Embed Size (px)
Citation preview

American Journal of Transplantation 2012; 12: 965–975Wiley Periodicals Inc.
C© Copyright 2011 The American Society of Transplantationand the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2011.03894.x
Donation After Cardiac Death Liver TransplantRecipients Have an Increased Frequencyof Acute Kidney Injury
J. A. Leitheada,b,∗, L. Tariciottia, B. Gunsonb,
A. Holta, J. Isaaca, D. F. Mirzaa, S. Bramhalla,
J. W. Fergusona and P. Muiesana
aLiver Unit, Queen Elizabeth Hospital, Birmingham, UKbNIHR Biomedical Research Unit and Center forResearch, University of Birmingham, Birmingham, UK*Corresponding author: Joanna Agnes Leithead,[email protected]
Donation after cardiac death (DCD) liver transplan-tation is associated with an increased frequency ofhepato-biliary complications. The implications for re-nal function have not been explored previously. Theaims of this single-center study of 88 consecutiveDCD liver transplant recipients were (1) to comparerenal outcomes with propensity-risk-matched dona-tion after brain death (DBD) patients and (2) in theDCD patients specifically to examine the risk fac-tors for acute kidney injury (AKI; peak creatinine ≥2times baseline) and chronic kidney disease (CKD; eGFR<60 mL/min/1.73 m2). During the immediate postoper-ative period DCD liver transplantation was associatedwith an increased incidence of AKI (DCD, 53.4%; DBD31.8%, p = 0.004). In DCD patients AKI was a risk factorfor CKD (p = 0.035) and mortality (p = 0.017). The cu-mulative incidence of CKD by 3 years post-transplantwas 53.7% and 42.1% for DCD and DBD patients, re-spectively (p = 0.774). Importantly, increasing peakperioperative aspartate aminotransferase, a surrogatemarker of hepatic ischemia reperfusion injury, was theonly consistent predictor of renal dysfunction afterDCD transplantation (AKI, p < 0.001; CKD, p = 0.032).In conclusion, DCD liver transplantation is associatedwith an increased frequency of AKI. The findings sug-gest that hepatic ischemia reperfusion injury may playa critical role in the pathogenesis of post-transplantrenal dysfunction.
Key words: Acute kidney injury, chronic kidney dis-ease, donation after cardiac death, ischemia reperfu-sion injury, transplantation
Abbreviations: AKI, acute kidney injury; AST, aspar-tate aminotransferase; BMI, body mass index; CI,confidence interval. DBD, donation after brain death;DCD, donation after cardiac death; eGFR, estimatedglomerular filtration rate; FFP, fresh frozen plasma;INR, international normalised ratio; IQR, inter-quartile
range; MELD, model for end-stage liver disease; NASH,non-alcoholic steatohepatitis; OR, odds ratio; PRS,propensity risk score; RCC, red cell concentrate; SD,standard deviation; UKELD, UK score for patients withend-stage liver disease.
Received 07 July 2011, revised 17 October 2011 andaccepted for publication 09 November 2011
The growing discrepancy between supply and demand forliver transplantation has necessitated the search for mea-sures to increase the donor pool (1). Donation after cardiacdeath (DCD) is recommended as one such strategy, andDCD liver transplantation has seen a rapid expansion inrecent years (2,3). The United States now sources 5% ofliver allografts from donors after cardiac death and in theUnited Kingdom, where the organ donation rate is com-paratively low and waiting list mortality high, 15% of livertransplants are from DCD (4–6).
Although DCD liver transplantation demonstrates satisfac-tory long-term outcomes, patient survival and graft survivalare worse than in donation after brain death (DBD) recipi-ents (7–9). Moreover, DCD patients have greater morbiditywith an increased incidence of ischemic cholangiopathy(10). The key mediator of this greater graft dysfunction ishypothesized to be the added donor warm ischemic time(DWIT) (11–13). Warm ischemia duration correlates withthe postoperative systemic inflammatory response, whichis the common pathway for the multiple organ dysfunc-tion of sepsis and other inflammatory disorders (14–17).Therefore, it follows that patients who undergo DCD livertransplantation may also be at greater risk of extrahepaticcomplications.
Renal dysfunction is a major cause of morbidityand mortality after liver transplantation. (18–20). Eti-ology is multifactorial with most studies focusing onpretransplant recipient risk factors and immunosuppres-sion (20). However, ischemia reperfusion injury has beenlinked with perioperative hemodialysis, and it is probablethat acute kidney injury post liver transplant shares someof the patho-physiological features of the renal dysfunctionof sepsis (21,22). Acute kidney injury can cause perma-nent structural damage, with progressive tubulo-interstitial
965

Leithead et al.
fibrosis and long-term implications for renal function(20,23–25). Thus, DCD liver transplantation may result in agreater frequency of acute kidney injury as well as chronickidney disease.
The clarification of the impact of DCD liver transplantationon renal function has important implications for patientselection and management. The minimization of renal in-jury has emerged as a priority for transplant physicians,and the identification of predictive variables could help todetermine those who may benefit from tailored immuno-suppressive regimens (26,27). Furthermore, any associa-tions could help to guide future therapeutic targets.
The aims of this study were firstly to compare renal out-comes following DCD liver transplantation with a matched
group of DBD recipients and secondly, in DCD recipientsspecifically, to examine the risk factors for acute kidneyinjury and chronic kidney disease.
Methods
This was a retrospective single-center study of 88 consecutive patientswho underwent controlled (Maastricht category III) donation after cardiacdeath (DCD) liver transplantation for chronic liver disease between January2007 and March 2011. In our unit we allocate DCD livers to older morestable recipients, preferring early cirrhotics with hepatocellular carcinoma(Table 1). A control group of patients matched by propensity risk score(PRS) to the DCD cohort who received a whole donation after brain death(DBD) liver transplant for chronic liver disease during the same time periodwas identified. No DCD or DBD patient had a previous history of renaltransplantation and no patient received a combined liver–kidney transplant.
