Embed Size (px)
Citation preview

Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 1 Getting Medicines Right Medicines on Discharge SOP 2.0
Document Control
Title
Getting Medicines Right on Discharge - Standard Operating Procedure
Authors
Author’s job title Governance and Community Services Pharmacist (Pharmacist and Lead Pharmacist Community Services respectively)
Directorate Planned Care
Department Team/Specialty Pharmacy Medicines Management
Version Date Issued Status Comment / Changes / Approval
0.1 September 2015
Draft Initial version drafted by Pharmacist and Lead Pharmacist Community Services for Community Hospitals.
0.2 December 2015
Draft
0.3 December 2015
Draft Draft 0.2 version amended to include acute services.
0.4 December 2015
Draft Further amendments made, following comments from Senior Pharmacy team, prior to stakeholder consultation.
0.5 January 2016
Draft Comments incorporated into draft 0.4, following stakeholder consultation in Dec 2015 / January 2016.
0.6 January 2016
Draft New Appendix added – flowchart for acute medicines discharge procedure and all SOPs referenced in the procedure added to section 8.
0.7 January 2016
Draft Letters removed from appendices to reduce length of document (still externally hyperlinked), in response to feedback and in preparation for submission to the Trust Drugs and Therapeutics Committee on 21st January 2016.
0.8 January 2016
Final Draft
Changes agreed by the Drugs and Therapeutics Committee incorporated into the final draft, for review by the Trust Medicines Governance Group meeting on 9th February 2016, prior to final version being published.
1.0 January 2016
FINAL Final version, approved by DTC 21-01-16
1.1 November 2016
Draft Minor amendment made, following publication of NICE QS120 (Medicines Optimisation), to expand information given to patients on discharge about possible / expected side effects and self-reporting of adverse effects of medication by patients to the Medicines and Healthcare products Regulatory Agency. Section 6.8 and Appendices 1 and 2 only updated.
2.0 January 2017
FINAL Changes approved by DTC 19-01-17
Main Contact Governance Pharmacist Northern Devon Healthcare NHS Trust Unit 1, Exeter International Office Park Clyst Honiton EX5 2HL
Tel: Direct Dial – 01392 356927
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 2 Getting Medicines Right Medicines on Discharge SOP 2.0
Lead Director Chief Pharmacist
Document Class Standard Operating Procedure
Target Audience Inpatient prescribers Nursing staff
Distribution List Deputy Director of Nursing for onward cascade; Ward Managers; Hospital Matrons Associate Medical Director for onward cascade; Inpatient prescribers (Acute) Trust Chief Pharmacist for onward cascade Lead Pharmacist, Community Services for onward cascade
Distribution Method Trust’s internal website
Superseded Documents There are no superseded documents.
Issue Date February 2016
Review Date February 2019
Review Cycle Three years
Consulted with the following stakeholders:
Trust Medicines Governance Group Chief Pharmacist, NDHCT and the
Senior Pharmacy Team Deputy Director of Nursing Ward Managers Community Hospital Matrons Associate Medical Director Head of Quality and Safety Medicines Management team Professional leads for community
nursing
Contact responsible for implementation and monitoring compliance: Chief Pharmacist
Education/ training will be provided by: Pharmacy Teams Workforce Development
Approval and Review Process
Drugs and Therapeutics Committee
Local Archive Reference G: PUBLIC Local Path PHARMACY/Policies & Procedures Filename Getting Medicines Right On Discharge SOP 2.0 Jan 2017
Policy categories for Trust’s internal website (Bob) Pharmacy, Medicines Management
Tags for Trust’s internal website (Bob) Getting Medicines Right, Discharge, Medicines Reconciliation, Medicines Policy, Pharmacy.
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 3 Getting Medicines Right Medicines on Discharge SOP 2.0
CONTENTS
Document Control........................................................................................................................ 1
1. Background .......................................................................................................................... 3
2. Purpose ................................................................................................................................ 5
3. Scope ................................................................................................................................... 5
4. Location ............................................................................................................................... 5
5. Equipment............................................................................................................................ 5
6. Procedure............................................................................................................................. 6
7. References ......................................................................................................................... 14
8. Associated Documentation ................................................................................................. 14
Appendix 1: Acute Hospital Medicines Discharge Planning Procedure ......................................... 15
Appendix 2: Community Hospitals Medicines Discharge Planning Procedure ............................... 16
1. Background
1.1. In 2009 the Care Quality Commission (CQC) published a report on discharge medication1 which emphasised the need for medicines reconciliation on admission and discharge and at point where the patient pathway crosses an interface.
