Embed Size (px)
Citation preview

Preventive Medicine 42 (2006) 401–408www.elsevier.com/locate/ypmed
Review
Does worry about breast cancer predict screening behaviors?A meta-analysis of the prospective evidence
Jennifer L. Hay a,⁎, Kevin D. McCaul b, Renee E. Magnan b
a Department of Psychiatry and Behavioral Sciences, Memorial Sloan-Kettering Cancer Center, 641 Lexington Avenue, New York, NY 10022, USAb North Dakota State University, Fargo, ND 58105, USA
Available online 19 April 2006
Abstract
Objective. Many women worry about the possibility of developing breast cancer, but there is conflicting evidence concerning whether cancerworry acts as a facilitator or inhibitor of breast cancer screening.
Method. We conducted a meta-analysis of 12 prospective studies that measured worry about breast cancer at baseline and subsequent breastself-examination (BSE) or mammography utilization among 3342 high-risk and general population women.
Results. The data consistently show that breast cancer worry has a small but reliable (r = 0.12) association with breast cancer screeningbehavior, such that greater worry predicts a greater likelihood of screening. We also found that the means for breast cancer worry were consistentlyin the lower third of the scales, despite differences in measurement approaches, sample utilization, or the date that the study was conducted.
Conclusion. The meta-analysis supports the contention that breast cancer worry may motivate screening behavior, and that high levels of breastcancer worry are uncommon.© 2006 Elsevier Inc. All rights reserved.
Keywords: Affect; Behavioral medicine; Behavioral sciences; Breast cancer; Health behavior; Preventive health services; Mental health; Risk reduction behavior
Contents
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 402Search strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 402Analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 402
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 403Does worry predict screening behavior? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 403
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 405Measuring worry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 405Implications for theory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 405
Conclusions and future research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 406Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 407References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 407
Many women worry about breast cancer, which is hardlysurprising given the attention that advocacy groups, celebrities,
⁎ Corresponding author. Fax: +1 212 888 2584.E-mail address: [email protected] (J.L. Hay).
0091-7435/$ - see front matter © 2006 Elsevier Inc. All rights reserved.doi:10.1016/j.ypmed.2006.03.002
health professionals, and the media have devoted to the disease(Burke et al., 2001; Blanchard et al., 2002). Some researchershave suggested that worry about breast cancer may havebenefits, prompting women to engage in self-protectivebehaviors such as breast cancer screening (Diefenbach et al.,1999; McCaul et al., 1996a,b). Other researchers, however,

402 J.L. Hay et al. / Preventive Medicine 42 (2006) 401–408
have proposed that worry about breast cancer is problematic,both because of the distress it causes individuals and alsobecause it causes screening avoidance (Kash et al., 1992; Kash,1995; Lerman et al., 1994).
Research conducted over the past 15 years has producedcontradictory evidence concerning whether cancer worryworks to facilitate or inhibit breast cancer screening, withevidence supporting both relationships (Consedine et al.,2004; Hay et al., 2005). These conflicting empirical findingscould be due partly to the multiple, unreconciled methods ofdefining and measuring cancer worry in the researchliterature, and partly to a preponderance of cross-sectionalstudies that measure cancer worry and screening adherence atthe same time, see reviews by Consedine et al. (2004) andHay et al. (2005).
An additional research strategy that may help resolve theseconflicting findings is meta-analysis. Despite the multiplemeasurement strategies, different research designs, diverse partic-ipant samples, and different screening outcomes used in thisliterature, the literature has grown sufficiently that we can ex-amine the findings quantitatively. The current paper contributes tothis literature by examining the direction and effect strength of theprospective evidence connecting cancer worry to subsequentbreast cancer screening.
Approximately 60 studies to date test the cross-sectionalrelationship between cancer worry and cancer screening(Consedine et al., 2004; Hay et al., 2005) and this literatureprovides evidence of significant positive and negative relation-ships between these factors. Because these studies assesscancer worry and screening behavior on one occasion only,they cannot be used to determine whether cancer worry hasinfluenced screening level, and/or whether completion ofscreening has influenced cancer worry. Indeed, both relation-ships may function simultaneously, with cancer worry facilitat-ing completion of screening, and screening immediately decreasingworry for some amount of time. As such, cross-sectional studies areinadequate to test any theories proposing that cancer worry (acause) influences subsequent breast cancer screening (an effect;Brewer et al., 2004). Therefore, we limited our meta-analytic studyto only prospective studies in which screening measures followedworry assessment.
1 Coding categories included study design, whether the dependent variablewas behavioral (as opposed to intentions), whether the bivariate, multivariate,or both relationships between cancer worry and screening were reported,recruitment rate, demographic descriptive data of the sample, method ofrecruitment, time interval between assessments, prospective retention rate,nature of the behavioral assessment (self-report, medical chart review), percentof sample screened, cost of screening reported, actual wording of behavioraloutcome measurement question, response categories provided, nature of cancerworry questions, number of items, response categories provided, distribution ofworry responses, statistics for bivariate, multivariate relationships betweencancer worry and mammography and BSE, respectively, and sample size usedfor each analysis.2 It is worth noting that all of the tests for homogeneity would be
nonsignificant were it not for the study conducted by Andrykowski et al.(2001), a point to which we return in the discussion.
