Embed Size (px)
Citation preview

10ournal ofNeurology, Neurosurgery, and Psychiatry 1993;56:1290-1294
Dorsolateral prefrontal cortex dysfunction in themajor psychoses; symptom or disease specificity?
R J Dolan, C J Bench, P F Liddle, K J Friston, C D Frith, P M Grasby, R S J Frackowiak
MRC Cyclotron Unit,HammersmithHospital, London, UKR J DolanC J BenchP F LiddleK J FristonC D FrithP M GrasbyR S FrackowiakAcademicDepartment ofPsychiatry, RoyalFree Hospital andSchool ofMedicine,London, UKR J DolanC J BenchP M GrasbyNational Hospital forNeurology andNeurosurgery,London, UKR J DolanR S FrackowiakPsychologyDepartnentUniversity CollegeLondon, UKC D FrithCorrespondence to:Dr Dolan, AcademicDepartment of Psychiatry,Royal Free Hospital andSchool of Medicine, PondStreet, London NW3 2QG,UK.Received 7 August 1992and in final revised form25 February 1993.Accepted 9 March 1993
AbstractNeurophysiological deficits in the leftdorsolateral prefrontal cortex (DLPFC)have been described in positron emissiontomography studies of schizophrenia anddepression. In schizophrenia and depres-sion this deficit has been associated withthe syndromes of psychomotor povertyand psychomotor retardation, res-pectively. Such findings lead to a pre-diction that DLPFC dysfunction issymptom rather than disease related.This prediction was empirically tested ina retrospective study that pooled datafrom 40 patients meeting research diag-nostic criteria for depression and 30patients meeting DSM-III R criteria forschizophrenia. The patients were cate-gorised into those with and withoutpoverty of speech, a symptom that is anobservable manifestation ofpsychomotorimpairment. The profile ofregional cere-bral blood flow (rCBF), measured in allsubjects under resting conditions, wassubsequently compared in these twogroups. Patients with poverty of speechhad significantly lower rCBF in the leftDLFPC. This reduction of rCBF wasindependent of diagnosis. The findingssupport the view that the study of symp-toms, or symptom clusters, can provideinformation additional to that of tradi-tional diagnostic systems in the study ofthe major psychoses.
(7 Neurol Neurosurg Psychiatry 1993;56: 1290-1294)
Studies of cerebral neurophysiology, usingfunctional imaging techniques, indicate multi-focal regional abnormalities in both schizo-phrenia and depression. The presence of mul-tifocal deficits in both disorders is consistentwith current conceptualisations of an anatom-ically distributed neural basis to higher cere-bral functions."2 Among the range offunctional deficits reported in schizophreniaand depression, the most robust finding hasbeen that of 'hypofrontality'.4 Recent stud-ies, particularly those using more refined dataanalytic techniques, have provided greateranatomical specificity to this finding with thedemonstration of dysfunction in the left dor-solateral prefrontal cortex (DLPFC) in bothschizophrenia and depression.5 6The characterisation of the phenomenolog-
ical and neuropsychological correlates of
biological dysfunctions is an important,though often elusive, goal in neuropsychiatricresearch. Nevertheless PET studies havebegun to suggest important and reproduciblephenomenological correlates of DLPFCdysfunction. DeLisi et al reported significantcorrelations between relative hypofrontalityand symptom ratings for emotional with-drawal, disorientation, distractability andhelplessness/hopelessness.7 In a more recentstudy of chronic schizophrenic patients, leftDLPFC dysfunction was associated with asyndrome of psychomotor poverty.8 Indepression functional deficits in the leftDLPFC have also been associated with asyndrome of psychomotor retardation.9
These findings suggest that there are fea-tures common to the pathophysiology of bothdepression and schizophrenia, and in particu-lar, that diminished psychomotor activity isassociated with hypofrontality in both condi-tions. In this investigation we pooled PETdata from two large cohorts of patients diag-nosed as suffering with either schizophreniaor depression. This enabled us to test -thehypothesis that hypofrontality is associatedwith diminished psychomotor activity, irre-spective of diagnosis. Poverty of speech pro-vides a measure of diminished psychomotoractivity that can be assessed in a manner notlikely to be confounded by qualitativeaffective differences between depressed andschizophrenic patients. Poverty of speech inthis study is defined as a "restriction in theamount of spontaneous speech, so that repliesto questions tend to be brief, concrete andunelaborated".'0 Furthermore, poverty ofspeech is highly correlated with syndromes ofpsychomotor poverty in schizophrenia" andpsychomotor retardation in depression."2 Wehave therefore tested the specific hypothesisthat poverty of speech is associated withdecreased perfusion in the left DLPFC indepression and schizophrenia in a mannerthat is independent of diagnosis.
