Embed Size (px)
Citation preview
To learn more, please visit www.hcp.novartis.com/ products/arzerra.
INDICATIONS for ARZERRA® (ofatumumab)• In combination with chlorambucil, for the treatment of
previously untreated patients with chronic lymphocytic leukemia (CLL) for whom fludarabine-based therapy is considered inappropriate
• For extended treatment of patients who are in complete or partial response after at least two lines of therapy for recurrent or progressive CLL
• For the treatment of patients with CLL refractory to fludarabine and alemtuzumab
IMPORTANT SAFETY INFORMATION for ARZERRA® (ofatumumab)
WARNING: HEPATITIS B VIRUS REACTIVATION AND PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY• Hepatitis B Virus (HBV) reactivation can occur in
patients receiving CD20-directed cytolytic antibodies, including ARZERRA, in some cases resulting in fulminant hepatitis, hepatic failure, and death
• Progressive Multifocal Leukoencephalopathy (PML) resulting in death can occur in patients receiving CD20-directed cytolytic antibodies, including ARZERRA
Dosing and Administration Guide
for ARZERRA
Please see additional Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
2 3
Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
Understanding the Difference Between First-Line, Extended Treatment Following Two or More Lines of Therapy, and FA-Refractory Dosing for ARZERRAThis guide is designed to be used as a quick reference for the proper dosing of ARZERRA in the treatment of first-line CLL, extended treatment following two or more lines of therapy, and CLL that is refractory to fludarabine and alemtuzumab (FA).
For your convenience, dosing instructions specific to each indication are organized separately: first-line CLL in the first section (page 4), extended treatment after at least two lines of therapy in the second section (page 8), and FA-refractory CLL in the third section (page 12). General information about product handling is covered in the fourth section (page 18).
If you have any questions regarding ARZERRA or would like to schedule an in-service program, please contact Novartis Pharmaceuticals Corporation or visit us at www.hcp.novartis.com/products/arzerra.
Welcome
Table of Contents
Dosing for ARZERRA Plus Chlorambucil for First-Line CLL . . . . . . . . . . . . . . . . . . . . 4
Dosing Recommendations . . . . . . . . . . . . . . 4Premedication . . . . . . . . . . . . . . . . . . . . . . . 5Infusion Rates . . . . . . . . . . . . . . . . . . . . . . . 6
Dosing for ARZERRA for Extended Treatment of Patients With CLL After at Least Two Lines of Therapy . . . . . . . . . 8
Dosing Recommendations . . . . . . . . . . . . . . 8Premedication . . . . . . . . . . . . . . . . . . . . . . . 9Infusion Rates . . . . . . . . . . . . . . . . . . . . . . 10
Dosing for ARZERRA for CLL Refractory to Fludarabine and Alemtuzumab . . . . 12
Dosing Recommendations . . . . . . . . . . . . . 12Premedication . . . . . . . . . . . . . . . . . . . . . . 13Infusion Rates . . . . . . . . . . . . . . . . . . . . . . 14
Infusion Rate Dose Modifications for Infusion Reactions . . . . . . . . . . . . . . . . . 16
Product Handling . . . . . . . . . . . . . . . . . . 18Preparation of Solution . . . . . . . . . . . . . . . 18Administration . . . . . . . . . . . . . . . . . . . . . . 19How Supplied . . . . . . . . . . . . . . . . . . . . . . 20Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Support and Resources. . . . . . . . . . . . . . . . 22
Indications and Important Safety Information . . . . . . . . . . . . . . . . . 24

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
1000 mg
Cycles 2 up to 12
Day 1 of each 28-day cycle1000 mg
Median infusion time: 5.2 hours for Cycle 1, Day 1 and 4.2 to 4.4 hours for subsequent infusions
Cycle 1
300 mgDay 1 Day 8
1000 mg
Cycles 2 through 6
Day 1 of each 28-day cycle1000 mg
Cycle 1
300 mgDay 1 Day 8
Median infusion time: 5.3 hours for Cycle 1, Day 1 and 4.1 to 4.2 hours for subsequent infusions
2000 mg
Weeks 12, 16, 20, 24Weeks 1-8
300 mg Doses2-8 2000 mgDoses
9-12Dose
1
Weekly Every 4 Weeks
Administer first and second infusions over 6.5 hours; administer subsequent infusions (3-12) over 4 hours†
After Cycle 1, ARZERRA is dosed in 28-day cycles.