1.2. In 2015 the National Institute for Health and Care Excellence (NICE) produced a guideline “Medicines Optimisation: the safe and effective use of medicines to enable the best possible outcomes” (NG5)2 which incorporates medicines reconciliation and highlighted the need for:
Organisations to ensure that medicines reconciliation is carried out by a trained and competent health professional – ideally a pharmacist, pharmacy technician, nurse or doctor – with the necessary knowledge, skills and expertise including:
Effective communication skills
Technical knowledge of processes for managing medicines
Therapeutic knowledge of medicine use
1.3. The 2015 NICE Medicines Optimisation guideline NG5 highlighted that adverse events of medicines represent a considerable burden in the NHS and have a significant impact on patients. When people transfer from different care providers, such as at the time of hospital admission or discharge, there is a greater risk of poor communication and unintended changes to medicines. When people move from one care setting to another, between 30% and 70% of patients have an error or unintended change to their medicines.
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 4 Getting Medicines Right Medicines on Discharge SOP 2.0
1.4. The 2015 NICE Medicines Optimisation guideline NG5 also highlighted that relevant information about medicines should be shared with patients, and their family members of carers, where appropriate, and between health and social care practitioners when a person moves from one care setting to another, to support high-quality care. This includes transfers within an organisation - for example, when a person moves from intensive care to a hospital ward – or from one organisation to another – for example, when a person is admitted to hospital, or discharged from hospital to their home or other location.
1.5. In December 2015, NICE published a guideline (NG27) describing standards for the transition between inpatient hospital settings and community or care home settings for adults with social care needs3. This guideline emphasised the importance of ensuring that the person, their carers and all health and social care practitioners involved in someone's move between hospital and home are in regular contact with each other. This is to ensure the transition is coordinated and all arrangements are in place. Further information on medicines related communication is referenced in NICE NG5 and NICE's guideline on managing medicines in care homes4.
1.6. Studies have shown that unplanned discharges are associated with longer delays, a higher risk of medication errors and a lack of or incorrect information being sent to GPs. This document outlines principles of good medicines practice on discharge, with recommendations to reduce delays and risks of medicines incidents at discharge5.
Summary
1.7. Medicines reconciliation reduces preventable medication errors, incidents and discrepancies on admission, discharge or transfer between care settings, and ensures that we are ‘Getting Medicines Right’ for patients.
1.8. Completion of medicines reconciliation on discharge ensures that every patient receives all of their medication as intended (prescribed) following the transfer of care.
1.9. It is the responsibility of all healthcare professionals involved in the care of the patient, whilst in our care, to ensure that medicines reconciliation is completed on discharge, with all relevant information handed over to the next provider/s of care. This is particularly important for patients with on-going, complex medication regimen requirements such as on-going monitoring, follow-up, supply and / or administration.
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 5 Getting Medicines Right Medicines on Discharge SOP 2.0
2. Purpose
2.1. The Standard Operating Procedure (SOP) has been written to:
Identify the procedure to ensure safe discharge or transfer of all inpatients in relation to medicines.
Improve personal care for the patient and reduce the risks associated with poor communication of accurate medication required post discharge or transfer.
To promote person-centred care.
3. Scope 3.1. This Standard Operating Procedure (SOP) relates to the following staff
groups who may be involved in the discharge /transfer process
Medical staff Registered nurses Pharmacy /medicines management staff Multi-disciplinary team
4. Location 4.1. This Standard Operating Procedure must be implemented in all clinical areas
where competent staff are available to undertake discharge with medication.
4.2. Staff undertaking this procedure must be able to demonstrate continued competence as per the organisations policy on assessing and maintaining competence.
4.3. This Standard Operating Procedure must be used in conjunction with the Trust Discharge Policy and the Discharges from the Community Hospitals Standard Operating Procedure, where applicable.
5. Equipment Current Prescription and Medication Administration Record / in-patient
prescription sheet (PMAR)
To Take Out (TTO) (also referred to as ‘To Take Away - TTA) form / e-discharge form
Relevant Patient information
Where applicable (patient-specific):
Transdermal patch application record
Community authority to administer and administration record
Medicines Reminder Chart

Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 6 Getting Medicines Right Medicines on Discharge SOP 2.0
6. Procedure 6.1 General principles for medicines discharge planning procedure - see
Flowcharts for Acute Services (Appendix 1) and Community Hospitals (Appendix 2)
6.1.1 A multi-disciplinary review relating to discharge medication should take place on a regular basis involving nursing, medical and pharmacy staff for each patient.