Subjects and methodsSUBJECTSThe mode of selection and clinical character-istics of both the depressed and schizophrenicpatients have been described previously.68 Insummary, 40 depressed patients wereadministered the Schedule for Schizophreniaand Affective Disorders (SADS-L)13 and allmet the Research Diagnostic Criteria'4 forMajor Depressive Disorder and scored over17 on the Hamilton Depression Rating Scale
1290 on M
arch 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.12.1290 on 1 Decem
ber 1993. Dow
nloaded from

Dorsolateral prefrontal cortex dysfunction in the major psychoses
(HAM-D).'5 Exclusion criteria included agegreater than 75 years, a history of alcohol orsubstance abuse, significant previous or cur-rent medical illness, a score of over 4 on theHachinski ischaemic scale'6 or focal abnor-mality on CT or MRI scanning. Half of thispatient sample were receiving medication.The 30 schizophrenic patients were aged
less than 55 years and all met the DSM-III-Rcriteria for schizophrenia.'7 Symptomaticallyall the patients were in a persistently stablestate. These patients were assessed accordingto a protocol specified in the ComprehensiveAssessment of Symptoms and History, whichincludes the Scales for the Assessment ofNegative Symptoms (SANS).'0 All the schizo-phrenic patients were receiving neurolepticmedication with the mean daily dose,expressed in chlorpromazine equivalents,being 1465 (SD 1011) mg. All patients,schizophrenic and depressed, were rated fordepression on a subjective measure of dys-phoria derived from the SADS (item 234).
All patients gave informed consent. Ethicalapproval was obtained from all referringhospitals and locally from the RoyalPostgraduate Medical School Research EthicsCommittee. Permission to administer radio-isotopes was obtained from the Adminis-tration of Radioactive Substances AdvisoryCommittee of the United Kingdom.
PET METHODSRegional cerebral blood flow was measuredunder resting conditions, in a quiet darkenedroom, with the subjects supine in the PETscanner (CTI model 931-08/12). Subjectswere asked to close their eyes during theexamination but no other instructions weregiven. '5Oxygen in the form of C150, mixedwith air was administered via an oxygen maskaccording to an established protocol.'0 Asingle scan was acquired over the final 10minute period of an 18 minute inhalation andarterial blood samples were taken via anindwelling 22 g catheter at 0, 5 and 10 min-utes into the acquisition period. A Hanningfilter with a cut off frequency of 0-5 was usedin the reconstruction of the images giving atransaxial resolution of 8-5 mm. All scanswere performed on the same equipment usingthe same methods over a three year period upto June 1991.
IMAGE ANALYSISImage analysis was performed using SPMsoftware (MRC Cyclotron Unit, London,UK) on a SPARC 1 workstation (SunMicrosystems, Surrey, UK) using an interac-tive image analysis software package (ANA-LYZE, Biodynamic Research Unit, MayoClinic, USA). Calculations and image matrixmanipulations were performed in PROMATLAB (Mathworks, New York).
STEREOTACTIC NORMALISATIONEach reconstructed rCBF scan consisting of15 primary transverse planes was interpolatedto 43 planes to render the voxels approxi-mately cubic. The data were then trans-
formed into a standard stereotactic space.'8'9Such transformation of the data allows forvoxel by voxel averaging of data across sub-jects. In the standard space 1 voxel represents2 x 2 x 4 mm in the x, y and z dimensions,respectively, allowing direct cross reference tothe anatomical features of a standard stereo-tactic atlas.20 A Gaussian filter 10 pixels widewas applied to smooth each image to accom-modate inter-subject differences in gyral andfunctional anatomy and to suppress high fre-quency noise in the images.