54
Oral acetaminophen 1000 mg (or equivalent) plus
Oral or IV antihistamine (diphenhydramine 50 mg or cetirizine 10 mg or equivalent) plus
IV corticosteroid (prednisolone 50 mg or equivalent)
Corticosteroid may be reduced or omitted for subsequent infusions if a grade 3 or greater infusion-related adverse event did
not occur during the first 2 infusions
Infusion reactions may occur despite premedication
Dosing for ARZERRA Plus Chlorambucil for First-Line CLL1
Premedication1
Patients should receive all of the following premedication agents 30 minutes to 2 hours prior to each infusion of ARZERRA
Chlorambucil:
• 10 mg/m2 orally days 1-7 of each 28-day cycle1
• Please note: The chlorambucil dosing information seen here was evaluated in the pivotal trial, but is not a recommendation from the Dosage and Administration section of the Prescribing Information2
In the pivotal trial1:
• Median number of cycles completed was 6
Dosing Recommendations1
• Administer ARZERRA in an environment where facilities to adequately monitor and treat infusion reactions are available
• Prepare according to instructions on page 18
• Administer as an intravenous (IV) infusion according to the schedule outlined above
• Do not administer as an IV push or bolus or as a subcutaneous injection
• Premedicate before each infusion
* The pivotal trial defined best response as 2 consecutive response assessments of stable disease, partial response, or complete response.1
Dosing for ARZERRATreatment should be continued for a minimum of 3 cycles until best response* or a maximum of 12 cycles
First-Line C
LL Do
sing
IMPORTANT SAFETY INFORMATION
Infusion ReactionsARZERRA can cause serious, including fatal, infusion reactions manifesting as bronchospasm, dyspnea, laryngeal edema, pulmonary edema, flushing, hypertension, hypotension, syncope, cardiac events, back pain, abdominal pain, pyrexia, rash, urticaria, angioedema, cytokine release syndrome, and anaphylactoid/anaphylactic reactions.

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
0-30 12 25
31-60 25 50
61-90 50 100
91-120 100 200
121-150 200 400
151-180 300 400
>180 400 400
Initial 300-mg dose 3.6 12
Subsequent infusions of 1000 mg 25 25
76
Dosing for ARZERRA Plus Chlorambucil for First-Line CLL1
Initial 300-mg Dosea
(mL/hour)
Interval After Start of Infusion (min)
Subsequent Infusionsb (mL/hour)
aInitial 300 mg: Median durations of infusions=4.8 to 5.2 hours.b Subsequent infusions of 1000 mg: Median durations of infusions=4.2 to 4.4 hours.
Dosemg/hour mL/hour
Infusion Initiation Rates
• Initiate infusion at a rate of 12 mg/hour if a grade 3 or greater infusion-related adverse event was experienced during the previous infusion
• In the absence of an infusion-related adverse event, the rate of infusion may be increased every 30 minutes as described in the Infusion Rate Table to the right. Do not exceed the infusion rates in the following Infusion Rate Table
Infusion rates for ARZERRAInfusion RatesInfusion initiation rates for ARZERRA
IMPORTANT SAFETY INFORMATION (cont’d)
Infusion Reactions (cont’d) Administer ARZERRA in an environment where facilities to adequately monitor and treat infusion reactions are available. Premedicate with acetaminophen, an antihistamine, and a corticosteroid. Infusion reactions may occur despite premedication.
Interrupt ARZERRA for infusion reactions of any severity and initiate appropriate medical treatment. If an anaphylactic reaction occurs, immediately and permanently discontinue ARZERRA.