Method
Search strategy
We searched for studies that included (1) a prospective design, (2) a breastcancer screening measure, and (3) measures of worry or anxiety about cancer.We comprehensively searched three computerized databases from theirinception through January 2006 and reviewed all empirical findings concerningcancer worry as a predictor of subsequent breast cancer screening behaviors. Thedatabases were as follows: PREMEDLINE and MEDLINE (from 1966),CANCERLIT (from 1975), and PsycINFO from (1872) using the key wordcommand and the search terms cancer worry, cancer worries, worry aboutcancer, concerns about cancer, cancer fear, fear of cancer, anxiety about cancer,cancer anxiety, cancer avoidant thoughts, cancer intrusive thoughts, distressabout cancer, cancer-related distress, or cancer-specific distress. We did notinclude assessments of generalized worry or anxiety, or worry about thescreening test itself, such as worries that the screening procedure would be
painful or embarrassing or that it would produce a cancer diagnosis (Bastani etal., 1994). Otherwise, we were inclusive concerning measures reflectingworries, fear, distress, or concerns about cancer, given that cancer worry hasbeen broadly defined in health behavior theories and in the cancer preventionand control literature as an emotional reaction to the threat of cancer, distinctfrom health cognitions. Common measurement strategies for cancer worryinclude cancer anxiety, fear of cancer, cancer-related distress, cancer-specificdistress, as well as cancer worry (Hay et al., 2005).
In a second search, we generated published articles for breast cancerscreening methods including breast cancer screening, breast self-examination,clinical breast examination, and mammography screening. We used the combinecommand to locate articles that included key words from each of the twosearches (cancer worry term, breast cancer screening modality). We thenreviewed all abstracts identified in the search, with the exception of dissertationabstracts and non-English articles. We also examined the reference lists from allthe collected articles. We approached the authors of four papers via e-mail toobtain data that were not reported in the published work. Three of those authorswere able to provide relevant data, so they were included in the meta-analysis.Although recent evidence indicates that BSE does not reduce breast cancermortality or morbidity (Thomas et al., 2002), we included BSE as a breast cancerscreening outcome because many women think of BSE as a meaningfulprocedure for breast cancer screening. Moreover, the extensive literatureexamining psychosocial predictors of BSE is theoretically relevant to otherindividually initiated screening modalities, such as testicular or skin self-examinations. We sought to include clinical breast examination as an additionalscreening outcome and found only one prospective study that reported thisoutcome (Andrykowski et al., 2001). We excluded one article (Sutton et al.,1994) that reported only a curvilinear relationship (overall chi-square statistic)between cancer worry and mammography screening because the authors did notreport any effect for the linear relationship. Our search resulted in 12 eligiblestudies for the meta-analysis.
Analyses
The first and third authors coded all articles,1 and disagreements were laterresolved by all three authors. As recommended by Rosenthal (1984), all sta-tistics were converted to Pearson's r as the effect size for each study.2 Eachstatistic used was a univariate statistic that was unconditional on other potentialcovariates of the worry–screening relationship. For any study that reportedmultiple measures of worry but used the same screening method, average effectsizes across worry measures were computed (McCaul et al., 1998; Schwartz etal., 2003). For computing the overall effect size, we also computed an averagefor McCaul et al. (1996a,b), who used a single measure of worry but twoscreening methods (BSE and mammography). The individual effect sizesreported for the two screening methods included the McCaul et al. (1996a,b)data for both BSE and mammography. Finally, we computed the effect size forCalnan (1984) using the P value because 4 degrees of freedom were reportedalong with the chi-square. Transformations produced from a chi-square requiredegrees of freedom equal to 1.
For all average effect size computations, we converted each study effectsize, r, to Fisher's z. We pooled effect sizes by calculating an average z

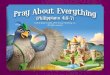
Fig. 1. Mean worry levels across studies. Note: *Mean computed from study results. **Median reported. IES refers to impact events scale.
3 Lerman et al. (1991a,b) reported an odds ratio (OR) to describe therelationship between worry and mammography screening and we converted ORto r, using the formula: OR − 1 / OR + 1. However, it is known that thistransformation produces an effect size that is larger than it should be (Sheskin,1997).
403J.L. Hay et al. / Preventive Medicine 42 (2006) 401–408
across studies and then converted the average z back to r for reporting results.Similar computational procedures were used to produce the overall effect sizeacross studies. Four variations of the average effect size were computed: overallunweighted (by sample size), overall weighted, unweighted BSE, andunweighted mammography only. First, unweighted average effect size wascomputed for all 12 studies using the procedure previously described. Second, aweighted overall effect size was calculated for all 12 studies by (a) convertingeach study's r to Fisher's z, (b) weighting the z value by the study sample andcomputing an average z, and (c) transforming the average z back to r. Third, anaverage unweighted effect size was calculated for the five studies that reportedusing BSE as the screening outcome (Audrain et al., 1999; Cameron et al., 1998;McCaul et al., 1996a,b, 1998; Williams and Clarke, 2001). Fourth, an averageunweighted effect size was calculated for the eight studies that reported usingmammography as the screening outcome (Andrykowski et al., 2001; Calnan,1984; Diefenbach et al., 1999; Lerman et al., 1991a,b, 2000; McCaul et al.,1996a,b; Schwartz et al., 2003; Williams-Piehota et al., 2003). We usedunweighted values for the separate analyses of BSE and mammography becauseof the relatively smaller number of studies and a wish to avoid an effect sizedependent on a single study with large N.
