Embed Size (px)
Citation preview
DoctoralThesisproject:
"EVALUATIONOFTHEEFFECTIVENESSOFAPROGRAMTOSTRENGTHENTHEPELVICFLOORINTHEPOSTPARTUMWOMEN"
Alumna:Ms.ElisaHernándezLlorente.
Director1:Dr.CarmenSuárezSerrano.Director2:Dr.FátimaLeónLarios.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
2
Index:
1. Introduction3
2. TheoreticalFramework4to11
3. Justification12
4. objectives13
5. hypothesis14
6. Methodology15to20
7. WorkPlan21
8. References22to24
9. Annexes25to29
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
3
1.INTRODUCTION:
Pelvic floor dysfunction is a problem of high prevalence in the puerperal period of
women. Urinary incontinence is one of the most frequent dysfunctions that most
affect their health after childbirth. Recent studies expose the idea that pelvic floor
muscle training using vaginal areas, generally, reduces the appearance of pelvic
dysfunction,andthusimprovesthequalityoflifeofthesewomen.
Pelvicfloorhealthisanimportantissueforwomenaroundtheworldastheimpactof
pelvic-perineal problems in any woman life is often considerable. Pelvic problems
impairthequalityoflifeofwomenwhosufferthem,becausetheyfeelvulnerable,and
experienceagreat impotencebythe inability topredicthowwill theirbodyreact to
certainsituationsofdailylife;thisaffectsnegativelytheirintimaterelationships,work
andsocialsactivities1.
Pregnancyandbirthhavehistoricallybeenidentifiedasthemajoretiologicalfactorsof
pelvicfloordysfunctions2.Theliteraturedemonstratesthat33%ofwomenexperience
urinary incontinence (UI) during the first three months postpartum, with no major
improvements until the first anniversary of birth3. We also find 10% of fecal
incontinence during quarantine, extended by 1% of women until 9 months
postpartum4.Therearealsopelvicorganprolapse,rangingbetween7.7%and56%of
women3-6monthsPostpartum5.
Ashasbeenevidenced,afunctionalweaknessofthepelvicfloormuscles,cannotonly
enhancetheinfluenceoftheUIforwomeninthepostpartumperiod,butwillalsobea
contributingfactortofecalincontinenceandprolapseofpelvicorgans2.
2.Framework:
In Spanish hospitals over the past 15 years a change is taking place in attention to
normaldelivery,becauseuntilrelativelyrecentlydays,theepisiotomywassystematic
foreverywomanwhowasperceivedthatdidnothaveasufficientlyelasticperineum
under criterion of the professional who was attending the birth. With the perineal
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
4
consequencesthatsubsequenthealingofalateralhalfcutinthepelvicfloormuscles
had.
Fortunately,todayprofessionalsobstetricsaremoreupdatedandhavegreateraccess
to new scientific evidence that contributes to our environment, so this type of
intervention, unless the professional deems strictly necessary, are notmade.Unless
exists a risk of loss of fetal well-being, or the need to end the labor through an
instrumenteddelivery (forcepsorvacuum),althoughthese finaldecisionsarealways
underthecriterionoftheprofessionalwhoisattendingchildbirth.
Themainthemethatoccupiesourstudyisthewomen`spelvicfloor,solet'sintroduce
a little deeper into the subject concisely describing this part of the female body
anatomy.
Thepelvic floor is thesetofsoft tissue (muscles, fasciaand ligaments) that limit the
pelviccavityat thebottom. It is responsible forsupporting theweightof theviscera
andhelps toprevent the leakageofurineand stool5. Therefore it is imperative that
thesemuscleshavethestrengthandtoneneededtoperformtheirfunctionsandnot
disruptthedailylivesofwomen.
Pelvic floor dysfunctions are often caused by external aggression, such as surgery,
vaginaldelivery,orbylackofmusclestrength:hypotonia,orevenmusclehypertonia.
Thenewlinesofnormaldeliverycare,describedinthe"ClinicalPracticeGuidelinefor
NormalBirthCare"publishedbytheSpanishMinistryofHealthin2010recommended
thefollowingactions(withanAlevelofrecommendation):
• Itshouldnotbepracticedroutineepisiotomyinspontaneouslabor.
