Embed Size (px)
Citation preview

8/19/2019 Domestic Violence the Medical Forensic Response 2157 7145.1000192
http://slidepdf.com/reader/full/domestic-violence-the-medical-forensic-response-2157-71451000192 1/2
Open AccessConference Proceedings
ForensicResearch
Barefoot and Galvan, J Forensic Res 2013, 4:3
http://dx.doi.org/10.4172/2157-7145.1000192
Volume 4 • Issue 3 • 1000192J Forensic Res
ISSN: 2157-7145 JFR, an open access journal
Domestic Violence: The Medical Forensic ResponseEvangeline Barefoot* and Linda Galvan
Forensic Nurse Examiner, St. David’s HealthCare, USA
*Corresponding author: Evangeline Barefoot, Forensic Nurse Examiner, St.
David’s HealthCare, USA, E-mail: [email protected]
Received July 26, 2013; Accepted August 22, 2013; Published August 27, 2013
Citation: Barefoot E, Galvan L (2013) Domestic Violence: The Medical Forensic
Response. J Forensic Res 4: 192. doi:10.4172/2157-7145.1000192
Copyright: © 2013 Barefoot E, et al. This is an open-access article distributedunder the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
Domestic violence is ofen thought o as physical conflict between
a couple involved in an intimate relationship. In reality domestic violence is much broader in its scope and effect o the community.Domestic violence not only leaves physical and emotional injuries tothe individual involved but it has a ripple effect on all o the memberso the amily. Children and other amily members experience the bandso the ripple with each act. Te Centers or Disease Control reportthat 29% o violence perpetrated against women by a lone offenderis committed by someone they are intimately involved with such asa husband or boyriend [1]. What does a number like 29% representin a single state? According to the exas Council on Family Violence,2011 data, 102 women lost their lives to domestic violence/ trauma.Tere were nearly 180,000 incidences o amily violence (reported),205,793 hotline calls placed and 11,833 adults were sheltered. Nearly37,500 adults were not sheltered but received non-residential care
and 15,674 children required emergency shelter services [2]. Tesenumbers represent only those that are involved in the governmentalsupport system and does not in any way represent those who do not getinvolved with the system. Te issue o domestic violence is not solelya woman’s issue as it is reported that the numbers o men reportingabuse is rising. 7.5% o men report that they have been abused by anintimate partner.
Many times it is the local urgent care center or emergencydepartment that first becomes involved with a victim o domestic
violence. Te patient may present with a wide range o medicalcomplaints such as abdominal pain, headaches, alls o common origin,
various body aches, pain, bruising with inconsistent mechanism oinjury, and anxiety. Depending on the type o violence inflicted the
injuries can appear minor or severe. While hospitals are required toscreen all patients or domestic violence, many emergency departmentsare extremely busy and ofen don’t screen in a manner that is mostconducive to honest answers. Ideally the nurse or doctor speaks withthe patient privately and with patience and concern. When patientsare screen with riends or amily present they are ofen not ready toshare that inormation publicly or the person with them may, in act,be the person causing the abuse. When patients are taken to anotherarea and given privacy, they will be more likely to answer honestly. Ia patient does disclose a history o domestic violence it is importantto determine immediate risk/ danger to patient and children. Whilesome states allow the medical personnel to notiy police i they suspectdomestic violence many only allow reporting without the patientsconsent i children or elderly persons are victims.
Across the nation, ew medical providers have orensic trainingbeyond the most basic o levels. Tis translates to a brie introduction
Abstract
Each year countless numbers of men, women, and children present to emergency rooms and urgent care centers
seeking treatment following acts of domestic violence. Many times law enforcement is not involved until tragedy has
struck. Working with emergency department staff can greatly improve victim outcomes and help law enforcement to
understand why they may not see any visible injuries. Sexual assault, physical abuse, and strangulation are possible
ndings after an episode of domestic violence. Careful documentation of symptoms is one of the most important
measures to note.
during medical school or i they are lucky, a larger exposure during
residency. For registered nurses there is very little on the subject innursing school and much less in clinical rotations. For most providersit is a voluntary course or class that provides them with any orensictraining. Sexual assault nurse examiners and orensic nurses are oneo the most sought afer clinicians when orensic cases are suspected.Te evidence is clear that careul and considerate documentation othe patient’s statements during the history and physical is critical toimproving outcomes both medically and legally. In one case this wasclearly demonstrated. Te patient is Mary. She is in her late 70’s and shepresented to a local ree standing emergency department in a suburbancommunity. She was triaged by a registered nurse and her husband o51 years was at her side. Mary was coming in because she had allenand hurt her hip. Mary’s husband added that she had been alling a lotmore than usual o late. Te nurse noted the concern and completed
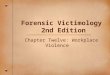
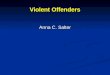
her assessment by asking: “Do you eel sae rom violence in yourhome?” and the nurse chuckled, “I guess you don’t eel to sae i youralling a lot” and went to the next question “As anyone hit, kicked, orslapped you in the past year” and she laughed saying “I eel ridiculousasking such a sweet couple these questions”. She marked no to all thequestions and moved the patient to the exam room. Te nurse gave thedoctor a report and he walked into the room saying “well , I hear you’rea bit accident prone these days”. Mary smiled and remained quiet. Tedoctor examined Mary and ound that she had a number o bruises allover her body in various stages o healing. With each set o bruises,Hank, Mary’s husband, was able to report how and when it happened.Te area on her lef hip was a “missed the chair when she went to sitdown” and the marks behind her ear was a run in with an open cabinetdoor. Each o the explanations made sense. Te doctor never talked toMary away rom Hank and Mary rarely responded to the questions.Mary was given some all saety inormation and a prescription ormild pain medication and sent home with Hank (Figures 1and 2).
Five days later Mary and Hank go to another emergency department

