Embed Size (px)
Citation preview
This section is filled with tips and tools to make documenting shots a more accurate, less complicated task.
Overview of this section:
Best Practices Checklist: Documenting Shots
Why Document Shots
How to Document Shots
Where to Document Shots
Documenting for Child Care and School
Key Resources for Documenting Shots
Remember:"If it isn't
documented, it isn't done!"
Who to CallMIIC Help Desk
651-201-5503 800-657-3970
Minnesota Immunization Program For Minnesota specific issues (e.g. Minnesota school law)
800-657-3970651-201-5503
181July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize
Documenting ShotsIt would be much easier if we all did it the same way!

How to document shots � We train our staff on what immunization
documentation is essential and required by law.
� We keep accurate, readable, up-to-date immunization records.
� We participate in the Minnesota Immunization Information Connection (MIIC) to ensure vaccination records are available.
Where to document shots � We always update the patient’s personal
immunization record with information on the vaccines we administer.
� We update the patient immunization record with vaccines received at other clinics, when we have appropriate documentation.
� We make sure patients don't leave without a personal immunization record that contains their immunization history.
� If we don't give a vaccine when it's due, we document the reason why in the patient’s chart.
Documenting for child dare and school � We train staff on documentation required
for child care and school under Minnesota's immunization law.
Best Practices Checklist: Documenting ShotsThe information in this checklist will be covered in more detail throughout this section.
182 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011
Why records are importantWritten or electronic documentation is the only way to make sure your patient:
y Receives the shots he or she needs at the recommended age and intervals. y Isn't over-vaccinated – which is not only costly but painful. y Has the shots needed for child care and school, or for a job or international
travel.
What immunization information is needed or required?Every time you give an immunization, certain information must be documented in the patient's immunization record – either because it is required by federal law or it is necessary to document administration of a prescribed drug (e.g., vaccines). See the table Documenting Vaccine Information on pages 184-185. Additional documentation may be required by state regulation or your facility. Be sure your facility has a written policy that describes what documentation is necessary and where it should be documented.
Required by federal lawFederal law requires you to document the following information as part of the National Childhood Vaccine Injury Act when you administer recommended vaccines to children as well as adults; see Immunization Laws on page 203
y Date vaccine given y Date of publication of the Vaccine Information Statement (VIS) (see
Instructions for the Use of Vaccine Information Statements on page 143.) y Date the VIS was given to the patient (or parent/legal guardian) y Manufacturer and lot number of vaccine y Name, title, and clinic address (location where immunization information will
be stored) of the individual who administered the vaccine
Essential to documentAs a best practice for documenting immunizations, the following additional information is essential to document:
y Vaccine type y Route and site of administration y Dosage y History of a vaccine reaction y Contraindications y Patient's date of birth
Why Document
Shots
How to Document
Shots
183July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize

How to Document Shots
184 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011
Documenting Vaccine InformationHow to record ... Guideline Example(s)
Required by federal law
Date vaccine given Use MM/DD/YYYY. 06/24/2010
Date on VIS Document the month, day, and year found on the VIS itself; use MM/DD/YYYY. 08/10/2010
Date VIS given to patient
Document the month, day, and year the VIS was given to the parent (or vaccinee); use MM/DD/YYYY.
10/10/2010
Vaccine manufacturer
Use 3-character abbreviation; these codes are universal and the same codes used by MIIC.
MSD for Merck & Co, Inc. See Vaccine Manufacturers for Selected Childhood and Adult Vaccines on page 201.
Vaccine lot number
Indicate the lot number as printed on the vial, syringe, or box. For combination vaccines use the lot number on the box; it is linked to the vaccine diluent and powder.
470-5275160C9
Person administering vaccine
Document name and title of person administering vaccine. Mary Jones, RN
Document the address of the clinic where the vaccine was administered.
Main St. Clinic, 1111 Main St., City, MN 55555
Essential to record
Vaccine type
Use standardized vaccine abbreviations. Hib, HepB, DTaP (See table on page 199.)
Use numbers or additional letters, if necessary, to distinguish different vaccines for the same disease.
Hib(PRP-T), Hib(PRP-OMP), HPV2, HPV4
Note: Indicating the type of vaccine is important when you give DT-pediatric rather than DTaP since children who receive DT-pediatric will be at higher risk of pertussis disease if there is a pertussis outbreak in the community.
Continued

How to Document Shots
185July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize
Essential to record, continued
Combination vaccines
Document a combination vaccine under each specific antigen the vaccine contains; use a hyphen between each antigen.
y Pentacel is DTaP-IPV-Hib. Record it under DTaP, IPV, and Hib.
y Twinrix is hepA-hepB. Record it under both hepatitis A and hepatitis B.
y Pediarix is DTaP-IPV-hep B. Record it under DTaP, IPV, and hepatitis B
Route of administering vaccine
Document method of administration.Intramuscular (IM), subcutaneous (SQ or SC), oral (PO), intranasal (ITN)
Site of administering vaccine
Document location of administration. Right thigh (RT), left thigh (LT), right arm (RA), left arm (LA)
Dosage Document the vaccine dosage. 0.5 mL, 1.0mL
History of vaccine reaction
If a patient experiences a clinically significant or unexpected event after an immunization (even if you are uncertain the vaccine caused it), provide specifics about the event in the patient's chart. See Report adverse reactions to vaccines on page 160.
ContraindicationsIndicate any vaccine contraindications the patient has; provide specifics in the patient's chart. See Contraindications and Precautions to Commonly Used Vaccines on page 135-138.
Patient's date of birth Use MM/DD/YYYY. 04/24/2010