6.1.2 In community hospitals, when an estimated date of discharge is known the discharge prescription can be written in preparation and should be ordered at least 48 hours in advance to allow for adequate preparation time for supply, by sending to the dispensing pharmacy.
6.1.3 In the acute hospital, pharmacy must be informed when the discharge prescription is available for clinical screening, in preparation for discharge.
6.1.4 The electronic discharge summary/prescription should be completed with the current medication list and include information on any changes to medication, such as medicines stopped, started or doses altered. Reasons for changes and any required follow up are also to be documented to inform onward care services. This summary is sent to the GP as a medication discharge summary.
6.1.5 The prescriber must state all medications to be continued on discharge /transfer, including PRN medication. This should match the current PMAR except where there are changes such as medication to be stopped before or on discharge.
6.1.6 Nurse, pharmacist or pharmacy technician to check appropriate TTO / TTA form (Paper TTO / TTA form, e-discharge form or hospital FP10(HNC) prescription) is complete, legal, clear and unambiguous before sending to be dispensed. Ensure the allergy status is complete, where required on the form.
6.1.7 Any reasonable adjustments (e.g. blister pack, eye drop dispenser, inhaler aid etc.) to be highlighted on the TTO / TTA prior to sending for dispensing (see also 6.4.9).
6.1.8 Any Patient’s Own Medication (Patient’s Own Drugs, PODs) bought into hospital must be assessed for appropriateness and only be returned to the patient on discharge if it is in date, labelled correctly and prescribed on the discharge summary. Refer to the Trust Standard Operating Procedure for Patients’ Own Drugs (PODs) for inpatient setting .
6.1.9 If the patient has suitable, labelled, in date PODs then these items can be used as part of the final TTO / TTA; ensure there is at least a 14 day supply. Annotate the TTO / TTA to highlight which items and quantities need dispensing. Example: 14 days supply of POD on ward.
6.1.10 Ensure that the patient is given a total of at least 14 days supply of medication on discharge.
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 7 Getting Medicines Right Medicines on Discharge SOP 2.0
6.2 Hospital Pharmacy supply of discharge medication
6.2.1 Write the date that the TTO / TTA prescription is needed on the top of the TTO / TTA form to ensure it is returned by the supplying pharmacy in time.
6.2.2 For discharge medication supplied by the RD&E, allow at least 48 hours for the medicines to be sent to the ward. If the TTO / TTA is urgent and is required the following day, send to the RD&E pharmacy department by fax (Fax number: 01392 406057), followed up by a phonecall (Telephone number: 01392 406028), or email to the RD&E generic pharmacy email inbox: [email protected] .
6.2.3 For discharge medication supplied by NDDH Pharmacy, the discharge prescription will be screened by the pharmacist who has responsibility to ensure that the discharge medications are dispensed and available for the agreed discharge time. When the Pharmacy is closed, refer to and follow the Trust Standard Operating Procedure for Discharge Prescriptions when NDDH Pharmacy is closed.
6.3 Community Pharmacy Supplier
6.3.1 Hospital FP10(HNC) prescription forms may be used to obtain discharge medication, according to the Trust Standard Operating Procedure for FP10 Prescription Form Management.
6.3.2 Only order on the FP10 TTO / TTA the items required to complete the prescription for a 14 day supply.
6.4 Patients with more complex medication needs
6.4.1 Blister packs: The request for the blister pack other compliance aids (e.g. blister packs) must be communicated clearly e.g. by writing ‘Blister Pack’ clearly at the top of the TTO / TTA form. This request must also be communicated to the GP and community pharmacy by the discharging team.
6.4.2 All pharmacies require at least 48 hours’ notice to fill a blister pack and it cannot be assumed that all community pharmacies will supply them without prior agreement.
6.4.3 The RD&E Pharmacy will dispense one weeks’ supply in a blister pack unless stated or agreed otherwise, or quantities specified (i.e. state 14 days’ supply to be dispensed). Annotate the TTO / TTA with timings for the dosing times required (i.e. breakfast, lunchtime, teatime, evening).
6.4.4 Northern Devon Healthcare Trust Pharmacy will dispense two weeks’ supply in a blister pack, unless stated otherwise. Annotate the TTO / TTA with timings for the dosing times required (i.e. breakfast, lunchtime, teatime, evening).