Table 1: Clinical characteristics of donation after cardiac death recipients and donation after brain death recipients at time of hospitaladmission for transplantation
Prematch Postmatch
DCD Whole DBD DCD Whole DBD(n = 88) (n = 291) p-Value (n = 88) (n = 88) p-Value
Age (years) 55.7 (8.5) 53.0 (10.8) 0.033 55.7 (8.5) 56.0 (9.2) 0.810Gender (male:female) 1.4:1 1.8:1 0.412 1.4:1 1.5:1 0.878Ethnicity
Caucasian 67 (76.1) 252 (86.6) 67 (76.1) 66 (75.0)Asian 15 (17.0) 28 (9.6) 15 (17.0) 18 (20.5)Other 6 (6.8) 11 (3.8) 0.062 6 (6.8) 4 (4.5) 0.712
Body mass index 27.0 (4.8) 27.4 (5.0) 0.503 27.0 (4.8) 28.3 (5.5) 0.085Etiology of liver disease
Alcoholic cirrhosis 24 (27.3) 76 (26.1) 24 (27.3) 21 (23.9)Hepatitis C cirrhosis 21 (23.9) 59 (20.3) 21 (23.9) 28 (31.8)Primary biliary cirrhosis 12 (13.6) 41 (14.1) 12 (13.6) 10 (11.4)Primary sclerosing cholangitis 8 (9.1) 23 (7.9) 8 (9.1) 5 (5.7)NASH cirrhosis 7 (8.0) 12 (4.1) 7 (8.0) 2 (2.3)Hepatitis B cirrhosis 6 (6.8) 15 (5.2) 6 (6.8) 6 (6.8)Autoimmune hepatitis 3 (3.4) 8 (2.7) 3 (3.4) 2 (2.3)Other 7 (8.0) 57 (19.6) 0.298 7 (8.0) 14 (15.9) 0.390
Hepatocellular carcinoma 37 (42.0) 73 (25.1) 0.002 37 (42.0) 32 (36.4) 0.440MELD score 14 (5) 16 (7) 0.014 14 (5) 13 (4) 0.537UKELD 50 (6) 51 (6) 0.051 50 (6) 49 (5) 0.568Regraft 0 (0) 18 (6.2) 0.008 0 (0) 0 (0) 1.000Inpatient at time of transplantation 0 (0) 13 (4.5) 0.030 0 (0) 0 (0) 1.000Measures of renal function
Creatinine (lmol/L) 77 (62–98) 86 (67–100) 0.077 77 (62–98) 74 (61–89) 0.177eGFR (mL/min/1.73 m2) 91 (30) 88 (36) 0.221 91 (30) 98 (34) 0.144Sodium (mmol/L) 138 (134–140) 138 (135–140) 0.842 138 (134–140) 138 (135–140) 0.392Hemodialysis 0 (0) 0 (0) 1.000 0 (0) 0 (0) 1.000Ascites 37 (42.0) 158 (54.3) 0.041 37 (42.0) 43 (48.9) 0.364Refractory ascites 13 (14.8) 50 (17.2) 0.586 13 (14.8) 10 (11.4) 0.502
ComorbidityDiabetes mellitus 29 (33.0) 67 (23.0) 0.061 29 (33.0) 27 (30.7) 0.746Insulin-dependent diabetes 10 (11.4) 29 (10.0) 0.711 10 (11.4) 11 (12.5) 0.816Hypertension 15 (17.0) 37 (12.8) 0.306 15 (17.0) 16 (18.2) 0.843
Waiting list time (days) 56 (25–138) 69 (23–185) 0.362 56 (25–138) 56 (19–182) 0.854Follow-up time (days) 724 (435–1016) 895 (480–1311) 0.014 724 (435–1016) 748 (410–1081) 0.473
Values expressed as mean (standard deviation), median (interquartile range) and number (percent) where appropriate. Follow-up timedefined as duration from transplant to present day (patients not censored at time of death or regraft).DBD = donation after brain death; DCD = donation after cardiac death; eGFR= estimated glomerular filtration rate; MELD = model forend-stage liver disease; NASH = nonalcoholic steatohepatitis; UKELD = UK score for patients with end-stage liver disease.
966 American Journal of Transplantation 2012; 12: 965–975

DCD Liver Transplantation: Renal Outcomes
Data were collected on the following donor and graft variables: age, gender,height, aspartate aminotransferase (AST), inotropes, warm ischemic time(in the United Kingdom most centers define donor warm ischemic timeas the time period between systolic blood pressure <50 mmHg or oxygensaturations <80% and cold reperfusion with preservation solution) and coldischemic time. Donor risk index was calculated as previously described (28).An allograft biopsy was performed immediately after reperfusion (time zero)in 76 DCD patients (86.4%) and 63 DBD patients (71.6%) and was gradedby an independent histopathologist.
The following recipient characteristics at the time of admission for trans-plantation were recorded: age, gender, ethnicity, body mass index (BMI),additional comorbidity including need for hemodialysis, international nor-malized ratio (INR), serum bilirubin, serum creatinine, serum sodium andpresence of ascites (past history or ultrasonographic evidence). Refrac-tory ascites was defined according the International Ascites Club criteria(29,30). The MELD (model for end-stage liver disease) score was deter-mined (31). The UK score for patients with end-stage liver disease (UKELD),a recently devised scoring system that incorporates serum sodium in addi-tion to the MELD variables that is now used routinely in the United Kingdomto prioritize graft allocation, was also calculated (32). Intraoperative red cellconcentrate (RCC), fresh frozen plasma (FFP) and platelet transfusion re-quirements, intraoperative inotropes (noradrenaline/adrenaline infusion attime of admission to the intensive care unit) and the occurrence of a car-diac arrest on reperfusion were noted. Documented perioperative variables(following transplantation but prior to hospital discharge) were peak serumAST, peak serum creatinine, need for renal replacement therapy and sepsis.Renal function was then recorded at 1, 3, 6, 9, 12, 18, 24, 30, 36, 42 and 48-months following transplantation. Patients receiving renal replacement ther-apy during the immediate postoperative period were given a peak serumcreatinine of three times baseline if the actual recorded value was less (33).Similarly, beyond the perioperative period patients on hemodialysis weregiven an estimated glomerular filtration rate of 15 mL/min/1.73 m2 (34).
Perioperative acute renal dysfunction (following transplantation but prior tohospital discharge) was defined according to the RIFLE criteria for acute kid-ney injury (AKI): peak serum creatinine ≥2 times the baseline level (33). Themain measure of renal function thereafter was estimated glomerular filtra-tion rate (eGFR), determined using the modification of diet in renal disease(MDRD) study 4-variable equation (eGFR = 186 × creatinine (mg/dL)−1.154
× age (years)−0.203 × 1.212 (if black) × 0.742 (if female) (35). Chronic kid-ney disease was defined as eGFR <60 mL/min/1.73 m2 on at least twooccasions and sustained from 6 months post-transplant onwards: stage 3,stage 4 and stage 5 chronic kidney disease were defined as eGFR 30–59mL/min/1.73 m2, 15–29 mL/min/1.73 m2 and <15 mL/min/1.73 m2 or ondialysis, respectively (34).