Where to Document Shots
Documenting immunizations in the patient's medical recordWhether you document immunizations on paper or electronically, make sure to include all of the required and essential information. See What immunization information is needed or required? on page 183.
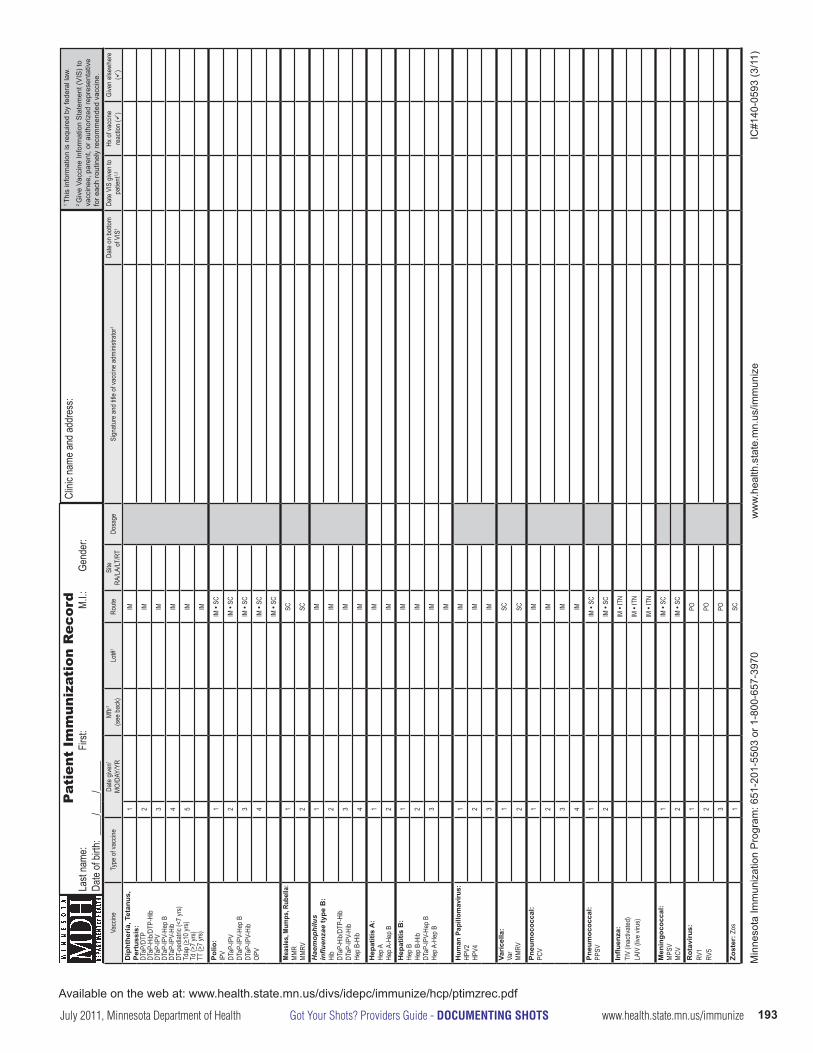
► Paper medical recordsDocument all vaccinations received on the immunization and/or medical record. Consider using the Patient Immunization Record form on pages 193-194. It not only makes it easy to collect all the information you need, but also:
y Accommodates all the legally required immunization data as well as other information you need
y Can be used for both pediatric and adult patients y Has easy-to-follow directions on the back of the form y Has the space to document all immunizations on one page y Has space to document immunizations given elsewhere y Allows notation of any reactions to vaccines y Can be copied and transferred to a patient’s new clinic y Helps Minnesota clinics and others gear up for electronic documentation
► Minnesota Immunization Information Connection (MIIC)Document all immunizations given at your clinic into MIIC, the statewide immunization registry. Make sure you enter all the information required by MIIC and follow up on any alerts you encounter in the process.
Note: In some clinics, you don't need to enter immunization data into MIIC because it is updated via the electronic transfer of the EHR or by the clinics billing department.
► Electronic health records (EHR)Document all immunizations received in the patient’s EHR. Make sure you are familiar with the information required by your EHR system and follow up on any alerts you encounter in the process.
Are you moving toward an electronic health record system but not quite there yet? Consider using the Patient Immunization Record form on pages 193-194 as a template, because it includes all the legally required elements. Don't get stuck having to make changes later to comply with federal law, which can be costly.
Use the tools in your EHR or MIIC or to create lists of patients whose immunizations are overdue and generate recall notices or labels for reminder cards.
If patients have received vaccine elsewhereInclude information regarding vaccines that patients received at other clinics to their medical record. If you don’t have complete information, document at least the date (mm/dd/yyyy) and type of vaccine. The responsibility for maintaining the federally required information is with the clinic that administered the vaccine; see the table What immunization information is needed or required? on page 183.
186 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011

Where to Document Shots
MIIC can help MIIC (Minnesota Immunization Information Connection), the statewide immunization registry, is a program used by health care providers, public health agencies, health plans, and schools to record, monitor, and view immunization information. MIIC uses a confidential, computerized information system to consolidate immunization information.
The benefits of MIIC include:
y Consolidating immunizations a person has received into a single record, no matter where in Minnesota they received the shots.
y Providing an accurate, official copy of a persons immunization history for child care, school, camp enrollment, medical records, or for personal records.
y Ensuring a person's immunizations are up to date by assessing the immunization status and identifying immunizations due or overdue.
y Offering access to a reminder system. y Providing recalls when an immunization has been missed. y Ensuring timely immunization for children whose families move or change
health care providers. y Preventing unnecessary (duplicative) immunization. y Providing easy 24/7 retrieval of immunization information during an
outbreak.
Give the patient a record to take homeYour patients need personal immunization records. Always update the patient’s personal immunization record with information on the vaccines that you administered. Here are some options:
► Paper medical recordsConsider using the Gold Card for personal immunization records. It is beneficial because it: y Can be used for both pediatric and adult patients. y Permits recording of all immunizations throughout a lifetime. y Allows recording of date for the next dose in a series. y Has space to record all information for children enrolling in child care,
school, or college. y Fits in a wallet and is durable (i.e., it’s rip-proof and smear-proof). y Compliments the MIIC record, particularly for providers who don't
participate in MIIC.
► Minnesota Immunization Information Connection (MIIC)Give the patient a printout of their personal immunization record from MIIC.
► Electronic health records (EHR)Give the patient a printout of their personal immunization record from your EHR system.
MIIC is located at https://miic.health.state.mn.us.
If you're not yet
participating, call 1-800-657-3970, or visit
www.health.state.mn.us/divs/idepc/immunize/
registry/index.html to find out how to enroll.
Gold cards are free! Order them by calling
800-657-3970, or 651-201- 5503, or by filling out
the order form at www.health.state.mn.us/
divs/idepc/immunize/ordermat.html
187July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize

Use MIIC and simplify the
work of schools in enforcing the School Immunization Law.
Documenting for Child Care and School
Minnesota's child care / school immunization law and documentationAccurate documentation of immunization(s) helps patients meet Minnesota's child care and school immunization requirements. By law, providers must document either that: y Recommended immunizations have been completed, or y Recommended immunizations have been initiated but are still in process, or y The child has a legal medical exemption to one or more recommended
vaccines. y Note: The patient/parent may also submit documentation of a conscientious
exemption to one or more immunizations.
Troubleshooting documentation for child care and schoolSpecifics of the immunization law and documentation can be complex. Use the table, Getting Your Patient “Immunization Ready” for School on page 189 to guide you.
► Paper medical recordsChild Care and Pupil Immunization Record formThe Child Care Immunization Record form and the Pupil Immunization Record form, see pages 195-198, contain all the essential pieces of documentation needed to satisfy the law, including:
y Spaces to document all vaccines given that are required by law. y A place to document that a required vaccine series has been initiated but
not yet completed. y A place for the provider to indicate a legal medical exemption (e.g.,
contraindication to a vaccine, history of disease). y A place for parents to indicate conscientious objection and have their
signature notarized.
► Minnesota Immunization Information Connection (MIIC)You can use the printed record from MIIC as an official copy of a child's immunization history for child care, school, or camp. Additionally, school nurses can use MIIC to look up students' immunizations and monitor completion of required vaccinations.
► Electronic health records (EHR)You can use the printed record from your EHR as an official copy of a child's immunization history for child care, school, or camp.
More on Minnesota's School Immunization LawFor more information on Minnesota's School Immunization Law (Minnesota Statutes, section 121A.15), see Provider's Quick Reference on Minnesota's Immunization Laws on pages 133-134. Also visit the MDH web site at www.health.state.mn.us/divs/idepc/immunize/laws/index.html.
188 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011

Reminder: Children whose
parents are opposed to immunization can legally
enroll in child care or school. Parents can use the Child Care or Pupil Immunization Record
form to file a legal exemption.
Getting Your Patient “Immunization Ready” for SchoolImmunization status Provider responsibilities
Children who have completed all their recommended immunizations
y Complete, sign (if necessary), and give the parent the Child Care or Pupil Immunization Record form; see pages 195-198, or
y Provide a MIIC printout, or y Complete, sign, and give the parent a
record that includes the dates (mm/dd/yyyy) of vaccines given.
Children who have not completed recommended immunizations
y Complete the Child Care or Pupil Immunization Record form to document vaccines given to date and sign the record indicating when additional dose(s) are due.
Children with a medical contraindication to a vaccine or vaccines
y Complete and sign the portion of the Child Care or Pupil Immunization Record form that verifies a medical exemption.
Children with laboratory evidence of immunity to a disease covered by the law
y Complete and sign the portion of the Child Care or Pupil Immunization Record form that verifies a medical exemption due to history of disease (provide date of diagnosis) or lab evidence of immunity (provide date of testing).
y Note: There is a specific place to document a child’s history of varicella disease.
Children whose parent(s)are conscientiously opposed to immunizations
y Discuss consequences to the child’s health if not immunized: risk of disease to the child, risk of spreading disease to other children, and the possibility of the child being asked to stay home during a disease outbreak.
y If parent/guardian refuses vaccination for a child, it is their responsibility to give the child care or school a signed and notarized statement that specifies which vaccine(s) they oppose. They can use the Child Care or Pupil Immunization Record for this purpose.
189July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize

190 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011

y Patient Immunization Record (MDH) A one-size-fits-all form to document immunizations for infants, children, teens, and adults. www.health.state.mn.us/divs/idepc/immunize/hcp/ptimzrec.pdf
y Child Care Immunization Record (MDH) Form designed to provide child care facilities with immunization information required by Minnesota law.
www.health.state.mn.us/divs/idepc/immunize/laws/childcareimzrec.pdf
y Pupil Immunization Record (MDH) Form designed to provide schools with immunization information required by Minnesota law. www.health.state.mn.us/divs/idepc/immunize/pupilimzrec.pdf
y Data Elements Used in Recording Selected Childhood and Adult Vaccines Table listing vaccine names, trade names, manufacturers, CPT and CVX codes. www.health.state.mn.us/divs/idepc/immunize/registry/hp/vaxcodes.html
y Vaccine Manufacturers for Selected Childhood and Adult Vaccines Table listing vaccine manufacturers and the abbreviations used for electronic data exchange. www.health.state.mn.us/divs/idepc/immunize/registry/hp/vaxcodes.html
Key Resources for Documenting Shots
191July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize

192 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011
Available on the web at: www.health.state.mn.us/divs/idepc/immunize/hcp/ptimzrec.pdf
Pat
ient
Im
mun
izat
ion
Rec
ord
Last
name
:
First:
M.I.:
Gend
er:
Date
of bir
th: _
___/_
___/_
____
_
Clini
c nam
e and
addr
ess:
Vacc
ineTy
pe o
f vac
cine
Date
give
n1
MO/
DAY/
YRM
ftr1
(see
bac
k)Lo
t#1
Rout
eSi
teRA
/LA/
LT/R
TDo
sage
Sign
atur
e an
d titl
e of
vacc
ine a
dmini
strat
or1
Date
on
botto
m
of V
IS1
Date
VIS
give
n to
pa
tient
1,2
Hx o
f vac
cine
reac
tion
(9)
Give
n els
ewhe
re
(9)
Dip
hthe
ria,
Tet
anus
, P
ertu
ssis
:DT
aP/D
TPDT
aP-H
ib/DT
P-Hi
bDT
aP-IP
VDT
aP-IP
V-He
p B
DTaP
-IPV-
Hib
DT-p
ediat
ric (<
7 yr
s)Td
ap (>
10 yr
s)Td
(>7
yrs)
TT (>
7 yr
s)
1IM
2IM
3IM
4IM
5IM IM
Pol
io:
IPV
DTaP
-IPV
DTaP
-IPV-
Hep
BDT
aP-IP
V-Hi
bOP
V
1IM
● SC
2IM
● SC
3IM
● SC
4IM
● SC
IM ●
SC
Mea
sles
, Mum
ps, R
ubel
la:
MM
RM
MRV
1SC
2SC
Hae
mop
hilu
sin
fl uen
zae
type
B:
Hib
DTaP
-Hib/
DTP-
Hib
DTaP
-IPV-
Hib
Hep
B-Hi
b
1IM
2IM
3IM
4IM
Hep
atiti
s A
:He
p AHe
p A-H
ep B
1IM
2IM
Hep
atiti
s B
:He
p B
Hep
B-Hi
bDT
aP-IP
V-He
p B
Hep A
-Hep
B
1IM
2IM
3IM IM
Hum
an P
apill
omav
irus:
HPV2
HPV4
1IM
2IM
3IM
Vari
cella
:Va
rM
MRV
1SC
2SC
Pne
umoc
occa
l:PC
V1
IM
2IM
3IM
4IM
Pne
umoc
occa
l:PP
SV1
IM ●
SC
2IM
● SC
Infl u
enza
:TI
V (in
activ
ated
)LA
IV (l
ive vi
rus)
IM ●
ITN
IM ●
ITN
IM ●
ITN
Men
ingo
cocc
al:
MPS
VM
CV
1IM
● SC
2IM
● SC
Rot
avir
us:
RV1
RV5
1PO
2PO
3PO
Zost
er: Z
os1
SC
1 Th
is in
form
atio
n is
requ
ired
by fe
dera
l law
.2 G
ive
Vacc
ine
Info
rmat
ion
Sta
tem
ent (
VIS
) to
vacc
inee
, par
ent,
or a
utho
rized
repr
esen
tativ
e fo
r eac
h ro
utin
ely
reco
mm
ende
d va
ccin
e.
Min
neso
ta Im
mun
izat
ion
Pro
gram
: 651
-201
-550
3 or
1-8
00-6
57-3
970
ww
w.h
ealth
.sta
te.m
n.us
/imm
uniz
e IC
#140
-059
3 (3
/11)
193July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize

Mak
e th
is re
cord
eas
ily a
cces
sibl
eK
eep
each
pat
ient
’s im
mun
izat
ion
reco
rd w
here
you
can
eas
ily re
view
it
durin
g ea
ch o
ffi ce
vis
it (e
.g.,
the
front
insi
de c
over
of t
he p
atie
nt’s
med
ical
ch
art).
Pa
tient
beh
ind
sche
dule
? Fl
ag th
e re
cord
if th
e pa
tient
is b
ehin
d on
reco
mm
ende
d im
mun
izat
ions
.R
ecor
d ty
pe o
f vac
cine
Be
sure
to in
dica
te th
e ty
pe o
f vac
cine
you
gav
e. T
his
is e
spec
ially
impo
rtant
w
hen
you
give
DT-
pedi
atric
rath
er th
an D
TaP
sinc
e ch
ildre
n w
ho re
ceiv
e D
T-pe
diat
ric w
ill b
e at
hig
her r
isk
of p
ertu
ssis
dis
ease
if th
ere
is a
per
tuss
is
outb
reak
in th
e co
mm
unity
.W
hat i
nfor
mat
ion
is re
quire
d by
fede
ral l
aw?
You
are
requ
ired
by fe
dera
l law
to re
cord
the
follo
win
g in
form
atio
n as
par
t of
the
Nat
iona
l Chi
ldho
od V
acci
ne In
jury
Act
, eve
n if
you
adm
inis
ter a
vac
cine
to
an
adul
t pat
ient
: •
Man
ufac
ture
r and
lot n
umbe
r of v
acci
ne g
iven
.•
Dat
e va
ccin
e gi
ven.
• D
ate
of p
ublic
atio
n of
the
Vacc
ine
Info
rmat
ion
Sta
tem
ent (
VIS
) and
the
date
the
VIS
was
giv
en to
the
vacc
inee
(or p
aren
t or l
egal
repr
esen
tativ
e of
the
min
or c
hild
).•
Nam
e, ti
tle, a
nd a
ddre
ss o
f the
per
son
who
adm
inis
tere
d th
e va
ccin
e.N
ote:
Fed
eral
and
Min
neso
ta la
ws
do n
ot re
quire
writ
ten
info
rmed
con
sent
. H
owev
er, s
ome
clin
ics
may
hav
e th
eir o
wn
polic
y.H
ow to
reco
rd c
ombi
natio
n va
ccin
esR
ecor
d a
com
bina
tion
vacc
ine
unde
r eac
h sp
ecifi
c an
tigen
that
the
vacc
ine
cont
ains
. Use
a h
yphe
n be
twee
n ea
ch a
ntig
en. E
xam
ples
:•
TriH
ibit
is D
TaP
-Hib
. Rec
ord
it un
der b
oth
DTa
P an
d H
ib.
• C
omva
x is
Hep
B-H
ib. R
ecor
d it
unde
r bot
h H
epat
itis
B a
nd H
ib.
• Pe
diar
ix is
DTa
P-IP
V-H
ep B
. Rec
ord
it un
der D
TaP,
IPV,
and
Hep
atitis
B.
How
to re
cord
inje
ctio
n ro
utes
and
site
sTh
e m
ost c
omm
on ro
utes
for v
acci
natio
n ar
e in
tram
uscu
lar (
IM) a
nd
subc
utan
eous
(SC
or S
Q).
Less
freq
uent
rout
es in
clud
e or
al (P
O) a
nd
intra
nasa
l (IT
N).
If th
ere
is m
ore
than
one
cho
ice
for r
oute
, circ
le th
e ro
ute
give
n. S
ites
for i
njec
tions
sho
uld
be n
oted
as
to w
hich
lim
b an
d w
hat s
ide.
Th
ese
incl
ude
right
thig
h (R
T), l
eft t
high
(LT)
, rig
ht a
rm (R
A),
and
left
arm
(L
A).
Hx
of v
acci
ne re
actio
n (h
isto
ry o
f vac
cine
reac
tion)
If th
e pa
tient
has
exp
erie
nced
a c
linic
ally
sig
nifi c
ant o
r une
xpec
ted
even
t af
ter a
n im
mun
izat
ion
(eve
n if
ther
e is
unc
erta
inty
that
the
vacc
ine
caus
ed
the
even
t), p
lace
a 9
in th
e “H
x of
vac
cine
reac
tion”
col
umn.
Pro
vide
mor
e sp
ecifi
cs a
bout
that
eve
nt e
lsew
here
in th
e pa
tient
’s c
hart.
Rep
ort v
acci
ne
reac
tions
to th
e Va
ccin
e A
dver
se E
vent
s R
epor
ting
Sys
tem
(h
ttp://
vaer
s.hh
s.go
v or
800
-822
-796
7).
Tran
sfer
ring
imm
uniz
atio
n in
form
atio
n on
to th
is fo
rmTr
ansf
er v
acci
ne in
form
atio
n th
at p
atie
nts
rece
ive
at o
ther
clin
ics
to th
is
reco
rd. I
f you
don
’t kn
ow a
ll of
the
info
rmat
ion,
reco
rd a
t lea
st th
e da
te (m
o/da
y/yr
) and
type
of v
acci
ne. T
he re
spon
sibi
lity
for m
aint
aini
ng th
e fe
dera
lly
requ
ired
info
rmat
ion
is w
ith th
e cl
inic
that
adm
inis
tere
d th
e va
ccin
e. B
e su
re to
pla
ce a
9 in
the
“Giv
en e
lsew
here
” col
umn.
If a
pat
ient
tran
sfer
s to
an
othe
r clin
ic, p
rovi
de a
pho
toco
py to
the
new
clin
ic.
Use
the
MIIC
regi
stry
to re
cord
and
fi nd
imm
uniz
atio
nsIf
you’
re p
artic
ipat
ing
in th
e M
inne
sota
Imm
uniz
atio
n In
form
atio
n C
onne
ctio
n (M
IIC),
be s
ure
to e
nter
or s
ubm
it da
ta o
n ne
w s
hots
for t
his
patie
nt s
o it
is
avai
labl
e to
oth
ers
who
may
be
givi
ng s
ubse
quen
t dos
es. M
IIC is
loca
ted
at
http
s://m
iic.h
ealth
.sta
te.m
n.us
. If y
ou a
re n
ot y
et p
artic
ipat
ing,
cal
l 80
0-65
7-39
70, o
r vis
it w
ww.
heal
th.s
tate
.mn.
us/im
mun
ize
(clic
k on
“MIIC
R
egis
try”)
to fi
nd o
ut h
ow to
enr
oll.
Man
ufac
ture
rs’ c
odes
Use
the
code
s lis
ted
in th
e ch
art b
elow
to in
dica
te th
e m
anuf
actu
rer o
f the
va
ccin
e. T
hese
are
the
sam
e co
des
used
uni
vers
ally
and
by
the
Min
neso
ta
Imm
uniz
atio
n In
form
atio
n C
onne
ctio
n (M
IIC).
Vacc
ine
Man
ufac
ture
rC
ode
CS
L B
ioth
erap
ies
CS
LG
laxo
Sm
ithK
line
SK
BM
assa
chus
etts
Bio
logi
c La
bsM
BL
Med
Imm
une,
Inc.
M
ED
Mer
ck &
Co.
, Inc
. M
SD
Nov
artis
NO
Vsa
nofi
past
eur I
nc.
PM
CW
yeth
Vac
cine
sW
AL
Your
pat
ient
s ne
ed p
erso
nal i
mm
uniz
atio
n re
cord
car
dsAl
way
s up
date
the
patie
nt’s
per
sona
l im
mun
izat
ion
reco
rd w
ith in
form
atio
n on
th
e va
ccin
es th
at y
ou a
dmin
iste
red.
If y
our c
linic
nee
ds p
erso
nal i
mm
uniz
atio
n re
cord
car
ds, o
rder
the
MD
H G
old
Car
d by
cal
ling
800-
657-
3970
, or 6
51-2
01-
5503
, or b
y fi l
ling
out t
he o
rder
form
at w
ww.
heal
th.s
tate
.mn.
us/im
mun
ize.
How
to u
se M
DH
’s P
atie
nt Im
mun
izat
ion
Rec
ord
form
Imm
uniz
atio
n P
rogr
amP.
O. B
ox 6
4975
St.
Pau
l, M
N 5
5164
-097
565
1-20
1-55
03 o
r 1-8
00-6
57-3
970
ww
w.h
ealth
.sta
te.m
n.us
/imm
uniz
e
Available on the web at: www.health.state.mn.us/divs/idepc/immunize/hcp/ptimzrec.pdf
194 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011