IMPORTANT SAFETY INFORMATION (cont’d)
Hepatitis B Virus (HBV) ReactivationHBV reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, has occurred in patients treated with ARZERRA.
Screen all patients for HBV infection before initiating ARZERRA.
Monitor patients with evidence of current or prior HBV infection for clinical and laboratory signs of hepatitis or HBV reactivation during and for several months following treatment with ARZERRA. HBV reactivation has been reported for at least 12 months following completion of therapy.
In ARZERRA-treated patients who develop reactivation of HBV, immediately discontinue ARZERRA and any concomitant chemotherapy, and institute appropriate treatment.

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
1000 mg
7 Weeks Later andEvery 8 Weeks
1000 mg
Cycle 1
300 mgDay 1 Day 8
98
Oral acetaminophen 1000 mg (or equivalent) plus
Oral or IV antihistamine (diphenhydramine 50 mg
or cetirizine 10 mg or equivalent) plus
IV corticosteroid (prednisolone 50 mg or equivalent)
Corticosteroid may be reduced or omitted for subsequent infusions if a grade 3 or greater infusion-related
adverse event did not occur during the first 2 infusions
Infusion reactions may occur despite premedication
Dosing for ARZERRA for Extended Treatment of Patients With CLL After at Least Two Lines of Therapy1
Premedication1
Patients should receive all of the following premedication agents 30 minutes to 2 hours prior to each infusion of ARZERRA
What Is Extended Treatment?Patients who achieve a partial or complete response to therapy may continue to have a leukemic burden, which could lead to progression. At the time of the efficacy analysis in the clinical trial, the median follow-up was 19.4 months with the ARZERRA arm and 18.7 months with the observation arm. The event rate (progressed or died) was 33% in the ARZERRA arm and 51% in the observation arm.
Dosing Recommendations1
• Administer ARZERRA in an environment where facilities to adequately monitor and treat infusion reactions are available
• Prepare according to instructions on page 18• Administer as an IV infusion according to the
schedule outlined above• Do not administer as an IV push or bolus or as a
subcutaneous injection• Premedicate before each infusion
Dosing for ARZERRASingle-agent ARZERRA for a maximum of 2 years Exten
ded
CLL Treatm
ent D
osin
g
IMPORTANT SAFETY INFORMATION (cont’d)
HBV InfectionFatal infection due to hepatitis B in patients who have not been previously infected has been observed with ARZERRA. Monitor patients for clinical and laboratory signs of hepatitis.
IMPORTANT SAFETY INFORMATION (cont’d)
Progressive Multifocal Leukoencephalopathy (PML)PML resulting in death has occurred with ARZERRA. Consider PML in any patient with new onset of or changes in pre-existing neurological signs or symptoms.If PML is suspected, discontinue ARZERRA and initiate evaluation for PML, including neurology consultation.

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
0-30 12 25
31-60 25 50
61-90 50 100
91-120 100 200
121-150 200 400
151-180 300 400
>180 400 400
Initial 300-mg dose 3.6 12
Subsequent infusions of 1000 mg 25 25
1110
Initial 300-mg Dosea
(mL/hour)
Interval After Start of Infusion (min)
Subsequent Infusionsb (mL/hour)
aInitial 300 mg: Median durations of infusions=4.8 to 5.2 hours.b Subsequent infusions of 1000 mg: Median durations of infusions=4.2 to 4.4 hours.
Dosemg/hour mL/hour
Infusion Initiation Rates
• Initiate infusion at a rate of 12 mg/hour if a grade 3 or greater infusion-related adverse event was experienced during the previous infusion
• In the absence of an infusion-related adverse event, the rate of infusion may be increased every 30 minutes as described in the Infusion Rate Table to the right. Do not exceed the infusion rates in the following Infusion Rate Table
Infusion rates for ARZERRA
Infusion RatesInfusion initiation rates for ARZERRA
Dosing for ARZERRA for Extended Treatment of Patients With CLL After at Least Two Lines of Therapy1
IMPORTANT SAFETY INFORMATION (cont’d)
Tumor Lysis Syndrome (TLS)TLS, including the need for hospitalization, has occurred in patients treated with ARZERRA. Patients with high tumor burden and/or high circulating lymphocyte counts (>25 x 109/L) are at greater risk.