6.4.5 New blister packs: Ensure a designated pharmacy is willing to take on dispensing of the prescription in a blister pack and that the patient is able to understand and use the type of blister pack supplied by their nominated pharmacy. Also ensure that the patient understands how to order and re-order, including the time needed by the pharmacy for preparation / dispensing of the blister packs.

Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 8 Getting Medicines Right Medicines on Discharge SOP 2.0
6.4.6 Inform the patient’s GP that their patient now requires a blister pack and why this has been agreed as an adjustment to support their medicines-taking.
6.4.7 Existing blister packs: Inform the patient’s GP that their patient is being discharged and required a restart of their blister pack medication supply.
6.4.8 Inform the patient’s nominated community pharmacy of the patient’s discharge date and that a blister pack restart is required but with possible changes from pre admission medication. The pharmacy / medicines management team will endeavour to write the phone number for the supplying pharmacy on the front of the inpatient drug chart. Inform the patient and pharmacy of any medication changes and advise the pharmacy to wait for a copy of the new prescription from the GP before dispensing. It is helpful to offer to fax a copy of the patient’s up to date prescription to the supplying pharmacy, to ensure on-going, timely medication supplies.
6.4.9 Other adjustments (e.g. haler-aids, eye drop aids etc.): Ensure that the patient is able to use the device before supplying: If a device has been used by the patient whilst on the ward (e.g. for self-administration), the patient may be given the device to take home with them to use at home. Annotate the TTO / TTA to inform the prescriber of the device supplied to the patient, in case of on-going requirements.
6.5 Store TTO / TTAs safely and securely 6.5.1 Store the TTO / TTA medication in the locked TTO / TTA cupboard or in the
patient’s locker, according to local arrangements. Write on the drug chart or inform patient’s named nurse where it is stored and if there are other items stored in the fridge or CD cupboard.
6.6 Checking the accuracy of medication supplied at point of discharge 6.6.1 Before supplying medication to the patient the nurse giving out the supply
must check the discharge prescription (TTO / TTA form, copy of the FP10HNC prescription or e-discharge record) against the Prescription and Medication Administration Record (PMAR) / Medicines Chart, to identify if there are any late changes. This final check of the TTO / TTA must occur no earlier than 24 hours prior to discharge date. Each medicine in turn should be checked against the discharge TTO / TTA supplied with it, ensuring that it is the:
• Right patient
• Right medicine
• Right dose
• Right frequency
• Right route
6.6.2 Ensure everything is present, including fridge items, insulin, inhalers, eye drops, Controlled Drugs, Drugs of Diversion, enteral / sip feeds.

Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 9 Getting Medicines Right Medicines on Discharge SOP 2.0
6.6.3 Where required to support safe administration of medicines following discharge, ensure that a medicines reminder chart has been completed for the patient or the patient’s carer and that it has been checked against both the TTO / TTA prescription and the medicines supplied at discharge (to ensure that the medicines reminder chart has is accurate and complete). The medicines reminder chart can be used to support discussion and must be given to the patient or their carer on discharge. Refer to the Preparation of Medicine Reminder Charts (MRC) Standard Operating Procedure.
6.6.4 Where discharge is delayed, nursing staff must check that the TTO / TTA medicines to be supplied are checked and reconciled against the current in-patient prescription and any alteration reflected in the medicines and reminder chart supplied on discharge.
6.7 Prescription alterations before discharge but after dispensing
6.7.1 Order altered or new items according to local arrangements. If a TTO / TTA form is used, cross items that are no longer required off the original TTO / TTA - there is no need to re-order the whole TTO / TTA. Remove medicines no longer required from the patient medication bag. Where e-discharge is being used, contact pharmacy to unlock the e-discharge record to allow amendments to be made.
6.7.2 Annotate the prescriptions clearly if there is more than one prescription. If a discharge has been delayed, recheck the TTO / TTA against the inpatient drug chart before discharge to identify any medication alterations.
6.8 Patient education before discharge
6.8.1 Only qualified nurses should give discharge medication to patients being discharged from wards. When discharging the patient from a community hospital, the nurse must sign and print their name on the final page of the community hospital PMAR chart (‘Medication Discharge Information’ section). When discharging from the acute setting, the nurse must document their actions, in relation to medicines, in the patient’s care records.
Go through all medicines and medication reminder charts with the patient (carer or relative as required), highlighting medicines which have stopped, started or changed. E.g.’ these are your paracetamol tablets. Take two four times a day for pain relief.’