Results
Fig. 1 presents the means for the worry measures used in 10of the 12 studies (the means were not reported in the other 2studies). We standardized the scales for comparison acrossstudies by converting them to 10-point scales. As shown, themeans are consistently in the lower third of the scales, with nooutliers among the 10 studies. Thus, the distribution of cancerworry scores is positively skewed in each case, despite dif-ferences in measurement approaches, sample utilization, or thedate that the study was conducted. In short, overall worry levelsare low.
Twelve prospective studies, shown in Table 1, examinedthe relationship between cancer worry and breast cancerscreening in 3342 women. Table 1 also reveals widelydivergent methodologies across studies. Diverse measurementstrategies for cancer worry included face-valid items aboutthe frequency and extent of worries about breast cancer, theRevised Impact of Events scale (RIES; Horowitz et al.,
1979) and the Intrusion subscale of the RIES. Even theseRIES questions diverged in that some assessed intrusive andavoidant ideation about the participant developing cancerherself, having cancer in their family, or having a familymember with breast cancer. Additionally, Lerman's cancerworry scale (Lerman et al., 1991a,b) was utilized. Screeningbehaviors (BSE and mammography) were measured pro-spectively from 1 month to 1 year following the assessmentof worry. The studies utilized diverse samples, includingwomen drawn randomly from the general population andthose at high risk for developing breast cancer, across a wideage range (starting at age 20). The samples primarily, but notexclusively, included Caucasian women. Finally, the datawere collected over approximately 20 years, from 1978 to2001.
Perhaps because of the wide diversity in studies, the effectsizes across the 12 studies were not homogenous. To examinehomogeneity, we conducted chi-square analyses following therecommendation of Rosenthal (1984). These analyses pro-duced a significant chi-square for the overall effect size, χ2
(11) = 26.24, P = 0.006, and for the mammography studies,χ2 (7) = 20.49, P = 0.005. The BSE studies alone compriseda relatively homogenous set, χ2 (4) = 7.05, P = 0.13.3
Does worry predict screening behavior?
With one exception (Andrykowski et al., 2001), all of thestudies listed in Table 1 reported a positive relationship betweencancer worry and screening behavior, with effect sizes rangingfrom 0.02 to 0.31. The exception is the first study listed with

Table 1Studies included in the meta-analysis
Study Worrymeasure
Numberof scaleitems
Behavior N Outcomes (r) Notes Date datacollected
Andrykowskiet al.(2001)
IES-intrusionsubscale
7 “Compliance” with physicianrecommendation (mammogramor clinical breast exam or bothin past year)
103 −0.23 Women were assessed for worryshortly following a breast biopsyfor cancer
1996–1997
Audrainet al.(1999)
IES 15 BSE (improved versus notimproved over 3 monthsto once monthly)
414 0.07 Worry interacted with treatmentsuch that high worriers were morelikely to improve in adherence
1993 ⁎⁎
Calnan(1984)
Concernabout breastcancer
– Attendance at mammographyscreening (yes versus no)
610 0.08 Received mammogram whenattending clinic
1978 ⁎⁎
Cameronet al.(1998)
Worry aboutBreast cancer
3 BSE (rate over the past 3and 6 months)
85 0.23 (3 months),0.29 (6 months)
1987–1988
Diefenbachet al.(1999)
Worry aboutbreast cancer
1 Mammogram(yes versus no in the past year)
213 0.14 High-risk family members of breastand ovarian cancer patients; afterbaseline, given educational program
1996 ⁎
Lermanet al.(1991a,b)
Anxiety aboutfuturemammograms
1 Mammogram(yes versus no in the past year)
236 0.25 1988–1989
Lermanet al.(2000)
IES-intrusionsubscale
7 Mammogram(yes versus no in the past year)
143 0.15 1994–1997
McCaulet al.(1996a,b)
Worry about breastcancer
3 Mammogram(yes versus no in the past year),BSE (BSE rate over the past year;yes versus no in the past month)
353 0.18, 0.13 1993–1994
McCaulet al.(1998)
Worry about breastcancer
4 BSE (typical rate of BSE; monthsBSE was performed over thepast year)
135 0.31 Has self-monitoring worry data(not included here)
1995
IES-intrusionsubscale
7 BSE (typical rate of BSE;months BSE was performedover the past year)
0.24
Schwartzet al.(2003)
IES-intrusionsubscale
7 Mammogram(yes versus no in the past year)
159 0.02 1996 ⁎⁎
breast cancer worry 3 Mammogram(yes versus no in the past year)
-thoughts 0.16-mood 0.08
Williams andClarke(2001)
Worry about Breastcancer
3 BSE (positive, negative,no change over 1 year)
539 0.08 Anxiety data collected only for thosealready doing BSE
1997
Williams-Piehotaet al.(2003)
Worry about Breastcancer
1 Mammogram (yes versus noin the past year)
352 0.13 Tailored message for high/lowneed for cognition
2000 ⁎
IES refers to the Impact of Events Scale.⁎ Date estimated by subtracting 3 years from the publication date.⁎⁎ Date estimated by subtracting 3 years from a previous publication that used the same data.