• Episiotomyshouldbeperformed if there isa clinicalneed,asan instrumental
birthorsuspectedfetalcompromise.
• Before performing an episiotomy effective analgesia should be performed,
exceptoneduetoacutefetalcompromiseemergency.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
5
• Whenanepisiotomyisperformed,therecommendedtechniqueismediolateral
episiotomy, starting it in the posterior commissure of the labia minora and
usually directed to the right side. The angle to the vertical axis should be
between45and60degreestoperformepisiotomy.
• Episiotomy should not be routinely performed during a vaginal delivery in
womenwithtearsinthirdorfourthgradeinpreviousbirths.
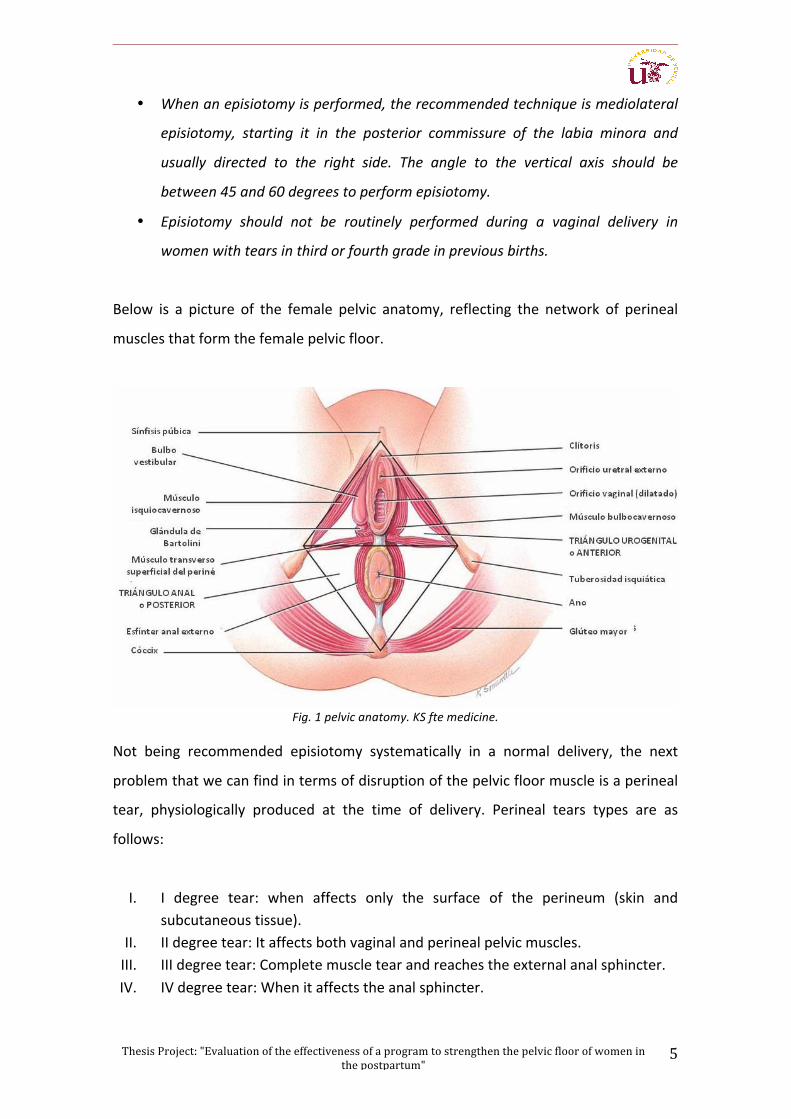
Below is a picture of the female pelvic anatomy, reflecting the network of perineal
musclesthatformthefemalepelvicfloor.
Fig.1pelvicanatomy.KSftemedicine.
Not being recommended episiotomy systematically in a normal delivery, the next
problemthatwecanfindintermsofdisruptionofthepelvicfloormuscleisaperineal
tear, physiologically produced at the time of delivery. Perineal tears types are as
follows:
I. I degree tear: when affects only the surface of the perineum (skin andsubcutaneoustissue).
II. IIdegreetear:Itaffectsbothvaginalandperinealpelvicmuscles.III. IIIdegreetear:Completemuscletearandreachestheexternalanalsphincter.IV. IVdegreetear:Whenitaffectstheanalsphincter.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
6
Thesetypesofperineal trauma(bothtearandepisiotomy)shouldbesuturedbythe
professionalwhoisattendingthedelivery(midwifeorobstetrician)asrecommended
bytheClinicalPracticeGuideline2010,wementionedearlier.Recommendationsasto
suturetear(recommendationA-level)are:
• Is recommended suturing first grade lacerations in order to improve healing,unlesstheedgesoftheskinarewellapproximated.