Consider TLS prophylaxis with anti-hyperuricemics and hydration prior to infusion of ARZERRA.
For treatment of TLS, administer aggressive intravenous hydration and anti-hyperuricemic agents, correct electrolyte abnormalities, and monitor renal function.
IMPORTANT SAFETY INFORMATION (cont’d)
CytopeniasSevere cytopenias, including neutropenia, thrombocytopenia, and anemia, can occur with ARZERRA. Pancytopenia, agranulocytosis, and fatal neutropenic sepsis have occurred in patients who received ARZERRA in combination with chlorambucil. Grade 3 or 4 late-onset neutropenia and/or prolonged neutropenia were reported in ARZERRA-treated patients.
Monitor complete blood counts at regular intervals during and after conclusion of therapy, and increase the frequency of monitoring in patients who develop Grade 3 or 4 cytopenias.

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
1000 mg
Diphenhydramine 50 mg or cetirizine
10 mg or equivalent plus
Prednisolone 100 mg or equivalenta
a Do not reduce corticosteroid dose for Infusions 1, 2, and 9. Corticosteroid dose may be reduced as follows:
• Infusions 3 through 8: Corticosteroid may be reduced or omitted with subsequent infusions if a grade 3 or greater infusion reaction did not occur with the preceding infusion(s)
• Infusions 10 through 12: Prednisolone may be given at reduced dose of 50 mg to 100 mg (or equivalent) if a Grade 3 or greater infusion-related adverse event did not occur with Infusion 9
Infusion reactions may occur despite premedication
1000 mg
Cycles 2 up to 12
Day 1 of each 28-day cycle1000 mg
Median infusion time: 5.2 hours for Cycle 1, Day 1 and 4.2 to 4.4 hours for subsequent infusions
Cycle 1
300 mgDay 1 Day 8
1000 mg
Cycles 2 through 6
Day 1 of each 28-day cycle1000 mg
Cycle 1
300 mgDay 1 Day 8
Median infusion time: 5.3 hours for Cycle 1, Day 1 and 4.1 to 4.2 hours for subsequent infusions
2000 mg
Weeks 12, 16, 20, 24Weeks 1-8
300 mg Doses2-8 2000 mgDoses
9-12Dose
1
Weekly Every 4 Weeks
Administer first and second infusions over 6.5 hours; administer subsequent infusions (3-12) over 4 hours†
In a study of FA-refractory patients (study 2), 88% of patients received at least 8 infusions of ARZERRA and 54% received all 12 infusions.
1312
Dosing for ARZERRAARZERRA is administered as 12 infusions over a 24-week period
Dosing Recommendations• Administer ARZERRA in an environment where
facilities to adequately monitor and treat infusion reactions are available
• Prepare according to instructions on page 18
• Administer as an IV infusion according to the schedule outlined above
• Do not administer as an IV push or bolus or as a subcutaneous injection
• Premedicate before each infusion
Oral or IV Antihistamine
Oral Acetaminophen
IV Corticosteroid
Dosing for ARZERRA for CLL Refractory to Fludarabine and Alemtuzumab1
PremedicationPatients should receive all of the following premedication agents 30 minutes to 2 hours prior to each infusion of ARZERRA
FA-R
efractory C
LL Do
sing
IMPORTANT SAFETY INFORMATION (cont’d)
ImmunizationsDo not administer live viral vaccines to patients who have recently received ARZERRA.

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
0-30 12 25
31-60 25 50
61-90 50 100
91-120 100 200
>120 200 400
Infusion 1 (300 mg) 3.6 12
Infusion 2 (2000 mg) 24 12
Infusions 3 through 12 (2000 mg)
50 25
14 15
Infusions 1 and 2a
(mL/hour)
Interval After Start of Infusion (min)
Subsequent Infusionsb (mL/hour)
a Infusions 1 and 2 (300 mg and 2000 mg): Median duration of infusions=6.8 hours.
b Subsequent infusions of 2000 mg: Median durations of infusions=4.2 to 4.4 hours.