All type biliary complications included ischemic cholangiopathy, biliary anas-tomotic stricture, bile leak, choledocholithiasis and biloma formation. Is-chemic cholangiopathy was defined as nonanastomotic biliary strictures onmagnetic resonance cholangiopancreatography or endoscopic retrogradecholangiopancreatography with a patent hepatic artery (13).
Immunosuppression at time of hospital discharge was noted, and cal-cineurin inhibitor trough levels at day 7, day 30 and 12 months. Standardimmunosuppression was tacrolimus aiming for a trough level of 8–10 withinthe first 3 months of transplantation, azathioprine and reducing dose steroiddiscontinued by 3 months. Renal sparing immunsuppression consisted ofhalf dose tacrolimus aiming for a trough level of 5–8, mycophenolate andreducing dose steroid discontinued by 3 months. Interleukin (IL-2) receptorantagonist induction therapy was not administered to any patient.
Hepatic ischemia reperfusion injury minimizing strategies were not usedin any donor. Intravenous n-acetylcysteine was administered to 33 DCD
recipients (37.5%) and 12 DBD recipients (13.6%) following admission tothe intensive care unit (p < 0.001). This decision was surgeon dependentand in all cases precipitated by clinical evidence of initial poor graft functionsuch as hemodynamic instability, lactic acidosis and/or high serum AST.
Statistical analyses
Matching patients by PRS is a recognized method of controlling for selectionbias (36,37). A PRS for the allocation of a DCD liver over a DBD liver amongthe 379 whole-liver transplant recipients (single organ) in our unit duringthe time period studied was generated by nonparsimonious multiple logisticregression. This model included all recipient variables of clinical relevance tothe outcome measure posttransplant AKI (age, gender, ethnicity, diagnosis,BMI, diabetes mellitus, hypertension, ascites, eGFR, MELD, waiting listtime). The nearest available matching on the estimated PRS method wasused to construct the control group (36). The model did not include the fivestatistically significant interaction terms: including the interaction termsincreased the c-statistic from 0.684 to 0.755 but reduced the number ofDCD liver transplant recipients that could be matched to 77 and had noimpact on the incidence of the outcome measures in the control group.Balance was achieved between the DCD and DBD groups on the recognizedconfounders (Table 1).
Normally distributed continuous variables and nonparametric continuousvariables were compared using the Student’s t test and Mann–Whitneytest, respectively. Chi-squared analysis or Fisher’s exact test were usedfor comparison of categorical data. Survival was estimated using Kaplan–Meier plots with log-rank test for differences, and adjusted survival wasdetermined using Cox proportional hazards analyses. Cumulative incidenceof chronic kidney disease was estimated using the Kaplan–Meier method.To identify variables associated with acute kidney injury in DCD patientsa logistic regression analysis was performed including all clinically relevantfactors simultaneously. Serum sodium was not included in this multivari-ate model because of collinearity. Cox proportional hazards analysis wasthen used to identify variables predictive of chronic kidney disease post-transplant. The MELD score was not included in this multivariate modelbecause of collinearity. p < 0.05 was considered statistically significantunless otherwise stated.
Data were analyzed using the SPSS 15 package. All values were expressedas mean and standard deviation (SD), and median and interquartile range(IQR) as appropriate.
Results
Patient, donor and graft characteristics
DCD and DBD patients were well matched with regardto etiology and severity of liver disease, and relevant co-morbidity (Table 1). Waiting list time was also similar (p =0.854).
Donor and graft characteristics are outlined in Table 2. DCDlivers had a shorter mean cold ischemic time than DBDlivers (p = 0.003) and, after exclusion of the DCD status,there was a trend toward a lower donor risk index in theDCD group (p = 0.060).
Graft and patient survival
During the immediate postoperative period, serum ASTpeaked within 24 h of admission to the intensive care unitin 94.9% of the entire cohort. There was no relationship
American Journal of Transplantation 2012; 12: 965–975 967

Leithead et al.
Table 2: Donor, graft and intraoperative characteristics of dona-tion after cardiac death and donation after brain death recipients.
DCD Whole DBD(n = 88) (n = 88) p-Value
Donor characteristicsAge (years) 46.4 (16.1) 50.4 (14.6) 0.083Gender (male:female) 1.1:1 1:1 1.000Height (cm) 170 (13) 170 (9) 0.814AST (u/L) 50 (27–86) 42 (30–79) 0.353Inotropes 58 (65.9) 75 (85.2) 0.003
Graft characteristics>30% macrovesicular
steatosis1 (1.3) 3 (4.8) 0.247
>30% microvesicularsteatosis
19 (25.3) 18 (28.6) 0.669
Donor warm ischemictime (minutes)
20.1 (9.0) −
Cold ischemic time(hours)
7.3 (1.9) 8.3(2.4) 0.003
Recipient warmischemic time(minutes)
40.1 (8.4) 40.9 (6.4) 0.455
Donor risk index 2.19 (0.57) 1.56 (0.34) < 0.001Donor risk index
excluding DCD status1.45 (0.38) 1.56 (0.34) 0.060
Recipient characteristicsRCC transfusion (units) 2 (0–5) 1 (0–3) 0.026FFP transfusion (units) 10 (5–15) 7 (4–11) 0.008Platelet transfusion
(units)10 (0–10) 5 (0–10) 0.054
Inotropes 65(73.9) 59 (67.0) 0.322Cardiac arrest on
reperfusion3 (3.4) 1 (1.1) 0.310
Values expressed as mean (standard deviation), median (in-terquartile range) and number (percent) where appropriate.AST = aspartate aminotransferase; DBD = donation after braindeath; DCD = donation after cardiac death; FFP = fresh frozenplasma; RCC = red cell concentrate.
between peak AST and donor age (Spearman’s r = −0.006,p = 0.934), donor warm ischemic time (n = 62, Spearman’sr = 0.102, p = 0.431), cold ischemic time (spearman’sr = 0.011, p = 0.885) or recipient warm ischemic time(spearman’s r = 0.108, p = 0.157). Peak AST correlatedwell with the histological grading of preservation injury (n =137, mild, 1680 u/L; mild-moderate, 1350 u/L; moderate,2246 u/L; moderate-severe, 2837 u/L; severe, 7649 u/L,median; p = 0.001).
The median peak AST (DCD, 2691 (1599–4651) u/L; DBD,1328 (870–2028) u/L, median (IQR); p < 0.001) was higherin DCD patients compared to controls. The estimated1- and 3-year graft survival were 83.7% and 77.0% forthe DCD group respectively, and 88.2% and 81.3% for theDBD group (log-rank p = 0.225).