DETECTION OF SIGNIFICANT CHANGES IN RCBFDifferences in global activity between subjectswere removed by analysis of covariance on avoxel by voxel basis with global counts ascovariate according to a method previouslydescribed.'8 For each voxel in stereotacticspace, in each experimental group, the analy-sis of covariance generated a condition-specific adjusted mean rCBF value (nor-malised to 50 ml/di/min) and an associatedadjusted error variance. Group means werethen compared using the t-statistic (SPM{t}).The resulting set of t values constitutes a sta-tistical parametric map.2' The omnibus signif-icance of the statistical parametric maps(SPM) was assessed for the whole data set bycomparing the observed and expected distrib-ution of the t-statistic under the null hypothe-sis of no treatment effect. The expected andobserved number of t values exceeding agiven threshold (p < 0-001) was compared(using the Chi squared test of proportions)and if significant the location of all voxelswith a t value equal to or greater than thechosen threshold was noted. The resultingSPMs of t values were displayed within thestandard stereotactic space, plane by plane,and as projections on to renderings of themedial and lateral cortical surfaces of thebrain.
STRATEGY FOR DATA ANALYSISThe first step in the analysis was the identifi-cation of pixels where there was a significantdifference in rCBF between patients with andwithout poverty of speech. For this purposewe identified two groups from the combinedpatient sample: those with definite poverty ofspeech (score for the SADS poverty of speechitem of 1, or score for the SANS poverty ofspeech item of 2 or more), and those withoutdefinite poverty of speech. Having identifiedthe locus of greatest difference in rCBFbetween the two groups, analysis of variancewas used to examine the contributions ofpoverty of speech and of diagnosis to variancein rCBF at that site, and to test the nullhypothesis of no interaction between theseindependent contributions. Furthermore, inthe light of the possibility that depressedmood is associated with decreased rCBF inthe DLPFC (irrespective of diagnosis), analy-sis of covariance was performed to allow forvariation in severity of depressed mood. Forthis purpose the SADS item score for dyspho-ria was used as a measure of depressed mood.
1291 on M
arch 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.12.1290 on 1 Decem
ber 1993. Dow
nloaded from

Dolan, Bench, Liddle, Friston, Frith, Grasby, Frackowiak
Table 1 Coordinates of the pixels where the most significant differences in bloodflow wereidentified. Co-ordinates refer to the stereotaxic atlas of Talairach and Tournoux. The CBFvalues are in units of mlldl tissuelmin, and have been adjustedfor a global mean bloodflow of 50mlidlimin. The Z score is a measure of the degree ofsignificance of the differenceand is the number ofstandard deviations from the mean t value in the (t) statistical mapof the t valuefor the most significant pixel in the plane
Co-ordinates Regional CBF
Location x y z (A) (B) Z Score
(L) Dorsolateral Prefrontal Cortex -32 36 24 47-5 50-0 3-15*- 34 30 28 48-0 50-6 3-26*-34 30 32 45-4 47.9 3.13*
(A) Patients with poverty of speech.(B) Patients without poverty of speech.
*p < 0-001.
ResultsThe mean (SD) age of the schizophrenic(25 male; 5 female) and depressed patients (25male; 15 female) were 36 (10) and 57 (13),respectively. Twenty seven of the total sample ofpatients (n = 70) were classified as havingpoverty of speech. These comprised 15 patientswith a diagnosis of depression and 12 with adiagnosis of schizophrenia. The mean (SD) ages[48 (15) vs 48 (16)] and sex distribution of thepoverty (17 male; 10 female) and non-poverty(33 male; 10 female) of speech patients were notsignificantly different (12 = 1-54, ns).