Infusionmg/hour mL/hour
Infusion Initiation Rates
Dosing for ARZERRA for CLL Refractory to Fludarabine and Alemtuzumab1
Infusion rates for ARZERRA
Infusion RatesInfusion initiation rates for ARZERRA
• Initiate infusion at a rate of 12 mg/hour if a grade 3 or greater infusion-related adverse event was experienced during the previous infusion
• In the absence of an infusion-related adverse event, the rate of infusion may be increased every 30 minutes as described in the Infusion Rate Table to the right. Do not exceed the infusion rates in the following Infusion Rate Table
IMPORTANT SAFETY INFORMATION (cont’d)
Most Common Adverse ReactionsPreviously untreated CLL:(≥10%, all grades) were infusion reactions (67% for ARZERRA plus chlorambucil vs 0% for chlorambucil) and neutropenia (27% vs18%).
Extended treatment therapy in CLL: Common adverse reactions (≥10%) were infusion reactions, neutropenia, and upper respiratory infection.
IMPORTANT SAFETY INFORMATION (cont’d)
Most Common Adverse Reactions (cont’d)In the single-arm refractory CLL clinical trial, the most common adverse reactions (≥10%, all grades) were neutropenia, pneumonia , pyrexia , cough , diarrhea , anemia , fatigue , dyspnea , rash , nausea , bronchitis , and upper respiratory tract infections . The most common serious adverse reactions were infections (including pneumonia and sepsis), neutropenia, and pyrexia.

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.16 17
• After resuming the infusion, the infusion rate may be increased according to the Infusion Rate Tables on pages 6-7, 10-11, and 14-15 based on patient tolerance
• Consider permanent discontinuation of ARZERRA if the severity of the infusion reaction does not resolve to less than or equal to grade 2 despite adequate clinical intervention
• Permanently discontinue therapy for patients who develop an anaphylactic reaction to ARZERRA
Infusion Rate Dose Modifications• Interrupt infusion for infusion reactions of any
severity. Treatment can be resumed at the discretion of the treating physician. The following infusion rate modifications can be used as a guide
• If the infusion reaction resolves or remains less than or equal to grade 2, resume infusion with the following modifications according to the initial grade of the infusion reaction
Infusion Rate Dose Modifications for Infusion Reactions1
Infu
sion
Rate D
ose M
od
ificatio
ns
IMPORTANT SAFETY INFORMATION (cont’d)
Laboratory AbnormalitiesIn the previously untreated CLL clinical trial, post-baseline hematologic laboratory abnormalities (all grades) occurring with ≥5% incidence in patients receiving ARZERRA plus chlorambucil, and also ≥2% more than patients receiving chlorambucil, were leukopenia (67% for ARZERRA plus chlorambucil vs 28% for chlorambucil), neutropenia (66% vs 56%), and lymphopenia (52% vs 20%).
Infusion reactions occur more frequently with the first 2 infusions.
Grade 1 or 2:
Grade 3 or 4:
Infuse at one-half of the previous infusion rate
Infuse at a rate of 12 mL/hour

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA. 1918
*First-line and extended treatment use only.†FA-refractory use only.