404 J.L. Hay et al. / Preventive Medicine 42 (2006) 401–408
women who had just had a biopsy to determine if they hadbreast cancer (r = −0.23). Across all the studies, the averageeffect size, weighted for sample size, was r = 0.12, a value thatwas significantly different from 0 (z = 7.40, P b 0.001). Asecond analysis that did not weight for sample size produced anidentical value, r = 0.12, (z = 7.40, P b 0.001).
Given the heterogeneity of the studies, we also computedseparate effect sizes for studies using BSE versus mammogra-phy and for studies using the IES versus other measures ofworry. For the BSE/mammography comparisons, we allowed
one study with both measures to contribute to each effect(McCaul et al., 1996a,b). The unweighted average effect size forBSE was r = 0.17 (z = 5.70, P b 0.001). The unweightedaverage effect size for mammography was r = 0.10 (z = 5.70,P b 0.001). For the IES/worry comparisons, we also allowedtwo studies with both measures to contribute to each effect(McCaul et al., 1998; Schwartz et al., 2003). The unweightedaverage effect size for the IES was very small, r = 0.05 (z = 2.30,P = 0.02). The unweighted average effect size for othermeasures of worry was r = 0.18 (z = 8.12, P b 0.001).

405J.L. Hay et al. / Preventive Medicine 42 (2006) 401–408
Discussion
The meta-analysis supports the contention that breast cancerworry is associated with a stronger likelihood of screening. Thisconclusion holds regardless of how cancer worry is measured orwhether the screening outcome was mammography or BSE.Given the data, we believe that arguments that worry generallyinhibits screening are unsupported. Indeed, the oppositeconclusion better fits the data. Although the worry–screeningrelationship is small in terms of total variance explained, itcould have practical importance in terms of worry increasingscreening. As Rosenthal (1990) has shown, small effects can beimportant when the behavioral outcome has significance forhealth. Using his Binomial Effect Size Display for the presentdata, and the conservative weighted r = 0.12 obtained here,approximately 56% of the women who worry would obtain amammogram compared to 44% of those who do not worry.Such a difference is certainly meaningful for early detection.
The predominantly low levels of cancer worry reported inthese studies provide an additional important piece to thepuzzle. The 3342 women participating in the studies weredrawn from the general population as well as high-risk samples,but the means for cancer worry were always in the lower third ofthe scales, as shown in Fig. 1. Our findings are consistent withevidence drawn from the general population, where two thirdsof women report no worry about breast cancer (Gram andSlenker, 1992; Sutton et al., 1994), and most (70–80%) womenat high risk of ovarian cancer report mild or nonexistent worryabout ovarian cancer (Andersen et al., 2002, 2003, 2004).Overall, the data suggest that high levels of cancer worry areuncommon. Moreover, higher worry levels are not associatedwith reduced screening. Taken together, our findings shouldsoften concerns that cancer worry is generally problematic, evenamong high-risk women (Coyne et al., 2003).
The generality of the worry–behavior association isstrengthened by prospective data obtained for other cancerscreening and genetic testing behaviors. For instance, worrypredicts adherence to fecal occult blood testing for colorectalcancer screening (Myers et al., 1994), greater uptake of anultrasound test that serves as a screening tool for ovarian cancer(Schwartz et al., 1995), genetic testing for breast cancer(Lerman et al., 1999), and attending a screening clinic formelanoma (de Rooij et al., 1997). Although these individualstudies reinforce the current analysis, it is important torecognize that this paper presents the only meta-analysis ex-amining the prospective effect of disease-specific worry on thelikelihood of self-protective health behaviors.
Measuring worry
Although we allowed many operational definitions of “cancerworry” to enter the meta-analysis, we restricted our analysis toworry about cancer as opposed toworry about cancer screening. Inthe only study distinctly assessing both cancer worry and concernsabout positive test findings, Clemow et al. (2000) found that breastcancer worry predicted stronger plans to obtain a mammogram,whereas fear about positive test results was associated with re-
duced mammography intentions. Identification of both constructsas “cancer worry” contributes to the mix of positive and negativerelationships between cancer worry and screening in the literature(Consedine et al., 2004; Hay et al., 2005).
Although all the measures of worry tested here werepositively related to screening, we did observe a smaller effectsize for the studies using the total RIES and the intrusionsubscale (Horowitz et al., 1979) than other measures of cancerworry (r = 0.05 versus 0.18). The RIES was originallyconstructed as a measure of stress reactions after traumaticevents, but in the cancer prevention and control literature, theRIES has become a commonly used measure of the frequencyof intrusive and avoidant thoughts and feelings about cancer inindividuals at increased cancer risk, as well as cancer patientsand survivors (Smith et al., 1999).
Recent reviews show that the RIES and the Intrusionsubscale of the RIES are internally consistent, and they predictsubsequent distress associated with traumatic stressors (Joseph,2000; Thewes et al., 2001). The present meta-analysis, however,indicates that these measures may not adequately assess thecancer worry construct, at least in the general population andnonclinical high-risk samples. We believe further psychometricdevelopment of the RIES and the Intrusion subscale isnecessary and should precede the continued use of this measureto assess cancer worry.