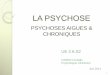
POVERTY OF SPEECH VS NON POVERTY OF SPEECHPATIENTSUsing SPM{t} a categorical comparison wasmade of the rCBF profiles of poverty and non-poverty of speech patients. There was a signifi-
cant difference in the observed and expecteddistribution of t values at a high threshold (p< 0-001). The SPM{t} identified two regionswhere there was a significant relative decreasein rCBF in the poverty of speech group.The areas identified were centred on theleft DLPFC (BA 46/9) and the left angulargyrus (BA 39) with the most significantdifferences centred on the left DLPFC. TheSPM{t} is shown in the figure with thecoordinates and rCBF values of maximalsignificance being displayed in table 1.The adjusted rCBF values, at the pixel
coordinates of maximal difference in theabove SPM {t}, were subsequently sampledfor each individual subject. These values wereentered into a two way analysis of variance(ANOVA), with diagnosis and poverty ofspeech as grouping variables. This analysisindicated a significant effect of poverty ofspeech on left DLPFC rCBF values(p < 0 005). A significant effect of diagnosiswas also apparent with depressed patients dis-playing lower DLPFC rCBF values (p <0 01). No interaction effects were evident.However, as depressed mood has been shownto be independently associated with leftDLPFC dysfunction its possible confoundingeffects were subsequently controlled byrepeating the analysis with a rating of dyspho-ria as covariate. The results of this analysis(ANCOVA) are presented in table 2. Aftercontrolling for the effects of mood the only
re Comparison ofpatients with (n = 27) and without (n = 43) poverty ofspeech using SPM {t}. Areas highlighted indicate regions where thereIgnificant decreases (p < 001) in rCBF in the poverty of speech relative to the non-poverty group. Regions where there are significant decreasesisplayed as orthogonal projections within standard stereotactic space (A) or rendered on to the medial and lateral cortical surface of the leftsphere (B).
1 292 on M
arch 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.12.1290 on 1 Decem
ber 1993. Dow
nloaded from

Dorsolateral prefrontal cortex dysfunction in the major psychoses
Table 2 Two wayANO VA, with dysphoria as covariate, ofrCBF values in the leftdorsolateral prefrontal cortex in depressed and schizophrenic patients with and withoutpoverty of speech
df F p
Diagnosis (schizophrenia v depression 1 0 34 nsSymptom (poverty of speech present v absent) 1 9-1 0 005Interaction (diagnosis by poverty of speech) 1 0-12 ns
significant effect was that of poverty ofspeech. Furthermore, there was no interac-tion effect between diagnosis and poverty ofspeech. The absence of an interaction indi-cates that the effects of poverty of speech onrCBF values in the DLPFC is independent ofdiagnosis. It also indicates that an effect ofpoverty of speech is present in both diagnos-tic groups.
DiscussionThe present study provides evidence that,after allowing for variance due to depressedmood, left DLPFC functional deficits asmeasured by rCBF, are predicted by a
symptom of decreased speech output but notby a diagnosis of schizophrenia or depression.The findings confirm our hypothesis thatDLPFC dysfunction in the major psychosesis related to a behavioural deficit rather than a
specific diagnosis. The data provide strongevidence that shared behavioural deficits innosologically distinct psychiatric disordersmay have common neurophysiological corre-lates.
In our study a single symptom, namelydecreased speech output, was used to predicta neurophysiological deficit. A decrease inspeech output in schizophrenia or depressionis usually a manifestation of a more pervasivevolitional disturbance that characterises psy-chomotor impairment. It can be argued thatsyndromes of psychomotor impairment, indepression and schizophrenia, represent dis-orders of willed or intentional behaviour.Intentional behaviour in this context may bedefined as behaviour not extrinsically speci-fied at the time of responding.