Product Handling1
Administration Instructions• Administer ARZERRA in an environment where
facilities to adequately monitor and treat infusion reactions are available
• Do not administer as an IV push or bolus or as a subcutaneous injection
• Do not mix ARZERRA with, or administer as an infusion with, other medicinal products
• Administer using an infusion pump and an administration set
• Flush the IV line with 0.9% Sodium Chloride Injection, USP before and after each dose
• Start infusion within 12 hours of preparation
• Discard prepared solution after 24 hours
Preparation and Administration• Do not shake product
• Inspect parenteral drug products visually for particulate matter and discoloration prior to administration. ARZERRA should be a clear to opalescent, colorless solution. The solution should not be used if discolored or cloudy, or if foreign particulate matter is present
Preparation of Solution• 300-mg dose: Withdraw and discard 15 mL from
a 1000-mL bag of 0.9% Sodium Chloride Injection, USP. Withdraw 5 mL from each of 3 single-use, 100-mg vials of ARZERRA and add to the bag
• 1000-mg dose*: Withdraw and discard 50 mL from a 1000-mL bag of 0.9% Sodium Chloride Injection, USP. Withdraw 50 mL from 1 single-use, 1000-mg vial of ARZERRA and add to the bag
• 2000-mg dose†: Withdraw and discard 100 mL from a 1000-mL bag of 0.9% Sodium Chloride Injection, USP. Withdraw 50 mL from each of 2 single-use, 1000-mg vials of ARZERRA and add to the bag
• Mix diluted solution by gentle inversion
• Store diluted solution between 2° to 8°C (36° to 46°F)
• No incompatibilities between ARZERRA and polyvinylchloride or polyolefin bags and administration sets have been observed
Prod
uct H
and
ling
Not actual size.
Prepare all doses in 1000 mL of 0.9% Sodium Chloride Injection, USP.
Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
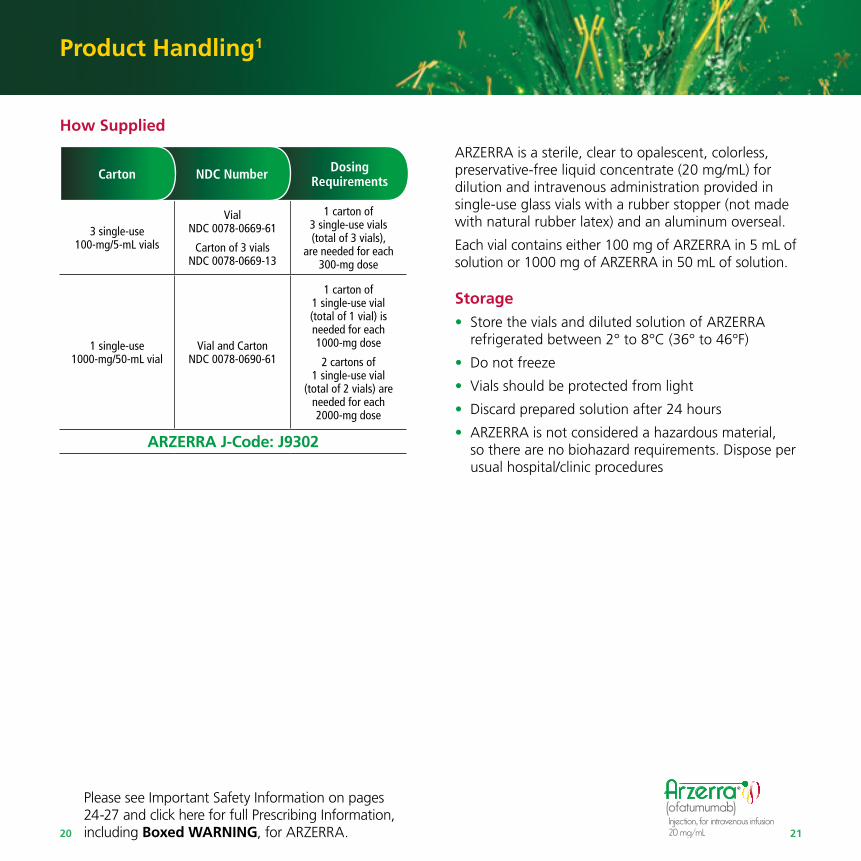
3 single-use 100-mg/5-mL vials
VialNDC 0078-0669-61
Carton of 3 vialsNDC 0078-0669-13
1 carton of 3 single-use vials(total of 3 vials),
are needed for each 300-mg dose
1 single-use 1000-mg/50-mL vial
Vial and CartonNDC 0078-0690-61
1 carton of 1 single-use vial (total of 1 vial) is needed for each 1000-mg dose
2 cartons of 1 single-use vial
(total of 2 vials) are needed for each 2000-mg dose
ARZERRA J-Code: J9302
20 21
ARZERRA is a sterile, clear to opalescent, colorless, preservative-free liquid concentrate (20 mg/mL) for dilution and intravenous administration provided in single-use glass vials with a rubber stopper (not made with natural rubber latex) and an aluminum overseal.