Implications for theory
Two influential theories propose a role for cancer worry ininfluencing health behavior change. Leventhal's self-regulationtheory (Leventhal et al., 2003; Cameron, 1997) hypothesizesthat people concurrently develop two action plans to cope withillness: (1) for managing the objective demands of the illness (orpotential illness) itself and (2) for managing affect associatedwith the illness threat (e.g., cancer worry). These coping effortscan lead an individual to either incorporate the process of copingwith emotional reactions into the objective action plan, or toprioritize coping with emotional reactions over objective coping.Therefore, expectations of the affective outcomes of screeningdrive whether illness worry will impede, or encourage, illnessmanagement. Theoretically, then, beliefs that breast cancerscreening will reduce worry would lead those experiencingcancer worry to get screened; alternatively, beliefs that screeningwould increase worry would lead those experiencing cancerworry to avoid screening. In contrast, low levels of cancer worryshould function to reduce screening adherence. Leventhal'sperspective fits with the notion that worry can have benefits,promoting adaptive information seeking, monitoring, andproblem-focused coping (Davey, 1993; Davey et al., 1992),and our meta-analytic findings support this perspective.
An alternative perspective allows for a worry–screeningrelationship that depends on the intensity of worry, with both verylow and very high worry levels predicted to inhibit screening(Hailey, 1991; Marcus, 1999; Miller et al., 1996). This proposal isalso known as a “curvilinear” or “inverted U-shaped” hypothesisand is prominently embedded within the Cognitive-Social HealthInformation Processing (C-SHIP) model (Miller et al., 1996). In

406 J.L. Hay et al. / Preventive Medicine 42 (2006) 401–408
this model, relevant affective states are broadly defined to includedepression, hopefulness, anger, irritability, and negative feelingsabout the self that become activated in health informationprocessing. High levels of negative affect and anxious arousalprompt maladaptive avoidant ideation that can reduce intentionsto perform the self-protective behavior (e.g., BSE); in contrast,low or nonexistent affect leads to reduced motivation for self-protective behavior. The C-SHIPmodel identifiesmoderate levelsof cancer worry as leading to the highest levels of screening. Itshould be noted that the predictions from the C-SHIP model aresimilar to historical theoretical arguments that fear has acurvilinear relationship to health protective behaviors. The evi-dence for such a relationship is weak; instead, fear typically isassociated with increasing self-protective motivation (Witte andAllen, 2000).
However, one study in the present set of prospective studiesprovides suggestive evidence of a relationship between strongnegative emotionality and lowered interest in screening—arelationship that would support the C-SHIP model. Specifically,Andrykowski et al. (2001) assessed women within the first fewweeks of having a biopsy to determine if they had breast cancer.Approximately one-third of these women failed to follow theirphysician's recommendation to have a mammogram or clinicalbreast exam (or both) during the following 12 months. Comparedto womenwho compliedwith recommendations, the nonadherentgroup was more worried about their risk for breast cancer (asassessed by intrusive thoughts), and these women were alsosignificantly more distressed; for example, the mean depressionlevel of this nonadherent group was centered on “clinicallysignificant” levels (Radloff, 1977; Schulberg et al., 1985). In thisstudy, Andrykowski et al. (2001) may have identified a group thatwas deeply distressed, aside from their levels of breast cancerworry, and such individuals may avoid self-protective behaviorsthat could exacerbate their negative affect.
Despite the suggestive evidence provided by Andrykowskiet al. (2001), the empirical literature on cancer worry and breastcancer screening is insufficient to test the curvilinear hypoth-esis. We were unable to test whether intense worry might inhibitscreening for the following reasons. First, most studiespresented only a Pearson correlation, which is insufficient totest for a curvilinear relationship. One must conduct quadratictests, assess several levels of worry, or at a minimum examinethe scatter plots of bivariate relationships. Second, as depictedin Fig. 1, most women exhibit only mild worry. Therefore,researchers are unlikely to find a curvilinear relationship be-cause so few women actually endorse high absolute levels onthe worry scales. Third, the few individuals at the very highestlevels of cancer worry are also highly anxious, perhaps becausenegative information is more accessible from memory inanxious persons (Butler and Mathews, 1987). Therefore, itwould be difficult to examine the curvilinear relationship evenin the latter cases unless researchers control for general anxiety.
The existence of the curvilinear relationship could beaddressed utilizing naturalistic differences in cancer worryand general anxiety among women drawn from different studypopulations. For example, such a study could include high-riskwomen drawn from a clinical sample who would be more likely
to report moderate to high cancer worry, as well as high andaverage-risk women drawn from the general population(Andersen et al., 2004), with analyses planned specifically totest for the existence of a curvilinear relationship.
We note some limitations of the current study. Mostimportantly, we relied on a restricted set of studies based ontheir prospective design and the presence of an assessment ofbreast-cancer-specific worry or distress. While we feel thisimproves our ability to discern the strength and direction of theeffect of this distress on subsequent breast cancer screening, itlimits our ability to examine age, racial, or sampling differencesin these relationships. We hope the current findings encourageresearchers to examine these intriguing issues.
