M. Bates, Mark Blostein, Susan R. Kahn, Sam Schulman, Elham Sabri, *Susan Solymoss, Tim Ramsay, Erik Yeo, and Marc A. Rodger; for the PERIOP2 Investigators(*These authors are deceased)
Corresponding Author: Dr. Michael J. Kovacs
Corresponding Author’s address:
London Health Sciences Centre800 Commissioners Road EastRoom E6-214London, Ontario, Canada N6A 5W9
Corresponding Author’s telephone #: 519-685-8500 ext. 52254Corresponding Author e-mail: [email protected]
Details of nature of conflict of interest:
Dr. Sam Schulman has received honoraria from Alnylam, Boehringer Ingelheim, Bayer HealthCare, Daiichi Sankyo, Pfizer, and Sanofi, and research support from Boehringer Ingelheim and Octapharma.None of these have any connection with the study.
Dr. Shannon M. Bates has received consultancy fees from Leo Pharma Canada.
Dr. Philip S. Wells declares honoraria from Bayer Healthcare, Janssen, Sanofi, Medscape, Servier Canada, Pfizer, BMS, WebMd and Grant fees from Bayer Healthcare, Pfizer/BMS in the last 3 years outside the submitted work.
There are no other conflicts of interest.
Page 34 of 34
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960





