• Perineal repair of second degree tears using continuous suture technique isrecommended.
• If aftermuscle suture of a second degree tear the skin iswell approximated,stitches are not need. But if the skin needs to be approached, therecommendations requires to be performed in a continuous intradermaltechnique.
Thetypeoftearoccurredduringdelivery,orifepisiotomyneedtobedone,andeven
thetypeofsutureusedforperinealrepair,willaffectlesserorgreatertherecoveryof
the pelvic floor postpartum. Therefore, the recommendation is always to be as less
aggressive as possible, taking into account the quality of life of women pelvic floor
dysfunctioninshort-andlong-term.
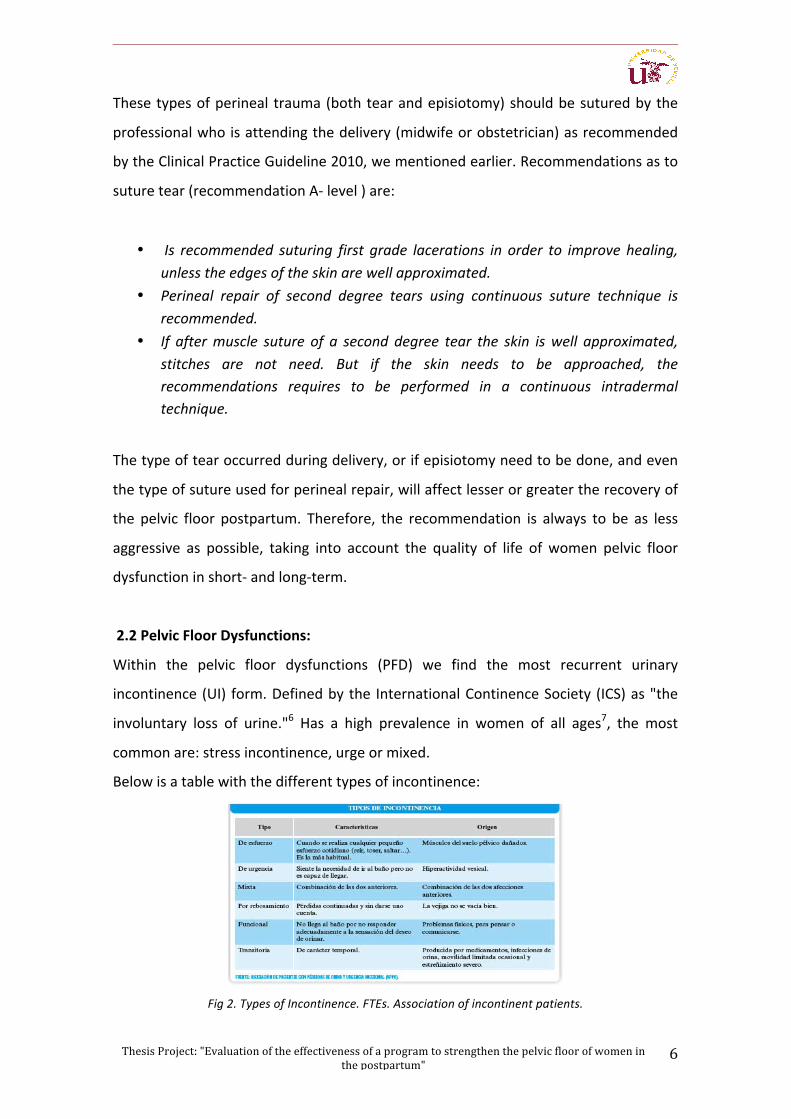
2.2PelvicFloorDysfunctions:
Within the pelvic floor dysfunctions (PFD) we find the most recurrent urinary
incontinence (UI) form.Definedbythe InternationalContinenceSociety (ICS)as"the
involuntary loss of urine."6 Has a high prevalence in women of all ages7, the most
commonare:stressincontinence,urgeormixed.