The patient should receive a copy of the prescribed medication and explain that this copy lists the medication you are taking. This must match the electronic discharge prescription when written, where this applies.
If changes have been made to the patient’s medication regimen, clearly explain the changes. If the patient has further supplies of medication at home, encourage the patient to take any medicines that are no longer required to their local community pharmacy for safe disposal.

Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 10 Getting Medicines Right Medicines on Discharge SOP 2.0
6.8 Patient education before discharge (continued)
Where applicable, discuss with the patient that community pharmacies may offer services such as a ‘Medicines Use Review’ for patients taking multiple medicines or offer support with new medicines (‘New Medicines Service’) - an appointment may need to be made with the community pharmacist for some services. These services are confidential and the patient will be able to talk to their community pharmacist in a private area in the pharmacy.
Advice for anticoagulants (e.g. warfarin, dabigatran, rivaroxaban, apixaban): Confirm the patient knows they are on an anticoagulant and have received specific education if newly prescribed. Complete and give/return the yellow anticoagulant card and book to the patient. For warfarin, make sure that the patient or their carer is aware of and understands their most recent INR result, warfarin dose and re-test date and that this information is included on the TTO / TTA / e-discharge. Confirm arrangements have been made for blood test monitoring by contacting GP surgery / community nursing team and ensure the patients knows what these arrangements are.
Advice for other high risk medicines* or complex medication regimens (e.g. antibiotic courses, treatments requiring on-going monitoring, specialist prescribing, non-standard collection arrangements [e.g. for clozapine], timing of doses etc.) must be clearly communicated to the patient or their carer. Arrangements must be made clear for the following:
On-going specialist prescribing
On-going monitoring
On-going supply and collection, if not via community pharmacy
* Trust agreed list of high risk medicines:
Anticoagulants
Anti-epileptics
Anti-infectives (antibacterial drugs, antifungal drugs, antivirals including antiretrovirals)
Anti-Parkinsons medication
Desmopressin (DDVAP) - for treatment of diabetes insipidus
Insulin and oral hypoglycaemics
Medicines prescribed via intra-venous (IV) route
Regular opioid analgesia
Resuscitation medicines
Ref: Standard Operating Procedure for Omitted / Delayed Medicines

Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 11 Getting Medicines Right Medicines on Discharge SOP 2.0
6.8 Patient education before discharge (continued)
Gain consent for removal of PODs which are no longer required prior to discharge and advise patient to return unused or out of date medication to a pharmacy for destruction.
Inform patients of any common or expected side effects of their medication and explain that printed information is included in the packaging of medicines supplied on discharge.
Refer patients to the ward pharmacist if they require further information about their medication, including possible side effects and what to do if they experience them.
Explain to patients that further information and advice can be obtained from the patient’s community pharmacist or GP following discharge.
Inform patients that they can report any suspected side effects or adverse drug reactions to the Medicines and Healthcare products Regulatory Agency (MHRA), via the MHRA website: www.yellowcard.mhra.gov.uk/
6.9 Additional information for patients
Keep all medicines out of reach of children.
Do not share your medicines with anyone.
If you need a further supply of medicines contact your GP several days in advance.
Medicines Reminder chart supplied.
Trust ‘Information about your medicines’ leaflet.
6.10 Other sources of help and advice
Where applicable, inform patients that community pharmacies provide the following services for their patients (NB: these are community pharmacy based and an appointment may be needed):
Medicines Use Reviews (MURs), a community pharmacy based review of medication, aimed particularly at patients taking: Non-Steroidal Anti-Inflammatories (NSAIDs), anticoagulants, antiplatelets and diuretics; Patients with respiratory disease taking certain medicines for asthma or COPD; Patients recently discharged from hospital who have had a change in medicines during their hospital stay.
New Medicines Services (NMS) schemes, which primarily focus on five clinical conditions: asthma; chronic obstructive pulmonary disease (COPD), type 2 diabetes, antiplatelet / anticoagulant therapy, and hypertension. Patients can be offered the service when they present with a prescription for a new medicine in pharmacies, or may be referred to the service by prescribers.
Medication ‘apps’ (e.g. Pill Manager) can be downloaded for mobile devices
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 12 Getting Medicines Right Medicines on Discharge SOP 2.0
6.11 Information for Onward Care
GP / Prescriber / Community Pharmacy / Community Nursing Services
Medicines on discharge letter/e-discharge letter
Medicines stopped, started, changed and those requiring review or discontinuation such as loading doses must be included in the discharge summary. Refer to the Trust Standing Operating Procedure for Medication Loading Doses.