8/19/2019 Domestic Violence the Medical Forensic Response 2157 7145.1000192
http://slidepdf.com/reader/full/domestic-violence-the-medical-forensic-response-2157-71451000192 2/2
Citation: Barefoot E, Galvan L (2013) Domestic Violence: The Medical Forensic Response. J Forensic Res 4: 192. doi: 10.4172/2157-7145.1000192
Page 2 of 2
Volume 4 • Issue 3 • 1000192J Forensic Res
ISSN: 2157-7145 JFR, an open access journal
and this time the triage nurse is a orensic nurse who happens to be onduty that day. Mary and Hank are in triage and the nurse asks Hankto go to registration and get Mary signed in while she takes her vitals.While Hank is gone the nurse goes over the events leading up to the visitand discovers that some o the history given by Mary is not consistent.Te nurse then asks Mary about saety. Mary looks at the nurse orseveral seconds and then looks to the ground. Te nurse repeats thequestion slowly and with great compassion. Mary looks up and says“what does sae in your home eel like?” Te nurse then says, “Sae isno being pushed, hit, talked down to, or hurt in anyway”. Mary thensays, “No, I don’t eel sae in my home”. Te nurse elt that the Hankwould be returning soon so she told Mary they would talk some morelater. Te nurse shared her concerns with the nurse taking over Mary’scare and the doctor. Tey discussed how they would examine Marywithout Hank and together provided saety or Mary in the emergencydepartment. Because Mary was over age 70 and they suspected abuse,they were required to make a report to Adult Protective Services. Teyalso elt that Mary was in immediate danger rom Hank so the policewere also called. Te orensic nurse on call came in and photographedMary’s 39 injuries and documented each o them by size, shape, andcolor. She also documented Mary’s exact statements as to how theyhappened. Te police arrived and took Mary’s and Hanks statementsand Mary was taken to a local shelter until one o her children out o
state could come and provide assistance. Eleven months later Mary’s
case went to trial. Te orensic nurses, the physician, and Mary alltestified about that day. Hank was 81 years old and had recently been
placed in a nursing home at the time o the trial. He was ound guiltyand sentenced to probation or 10 years. Mary moved to Caliornia tolive with her daughter and son-in-law. Te outcome could have been
very different had it not been or the ew changes between the two
emergency departments.
For healthcare providers, utilizing the Forensic Survey [3] asa ollow up to the primary and secondary survey [4] can be o great
benefit. Te primary and secondary surveys include identiyingaddressing all lie-threatening injuries and additional medical findings.Te NCC primary and secondary surveys utilize the alphabet or ease
o recall. Tese surveys cover A thru I o the alphabet and the traumasurvey picks up at J and goes to P. Te orensic survey or healthcareproviders is as ollows: J: Just the acts as spoken by the patient (i the
patient states that she was stabbed by her boyriend, document exactlywhat she says and note the statement in quotes), K: Keep evidence sae,L: Limit contact to those who must be a part o the treatment team and
record who was in the room, M: Maintain integrity when possible bycutting around points o contact with clothes such as gunshot wounds,stab marks, or patterns o injury on clothing, N: No gossip or sharing
o inormation outside the treatment team and law enorcement,O: Observe and document everything you see, smell, or hear romthe patient, and P: Photograph the patient beore, during , and posttreatment when possible to retain visual documentation or case review
as well as investigative evidence.
When healthcare providers are involved in criminal investigationsthey are ofen in an environment that is uncomortable and conusing.
When asked, in court about a patient they cared or 12 or 13 monthsearlier, it is nearly impossible to recall any details that are not in theiremergency department notes. Electronic medical records ofen lack
narrative notes that ully explain the patients’ physical, mental, andcollateral condition. It is important to add such inormation in casesinvolving acts o violence as they will be more likely to end up in a
court o law.
References
1. (2008) Centers for Disease Control and Prevention.
2. (2011) Texas Council on Family Violence.
3. Barefoot E, Evangeline BSN (2007) Forensics in the Hospital Setting: What
Everyone Touching the Patient Should Know. The Journal of Trauma and
Acute Care Surgery 62: S76.
4. Trauma Nurse Core Course (2007) Emergency Nurses Association, Des
Plaines.
Figure 1: Bruises on the patient’s ear.
Figure 2: Area of bruises on the patient’s left hip.
Citation: Barefoot E, Galvan L (2013) Domestic Violence: The Medical
Forensic Response. J Forensic Res 4: 192. doi:10.4172/2157-7145.1000192
Submit your next manuscript and get advantages of OMICS
Group submissions
Unique features:
• User friendly/feasible website-translation of your paper to 50 world’s leading languages• Audio Version of published paper• Digital articles to share and explore
Special features:
• 250 Open Access Journals• 20,000 editorial team• 21 days rapid review process• Quality and quick editorial, review and publication processing• Indexing at PubMed (partial), Scopus, EBSCO, Index Copernicus and Google Scholar etc• Sharing Option: Social Networking Enabled• Authors, Reviewers and Editors rewarded with online Scientifc Credits
• Better discount for your subsequent articles
Submit your manuscript at: http://www.omicsonline.org/submission



















![Hotline:+49[2157]8186-0 • Fax:+49[2157]818650 Alben](https://img.dokumen.tips/doc/110x75/6169cc4911a7b741a34b79da/hotline4921578186-0-fax492157818650-alben-.jpg)