Ninety-one percent of DCD patients and 94.3% of DBD pa-tients survived to hospital discharge (p = 0.387). Estimated1- and 3-year patient survival were 84.9% and 78.0% for
DCD patients respectively, and 90.5% and 83.4% for DBDpatients (log-rank p = 0.142).
Immunosuppression
DCD patients were more likely than DBD patients to beprescribed a renal sparing immunosuppression regime attime of hospital discharge (DCD, 61.7%; DBD, 34.9%;p = 0.001). Nevertheless, tacrolimus trough levels at day7 (DCD, 8.2 (3.6) lg/L; DBD, 8.6 (3.9) lg/L, mean (SD); p= 0.445), day 30 (DCD, 6.9 (2.7) lg/L; DBD, 7.6 (3.2) lg/L,mean (SD); p = 0.152) and 12 months (DCD, 6.6 (2.1) lg/L;DBD, 6.9 (2.4) lg/L, mean (SD); p = 0.532) were similar(p < 0.017 considered significant).
Perioperative renal function
Baseline serum creatinine (p = 0.177), eGFR (p = 0.144),serum sodium (p = 0.392) and the prevalence of ascites(p = 0.364) and refractory ascites (p = 0.502) were com-parable for both DCD and DBD groups (Table 1).
Immediately following transplantation acute renal dysfunc-tion was a common complication, occurring with increased
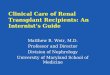
Figure 1: Stacked bar graph demonstrating the proportion
of donation after cardiac death liver transplant recipients
(DCD) and donation after brain death liver transplant recip-
ients (DBD) who developed acute renal dysfunction during
the immediate postoperative period. Renal dysfunction classi-fied according to the RIFLE criteria: Risk of renal dysfunction, peakserum creatinine 1.5–1.9 times baseline; Injury to the kidney, peakserum creatinine 2.0–2.9 times baseline; Failure of kidney func-tion, serum creatinine ≥3 times baseline; Loss of kidney function,renal replacement therapy for >4 weeks; End-stage kidney dis-ease (ESKD), dialysis for >3 months (Ref. 32). In the manuscript“acute kidney injury” included the RIFLE Injury, Failure, Loss andESKD categories.
968 American Journal of Transplantation 2012; 12: 965–975

DCD Liver Transplantation: Renal Outcomes
Table 3: Univariate analysis of variables associated with perioperative acute kidney injury following donation after cardiac death livertransplantation
AKI No AKI(n = 47) (n = 41) p-Value
Donor characteristicsAge (years) 47.5 (13.9) 46.3 (17.2) 0.729Inotropes 27 (57.4) 31 (75.6) 0.073
Graft characteristics>30% macrovesicular steatosis 0 (0) 1 (2.9) 0.461>30% microvesicular steatosis 6 (14.6) 12 (34.3) 0.045Donor warm ischemic time (minutes) (n = 62) 22 (11) 19 (7) 0.267Cold ischemic time (hours) 7.3 (2.0) 7.3 (1.9) 0.920Recipient warm ischemic time (minutes) 44 (13) 37 (7) 0.006Donor risk index 2.16 (0.56) 2.21 (0.60) 0.674
Recipient characteristicsAge (years) 56.3 (9.0) 54.5 (7.8) 0.320Gender (male:female) 1.2:1 1.7:1 0.441Pretransplant
MELD score 14 (6) 14 (5) 0.957UKELD score 49 (6) 50 (5) 0.465Creatinine (lmol/L) 71 (60–102) 84 (66–98) 0.451eGFR (mL/min/1.73 m2) 92 (30) 90 (31) 0.748Sodium (mmol/L) 138 (134–141) 137 (135–140) 0.801Ascites 20 (42.6) 16 (39.0) 0.737Refractory ascites 9 (19.1) 3 (7.3) 0.107Diabetes mellitus 17 (36.2) 12 (29.3) 0.492Insulin-dependent diabetes 6 (12.8) 4 (9.8) 0.460Hypertension 7 (14.9) 8 (19.5) 0.565
IntraoperativeRCC transfusion (units) 2 (0–6) 1 (0–4) 0.058FFP transfusion (units) 10 (5–18) 7 (5–12) 0.045Platelet transfusion (units) 10 (0–20) 10 (0–10) 0.504Inotropes 39 (83.0) 26 (63.4) 0.037
PerioperativeN-acetyl cysteine 25 (53.2) 8 (19.5) 0.001Peak AST (u/L) 4322 (2364–5621) 2117 (998–2984) < 0.001Sepsis 6 (12.8) 2 (4.9) 0.182
Values expressed as mean (standard deviation), median (interquartile range) and number (percent) where appropriate.AKI = acute kidney injury; AST = aspartate aminotransferase; eGFR = estimated glomerular filtration rate; FFP = fresh frozenplasma; MELD = model for end-stage liver disease; RCC = red cell concentrate; UKELD = UK score for patients with end-stage liverdisease.
frequency in DCD recipients (Figure 1). DCD patients hada greater peak perioperative serum creatinine than DBDpatients (DCD, 171 (106–335) lmol/L; DBD, 109 (79–192)lmol/L, median (IQR); p < 0.001), and a greater change inperioperative serum creatinine from baseline (DCD, +114(35–263) %; DBD, +42 (16–164) %, median (IQR); p <
0.001). DCD patients were more likely to develop AKI(DCD, 53.4%; DBD 31.8%; p = 0.004). Duration of AKIwas 8.0 (IQR 2.0–35.0) days for DCD patients and 5.5 (IQR2.0–12.5) days for DBD patients (p = 0.135). Furthermore,DCD patients had a greater frequency of renal replacementtherapy (DCD, 39.8%; DBD, 20.5%; p = 0.005). Median re-nal replacement therapy duration was 8.5 (IQR 2.8–26.0)days and 7.5 (IQR 2.8–14.0) days for DCD and DBD pa-tients, respectively (p = 0.603).
Variables associated with perioperative AKI
in DCD patients
In view of the increased rate of AKI following DCD livertransplantation variables associated with AKI in these pa-tients specifically were examined (Table 3). There was nodifference in the pretransplant serum creatinine (p = 0.451)or eGFR (p = 0.748) of DCD patients who did and did notdevelop AKI. The prevalence of diabetes (p = 0.492) andhypertension (p = 0.565) was also no different betweenthe two groups. Furthermore, the mean MELD (p = 0.957)and UKELD scores (p = 0.465) were similar.