If compliance aids have been agreed (e.g. blister packs), provide information to all relevant professionals regarding the on-going requirements and arrangements for supply.
Information letter on unlicensed medicines – Unlicensed Medicines Letter Template

Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 13 Getting Medicines Right Medicines on Discharge SOP 2.0
6.11 Information for onward care (continued)
GP / Prescriber / Community Pharmacy / Community Nursing Services (continued)
If an injectable medicine is required to be administered post discharge, and the patient is unable to administer themselves (e.g. a low molecular weight heparin, LMWH), arrangements must be made for this to be administered in the patient’s next care setting; the first consideration should be for the patient to attend the GP surgery for administration by the Practice Nurse. If it is not possible for the patient to attend the GP surgery, a referral to the Community Nursing team will be required. Arrangements must include completion of a community authority to administer and administration record, which must be signed by the prescriber responsible for the patient’s care prior to discharge and must be sent with the patient or carer, with an explanation of its requirement / use in the next care setting.
If the patient is on antipsychotics or benzodiazepines for behavioural symptoms of dementia, the GP should be informed of the medication for symptom management prescribed and the review date; it may be appropriate to use the letter templates published on Bob: Antipsychotics Master Letter or Benzodiazepines Master Letter, if the information is not already included on the discharge letter / e-discharge, or Key Information Needed on Discharge, ‘KIND’ form if sent to the GP.
Specialist input post discharge (e.g. Community Psychiatric Nurse, Cluster Team)
Where the patient requires on-going input, post discharge, from other health or social care professionals, information about complex medication regimens must be clearly communicated to ensure continuity and arrangement of care.
Packages of care / care homes
Where the patient requires a package of care post discharge, ensure that the timing for medication dosing has been aligned to care visit provision, or vice versa.
Where the patient is being discharged to a care home, ensure that information about the patient’s medication is clearly communicated to the care home, particularly when there have been changes made to the medication regimen, or when the patient is being discharged to a new care setting.