Conclusions and future research
The hypothesis that cancer worry inhibits breast cancerscreening is not supported by the prospective evidence. Fur-thermore, levels of cancer worry reported in the literature arequite low. Therefore, the scenario of frightened, screening-avoidant women is unfounded, perpetuated more by the mediathan by adequate empirical evidence (Blanchard et al., 2002).We recognize that cases of excessive worry and avoidingscreening do exist, and we do not mean to minimize the problemfor those who are experiencing such distress. Indeed, continuedresearch examining women who are highly distressed aboutbreast cancer is certainly warranted. But from a public healthview, worry does not seem to represent a problem for the publicin general. We should acknowledge, however, that no true ex-perimental evidence is available to confirm the positive worry–screening connection. That is, no investigators have purposelycreated worry in order to test its effects on screening, althoughthat strategy would be the strongest way to test the relationship.Some investigators have tested interventions intended in part toreduce cancer worry; the present analysis suggests that suchtreatments run the risk of also reducing screening levels(Schwartz et al., 1999). Based on the findings reported here,our worries about the detrimental effects of cancer worry areunsupported by the empirical evidence.
What are the most important next steps in this research? Wesuggest that the strongest test of the relationship between breastcancer worry and subsequent breast cancer screening would beprovided by experimental studies. Such studies could randomlyassign women to low, moderate, and high cancer worry inter-vention arms, and examine subsequent screening outcomes. Weargue that empirical levels of cancer worry in the generalpopulation as well as among high-risk women and the theoreticaljustification that it likely acts by serving as a reminder or cue toaction justifies such an approach. Additionally, it may beworthwhile to examine different types of cancer-related affect todetermine under what conditions specific worries about aspectsof mammography, or about positive results that could result frommammography, may discourage screening. Prior experiencewithmammography, whether positive or negative, might be partic-ularly important here. Additionally, clinical breast examinationhas received little attention in the prospective literature andwarrants attention as an important breast cancer screening

407J.L. Hay et al. / Preventive Medicine 42 (2006) 401–408
outcome. Experimental paradigms drawn from the framingliterature (Rothman and Salovey, 1997) may prove useful here.We acknowledge that researchers may be reluctant to implementa research strategy that increases women's breast cancer worries;excluding those women with high levels of general anxiety mayhelp to address this important ethical and clinical concern. Wewould suggest that to the extent that provision of information(about a woman's risk of breast cancer) increases worry to themodest levels uncovered in this study, it is unlikely to inhibit themotivation that women have to seek out screening.
At the present time, approximately 30% of United Stateswomen age 40 and older have not had a mammogram in the past2 years (NHIS Public Use File 2000, 2002). As such, weadvocate for continued innovative examination of instrumental,cognitive, and affective facilitators to mammography screening,including multiple conceptualizations of cancer worry, focusingin particular on those women who have not yet achievedconsistency with their annual mammography.
Acknowledgments
Preparation of the manuscript was supported by NCI GrantK07 CA98106 to Jennifer Hay and NCI Grants R21 CA098962and K05 CA92633 to Kevin McCaul. We would like to thankTanna Mehlhoff, Katie Quinlan, Amy Canevello, SunitaMohabir, and Christopher S. Webster for helping with variousaspects of this review. We also thank Linda Cameron, MichaelDiefenbach, and Victoria White, who kindly conducted addi-tional statistical analyses that were included in this meta-analysis. We also appreciate the input from three anonymousreviewers who provided comments and suggestions that im-proved the manuscript.
References
Andersen, M.R., Peacock, S., Nelson, J., Wilson, S., McIntosh,M., Drescher, C.,Urban, N., 2002. Worry about ovarian cancer risk and use of ovarian cancerscreening by women at risk for ovarian cancer. Gynecol. Oncol. 85, 3–8.
Andersen, M.R., Smith, R., Meischke, H., Bowen, D., Urban, N., 2003. Breastcancer worry and mammography use by women with and without a familyhistory in a population-based sample. Cancer Epidemiol. Biomarkers Prev.12, 314–320.
Andersen, M.R., Nelson, J., Peacock, S., Giedzinska, A., Dresher, C., Bowen,D., Urban, N., 2004. Worry about ovarian cancer risk and use of screeningby high-risk women: how you recruit affects what you find. Am. J. Med.Genet., Part A 129, 130–135.
Andrykowski, M.A., Carpenter, J.S., Studts, J.L., Cordova, M.J., Cunningham,L.L., Mager, W., Sloan, D., Kenady, D., McGrath, P., 2001. Adherence torecommendations for clinical follow-up after benign breast biopsy. BreastCancer Res. Treat. 69, 165–178.
Audrain, J., Rimer, B., Cella, D., Stefanek, M., Garber, J., Pennanen, M.,Helzlsouer, K., Vogel, V., Lin, T.H., Lerman, C., 1999. The impact of a briefcoping skills intervention on adherence to breast self-examination amongfirst-degree relatives of newly diagnosed breast cancer patients. Psychoon-cology 8, 220–229.
Bastani, R., Marcus, A.C., Maxwell, A.E., Das, I.P., Yan, K.X., 1994.Evaluation of an intervention to increase mammography screening in LosAngeles. Prev. Med. 23, 83–90.