Peak AST demonstrated a close correlation with peak peri-operative serum creatinine (Spearman’s r = 0.499, p <
0.001) and peak perioperative change in serum creatininefrom baseline (Spearman’s r = 0.535, p < 0.001). On
American Journal of Transplantation 2012; 12: 965–975 969

Leithead et al.
Table 4: Logistic regression analysis of variables associated with perioperative acute kidney injury following donation after cardiac deathliver transplantation
Univariate analysis Multivariate model
OR (95% CI) p-Value OR (95% CI) p-Value
Age (years) 1.03 (0.98–1.08) 0.319 1.04 (0.97–1.12) 0.266Female gender 1.40 (0.59–3.30) 0.442 1.19 (0.38–3.73) 0.760Pretransplant
MELD score 1.00 (0.92–1.08) 0.956 1.01 (0.91–1.13) 0.825eGFR (mL/min/1.73 m2) 1.00 (0.99–1.02) 0.744 1.01 (0.99–1.03) 0.384Refractory ascites 3.00 (0.75–11.95) 0.119 3.81 (0.78–18.52) 0.097Insulin-dependent diabetes 1.35 (0.35–5.18) 0.658 0.94 (0.18–5.00) 0.940Hypertension 0.72 (0.24–2.20) 0.566 0.66 (0.15–2.95) 0.587
PerioperativeLog intraoperative RCC transfusion (units) 6.35 (1.09–37.03) 0.040 8.88 (0.91–86.26) 0.060Log peak AST (u/L) 6.14 (2.62–14.40) <0.001 7.44 (2.78–19.88) <0.001
Reference group (relative risk 1.00): male gender, no refractory ascites, no insulin-dependent diabetes mellitus, no hypertension.AST = aspartate aminotransferase; CI = confidence interval; eGFR = estimated glomerular filtration rate; MELD = model for end-stageliver disease; OR = odds ratio; RCC = red cell concentrate.
univariate analysis peak AST was strongly associated withthe development of AKI (p < 0.001).
A multivariate model including all clinically relevant vari-ables simultaneously (Table 4) identified that a higherpeak AST during the immediate postoperative period wasthe only variable associated with acute kidney injury(p < 0.001).
Acute kidney injury and morbidity and mortality
in DCD patients
Given the greater frequency of AKI after DCD liver trans-plantation the implications for morbidity and mortality werealso assessed.
DCD patients with AKI had a prolonged ITU admission(AKI, 7.0 (3.0–9.0) days; no AKI, 2.0 (1.0–3.0) days, me-dian (IQR), p < 0.001) and hospital stay (AKI, 16.0 (11.0–24.0) days; no AKI, 9.0 (7.0–12.0) days, median (IQR), p <
0.001). Moreover, AKI was associated with an increasedlikelihood of chronic kidney disease (AKI, 80.6%; no AKI,39.4%, estimated 3-year cumulative incidence; log rankp = 0.013). In a multivariate model (including the relevantclinical variables simultaneously; age, gender, pretrans-plant eGFR, pretransplant diabetes mellitus, pretransplanthypertension; data not shown) AKI had a hazard ratio forthe development of chronic kidney disease of 2.80 (95%CI 1.07–7.31, p = 0.035).
AKI was not a risk factor for the development of all type bil-iary complications both on univariate (AKI, 31.2%; no AKI,22.8%, estimated 3-year cumulative incidence; log rankp = 0.252) and multivariate analyses (multivariate modelincluding donor age, donor inotropes, cold ischemic time,pretransplant MELD score; data not shown; HR 1.73, 95%CI 0.56–5.33, p = 0.338). AKI was not associated withan increased risk of ischemic cholangiopathy on univari-ate analysis (AKI, 5.0%; no AKI, 8.2%, estimated 3-year
cumulative incidence; log rank p = 0.495) or in a simi-lar multivariate model (HR 0.63, 95% CI 0.05–7.80, p =0.713).
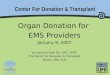
Patient survival was reduced in the AKI group (AKI,66.4%; no AKI, 87.9%, estimated 3-year survival; log rankp = 0.009, Figure 2). After adjusting for relevant clinicalvariables (multivariate model including age, gender, pre-transplant MELD score, pretransplant eGFR, pretransplantdiabetes mellitus simultaneously; data not shown) peri-operative AKI remained a predictor of mortality thereafter(HR 4.17; 95% CI 1.29–12.86, p = 0.017).
Long-term renal function following transplantation
By 1 month posttransplant the mean eGFR was similarin DCD and DBD patients (DCD, 74 (38) mL/min/1.73 m2;DBD, 83 (34) mL/min/1.73 m2, mean (SD), p = 0.104).Furthermore, the mean change in eGFR by 12 months frombaseline was no different for the two groups (DCD patients,−19.5 (27.8) %; DBD patients, −25.3 (23.2) %, mean (SD);p = 0.221).
The cumulative incidence of chronic kidney disease by3 years posttransplant was 53.7% and 42.1% for DCDand DBD patients, respectively (log rank p = 0.774,Figure 3). The cumulative incidence of severe chronic kid-ney disease (stages 4–5) by 3 years after transplantationwas 10.3% for DCD patients and 5.3% for DBD patients(p = 0.282).
Predictors of stage 3–5 chronic kidney disease
posttransplant in DCD patients
Although DCD liver transplantation was not associatedwith a statistically significant increased incidence ofchronic kidney disease, a cox regression analysis was per-formed to examine whether initial graft injury had impli-cations for long-term renal function. Variables associatedwith chronic kidney disease in DCD patients on univariate
970 American Journal of Transplantation 2012; 12: 965–975

DCD Liver Transplantation: Renal Outcomes
Figure 2: Kaplan–Meier plot of the
probability of survival following do-
nation after cardiac death liver trans-
plantation subdivided based on the
presence or absence of acute kidney
injury during the immediate postop-
erative period.
analysis are outlined in Table 5. A subsequent multivari-ate model including all clinically relevant variables simul-taneously found that a greater peak posttransplant ASTwas the only variable predictive of chronic kidney disease(p = 0.032).
Discussion
In this large single-center, case-controlled study we haveexamined for the first time the renal consequences ofliver transplantation using DCD grafts. We have shownthat DCD recipients were more likely to develop AKI thanmatched DBD patients, and had a greater frequency of re-nal replacement therapy. Importantly, peak perioperativeAST, a surrogate marker of hepatic ischemia reperfusioninjury, demonstrated a strong relationship with AKI in thissetting (38). The development of AKI after DCD liver trans-plantation had significant implications for morbidity andmortality, as highlighted by the longer duration of hospital-ization, increased likelihood of chronic kidney disease andworse survival of AKI patients.