D.If
the
pare
nt/g
uard
ian
cons
cien
tious
ly o
ppos
es im
mun
izat
ions
:
I und
erst
and
that
not
follo
win
g va
ccin
atio
n re
com
men
datio
ns m
ay e
ndan
ger t
he h
ealth
or l
ife o
f my
child
and
oth
ers
that
my
child
mig
ht c
ome
in c
onta
ct w
ith. I
her
eby
certi
fy b
y no
tariz
atio
n th
at:
I am
opp
osed
to a
ll im
mun
izat
ions
.I a
m o
ppos
ed to
onl
y th
e va
ccin
es in
dica
ted.
Vac
cine
(s) I
opp
ose:
Sig
natu
re o
f Par
ent/G
uard
ian
Dat
e
Chi
ld C
are
Imm
uniz
atio
n R
ecor
dbe
fore
IMM
UN
IZAT
ION
HIS
TORY
: Fill
in th
e M
O/D
AY/Y
R in
form
atio
n fo
r chi
ldre
n 2
mon
ths
of a
ge
and
olde
r. If
child
rece
ived
a c
ombi
ned
shot
(lik
e H
ib-h
ep B
), w
rite
the
date
in a
ll th
e bo
xes
that
ap
ply.
Vac
cine
dos
es th
at a
re c
ircle
d
ar
e no
t req
uire
d by
law
.
Dip
hthe
ria, T
etan
us, P
ertu
ssis
(DTa
P)Va
ccin
eD
ose
MO
DAY
YR3
dose
s du
ring
1st y
ear
4th d
ose
at 1
2-18
mon
ths
5th d
ose
at 4
-6 y
ears
or a
t sch
ool e
ntra
nce
1 2 3 4 5Po
lio (I
PV a
nd/o
r OPV
)Va
ccin
eD
ose
MO
DAY
YR3
dose
s at
2-1
8 m
onth
s4th
dos
e at
4-6
yea
rs o
r at s
choo
l ent
ranc
e1 2 3 4
Mea
sles
, Mum
ps, R
ubel
la (M
MR
)Va
ccin
eD
ose
MO
DAY
YRR
equi
red
for c
hild
ren
15 m
onth
s an
d ol
der
Mus
t be
give
n on
or a
fter 1
st b
irthd
ay2nd
dos
e at
4-6
yea
rs
1 2
type
b (H
ib)
Vacc
ine
Dos
eM
OD
AYYR
3-4
dose
s fo
r chi
ldre
n at
2-1
5 m
onth
s1
dose
giv
en a
fter 1
2 m
onth
s or
old
er re
quire
d1
dose
for p
revi
ousl
y un
vacc
inat
ed c
hild
ren
15
-59
mon
ths
Not
indi
cate
d fo
r chi
ldre
n 5
year
s or
old
er
1 2 3 4Va
ricel
la (C
hick
enpo
x)Va
ccin
eD
ose
MO
DAY
YR1st
dos
e be
twee
n 12
-18
mon
ths
2nd d
ose
at 4
-6 y
ears
or a
t sch
ool e
ntra
nce
(req
uire
d fo
r kin
derg
arte
n)
1 2D
isea
se D
ate:
Pneu
moc
occa
l Con
juga
te V
acci
ne (P
CV)
Vacc
ine
Dos
eM
OD
AYYR
2-4
dose
s fo
r chi
ldre
n 2-
24 m
onth
sC
onsi
der f
or u
nvac
cina
ted
child
ren
at 2
4-59
m
onth
s in
chi
ld c
are
Not
indi
cate
d fo
r chi
ldre
n 5
year
s or
old
er
1 2 3 4H
epat
itis
B (H
ep B
)–re
quire
d fo
r kin
derg
arte
nVa
ccin
eD
ose
MO
DAY
YR3
dose
s be
twee
n bi
rth a
nd 1
8 m
onth
s1 2 3
Rot
aviru
sVa
ccin
eD
ose
MO
DAY
YR2-
3 do
ses
betw
een
2 an
d 6
mon
ths
1 2 3Va
ccin
eD
ose
MO
DAY
YR1
dose
ann
ually
for c
hild
ren
6 m
onth
s or
old
er(1
st
1 2H
epat
itis
A (H
ep A
)Va
ccin
eD
ose
MO
DAY
YR2
dose
s se
para
ted
by 6
mon
ths
for c
hild
ren
12
-24
mon
ths
1 2
A. Fo
r chi
ldre
n w
ho a
re 1
5 m
onth
s or
old
er a
nd w
ho h
ave
rece
ived
all
the
imm
uniz
atio
ns
requ
ired
by la
w fo
r chi
ld c
are:
I cer
tify
that
the
abov
e-na
med
chi
ld is
at l
east
15
mon
ths
of a
ge a
nd h
as c
ompl
eted
the
imm
uniz
atio
ns
whi
ch a
re re
quire
d by
law
for c
hild
car
e.
Sign
atur
e of
Par
ent/G
uard
ian
or P
hysi
cian
/Nur
se P
ract
itione
r/Phy
sici
an A
ssis
tant
/Pub
lic C
linic
D
ate
Nam
e:
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
__
Birt
hdat
e: _
____
____
____
____
____
____
_D
ate
of E
nrol
lmen
t: __
____
____
____
____
___
B.Fo
r chi
ldre
n w
ho a
re y
oung
er th
an 1
5 m
onth
s O
R h
ave
not r
ecei
ved
all r
equi
red
imm
uniz
atio
ns:
I cer
tify
that
the
abov
e-na
med
chi
ld h
as re
ceiv
ed th
e im
mun
izat
ions
indi
cate
d. In
ord
er to
rem
ain
enro
lled
this
chi
ld m
ust r
ecei
ve a
ll re
quire
d va
ccin
es w
ithin
18
mon
ths
from
initi
al e
nrol
lmen
t dat
e.
Sign
atur
e of
Phy
sici
an/N
urse
Pra
ctitio
ner/P
hysi
cian
Ass
ista
nt/P
ublic
Clin
ic
Dat
e
SIG
NAT
UR
E(S)
Not
ary
Pub
lic S
tam
pM
inne
sota
Imm
uniz
atio
n P
rogr
am: 6
51-2
01-5
503
or 1
-800
-657
-397
0 (M
DH
, 8/2
011)
C.Fo
r chi
ldre
n w
ho h
ave
a hi
stor
y of
dis
ease
or a
re m
edic
ally
exe
mpt
from
vac
cine
(s):
Th
e fo
llow
ing
imm
uniz
atio
n(s)
are
not
indi
cate
d be
caus
e of
med
ical
reas
ons,
his
tory
of d
isea
se, o
r (S
ee b
elow
for v
aric
ella
dis
ease
.) __
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
Sign
atur
e of
Phy
sici
an/N
urse
Pra
ctitio
ner/P
hysi
cian
Ass
ista
nt
Dat
e
Star
ting
Sept
embe
r 201
0 (B
efor
e Se
ptem
ber 2
010,
a p
aren
t can
sig
n.):
For c
hild
ren
who
are
18
mon
ths
or o
lder
who
hav
e a
hist
ory
of v
aric
ella
dis
ease
: I c
ertif
y th
at v
aric
ella
imm
uniz
atio
n is
not
indi
cate
d fo
r the
abo
ve-n
amed
chi
ld d
ue to
a h
isto
ry o
f va
ricel
la d
isea
se th
at I
have
dia
gnos
ed o
r had
ade
quat
ely
desc
ribed
to m
e by
the
pare
nt to
indi
cate
pa
st v
aric
ella
infe
ctio
n in
___
____
__.
ye
ar
Sign
atur
e of
Phy
sici
an/N
urse
Pra
ctitio
ner/P
hysi
cian
Ass
ista
nt (B
efor
e Se
ptem
ber 2
010,
a p
aren
t can
sig
n.)
Dat
e
Sig
natu
re o
f not
ary
publ
ic
Sub
scrib
ed a
nd s
wor
n to
bef
ore
me
this
___
____
__ d
ay o
f __
____
____
____
____
__, 2
0 __
____
____
.
Available on the web at: www.health.state.mn.us/divs/idepc/immunize/laws/childcareimzrec.pdf
195July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize

Chi
ld C
are
Imm
uniz
atio
n R
ecor
d - I
nstr
uctio
nsbe
fore
a c
hild
atte
nds
child
car
e.W
ho s
houl
d co
mpl
ete
and
sign
this
form
?W
ho s
igns
dep
ends
on
the
child
’s a
ge a
nd s
ituat
ion.
Eith
er th
e pa
rent
/gua
rdia
n,
hi
stor
y.If
the
child
is a
t lea
st 1
5 m
onth
s ol
d an
d ha
s ha
d al
l the
sho
ts re
quire
d by
law,
a
pare
nt o
r gua
rdia
n ca
n si
gn th
e fo
rm in
Sec
tion
A.If
the
child
is y
oung
er th
an 1
5 m
onth
s or
has
not
had
all
the
shot
s re
quire
d by
law,
th
en a
hea
lth c
are
prov
ider
mus
t sig
n in
Sec
tion
B, s
ayin
g th
e ch
ild h
as b
egun
the
requ
ired
shot
s or
can
’t fo
r med
ical
reas
ons.
Star
ting
in S
epte
mbe
r 201
0, if
the
child
is 1
8 m
onth
s or
old
er a
nd h
as h
ad
varic
ella
dis
ease
(chi
cken
pox)
, a h
ealth
car
e pr
ovid
er m
ust s
ign
in S
ectio
n C
. (B
efor
e Se
ptem
ber 2
010,
a p
aren
t can
sig
n.)
If a
pare
nt o
r gua
rdia
n ob
ject
s to
a c
erta
in s
hot o
r all
shot
s, th
e pa
rent
or
guar
dian
mus
t com
plet
e Se
ctio
n D
and
hav
e it
nota
rized
by
a no
tary
pub
lic.
Not
es fo
r Par
ents
1. G
ive
your
chi
ld’s
imm
uniz
atio
n hi
stor
y to
the
child
car
e pr
ovid
er w
hen
you
enro
ll.M
inne
sota
law
(Min
n. S
tat.1
21A.
15) r
equi
res
child
ren
enro
lled
in a
Min
neso
ta
child
car
e to
be
imm
uniz
ed a
gain
st c
erta
in d
isea
ses
or h
ave
a le
gal e
xem
ptio
n.
This
form
is d
esig
ned
to p
rovi
de th
e ch
ild c
are
prov
ider
with
the
info
rmat
ion
re-
quire
d by
law.
Thi
s or
ano
ther
form
doc
umen
ting
imm
uniz
atio
ns o
r an
exem
ptio
n
are
an a
llow
able
form
.2.
Kee
p tr
ack
of y
our c
hild
’s s
hots
, and
tell
your
chi
ld c
are
prov
ider
eac
h tim
e yo
ur c
hild
get
s a
shot
.It
will
save
you
tim
e if
you
keep
a s
hot r
ecor
d fo
r eac
h of
you
r chi
ldre
n. B
e su
re
to h
ave
the
reco
rd u
pdat
ed e
ach
time
your
chi
ld re
ceiv
es a
sho
t.
also
nee
d th
is re
cord
for s
choo
l, ca
mp,
col
lege
, and
if y
ou g
o to
a n
ew d
octo
r or
clin
ic.
3. I
f you
r chi
ld is
not
up
to d
ate
on h
is o
r her
sho
ts, y
ou c
an c
atch
up.
By
law
you
hav
e 18
mon
ths
afte
r enr
ollin
g fo
r you
r chi
ld to
hav
e al
l his
or h
er
Min
neso
ta c
hild
ren
are
still
getti
ng d
isea
ses
like
mea
sles
, mum
ps, a
nd ru
bella
. Th
ese
dise
ases
are
con
tagi
ous.
The
y ca
n sp
read
rapi
dly—
espe
cial
ly a
mon
g gr
oups
of c
hild
ren
who
hav
e no
t rec
eive
d th
eir s
hots
. And
som
e of
them
, lik
e pe
rtuss
is (w
hoop
ing
coug
h), a
re m
uch
mor
e se
rious
for c
hild
ren
than
they
are
fo
r adu
lts. A
s a
pare
nt, y
ou c
an p
rote
ct y
our c
hild
ren
by m
akin
g su
re th
ey g
et a
ll th
eir s
hots
. Mos
t sho
ts a
re d
ue b
y 2
year
s of
age
.4.
If y
our c
hild
has
had
chi
cken
pox,
he
or s
he d
oes
not n
eed
a va
ricel
la s
hot.
But s
tarti
ng in
Sep
tem
ber 2
010,
if th
e ch
ild is
18
mon
ths
or o
lder
and
has
had
va
ricel
la d
isea
se (c
hick
enpo
x), a
hea
lth c
are
prov
ider
mus
t sig
n in
Sec
tion
C.
(Bef
ore
Sept
embe
r 201
0, a
par
ent c
an s
ign.
)
Not
es fo
r Chi
ld C
are
Prov
ider
s1.
mon
ths
of a
ge a
nd o
lder
.W
hen
the
prov
ider
GIV
ES p
aren
ts im
mun
izat
ion
info
rmat
ion
abou
t enr
ollm
ent f
or
child
car
e, th
e pr
ovid
er m
ust u
se th
is fo
rm o
r a s
imila
r for
m a
ppro
ved
by M
DH
as
requ
ired
by la
w.H
owev
er, t
he re
cord
that
is
that
doc
umen
ts im
mun
izat
ions
or a
n
a re
port
prin
ted
off o
f MIIC
(the
sta
te im
mun
izat
ion
regi
stry
) or a
noth
er e
lect
roni
c
a ch
ild e
nrol
ls a
t a y
oung
er a
ge, y
ou m
ust o
btai
n im
mun
izat
ion
info
rmat
ion
whe
n th
ey re
ach
2 m
onth
s of
age
.2.
Kee
p tr
ack
of th
e da
te w
hen
each
chi
ld’s
requ
ired
imm
uniz
atio
ns a
re d
ue
by la
w.
If a
child
is 2
mon
ths
of a
ge o
r old
er a
nd h
as n
ot y
et re
ceiv
ed a
ll th
eir r
equi
red
shot
s, y
ou s
houl
d no
te th
e da
te w
hen
thes
e im
mun
izat
ions
will
be d
ue b
y la
w: 1
8 m
onth
s af
ter t
he c
hild
enr
olls
in y
our f
acilit
y.U
nles
s th
ey a
re o
ther
wis
e ex
empt
, Min
neso
ta la
w re
quire
s pr
esch
oole
rs in
chi
ld
care
to h
ave
shot
s fo
r DTP
, pol
io, M
MR
, PC
V, H
ib, a
nd v
aric
ella
. If t
he c
hild
has
ha
d ch
icke
npox
dis
ease
, he
or s
he d
oes
not n
eed
a va
ricel
la s
hot,
but s
tarti
ng in
Se
ptem
ber 2
010,
they
mus
t hav
e a
heal
th c
are
prov
ider
’s s
igna
ture
to d
ocum
ent
the
year
the
child
had
chi
cken
pox.
Imm
uniz
atio
n ag
ains
t hep
atiti
s A,
hep
atiti
s B,
-
men
ded
for c
hild
ren
in c
hild
car
e.3.
Be
sure
eac
h ch
ild’s
imm
uniz
atio
n hi
stor
y cl
early
indi
cate
s w
heth
er o
r not
th
ey re
ceiv
ed p
ertu
ssis
vac
cine
.D
T do
es n
ot.)
Nat
ionw
ide
ther
e ha
s be
en a
n in
crea
se in
per
tuss
is d
isea
se (w
hoop
ing
coug
h). I
f an
out
brea
k of
per
tuss
is o
ccur
s in
you
r chi
ld c
are
cent
er, y
ou w
ill ne
ed to
be
able
to
qui
ckly
iden
tify
whi
ch c
hild
ren
are
prot
ecte
d an
d w
hich
are
not
.4.
Rem
ind
pare
nts
to im
mun
ize
child
ren
on ti
me.
As a
chi
ld c
are
prov
ider
, you
are
in a
n ex
celle
nt p
ositi
on to
hel
p re
min
d pa
rent
s ab
out i
mm
uniz
atio
ns.
date
, and
regu
larly
rem
ind
pare
nts
whe
n sh
ots
are
due.
Ask
your
loca
l hea
lth d
epar
tmen
t for
an
upda
ted
imm
uniz
atio
n sc
hedu
le e
ach
cale
ndar
yea
r, so
you
will
have
the
late
st in
form
atio
n on
han
d.Q
uest
ions
?If
you
have
a q
uest
ion
abou
t im
mun
izat
ions
, cal
l you
r clin
ic o
r you
r loc
al p
ublic
he
alth
dep
artm
ent.
Imm
uniz
atio
n Pr
ogra
mP.
O. B
ox 6
4975
St. P
aul,
MN
551
64-0
975
651-
201-
5503
or 1
-800
-657
-397
0w
ww.
heal
th.s
tate
.mn.
us/im
mun
ize
IC#1
40-0
163
(MD
H, 8
/201
1)
Available on the web at: www.health.state.mn.us/divs/idepc/immunize/laws/childcareimzrec.pdf
196 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011