Blanchard, D., Erblich, J., Montgomery, G.H., Bovbjerg, D.H., 2002. Read allabout it: the over-representation of breast cancer in popular magazines. Prev.Med. 35, 343–348.
Brewer, N.T., Weinstein, N.D., Cuite, C.L., Herrington, J.E., 2004. Riskperceptions and their relation to risk behavior. Ann. Behav. Med. 27,125–130.
Burke, W., Olsen, A., Pinsky, L., Reynolds, S., Press, N., 2001. Misleadingpresentation of breast cancer in popular magazines. Effect. Clin. Pract. 4,58–64.
Butler, W., Mathews, A., 1987. Anticipatory anxiety and risk perception. Cogn.Ther. Res. 11, 551–565.
Calnan, M., 1984. The health belief model and participation in programmes forthe early detection of breast cancer: a comparative analysis. Soc. Sci. Med.19, 823–830.
Cameron, L.D., 1997. Screening for Cancer: Illness Perceptions and IllnessWorry. Hardwood Academic Publishers, Amsterdam.
Cameron, L.D., Leventhal, H., Love, R.R., 1998. Trait anxiety, symptomperceptions, and illness-related responses among women with breast cancerin remission during a tamoxifen clinical trial. Health Psychol. 17, 459–469.
Clemow, L., Costanza, M.E., Haddad, W.P., Luckmann, R., White, M.J., Klaus,D., Stoddard, A.M., 2000. Underutilizers of mammography screening today:characteristics of women planning, undecided about, and not planning amammogram. Ann. Behav. Med. 22, 80–88.
Consedine, N.S., Magai, C., Krivoshekova, Y.S., Ryzewicz, L., Neugut, A.I.,2004. Fear, anxiety, worry, and breast cancer screening behavior: a criticalreview. Cancer Epidemiol. Biomarkers Prev. 13, 501–510.
Coyne, J.C., Kruus, L., Racioppo, M., Calzone, K.A., Armstrong, K., 2003.What do ratings of cancer-specific distress mean among women at high riskof breast and ovarian cancer? Am. J. Med. Genet., Part A 116, 222–228.
Davey, G., 1993. A comparison of three cognitive appraisal strategies: the roleof threat in devaluation of problem-focused coping. Personality andIndividual Differences 14, 535–546.
Davey, G., Hampton, J., Farrell, J., Davidson, S., 1992. Some characteristics ofworrying: evidence for worrying and anxiety as separate constructs. Pers.Individ. Differ. 13, 133–147.
de Rooij, M.J., Rampen, F.H., Schouten, L.J., Neumann, H.A., 1997. Factorsinfluencing participation among melanoma screening attenders. Acta Derm.Venereol. 77, 467–470.
Diefenbach, M.A., Miller, S.M., Daly, M.B., 1999. Specific worry about breastcancer predicts mammography use in women at risk for breast and ovariancancer. Health Psychol. 18, 532–536.
Gram, I.T., Slenker, S.E., 1992. Cancer anxiety and attitudes towardmammography among screening attenders, nonattenders, and womennever invited. Am. J. Public Health 82, 249–251.
Hailey, B.J., 1991. Family history of breast cancer and screening behavior: aninverted U-shaped curve? Med. Hypotheses 36, 397–403.
Hay, J.L., Buckley, T.R., Ostroff, J.S., 2005. The role of cancer worry in cancerscreening: a theoretical and empirical review of the literature. Psychooncol-ogy 14, 517–534.
Horowitz, M., Wilner, N., Alvarez, W., 1979. Impact of event scale: a measureof subjective stress. Psychosom. Med. 41, 209–218.
Joseph, S., 2000. Psychometric evaluation of Horowitz's Impact of Event Scale:a review. J. Trauma Stress 13, 101–113.
Kash, K.M., 1995. Psychosocial and ethical implications of defining genetic riskfor cancers. Ann. N. Y. Acad. Sci. 768, 41–52.
Kash, K.M., Holland, J.C., Halper, M.S., Miller, D.G., 1992. Psychologicaldistress and surveillance behaviors of women with a family history of breastcancer. J. Natl. Cancer Inst. 84, 24–30.
Lerman, C., Trock, B., Rimer, B.K., Boyce, A., Jepson, C., Engstrom, P.F.,1991a. Psychological and behavioral implications of abnormal mammo-grams. Ann. Intern. Med. 114, 657–661.
Lerman, C., Trock, B., Rimer, B.K., Jepson, C., Brody, D., Boyce, A., 1991b.Psychological side effects of breast cancer screening. Health Psychol. 10,259–267.
Lerman, C., Kash, K., Stefanek, M., 1994. Younger women at increased risk forbreast cancer: perceived risk, psychological well-being, and surveillancebehavior. J. Natl. Cancer Inst. Monogr. 171–176.
Lerman, C., Hughes, C., Benkendorf, J.L., Biesecker, B., Kerner, J., Willison, J.,Eads, N., Hadley, D., Lynch, J., 1999. Racial differences in testingmotivation and psychological distress following pretest education forBRCA1 gene testing. Cancer Epidemiol. Biomarkers Prev. 8, 361–367.