AKI after liver transplantation is multifactorial in origin.Pretransplant neuro-humoral and circulatory derangement,and intrinsic chronic kidney disease, predisposes patientswith end-stage liver failure to acute renal dysfunction (39).
Intraoperatively, hemodynamic insults including the surgi-cal technique and hemorrhage culminate in renal ischemia,inflammation and injury (18,19,40). Thereafter, the adminis-tration of a calcineurin inhibitor further compromises renalperfusion and function (41).
The role of graft injury in the pathogenesis of AKI follow-ing liver transplantation is less well recognized. Hepaticischemia reperfusion injury is associated with a systemicinflammatory response, which can cause AKI throughhemodynamic mechanisms and direct tubular cell death(22,42–45). Liver transplant recipients with ischemia reper-fusion injury are more likely to develop acute renal dys-function and to require perioperative hemodialysis (21,46).Therefore, it is probable that graft injury, by driving a sys-temic inflammatory response, is a contributing factor inposttransplant AKI.
The findings of our study suggest that hepatic ischemiareperfusion injury in fact plays a critical role in the patho-genesis of AKI after liver transplantation. The prolongedwarm ischemic time and greater injury of DCD livers wasaccompanied by a 1.7-fold increased incidence of AKI inthe recipient compared to DBD patients. In the DCD groupspecifically, peak AST correlated closely with peak peri-operative serum creatinine, and peak AST was the only
American Journal of Transplantation 2012; 12: 965–975 971

Leithead et al.
Figure 3: Cumulative incidence of
stage 3–5 chronic kidney disease
following liver transplantation sub-
divided into donation after cardiac
death and donation after brain death
recipients.
variable associated with the development of acute renaldysfunction.
AKI patients were more likely to develop chronic kidneydisease following DCD liver transplantation, echoing obser-
vations in the general transplant as well as nontransplantpopulations (20,23,24). Animal studies have confirmed thatAKI can cause permanent structural kidney damage withprogressive tubulo-interstitial fibrosis (25). It is thereforeperhaps surprising that we did not demonstrate that DCD
Table 5: Cox regression analysis of variables associated with chronic kidney disease following donation after cardiac death livertransplantation
Univariate analysis Multivariate model
HR (95% CI) p-Value HR (95% CI) p-Value
Age 1.06 (1.00–1.13) 0.063 1.07 (0.99–1.15) 0.077Female gender 0.90 (0.38–2.16) 0.819 0.97 (0.37–2.59) 0.954Pretransplant
eGFR (mL/min/1.73 m2) 0.99 (0.97–1.00) 0.132 0.99 (0.98–1.01) 0.476Refractory ascites 1.95 (0.65–5.83) 0.232 1.32 (0.42–4.17) 0.632Insulin-dependent diabetes 3.02 (1.01–9.06) 0.049 2.62 (0.75–9.13) 0.130Hypertension 1.72 (0.67–4.41) 0.257 1.59 (0.55–4.61) 0.394
PerioperativeLog peak AST (u/L) 2.01 (1.08–3.74) 0.027 2.14 (1.07–4.29) 0.032RS immunosuppression 2.53 (0.97–6.63) 0.059 1.63 (0.54–4.93) 0.383
Reference group (relative risk 1.00): male gender, no refractory ascites, no insulin-dependent diabetes mellitus, no hypertension, no RSimmunosuppression.AST = aspartate aminotransferase; CI = confidence interval; eGFR = estimated glomerular filtration rate; HR = hazard ratio; RS immuno-suppression = renal sparing immunosuppression.
972 American Journal of Transplantation 2012; 12: 965–975

DCD Liver Transplantation: Renal Outcomes
patients were more likely to develop chronic renal impair-ment. Nevertheless, the lack of difference could be ex-plained by the duration of follow-up or sample size. Further-more, the greater use of renal sparing immunosuppressionin DCD recipients may have contributed to the results (27).In agreement with the hypothesis that DCD livers do haveconsequences for long-term renal function after transplan-tation, increasing peak perioperative AST was associatedwith an increased risk of chronic kidney disease in DCDrecipients. Therefore, it seems feasible that graft injury,through its causal role in perioperative AKI, may also helpto shape chronic renal function following transplantation.
DCD recipients had greater intraoperative transfusion re-quirements implying that greater intraoperative hemody-namic instability contributes to the increased frequency ofAKI after DCD transplantation. Given that the most dra-matic hemodynamic derangement typically occurs at thetime of graft reperfusion, this suggests that postreperfu-sion syndrome, and lesser degrees of postreperfusion cir-culatory dysfunction, are of importance (47,48). However,the systemic release of vasoactive mediators from thegraft or splanchnic circulation is thought to be central tothe development of postreperfusion hemodynamic insta-bility, and the systemic inflammatory response feasibly hasfurther ramifications for graft injury (47,48). Hemostasisand inflammation are equally intricately linked (49). There-fore, intraoperative hemodynamic instability may not be acausal factor in postliver transplant renal injury and insteadboth may be clinical manifestations of the same complexprocess.
It is noteworthy that AST is not specific to the liver beingpresent in many tissues including the kidneys (50). As aresult, an alternative explanation for the relationship be-tween peak AST and renal outcomes could be increasedrenal release of AST as a consequence of kidney injury(51). However, peak AST correlated well with the histo-logical grade of hepatic preservation injury as previouslydescribed (38). Furthermore, serum AST levels have beenshown to be only marginally elevated after renal damage(51). Consequently, this interpretation seems unlikely. Uri-nary excretion does not participate in the clearance of AST(50).
The study has some additional potential limitations thatshould be mentioned. Firstly, the retrospective nature ofthe study meant that the frequency of perioperative ASTand creatinine measurement was variable. All patients hadbloods sampling immediately on arrival to the intensivecare unit and, in most cases, 12 hourly for the first 24–48h. It is possible, for example, that the peak AST under-estimated the severity of graft injury. However, correlationwith time zero biopsies does suggest that values were rep-resentative. Secondly, nephrotoxic medication could haveinfluenced the severity of AKI and development of chronickidney disease. Our unit avoids nephrotoxic drugs duringthe perioperative period but this does not preclude expo-
sure after discharge. All patients were under regular outpa-tient review and there were no documented drug-inducedadverse renal events. Finally, the lack of pretransplant re-nal impairment in the DCD and DBD patients may raisesome concerns about the generalizability of the resultsfor a standard population of liver transplant recipients. Cer-tainly, the relatively low incidence of chronic kidney diseaseafter transplantation in the control group when comparedwith earlier published series could in part be explained bythis (20,52). Nevertheless, our local practice of allocatingDCD organs to less sick patients, particularly those withmalignancy, is not unique (9).