Available on the web at: www.health.state.mn.us/divs/idepc/immunize/pupilimzrec.pdf
Pupil Immunization Record FOR SCHOOL USE ONLY( ) Complete; booster required in ___________( ) In process; 8 mos. expires _____________( ) Medical exemption for _________________( ) Conscientious objection for _____________( ) Parental/guardian consent _____________
Minnesota law requires children enrolled in school to be immunized against certain diseases or fi le a legal medical or conscientious exemption (see back for exemption information).Parent: Enter the MONTH, DAY, and YEAR for all vaccines your child received. DO NOT USE (9) or (). Vaccines/doses in shaded boxes are recommended but not required by law.School Personnel: Be sure to initial and date any new information that you add to this form after the parent/guardian submits it. Also, record combination vaccines (e.g., DTaP+HepB+IPV, Hib+HepB) in each applicable space.
Type of Vaccine 1st DoseMo/Day/Yr
2nd DoseMo/Day/Yr
3rd DoseMo/Day/Yr
4th DoseMo/Day/Yr
5th DoseMo/Day/Yr
Diphtheria, Tetanus, and Pertussis (DTap, DTP)
Diphtheria and Tetanus (DT) • for 6-year-olds and younger
Tetanus and Diphtheria (Tdap, Td) • for 7-year-olds and older
Polio (IPV, OPV)
Measles, Mumps, and Rubella (MMR)• minimum age: on or after 1st birthday • required for kindergarten and 7th grade
Hepatitis B (hep B)• required for kindergarten and 7th grade
Varicella (chickenpox)• minimum age: on or after 1st birthday • vaccine or disease history required for kindergarten
and 7th grade
Haemophilus infl uenza type b (Hib)
Meningococcal (MCV, MPSV)
Human Papillomavirus (HPV)
Hepatitis A (hep A)
Developed by the Minnesota Department of Health - Immunization Program (5/11) #140-0155www.health.state.mn.us/immunize Page 1 of 2
Student Name _________________________________________________
Birthdate _____________________Student Number __________________
1. Choose one of the following to indicate student’s immunization status and the source of the information above:A. I certify that this student has received all immunizations required by law.
____________________________________________________________________________________________Signature of parent/guardian or physician/public clinic Date
B. I certify that this student has received at least one dose of vaccine for diphtheria, tetanus, and pertussis (if age-appropriate), polio, hepatitis B (K and 7th), varicella (K and 7th), measles, mumps, and rubella and will complete his/her diphtheria, tetanus, pertussis, hepatitis B, and/or polio vaccine series within the next 8 months. The dates on which the remaining doses are to be given are:
____________________________________________________________________________________________
____________________________________________________________________________________________Signature of physician/public clinic Date
–OVER–
197July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize
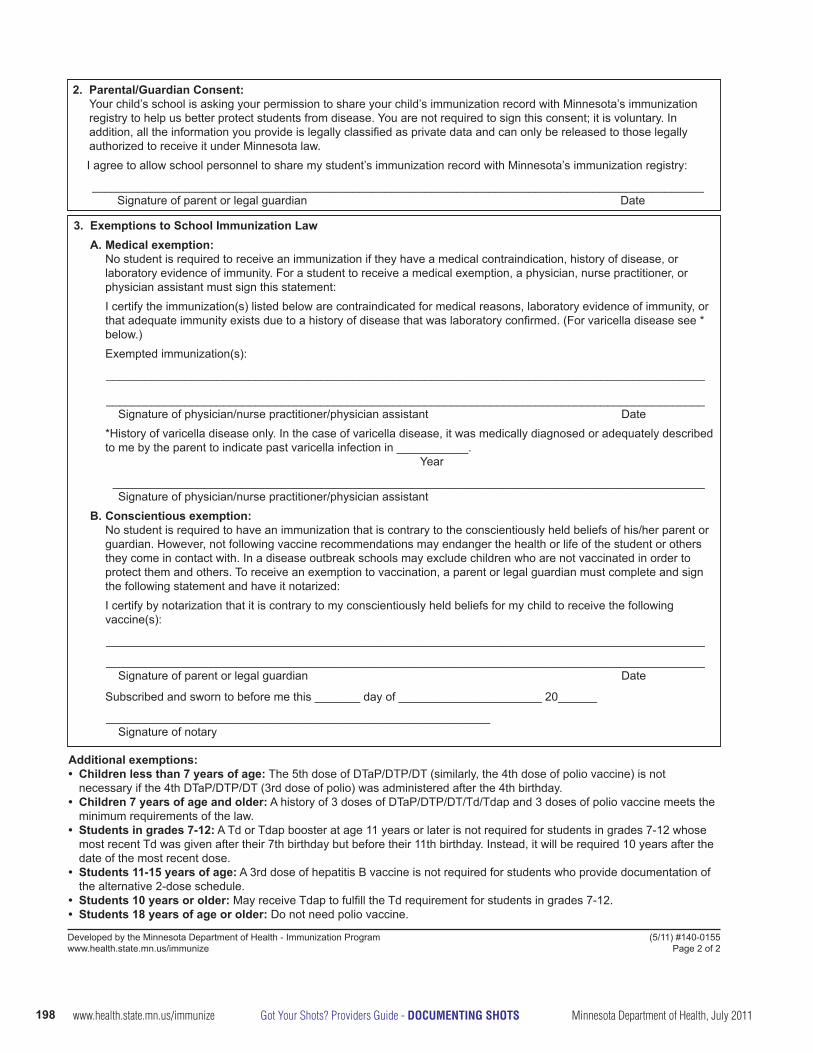
2. Parental/Guardian Consent: Your child’s school is asking your permission to share your child’s immunization record with Minnesota’s immunization registry to help us better protect students from disease. You are not required to sign this consent; it is voluntary. In addition, all the information you provide is legally classifi ed as private data and can only be released to those legally authorized to receive it under Minnesota law.
I agree to allow school personnel to share my student’s immunization record with Minnesota’s immunization registry:
______________________________________________________________________________________________Signature of parent or legal guardian Date
Developed by the Minnesota Department of Health - Immunization Program (5/11) #140-0155www.health.state.mn.us/immunize Page 2 of 2
3. Exemptions to School Immunization Law A. Medical exemption:
No student is required to receive an immunization if they have a medical contraindication, history of disease, or laboratory evidence of immunity. For a student to receive a medical exemption, a physician, nurse practitioner, or physician assistant must sign this statement:I certify the immunization(s) listed below are contraindicated for medical reasons, laboratory evidence of immunity, or that adequate immunity exists due to a history of disease that was laboratory confi rmed. (For varicella disease see * below.)Exempted immunization(s):
____________________________________________________________________________________________
____________________________________________________________________________________________Signature of physician/nurse practitioner/physician assistant Date
*History of varicella disease only. In the case of varicella disease, it was medically diagnosed or adequately described to me by the parent to indicate past varicella infection in ___________.
Year
___________________________________________________________________________________________Signature of physician/nurse practitioner/physician assistant
B. Conscientious exemption: No student is required to have an immunization that is contrary to the conscientiously held beliefs of his/her parent or guardian. However, not following vaccine recommendations may endanger the health or life of the student or others they come in contact with. In a disease outbreak schools may exclude children who are not vaccinated in order to protect them and others. To receive an exemption to vaccination, a parent or legal guardian must complete and sign the following statement and have it notarized:I certify by notarization that it is contrary to my conscientiously held beliefs for my child to receive the following vaccine(s):
____________________________________________________________________________________________
____________________________________________________________________________________________Signature of parent or legal guardian Date
Subscribed and sworn to before me this _______ day of ______________________ 20______
___________________________________________________________Signature of notary
Additional exemptions:• Children less than 7 years of age: The 5th dose of DTaP/DTP/DT (similarly, the 4th dose of polio vaccine) is not
necessary if the 4th DTaP/DTP/DT (3rd dose of polio) was administered after the 4th birthday.• Children 7 years of age and older: A history of 3 doses of DTaP/DTP/DT/Td/Tdap and 3 doses of polio vaccine meets the
minimum requirements of the law.• Students in grades 7-12: A Td or Tdap booster at age 11 years or later is not required for students in grades 7-12 whose
most recent Td was given after their 7th birthday but before their 11th birthday. Instead, it will be required 10 years after the date of the most recent dose.
• Students 11-15 years of age: A 3rd dose of hepatitis B vaccine is not required for students who provide documentation of the alternative 2-dose schedule.
• Students 10 years or older: May receive Tdap to fulfi ll the Td requirement for students in grades 7-12.• Students 18 years of age or older: Do not need polio vaccine.
198 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011