408 J.L. Hay et al. / Preventive Medicine 42 (2006) 401–408
Lerman, C., Hughes, C., Croyle, R.T., Main, D., Durham, C., Snyder, C.,Bonney, A., Lynch, J.F., Narod, S.A., Lynch, H.T., 2000. Prophylacticsurgery decisions and surveillance practices one year following BRCA1/2testing. Prev. Med. 31, 75–80.
Leventhal, H., Brissette, I., Leventhal, E.A., 2003. Observer ratings of healthand sickness: can other people tell us anything about our health that we don'talready know? Health Psychol. 22, 471–478.
Marcus, A.C., 1999. New directions for risk communication research: adiscussion with additional suggestions. J. Natl. Cancer Inst. Monogr. 35–42.
McCaul, K.D., Reid, P.A., Rathge, R., Martinson, B., 1996a. Does concernabout breast cancer inhibit or promote breast cancer screening? Basic Appl.Soc. Psychol. 18, 183–194.
McCaul, K.D., Schroeder, D.M., Reid, P.A., 1996b. Breast cancer worry andscreening: some prospective data. Health Psychol. 15, 430–433.
McCaul, K.D., Branstetter, A.D., O'Donnell, S.M., Jacobson, K., Quinlan, K.B.,1998. A descriptive study of breast cancer worry. J. Behav. Med. 21,565–579.
Miller, S.M., Shoda, Y., Hurley, K., 1996. Applying cognitive–social theory tohealth-protective behavior: breast self-examination in cancer screening.Psychol. Bull. 119, 70–94.
Myers, R.E., Ross, E., Jepson, C., Wolf, T., Balshem, A., Millner, L., Leventhal,H., 1994. Modeling adherence to colorectal cancer screening. Prev. Med. 23,142–151.
National Health Interview Survey Public Use File (2000), 2002. National HealthInterview Survey Public Use File (2000). National Center for HealthStatistics, Centers for Disease Control and Prevention.
Radloff, L.S., 1977. The ces-d scale: a self-report depression scale for researchin the general population. Appl. Psychol. Meas. 1, 385–401.
Rosenthal, O., 1984. Parametric measures of effective size. In: Cooper, H.,Hedges, L.V. (Eds.), The Handbook of Research Synthesis. Russell SageFoundation, New York, pp. 231–244.
Rosenthal, O., 1990. How are we doing in soft psychology? Am. Psychol. 45,775–777.
Rothman, A.J., Salovey, P., 1997. Shaping perceptions to motivate healthybehavior: the role of message framing. Psychol. Bull. 121, 3–19.
Schulberg, H.C., Saul, M., McClelland, M., Ganguli, M., Christy, W., Frank, R.,1985. Assessing depression in primary medical and psychiatric practices.Arch. Gen. Psychiatry 42, 1164–1170.
Schwartz, M., Lerman, C., Daly, M., Audrain, J., Masny, A., Griffith, K., 1995.Utilization of ovarian cancer screening by women at increased risk. CancerEpidemiol. Biomarkers Prev. 4, 269–273.
Schwartz, M.D., Rimer, B.K., Daly, M., Sands, C., Lerman, C., 1999. Arandomized trial of breast cancer risk counseling: the impact on self-reportedmammography use. Am. J. Public Health 89, 924–926.
Schwartz, M.D., Taylor, K.L., Willard, K.S., 2003. Prospective associationbetween distress and mammography utilization among women with a familyhistory of breast cancer. J. Behav. Med. 26, 105–117.
Sheskin, D., 1997. Handbook of Parametric and Nonparametric StatisticalProcedures. CRC Press, Boca Raton, FL.
Smith, M.Y., Redd, W.H., Peyser, C., Vogl, D., 1999. Post-traumatic stressdisorder in cancer: a review. Psychooncology 8, 521–537.
Sutton, S., Bickler, G., Sancho-Aldridge, J., Saidi, G., 1994. Prospective studyof predictors of attendance for breast screening in inner London. J.Epidemiol. Commun. Health 48, 65–73.
Thewes, B., Meiser, B., Hickie, I.B., 2001. Psychometric properties of theImpact of Event Scale amongst women at increased risk for hereditary breastcancer. Psychooncology 10, 459–468.
Thomas, D.B., Gao, D.L., Ray, R.M., Wang, W.W., Allison, C.J., Chen, F.L.,Porter, P., Hu, Y.W., Zhao, G.L., Pan, L.D., Li, W., Wu, C., Coriaty, Z.,Evans, I., Lin, M.G., Stalsberg, H., Self, S.G., 2002. Randomized trial ofbreast self-examination in Shanghai: final results. J. Natl. Cancer Inst. 94,1445–1457.
Williams, T., Clarke, V.R.B., 2001. Effects of message framing on breast-cancer-related beliefs and behaviors: the role of mediating factors. J. Appl. Soc.Psychol. 31, 925–950.
Williams-Piehota, P., Schneider, T.R., Pizarro, J., Mowad, L., Salovey, P., 2003.Matching health messages to information-processing styles: need forcognition and mammography utilization. Health Commun. 15, 375–392.
Witte, K., Allen, M., 2000. A meta-analysis of fear appeals: implications foreffective public health campaigns. Health Educ. Behav. 27, 591–615.