The findings of our study have important implications forpatient management. Patients who undergo DCD livertransplantation should be considered a high risk group fordeveloping AKI during the immediate postoperative period.Consequently, renal sparing immunosuppression may beappropriate particularly in those individuals with a greatly in-creased AST level. Renal sparing immunosuppression reg-imens may also be beneficial for long-term renal function(26,27). Treatments that target the hepatic ischemia reper-fusion injury and the systemic inflammatory response maybe future therapeutic options that require further study(14,53–56).
In conclusion, in this large single-center case-controlledstudy we have shown for the first time that DCD livertransplantation was associated with greater frequency ofAKI. Importantly, in DCD patients peak perioperative AST,a surrogate marker of hepatic ischemic reperfusion injury,was the only consistent predictor of renal outcomes.
Acknowledgment
We thank James Hodson, statistician, for his helpful advice in the analysisof the data.
Disclosure
The authors of this manuscript have no conflicts of inter-est to disclose as described by the American Journal ofTransplantation.
References
1. Neuberger J. Liver transplantation. QMJ 1999; 92: 547–550.2. Reich DJ, Mulligan DC, Abt PL, et al. ASTS recommended prac-
tice guidelines for controlled donation after cardiac death organprocurement and transplantation. Am J Transplant 2009; 9: 2004–2011.
3. Department of Health. Saving lives, valuing donors: A transplantframework for England. Crown Copyright, 7 July 2003. Available at:http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4061382.pdf. AccessedDecember 10, 2011.
4. Annual Report of the U.S. Organ Procurement and Transplanta-tion Network and the Scientific Registry of Transplant Recipients:
American Journal of Transplantation 2012; 12: 965–975 973

Leithead et al.
Transplant data 1999–2008. U.S. Department of Health and Hu-man Services, Health Resources and Services Administration,Healthcare Systems Bureau, Division of Transplantation, Rockville,MD.
5. Gelder FV, Manyalich M, Nanni Costa A, Paez G. 2009 Internationaldonation and transplantation activity IRODaT prelimary data. Or-gans Tissues Cells 2010; 13: 5–8.
6. Activity Report 2009/10. NHS Blood and Transplant, NationalHealth Service. Available at: http://www.uktransplant.org.uk/ukt/statistics/transplant_activity_report/current_activity_reports/ukt/activity_report_2009_10.pdf. Accessed December 10, 2010.
7. Pine JK, Aldouri A, Young AL, et al. Liver transplantation followingdonation after cardiac death: An analysis using matched pairs.Liver Transpl 2009; 15: 1072–1082.
8. de Vera ME, Lopez-Solis R, Dvorchik I, et al. Liver transplantationusing donation after cardiac death donors: Long-term follow-upfrom a single center. Am J Transplant 2009; 9: 773–781.
9. Jay C, Skaro A, Ladner D, et al. A comprehensive risk assess-ment of mortality following donation after cardiac death livertransplant—an analysis of the National Registry. J Hepatol 2011;55: 808–813.
10. Jay CL, Lyuksemburg V, Ladner DP, et al. Ischemic cholangiopathyafter controlled donation after cardiac death liver transplantation:A meta-analysis. Ann Surg 2011; 253: 259–264.
11. Monbaliu D, Crabbe T, Roskams T, Fevery J, Verwaest C, PirenneJ. Livers from non-heart-beating donors tolerate short periods ofwarm ischemia. Transplantation 2005; 79: 1226–1230.
12. Mathur AK, Heimbach J, Steffick DE, Sonnenday CJ, GoodrichNP, Merion RM. Donation after cardiac death liver transplantation:Predictors of outcome. Am J Transplant 2010; 10: 2512–2519.
13. Foley DP, Fernandez LA, Leverson G, et al. Biliary complicationsafter liver transplantation from donation after cardiac death donors:An analysis of risk factors and long-term outcomes from a singlecenter. Ann Surg 2011; 253: 817–825.
14. Aldrighetti L, Pulitano C, Arru M, et al. Impact of preoperativesteroids administration on ischemic-reperfusion injury and sys-temic responses in liver surgery: A prospective randomized study.Liver Transpl 2006; 12: 941–949.
15. Monbaliu D, van Pelt J, De Vos R, et al. Primary graft nonfunc-tion and Kupffer cell activation after liver transplantation from non-heart-beating donors in pigs. Liver Transpl 2007; 13: 239–247.
16. Arranz Duran J, Arteaga Gonzalez A, Dominguez Garcia D, et al.Variation in the levels of inflammatory cytokines depending onischemic time: Effects on respiratory variables. Transpl Proc 2009;41: 980–982.
17. Bone RC. Toward a theory regarding the pathogenesis of the sys-temic inflammatory response syndrome: What we do and do notknow about cytokine regulation. Crit Care Med 1996; 24: 163–172.
18. O’Riordan A, Wong V, McQuillan R, McCormick PA, Hegarty JE,Watson AJ. Acute renal disease, as defined by the RIFLE criteria,post-liver transplantation. Am J Transplant 2007; 7: 168–176.
19. Chen J, Singhapricha T, Hu KQ, et al. Post liver transplant acuterenal injury and failure by the RIFLE criteria in patients with normalpretransplant serum creatinine concentrations: A matched study.Transplantation 2011; 91: 348–353.
20. Ojo AO, Held PJ, Port FK, et al. Chronic renal failure after trans-plantation of a nonrenal organ. N Engl J Med 2003; 349: 931–940.
21. Glanemann M, Mangrehr JM, Stange BJ, et al. Clinical implicationsof hepatic preservation injury after adult liver transplantation. AmJ Transpl 2003; 3: 1003–1009.
22. Wan L, Bagshaw S, Langenberg C, et al. Pathophysiology of septicacute kidney injury: What do we really know? Crit Care Med 2008;36(Suppl 4): S198–S203.
23. van Kuikj J, Flu W, Chonchol M, et al. Temporary peri-operativedecline of renal function is an independent predictor for chronickidney disease. Clin J Am Soc Neph 2010; 5: 1198–1204.
24. Wald R, Quinn RR, Luo J, et al. Chronic dialysis and death amongsurvivors of acute kidney injury requiring dialysis. JAMA 2009;302: 1179–1185.
25. Basile SP, Donohoe D, Roethe K, Osborn JL. Renal ischemic injuryresults in permanent damage to perirubular capillaries and influ-ences long-term function. Am J Physiol Renal Physiol 2001; 281:F887–F899.