Data Elements Used in Recording Selected Childhood and Adult VaccinesVaccine Generic Name and Abbreviation Vaccine Brand Name MVX
codeCPT code
CVX code
Diphtheria, tetanus, pertussis (DTaP)
Daptacel PMC 90700 106Infanrix SKB 90700 20
Diphtheria, tetanus (pediatric) (DT) Generic PMC 90702 28DTaP–HepB–IPV Pediarix SKB 90723 110DTaP–IPV Kinrix SKB 90696 130DTaP–IPV–Hib Pentacel PMC 90698 120Tetanus, diphtheria (Td)
Decavac PMC 90714 113Generic MBL 90714 113
Tetanus, diphtheria, pertussis (Tdap)
Boostrix SKB 90715 115Adacel PMC 90715 115
Haemophilus influenzae type B (Hib)
PedvaxHIB (PRP-OMP) MSD 90647 49ActHIB (PRP-T) PMC 90648 48Hiberix (PRP-T) SKB 90648 48
Hib–HepB Comvax MSD 90748 51
Hepatitis A (HepA)
PediatricHavrix SKB 90633 83VAQTA MSD 90633 83
AdultHavrix SKB 90632 52VAQTA MSD 90632 52
Hepatitis B (HepB)
PediatricEngerix-B SKB 90744 8Recombivax HB MSD 90744 8
AdultEngerix-B SKB 90746 43Recombivax HB MSD 90746 43
HepA–HepB Twinrix SKB 90636 104
Human papillomavirus (HPV2, HPV4)
Gardasil, HPV4 (Types 6, 11, 16, 18) MSD 90649 62
Cervarix HPV2 (Types 16, 18) SKB 90650 118
Inactivated polio (IPV) IPOL PMC 90713 10
Influenza, trivalent inactivated influenza (TIV)
6-35 monthsFluzone PMC 90657 141Fluzone p-free PMC 90655 140
3 years or older
Fluzone PMC 90658 141Fluzone p-free PMC 90656 140Fluarix SKB 90656 140
4 years or older
Fluvirin NOV 90658 141Fluvirin p-free PMC 90656 140
9 years or older
Afluria CSL 90658 141Afluria p-free PMC 90656 140
18 years or older
FluLaval SKB 90658 141Agriflu PMC 90656 140
65 years or older
Fluzone high-dose PMC 90662 135
Continued199July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize

Data Elements Used in Recording Selected Childhood and Adult VaccinesVaccine Generic Name Vaccine Brand Name MVX
codeCPT code
CVX code
Influenza, live attenuated influenza vaccine (LAIV)
Flumist MED 90660 111
Japanese Encephalitis (JE) Ixiaro INT 90738 134Measles, mumps, rubella (MMR) M-M-R II MSD 90707 3
Measles, mumps, rubella, varicella (MMRV) ProQuad MSD 90710 94
Meningococcal conjugate (MCV)
Menactra PMC 90734 114Menveo NOV 90734 136
Meningococcal polysaccharide (MPSV) Menomune PMC 90733 32
Pneumococcal Conjugate, 7-valent (PCV) Prevnar PFR 90669 100
Pneumococcal Conjugate, 13-valent (PCV)
Prevnar PFR 90670 133
Pneumococcal, polysaccharide, 23-valent(PPSV)
Pneumovax23 MSD 90732 33
RabiesImovax PMC 90675 18
RabAvert NOV 90675 18
Rotavirus(RV1, RV5)
Rotarix (RV1) SKB 90681 119RotaTeq (RV5) MSD 90680 116
TyphoidTyphim Vi PMC 90691 101
Vivotif BPC 90690 25Varicella (chickenpox)(VAR) Varivax MSD 90716 21
Yellow Fever YF-VAX PMC 90717 37(ZOS) Zoster (shingles) Zostavax MSD 90736 121
This list includes the most commonly used vaccines. A current and comprehensive list of vaccines and their MVX, CPT, and CVX codes is available on the web at: www.health.state.mn.us/divs/idepc/immunize/registry/hp/vaxcodes.html.
200 www.health.state.mn.us/immunize Got Your Shots? Providers Guide - DOCUMENTING SHOTS Minnesota Department of Health, July 2011

Available on the web at: www.health.state.mn.us/divs/idepc/immunize/registry/hp/vaxcodes.html#mvx
Vaccine Manufacturers for Selected Childhood and Adult VaccinesMVX Code Vaccine Manufacturers
BPC Berna Products Corporation
CSL CSL Biotherapies, Inc.
MBL Massachusetts Biologic Laboratories (formerly Massachusetts Public Health Biologic Laboratories)
MED MedImmune, Inc.
MSD Merck & Co., Inc.
NOV Novartis Pharmaceutical Corporation (includes Chiron, PowderJect Pharmaceuticals, Celltech Medeva Vaccines and Evans Limited, Ciba-Geigy Limited, and Sandoz Limited)
PFR Pfizer, Inc
PMC sanofi pasteur (formerly Aventis Pasteur, Pasteur Merieux Connaught; includes Connaught Labo-ratories and Pasteur Merieux)
SKB GlaxoSmithKline (formerly SmithKline Beecham; includes SmithKline Beecham and Glaxo Wel-come)
201July 2011, Minnesota Department of Health Got Your Shots? Providers Guide - DOCUMENTING SHOTS www.health.state.mn.us/immunize






