Each vial contains either 100 mg of ARZERRA in 5 mL of solution or 1000 mg of ARZERRA in 50 mL of solution.
Storage• Store the vials and diluted solution of ARZERRA
refrigerated between 2° to 8°C (36° to 46°F)
• Do not freeze
• Vials should be protected from light
• Discard prepared solution after 24 hours
• ARZERRA is not considered a hazardous material, so there are no biohazard requirements. Dispose per usual hospital/clinic procedures
NDC NumberCarton Dosing Requirements
Product Handling1
How Supplied

Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA. 2322
1-888-NOW-NOVA (1-888-669-6682)
Monday-Friday, 8:30 am-5:00 pm ET
Customer Interaction CenterNovartis Pharmaceuticals Corporation One Health Plaza East Hanover, NJ 07936-1080
Support and Resources
Novartis Pharmaceuticals Corporation is committed to providing you with direct access to the resources you and your patients need while treating CLL with ARZERRA.
Contact InformationCustomized Medical Support You can request personalized assistance from an ARZERRA Medical Sciences Liaison by contacting Novartis Pharmaceuticals Corporation directly via the contact information provided at left.
Available Now!Information about ARZERRA is available for you at www.hcp.novartis.com/products/arzerra/ and for your patients at www.us.ARZERRA.com.
24 25
Please see additional Important Safety Information on pages 26 and 27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
Indications and Important Safety Information
INDICATIONS for ARZERRA ® (ofatumumab)
• In combination with chlorambucil, for the treatment of previously untreated patients with chronic lymphocytic leukemia (CLL) for whom fludarabine-based therapy is considered inappropriate
• For extended treatment of patients who are in complete or partial response after at least two lines of therapy for recurrent or progressive CLL
• For the treatment of patients with CLL refractory to fludarabine and alemtuzumab
IMPORTANT SAFETY INFORMATION for ARZERRA® (ofatumumab)
Infusion Reactions
• ARZERRA can cause serious, including fatal, infusion reactions manifesting as bronchospasm, dyspnea, laryngeal edema, pulmonary edema, flushing, hypertension, hypotension, syncope, cardiac events, back pain, abdominal pain, pyrexia, rash, urticaria, angioedema, cytokine release syndrome, and anaphylactoid/anaphylactic reactions
Infusion Reactions (cont’d)
• Administer ARZERRA in an environment where facilities to adequately monitor and treat infusion reactions are available. Premedicate with acetaminophen, an antihistamine, and a corticosteroid. Infusion reactions may occur despite premedication
• Interrupt ARZERRA for infusion reactions of any severity and initiate appropriate medical treatment. If an anaphylactic reaction occurs, immediately and permanently discontinue ARZERRA
Hepatitis B Virus (HBV) Reactivation
• HBV reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, has occurred in patients treated with ARZERRA
• Screen all patients for HBV infection before initiating ARZERRA
• Monitor patients with evidence of current or prior HBV infection for clinical and laboratory signs of hepatitis or HBV reactivation during and for several months following treatment with ARZERRA. HBV reactivation has been reported for at least 12 months following completion of therapy
• In ARZERRA-treated patients who develop reactivation of HBV, immediately discontinue ARZERRA and any concomitant chemotherapy, and institute appropriate treatment
HBV Infection
• Fatal infection due to hepatitis B in patients who have not been previously infected has been observed with ARZERRA. Monitor patients for clinical and laboratory signs of hepatitis
Imp
ortan
t Safety Info
rmatio
n
WARNING: HEPATITIS B VIRUS REACTIVATION AND PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY
• Hepatitis B Virus (HBV) reactivation can occur in patients receiving CD20-directed cytolytic antibodies, including ARZERRA, in some cases resulting in fulminant hepatitis, hepatic failure, and death
• Progressive Multifocal Leukoencephalopathy (PML) resulting in death can occur in patients receiving CD20-directed cytolytic antibodies, including ARZERRA
Please see additional Important Safety Information on pages 24 and 25 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.26 27
Indications and Important Safety Information (cont’d)
References: 1. ARZERRA [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2016. 2. Data on file. Novartis Pharmaceuticals Corp; 2014.