26. Neuberger JM, Mamelok PN, Prienne J, et al for the ReSpECTStudy Group. Delayed introduction of reduced-dose tacrolimus,and renal function in liver transplantation: The ReSpECT study.Am J Transpl 2009;9:327–336.
27. Boudjema K, Camus C, Saliba F, et al. Reduced-dose tacrolimuswith mycophenolate mofetil versus standard-dose tacrolimus inliver transplantation: A randomized study. Am J Transplant 2011;11: 965–976.
28. Feng S, Goodrich NP, Bragg-Gresham JL, et al. Characteristicsassociated with liver graft failure: The concept of a donor riskindex. Am J Transplant 2006; 6: 783–790.
29. Arroyo V, Gines P, Gerbes AL, et al. Definition and diagnosticcriteria of refractory ascites and hepatorenal syndrome in cirrhosis.Hepatology 1995; 23: 164–176.
30. European Association for the Study of the Liver. EASL clinical prac-tice guidelines on the management of ascites, spontaneous bac-terial peritionitis, and hepatorenal syndrome in cirrhosis. J Hepatol2010; 53: 397–417.
31. United Network for Organ Sharing (UNOS). MELD/PELD cal-culator documentation. Available at: http://www.unos.org/docs/MELD_PELD_Calculator_Documentation.pdf. Accessed Decem-ber 10, 2010.
32. Barber KM, Pioli SE, Blackwell JE, Collett D, Neuberger JM, Gim-son AE. Development of a UK score for patients with end-stageliver disease [abstract]. Hepatology 2007; 46: 510A.
33. Bellomo R, Ronco C, Kellum JA, et al. Acute renal failure, defini-tion, outcome measures, animal models, fluid therapy and infor-mation technology needs: The Second International ConsensusConference of the Acute Dialysis Quality Initiative (ADQI) Group.Crit Care 2004; 8: R204–212.
34. NKF K/DOQI Clinical Practice Guidelines for Chronic Kidney Dis-ease: Evaluation, Classification, and Stratification; Guideline 1:Definition and stages of chronic kidney disease. New York: Na-tional Kidney Foundation; 2002.
35. Gonwa TA, Jennings L, Mai ML, Stark PC, Levey AS, KlintmalmGB. Estimation of glomerular filtration rates before and afterliver transplantation: Evaluation of current equations. Liver Transpl2004; 10: 301–309.
36. D’Agostino RB. Propensity score methods for bias reduction in thecomparison of a treatment to a non-randomised control group. StatMed 1998; 17: 2265–2281.
37. Weitzen S, Lapane KL, Toledano AY, Hume AL, Mor V. Principlesfor modelling propensity scores in medical research: A systemicliterature review. Pharmacoepidemiol Drug Saf 2004; 13: 841–853.
38. Gaffey MJ, Boyd JC, Traweek ST, et al. Predicive value of intraop-erative biopsies and liver function tests for preservation injury inorthoptic liver transplantation. Hepatology 1997; 25: 184–189.
39. Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis.Hepatology 2008; 48: 2064–2077.
40. Charlton MR, Wall WJ, Ojo AO, et al. Report of the first interna-tional liver transplantation society expert panel consensus confer-ence on renal insufficiency in liver transplantation. Liver Transpl2009; 15: S1–S34.
974 American Journal of Transplantation 2012; 12: 965–975

DCD Liver Transplantation: Renal Outcomes
41. Olyaei AJ, de Mattos AM, Bennett WM. Nephrotoxicity of im-munosuppressive drugs: New insight and preventative strategies.Curr Opin Crit Care 2001; 7: 384–389.
42. Schrier RW, Wang W. Acute renal failure and sepsis. N Engl J Med2004; 351: 159–160.
43. Bonegio R, Lieberthal W. Role of apoptosis in the pathogenesis ofacute renal failure. Curr Opin Nephrol Hypertens 2002; 11: 301–308.
44. Bonventre JV, Weinberg JM. Recent advances in the pathophysi-ology of ischemic acute renal failure. J Am Soc Nephrol 2003; 14:2199–2210.
45. Park SW, Kim M, Brown KM, D’Agati VD, Lee HT. Panethcell-derived interleukin-17A causes multiorgan dysfunction afterhepatic ischemia and reperfusion injury. Hepatology 2011; 53:1662–1675.
46. Cabezuelo JB, Ramirez P, Rios A, et al. Risk factors of acute renalfailure after liver transplantation. Kidney Int 2006; 69: 1073–1080.
47. Paugam-Burtz C, Kavafyan J, Merckx P, et al. Postreperfusion syn-drome during liver transplantation for cirrhosis: Outcome and pre-dictors. Liver Transpl 2009; 15: 522–529.
48. Bellamy MC, Galley HF, Webster NR. Changes in inflammatorymediators during orthoptic liver transplantation. Br J Anaesth1997; 79: 338–341.
49. Laffey JG, Boylan JF, Cheng DC. The systemic inflammatory re-sponse to cardiac surgery: Implications for the anaesthesiologist.Anesthesiology 2002; 97: 215–252.
50. Schiff ER, Sorrell MF, Maddrey WC. Schiff’s Diseases of theLiver 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2003.
51. Maessen JG, Hermens WT, Vork M, Willems GM, Kootstra G.Appearance of enzymes in plasma or urine following renal injury.Nephrol Dial Transplant 1987; 2: 17–21.
52. O’Riordan A, Wong V, McCormick PA, Hegarty JE, Watson AJ.Chronic kidney disease post-liver transplantation. Nephrol DialTransplant 2006; 21: 2630–2636.
53. Kotsch K, Ulrich F, Reutzel-Selke A, et al. Methylprednisolonetherapy in deceased donors reduces inflammation in the donorliver and improves outcome after liver transplantation: A prospec-tive randomized controlled trial. Ann Surg 2008; 248: 1042–1050.
54. Franchello A, Gilbo N, David E, et al. Ischemic precondition-ing (IP) of the liver as a safe and protective technique againstischemia/reperfusion injury. Am J Transplant 2009; 9: 1629–1639.
55. Hilmi IA, Peng Z, Planinsic RM, et al. N-acetylcysteine does notprevent hepatorenal ischemia-reperfusion injury in patients under-going orthoptic liver transplantation. Nephrol Dial Transplant 2010;25: 2328–2333.
56. Lee WM, Hynan LS, Rossaro L, et al. Intravenous N-acetylcysteine improves transplant-free survival in early stage non-acetaminophen acute liver failure. Gastroenterology 2009; 137:856–864.
American Journal of Transplantation 2012; 12: 965–975 975