Embed Size (px)
Citation preview

Donation After Circulatory Death (DCD) Heart Transplantation in Australia: a solution to the donor shortage?
Dr Sarah Scheuer, Dr Hong Chee Chew, Professor Peter Macdonald, Assoc Prof Kumud Dhital
On Behalf of St Vincent’s Hospital DCD Heart Transplant Group

Transplantation pathways
Donation after brain death (DBD)
Controlled death - minimal to no warm ischaemic time (WIT)
Donation after circulatory death (DCD)
Uncontrolled progression to asystole - variable WIT
Declaration of brain death
Preservation flush
ProcurementCold static
storage
Withdrawal of life
supportAsystole
Stand off period
Declaration of circulatory
death
Blood collection
Preservation flush
ProcurementNormothermic
machine reperfusion
WITCold ischaemic
time
Combined ischaemic time (CiT)

Overcoming the DCD heart barriers
Enhancing tolerance to warm ischemia with supplementation
GTN – nitric oxide donor
• Hing A J, et al. Combining Cariporide with Glyceryl Trinitrate
Optimizes Cardiac Preservation During Porcine Heart
Transplantation. American Journal of Transplantation. 2009; 9:
2048–2056
EPO – glycoprotein hormone, active in SAFE cardioprotective
pathway
• Watson AJ, et al. Enhanced preservation of the rat heart following
prolonged hypothermic ischemia with erythropoietin supplemented
Celsior solution. J Heart Lung Transplant. 2013; 32: 633–640
• DCD hearts are exposed to an
unavoidable warm ischaemic injury
• Ideal preservation modality
• Minimizes ischaemic injury
• Allow for organ resuscitation
• Facilitate viability assessment prior to
transplantation
Normothermic perfusion device

Current outcomes of the clinical DCD program
59 DCD retrievals
44 Hearts Retrieved
41 Clinical
28 Transplanted
13 Declined
11 Inadequate Recovery
2 OCS Failure3 Research
15 Did Not Progress (DNP)
Protocol modifications
• Commencement of WIT at systolic BP < 90 mmHg
• Extension of donor age to <55
• Addition of increased dose of methylprednisolone and regular albumin
to combat oedema whilst on the TransMedics
26 27
4238 37
4 2
7
7 8
0
10
20
30
40
50
60
Heart transplants per annum by donation pathway
DCD
DBD
2014 2015 2016 2017 2018
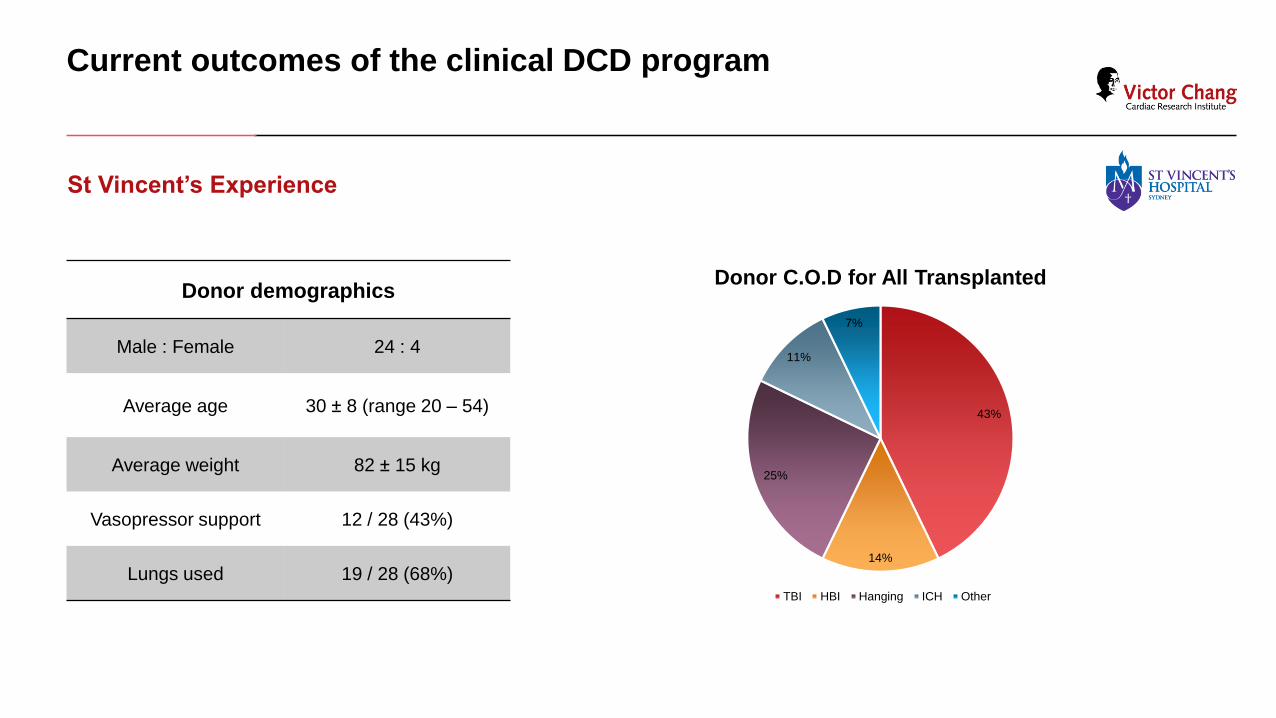
Current outcomes of the clinical DCD program
St Vincent’s Experience
Donor demographics
Male : Female 24 : 4
Average age 30 ± 8 (range 20 – 54)
Average weight 82 ± 15 kg
Vasopressor support 12 / 28 (43%)
Lungs used 19 / 28 (68%)
43%
14%
25%
11%
7%
Donor C.O.D for All Transplanted
TBI HBI Hanging ICH Other