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 14 Getting Medicines Right Medicines on Discharge SOP 2.0
7. References
1. Care Quality Commission, Managing patients’ medication after discharge from hospital, October 2009.
2. NICE guidelines [NG5], Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes, March 2015.
3. NICE guidelines [NG27], Transition between inpatient hospital settings and community or care home settings for adults with social care needs, December 2015.
4. NICE guidelines [SC1], Managing medicines in care homes, March 2014.
5. Royal Pharmaceutical Society of Great Britain; the Guild of Hospital Pharmacists; the Pharmaceutical Services Negotiating Committee; the Primary Care Pharmacists’ Association; joint publication: Moving patients, moving medicines, moving safety: Guidance on discharge and transfer planning. 2006.
6. Royal Pharmaceutical Society, Keeping patients safe when the transfer between care providers – getting medicines right. Final Report. June 2012.
8. Associated Documentation
8.1. Northern Devon Healthcare NHS Trust Medicines Policy and associated Standard Operating Procedures (SOPs):
FP10 Prescription Form Management
Preparation of Medicine Reminder Charts (MRC)
Standard Operating Procedure for Omitted / Delayed Medicines
Medication Loading Doses
Patients Own Drugs for inpatient setting (Community Hospitals)
Self-Administration of Medication
Management of patients taking oral anticoagulants in community hospitals
Management of Pharmaceutical Waste Standard Operating Procedure
8.2. NDHCT Discharge Policy
8.3. NDHCT Incident Management Policy
8.4. NDHCT Consent Policy
8.5. NDHCT Patient Information Leaflet – ‘Information about your medicines’
8.6. NDHCT Key Information Needed at Discharge (‘KIND’ Form)
8.7. NDHCT Discharge Prescriptions when NDDH Pharmacy is closed
8.8. NDHCT Discharges from Community Hospitals Standard Operating Procedure
8.9. NDHCT Patient and Ward Focused Discharges (Pharmacy SOP) - DSOP54
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 15 Getting Medicines Right Medicines on Discharge SOP 2.0
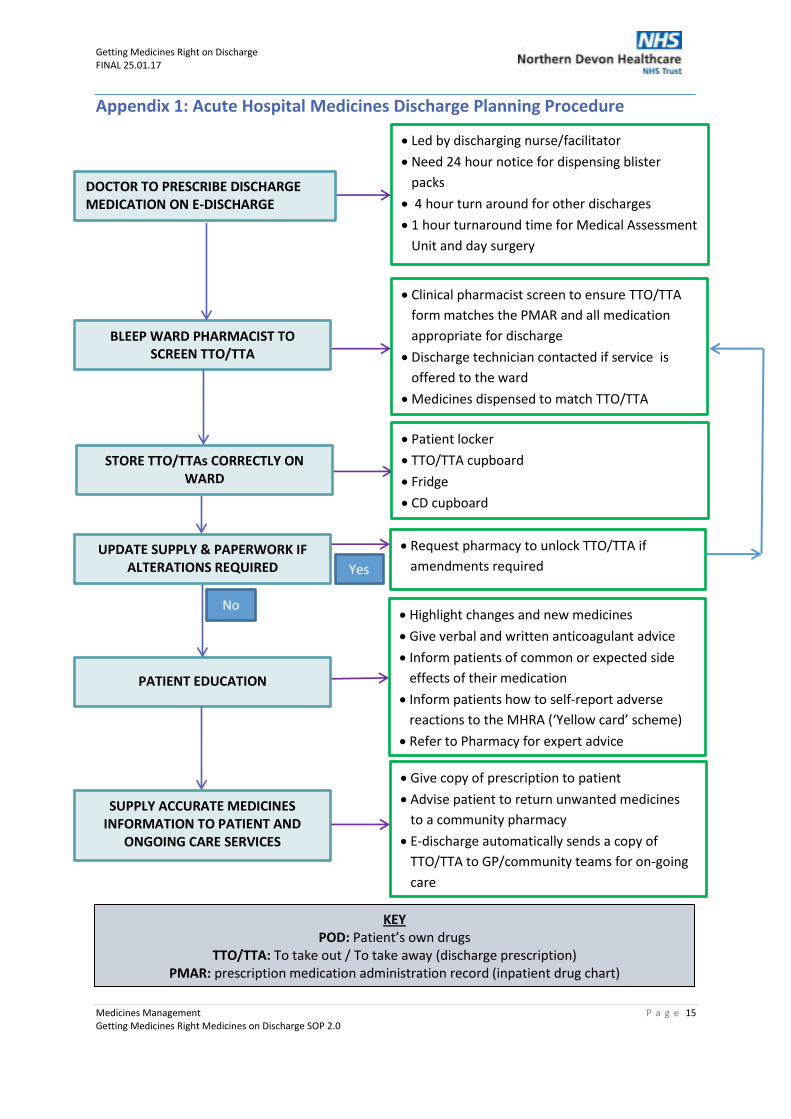
Appendix 1: Acute Hospital Medicines Discharge Planning Procedure
DOCTOR TO PRESCRIBE DISCHARGE MEDICATION ON E-DISCHARGE
BLEEP WARD PHARMACIST TO SCREEN TTO/TTA
Led by discharging nurse/facilitator
Need 24 hour notice for dispensing blister
packs
4 hour turn around for other discharges
1 hour turnaround time for Medical Assessment
Unit and day surgery
Clinical pharmacist screen to ensure TTO/TTA
form matches the PMAR and all medication
appropriate for discharge