Previous studies have shown thatdepressed and schizophrenic patients displaydecreases in rCBF or regional metabolism inthe left DLPFC.622-25 In separate studies ofthe depressed and schizophrenic patientsamples, that comprise the data for thisreport, DLPFC dysfunction was significantlyrelated to either a syndrome of psychomotorpoverty or a syndrome of psychomotor retar-dation, respectively.8 9
Neither of these two groups displayed socalled "hypofrontality", that is, a globaldecrease in frontal lobe perfusion when com-
pared to controls. Both, however, displayed a
focal decrease in prefrontal perfusion in theDLPFC. The present study extends thesefindings by demonstrating that DLPFC rCBFis predicted by a behavioural deficit ratherthan diagnosis. The findings also indicate thatthe inclusion of significant numbers ofpatients with psychomotor impairment, instudies of depression or schizophrenia,increases the probability of finding a decrease
in DLPFC metabolism or perfusion. Thisassociation of DLPFC hypoperfusion withpsychomotor impairment implies a three waylink between abnormal DLPFC function inmajor psychiatric disorder, psychomotorimpairment and the normal functionalanatomy of the DLPFC. The evidence fromthis study is consistent with the proposal thatthe DLPFC plays an important part in theintrinsic generation of behaviour.The possibility that our findings could be
attributable to the confounding effects ofmedication needs consideration. A proportionof both patients' groupings (poverty and non-poverty) were receiving either neuroleptics orantidepressant medication. In the case ofantidepressants we have previously beenunable to demonstrate significant effects onrCBF at thresholds of significance akin tothose used in the present study.6 A small, butsignificant, effect on cerebral metabolism hasbeen reported in patients receiving neurolep-tics.26 However, the fact that a similar propor-tion of patients in the poverty andnon-poverty groups were receiving neurolep-tics makes a differential effect of this medica-tion an insufficient explanation for thepresent findings.A considerable number of animal and of
human studies highlight a role for theDLPFC in intrinsic generation of behaviour.Lesion studies indicate a role in responseselection in the absence of extrinsic informa-tion.27 A range of volitional and behaviouraldisturbances have been reported in humansubjects with DLPFC lesions. These includea syndrome of decreased speech output,28 areduction in both the frequency and variety ofvoluntary motility29 and more pervasive dis-turbances characterised by apathy, hypokine-sis, lack of initiative and spontaneity.30 Theseclinical observations suggest that DLPFClesions preferentially effect repertoires ofbehavioural expression that are independentof external guidance (ie, non-cued behaviour).The functional specialisation of discrete
brain systems can be established in studies ofnormal subjects using PET activation para-digms. The functional anatomy of intentionalbehaviour has been investigated in two sepa-rate studies, using a verbal fluency and a*motor generation task, respectively. In bothinvestigations the critical neuropsychologicalparameter was that of internal generation.Across both tasks the common region of acti-vation was centred on the left DLPFC."These findings are of direct relevance to thepresent study as they highlight activations,during the performance of willed actions, in acortical area that is dysfunctional in patientswith poverty of speech. The findings couldindicate that the fundamental deficit inpatients with this symptom is that of internalgeneration. Furthermore, the largely asym-metric nature of the activations observed dur-ing tasks based upon internal generationagrees with the asymmetric findings in ourstudy.
In the present study a decrease in rCBFwas also seen in the poverty of speech group
1293 on M
arch 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.12.1290 on 1 Decem
ber 1993. Dow
nloaded from

Dolan, Bench, Liddle, Friston, Frith, Grasby, Frackowiak
in the left angular gyrus. This cortical area isdescribed as multimodal and its functions inhumans include visuospatial orientation andattention.32-34 Previous studies have impli-cated this area in the psychomotor povertysyndrome of schizophrenia, of which povertyof speech is an important symptom.8 In aPET activation study, consisting of a motorgeneration task, activation of the DLPFC wasassociated with a decrease in rCBF in the leftangular gyrus.31 This finding suggests thatthis cortical area may be part of a large scaleneuronal network whose cooperative interac-tions with the DLPFC may be necessary intasks involving internal generation.