Current outcomes of the clinical DCD program
Time on OCS (TransMedics) 285 min (mean, range 141 – 410)
Recipient Cross Clamp Time (min) 87 ± 33
Recipient Bypass Time (min) 190 ± 69
Mechanical Support
• ECMO
• IABP
43% (12/28)
*36% (10/28)
11% (3/28)
ICU Stay (days) 7 – median (mean 9 ± 7)
Hospital Stay (days) 24 – median (mean 28 ± 19)
LVEF - 1 week 67 ± 5%
Survival (Log Rank) 96% (vs. 87% DBD at 4 years)
No-ECMO ECMO P-value
Warm Ischaemic Time 23 ± 6 mins 23 ± 3 mins 0.32
Time to Asystole 11 ± 5 mins 9 ± 3 mins 0.08
Asystole – Cardioplegia 12 ± 2 mins 15 ± 3 mins 0.003
Cold Ischaemic Time 29 ± 5 mins 27 ± 6 mins 0.20
OCS 277 ± 70 mins 306 ± 60 mins 0.14
Conclusion
• DCD heart procurement is a feasible alternative to the traditional DBD pathway, with excellent results in patient cohort to date
• Combined approach, to both further improve ischaemic tolerance and minimise asystole-plegia time required to reduce high early ECMO rates
• High staff requirements and cost may be prohibitive in some centres

Clinical studies
Heart and Lung Clinic
• Dr Mark Connellan
• Dr Alasdair Watson
• Dr Emily Granger
• Prof Chris Hayward
• A/Prof Andrew Jabbour
• Dr Paul Jansz
• Prof Anne Keogh
• A/Prof Eugene Kotlyar
• Dr Phillip Spratt
Pre-clinical studies
Victor Chang Cardiac Research Institute – Transplant laboratory
• Dr Ling Gao
• Dr Hong Chee Chew
• Dr Arjun Iyer
• Dr Jeanette Villaneuva
• Aoife Doyle
• Dr Mark Hicks
Perfusionists
• Mr Claudio Soto
• Mr Adam Roshan
Transplant Coordinators
ICU
• Dr Priya Nair





