Belowisatablewiththedifferenttypesofincontinence:
Fig2.TypesofIncontinence.FTEs.Associationofincontinentpatients.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
7
Incontinenceaffectsfiveoutoftenpregnantwomen(48.3%).Fouroutoftenpregnant
women experience urine leakage for the first time during pregnancy (40%). In
pregnant women with pre-UI severity increases during pregnancy. Urinary
incontinencebeforeandduringpregnancyisassociatedwithpreviousgestations8.
In fact, the most common reason that a woman usually consult a health care
professionalwithinthefieldofperineal-sphincterreeducation isundoubtedlyurinary
incontinence, being the postpartum period and menopause the highest incidence.
Thesedata are shown in the survey conductedbyWilsonon1,505womenat three
months postpartum with 34.3% of incontinents9, while in another study with
perimenopausal women Minaire discloses that 47.6% of these women report
involuntaryleakageofurine10
Atothertimes,thereasonforconsultationisapelvicorganprolapse,presentin30%
ofwomenbetween29and59 years according toa Swedish studyof487peopleby
SamuelssonandVictor11.However,thistypeofdysfunctionsareoftenassociatedwith
perineal pain, faecal incontinence or sexual dysfunction, that the patient will not
initiallyrefer.Buttheseproblems,mayinsteadposeabiggersocialproblem,greater
thanurinaryincontinence.
Aswediscussedearlier,vaginaldeliveryisaknownriskfactorforUIandtheresultsof
multiplestudiesconfirmitsimpactonhospitalclinicalpractice.Althoughseverecases
persist,itisincludedasignificantreductioninsymptomsduringthefirst12monthsas
longastheperinealmusculatureisbeingtonedbyperformingspecificexercises12.
Intheimmediatepostpartumitisestimatedthat50%ofwomenwithvaginaldelivery
havea transienteffortUI, evolving toward regressionor spontaneoushealing in50-
70% of cases after spending six weeks after childbirth. However, these transient
incontinence reflect a perineal alteration, represents an increased risk of 2.5%
posteriordevelopingincontinence13.
Taking into consideration, pregnancy and childbirth as a major risk for developing
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
8
incontinence is due to a decrease of 22-35% of the strength of the pelvic floor
muscles14. In addition, if incontinencedevelopsduringpregnancyor thepostpartum