Both schizophrenia and depression, as cur-rently defined, encompass a wide range ofphenomenological and neuropsychologicaldeficits. In the absence of external biologicaldiscriminators the validity of the clinical dis-tinction between these disorders has beenquestioned, particularly in the context of con-tinuities in symptom profiles across both con-ditions.'5 Therapeutic interventions have alsofailed to validate the distinction, with clinicalresponse to pharmacological interventionsbeing more strongly predicted by symptomsand not diagnosis.'6 The findings of our studyindicate an overlap in the neurobiologicaldeficits of both depression and schizophreniawith a shared neurophysiological abnormalityaccounting for a similar symptom of povertyof speech.Most biological studies of schizophrenia
and depression are predicted on an assump-tion that both are distinct disease entities.Alternative viewpoints have posited a func-tional approach to psychopathology.'7 Theessence of this approach is that the basic unitsof classification in psychopathology are nei-ther diseases nor syndromes but psychologi-cal dysfunctions. Within this framework themajor psychoses, schizophrenia and depres-sion, can be viewed as conglomerates of psy-chological dysfunctions that are nosologicallynonspecific. This approach has echoes inmore recent arguments for a symptom ratherthan a disease approach to psychiatricresearch.'8 In the present study a symptom,but not a disease, was strongly predictive of aneurobiological dysfunction. This finding canbe seen as supportive of a viewpoint that thestudy of symptoms, or symptom constel-lations, can provide information additional tothat of categorical diagnostic systems inneurobiological studies of functional psychi-atric disorders.
CJB and KF were both supported by the Wellcome Trust.
1 Edelman GM, Mountcastle VB. The Mindful Brain: corti-cal organisation and the group-selective theory of higherbrain function. Cambridge, MA: MIT Press, 1977:7-100.
2 Mountcastle VB, Lynch JC. Posterior parietal associationcortex of the monkey: Command functions for opera-tions within extrapersonal space. Y Neurophysiol 1975;38:871-909.
3 Buchsbaum MS, DeLisi LE, Holcomb HH, et al.Anteroposterior Gradients in Cerebral Glucose Use inSchizophrenia and Affective Disorders. Arch GenPsychiatry 1984;41:1 159-66.
4 Ingvar DH, Franzen G. Abnormalities of Cerebral BloodFlow Distribution In Patients With Chronic
Schizophrenia. Acta Psychiatr Scand 1974;50:425-62.5 Wolkin A, Angrist B, Wolf A, et al. Low Frontal Glucose
Utilisation in Chronic Schizophrenia: A ReplicationStudy. Am J Psychiatry 1988;145:251-3.
6 Bench CJ, Friston KJ, Brown RG, Scott L, FrackowiakRSJ, Dolan RJ. The Anatomy of Melancholia.Abnormalities of Regional Cerebral Blood Flow inMajor Depression. PsycholMed 1992;22:607-15.
7 DeLisi LE, Holcomb HH, Cohen RM, et al. PositronEmission Tomography in Schizophrenic Patients Withand Without Neuroleptic Medication. J Cereb BloodFlow Metab 1985;5:201-6.
8 Liddle P, Friston KJ, Frith CD, Hirsch SR, Jones T,Frackowiak RSJ. Patterns of cerebral blood flow inschizophrenia. BrJPsychiatry 1992;160:179-86.
9 Bench CJ, Friston KJ, Brown R, Frackowiak RSJ, DolanRJ. Regional cerebral blood flow (rCBF) in depressionmeasured by positron emission tomography (PET): therelationship with clinical dimensions. Psychol Med 1993;23:579-90.
10 Andreasen NC. The scale for assessment of negativesymptoms. Iowa City: University of Iowa, 1983.
11 Liddle P. Schizophrenic syndromes, cognitive perfor-mance and neurological dysfunction. Psychol Med1987;17:49-57.
12 Widlocher DJ. Psychomotor retardation: Clinical, theor-etical, and psychometric aspects. Psychiatric Clin N Am1983;6:27-40.
13 Endicott J, Spitzer RL. A Diagnostic Interview. TheSchedule for Affective Disorders and Schizophrenia.Arch Gen Psychiatry 1978;35:837-44.
14 Spitzer RL, Endicott J, Robins E. Research diagnosticcriteria for a selected group of functional disorders. NewYork: Biometrics Research Division, New York StatePsychiatric Institute, 1977.
15 Hamilton M. A rating scale for depression. J7 NeurolNeurosurg Psychiatry 1960;23:56-62.
16 Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral BloodFlow in Dementia. Arch Neurol 1975;32:632-7.