Progressive Multifocal Leukoencephalopathy (PML)
• PML resulting in death has occurred with ARZERRA. Consider PML in any patient with new onset of or changes in pre-existing neurological signs or symptoms
• If PML is suspected, discontinue ARZERRA and initiate evaluation for PML, including neurology consultation
Tumor Lysis Syndrome (TLS)
• TLS, including the need for hospitalization, has occurred in patients treated with ARZERRA. Patients with high tumor burden and/or high circulating lymphocyte counts (>25 x 109/L) are at greater risk
• Consider TLS prophylaxis with anti-hyperuricemics and hydration prior to infusion of ARZERRA
• For treatment of TLS, administer aggressive intravenous hydration and anti-hyperuricemic agents, correct electrolyte abnormalities, and monitor renal function
Cytopenias
• Severe cytopenias, including neutropenia, thrombocytopenia, and anemia, can occur with ARZERRA. Pancytopenia, agranulocytosis, and fatal neutropenic sepsis have occurred in patients who received ARZERRA in combination with chlorambucil. Grade 3 or 4 late-onset neutropenia and/or prolonged neutropenia were reported in ARZERRA-treated patients
• Monitor complete blood counts at regular intervals during and after conclusion of therapy, and increase the frequency of monitoring in patients who develop Grade 3 or 4 cytopenias
Immunizations
• Do not administer live viral vaccines to patients who have recently received ARZERRA
Most Common Adverse Reactions
• Previously untreated CLL:(≥10%, all grades) were infusion reactions (67% for ARZERRA plus chlorambucil vs 0% for chlorambucil) and neutropenia (27% vs18%)
• Extended treatment therapy in CLL: Common adverse reactions (≥10%) were inf usion reactions, neutropenia, and upper respiratory infection
• In the single-arm refractory CLL clinical trial, the most common adverse reactions (≥10%, all grades) were neutropenia, pneumonia , pyrexia , cough , diarrhea , anemia , fatigue , dyspnea , rash , nausea , bronchitis , and upper respiratory tract infections . The most common serious adverse reactions were infections (including pneumonia and sepsis), neutropenia, and pyrexia
Laboratory Abnormalities
• In the previously untreated CLL clinical trial, post-baseline hematologic laboratory abnormalities (all grades) occurring with ≥5% incidence in patients receiving ARZERRA plus chlorambucil, and also ≥2% more than patients receiving chlorambucil, were leukopenia (67% for ARZERRA plus chlorambucil vs 28% for chlorambucil), neutropenia (66% vs 56%), and lymphopenia (52% vs 20%)

© 2016 Novartis 2/16 ARZ-1132022
Please see Important Safety Information on pages 24-27 and click here for full Prescribing Information, including Boxed WARNING, for ARZERRA.
More information available at: www.hcp.novartis.com/products/arzerra













![Arzerra® (ofatumumab)€¦ · II. Dosing Limits A. Quantity Limit (max daily dose) [NDC Unit]: Arzerra 100 mg/5 mL: 3 vials Day 1 Arzerra 1000 mg/50 mL: 2 vials weekly x 7 doses,](https://img.dokumen.tips/doc/110x75/5f3873fd4737b54acc31689d/arzerra-ofatumumab-ii-dosing-limits-a-quantity-limit-max-daily-dose-ndc.jpg)