periodandnoreturnaddressbefore3monthspostpartum,there isasignificantrisk
thatpersistsfor5yearsafter15.
AccordingtoastudybyEwingsin2015“Thepresenceofoneormoreepisiotomiesis
also a significant risk factor, however, cesarean and epidural use during childbirth,
seem to be a protective factor”16. Although, this information continues to be
controversialbecause,accordingtoastudybyRotveit in2003withatotalof15,307
women, it was observed that compared with nulliparous women, women who had
given birth by Caesarean section had a probability of 1.5 to experience any
incontinence.Theexplanation isthatnotonly labor,butalsotheweightofthefetus
andposturalalterationduringpregnancyareriskfactorsofurinaryincontinenceinthe
postpartum period overloading the perineum previously17. In view of the results of
these studies, the importanceof knowing thehistoryofourobstetricalpatientsand
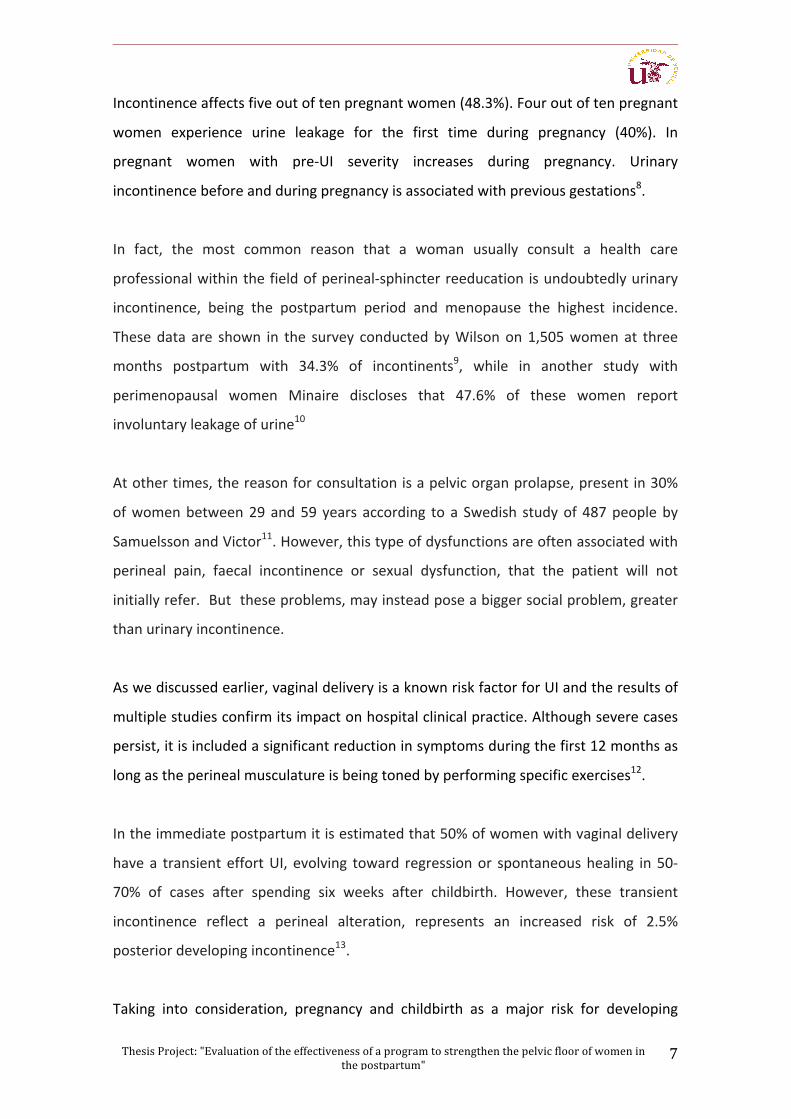
reflectitonitsclinichistoryisclear.
Fig.3organicincontinentpatientsFteDamages.Associationofincontinentpatients.
Thepelvicfloormuscletraining(PFMT)hasanimportantplaceinthetreatmentofUI,
withasuccessrateof56-75%18,Sothat,areviewbytheCochranein2011,concludes
that it isconsistentlybetter thannotreatmentorplacebo,andshouldbeofferedas
firsttreatmentforwomenwithUI19.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
9
ThemechanismofactionofPFMTishypertrophyofmusclefibers, improvingcortical
awarenessofthemuscle,connectivetissuestrengthand increasingtheeffectiveness
ofrecruitmentofmotoneurons18.
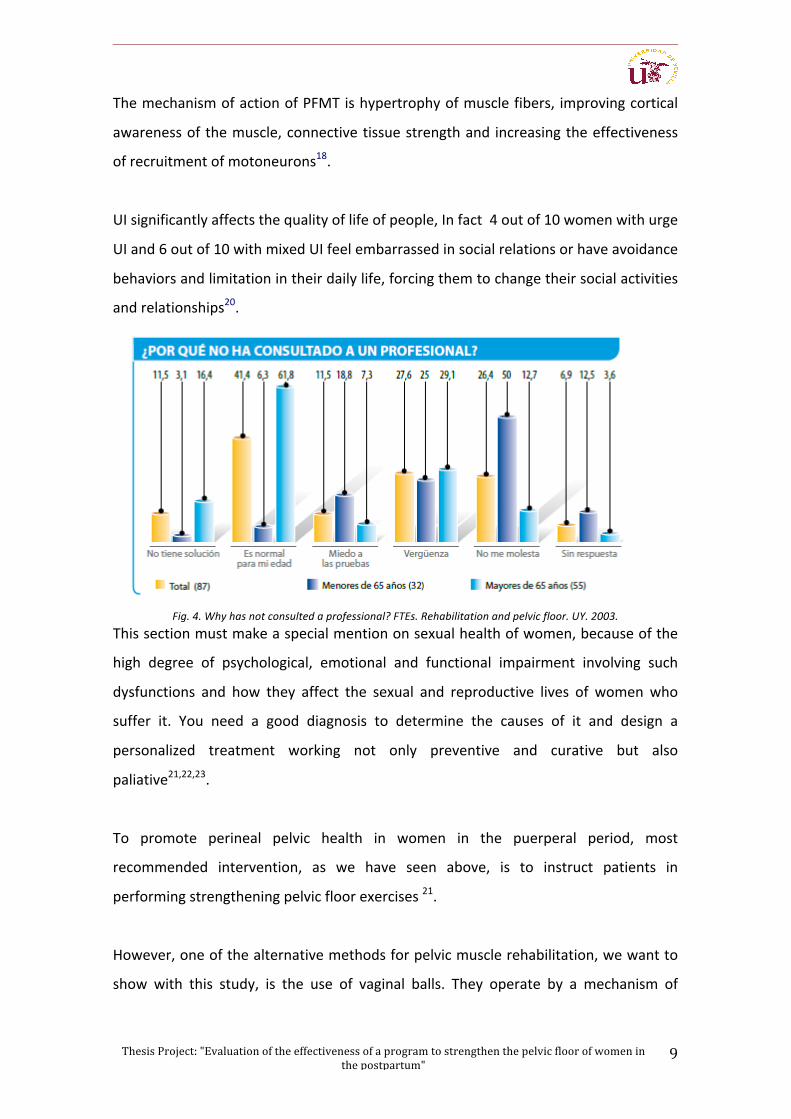
UIsignificantlyaffectsthequalityoflifeofpeople,Infact4outof10womenwithurge
UIand6outof10withmixedUIfeelembarrassedinsocialrelationsorhaveavoidance
behaviorsandlimitationintheirdailylife,forcingthemtochangetheirsocialactivities
andrelationships20.
Fig.4.Whyhasnotconsultedaprofessional?FTEs.Rehabilitationandpelvicfloor.UY.2003.
Thissectionmustmakeaspecialmentiononsexualhealthofwomen,becauseofthe
high degree of psychological, emotional and functional impairment involving such
dysfunctions and how they affect the sexual and reproductive lives of womenwho
suffer it. You need a good diagnosis to determine the causes of it and design a
personalized treatment working not only preventive and curative but also
paliative21,22,23.
To promote perineal pelvic health in women in the puerperal period, most