Discharge technician contacted if service is
offered to the ward
Medicines dispensed to match TTO/TTA
STORE TTO/TTAs CORRECTLY ON WARD
Patient locker
TTO/TTA cupboard
Fridge
CD cupboard
UPDATE SUPPLY & PAPERWORK IF ALTERATIONS REQUIRED
Request pharmacy to unlock TTO/TTA if
amendments required
PATIENT EDUCATION
Highlight changes and new medicines
Give verbal and written anticoagulant advice
Inform patients of common or expected side
effects of their medication
Inform patients how to self-report adverse
reactions to the MHRA (‘Yellow card’ scheme)
Refer to Pharmacy for expert advice
SUPPLY ACCURATE MEDICINES INFORMATION TO PATIENT AND
ONGOING CARE SERVICES
Give copy of prescription to patient
Advise patient to return unwanted medicines
to a community pharmacy
E-discharge automatically sends a copy of
TTO/TTA to GP/community teams for on-going
care
KEY POD: Patient’s own drugs
TTO/TTA: To take out / To take away (discharge prescription) PMAR: prescription medication administration record (inpatient drug chart)
Yes
No
Getting Medicines Right on Discharge FINAL 25.01.17
Medicines Management P a g e 16 Getting Medicines Right Medicines on Discharge SOP 2.0
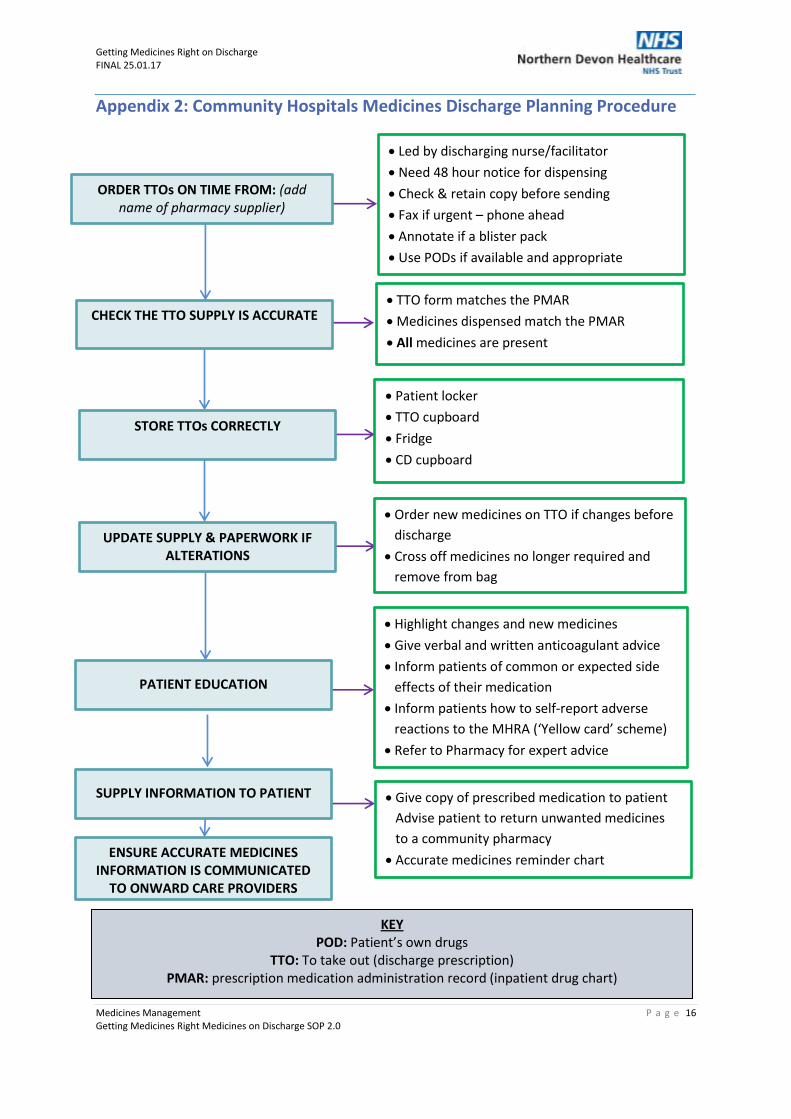
Appendix 2: Community Hospitals Medicines Discharge Planning Procedure
ORDER TTOs ON TIME FROM: (add name of pharmacy supplier)
CHECK THE TTO SUPPLY IS ACCURATE
TTO form matches the PMAR
Medicines dispensed match the PMAR
All medicines are present
STORE TTOs CORRECTLY
Patient locker
TTO cupboard
Fridge
CD cupboard
UPDATE SUPPLY & PAPERWORK IF ALTERATIONS
Order new medicines on TTO if changes before
discharge
Cross off medicines no longer required and
remove from bag
PATIENT EDUCATION
Highlight changes and new medicines
Give verbal and written anticoagulant advice
Inform patients of common or expected side
effects of their medication
Inform patients how to self-report adverse
reactions to the MHRA (‘Yellow card’ scheme)
Refer to Pharmacy for expert advice
SUPPLY INFORMATION TO PATIENT
Give copy of prescribed medication to patient
Advise patient to return unwanted medicines
to a community pharmacy
Accurate medicines reminder chart
KEY POD: Patient’s own drugs
TTO: To take out (discharge prescription) PMAR: prescription medication administration record (inpatient drug chart)
ENSURE ACCURATE MEDICINES INFORMATION IS COMMUNICATED
TO ONWARD CARE PROVIDERS
Led by discharging nurse/facilitator
Need 48 hour notice for dispensing
Check & retain copy before sending
Fax if urgent – phone ahead
Annotate if a blister pack
Use PODs if available and appropriate