17 American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. Washington DC: AmericanPsychiatric Association, 1980.
18 Friston KJ, Frith CD, Liddle PF, Dolan RJ, LammertsmaAA, Frackowiak RSJ. The relationship between globaland local changes in PET scans. J7 Cereb Blood FlowMetab 1990;10:458-66.
19 Friston KJ, Frith CD, Liddle PF, Frackowiak RSJ. PlasticTransformation of PET Images. J Comp Ass Tomog1991;15:634-9.
20 Talairach J, Tournoux P. Co-planar stereotaxic adas of thehuman brain. Stuttgart: George Thieme Verlag, 1988:1-122.
21 Friston KJ, Frith CD, Liddle PF, Frackowiak RSJ.Comparing Functional (PET) Images: The Assessmentof Significant Change. J Cereb Blood Flow Metab1991;11:690-9.
22 Baxter LR, Schwartz JM, Phelps ME, et al. Reduction ofPrefrontal Cortex Metabolism Common to Three Typesof Depression. Arch Gen Psychiatry 1989;46:243-50.
23 Weinberger DR, Berman KF, Zec RF. PhysiologicDysfunction of Dorsolateral Prefrontal Cortex inSchizophrenia. 1. Regional Cerebral Blood FlowEvidence. Arch Gen Psychiatry 1986;43: 114-24.
24 Martinot JL, Hardy P, Feline A, et al. Left PrefrontalGlucose Hypometabolism in the Depressed State: AConfirmation. AmJ Psychiatry 1990;147:1313-7.
25 Liddle PF, Friston KJ, Hirsch SR, Frackowiak RSJ.Regional Cerebral Metabolic Activity in ChronicSchizophrenia. Schiz Res 1990;3:23-4.
26 Wik G, Wiesel FA, Sjogren I, Blomqvist G, Greitz T,Stone Elander S. Effects of sulpiride and chlorpro-mazine on regional cerebral glucose metabolism inschizophrenic patients as determined by positron emis-sion tomography. Psychopharmacology 1989;97:309-18.
27 Goldman-Rakic PS. Circuitry of primate prefrontal cortexand regulation of behaviour by representationalmemory. In: Mountcastle VB, et al, eds. Handbook ofphysiology-The nervous system V. Baltimore: Williamsand Wilkins, 1987:373-417.
28 Luria AR. Traumatic aphasia. The Hague: Mouton, 1970.29 Klages W. Frontale und diencephale antriebsschwache.
Arch PsychiatrZ Neurol 1954;191:365-87.30 Stuss DT, Benson DF. Frontal lobe lesion and behaviour.
In: Localisation in neuropsychology. Academic Press,1983.
31 Frith CD, Friston KJ, Liddle PF, Frackowiak RSJ. Willedaction and the prefrontal cortex in man: a study withPET. ProcR Soc Lond B 1991;244:241-6.
32 Mesulam M-M. The functional anatomy and hemisphericspecialization for directed attention. Trends Neurosci1983;6:384-7.
33 Heilman KM, Pandya DN, Geschwind N. Trimodal inat-tention following parietal lobe ablations. Trans AmNeurol Assoc 1970;95:259-61.
34 Lynch JC. The functional organization of the posteriorparietal association cortex. Behav Brain Sci1980;3:485-99.
35 Kendell RE, Gourlay J. The clinical distinction betweenthe affective psychoses and schizophrenia. Br JPsychiatry 1970;117:261-6.
36 Johnstone EC, Crow TJ, Frith CD, Owens DGC. TheNorthwick park "Functional' Psychosis study: diagnosisand treatment response. Lancet 1988;ii: 119-24.
37 van Praag HM, Leijnse B. Neubewertung des syndroms.Psychiatr Neurol Neurochir 1965;68:50-66.
38 Costello CG. Research on symptoms versus research onsyndromes. BrJ Psychiatry 1992;160:304-8.
1294 on M
arch 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.12.1290 on 1 Decem
ber 1993. Dow
nloaded from