recommended intervention, as we have seen above, is to instruct patients in
performingstrengtheningpelvicfloorexercises21.
However,oneofthealternativemethodsforpelvicmusclerehabilitation,wewantto
show with this study, is the use of vaginal balls. They operate by a mechanism of
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
10
involuntarymusclecontractionstopreventpossibleremovalofthespheresoutofthe
vagina.
It is demonstrated in literature (last systematic review by Oblasser 2015)25, the
shortageofscientificevidencepublishedconcerningtheeffectivenessofvaginalballs
to improve the performance of pelvic-perineal muscles and the UI during the
puerperium. Most published studies suggest that vaginal spheres can be useful to
improve theUI in the postpartum, but all suggest thatmore studies are needed to
corroboratesuggestions,asthecurrentevidenceislimited.
Thanks to the above references,we can confirm the dependence of pregnancy and
childbirthalongwithafewetiologicalfactorsofpelvicfloordysfunctionand,especially
theUI,whichisanareaofinterestinepidemiologicalresearch.Althoughthenumbers
of studies examining the prevalence of UI in the postpartum period are highly
controversialandstudiesareinsufficientinourmidst.
3.RATIONALE:
Presentlyinthecurrentliteraturethereisnoempiricalknowledgetosupporttheuse
ofvaginalspheresor itseffectivenesscomparedwithstandardpelvic floorexercises.
Allitemsandissuesfoundrequiremorestudiestosupportitsusefortherecoveryof
thepelvicfloorofwomeninthepostpartumperiod.
UI isadiseasewithahighprevalence inwomenthatdoesnot involvean increase in
mortality, but it limits the autonomy, self-esteem and significantly reduces and
deteriorate the quality of life. Often it remains undiagnosed and untreated or is
treated inappropriately. The short experience and few studies indicate that some
professionals do certain exercises without knowing exactly muscle actions and side
effectsareimplicit.
Vaginal spheres stimulateperineal type I fibers,whichmakeup80%of theperineal
musculature and give response to a reflected tonic activity. While traditional
rehabilitation exercises of the pelvic floor and postpartum (PFMT) stimulates type II
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
11
fibers,whicharepartofother20%oftheperinealmusculatureandareresponsiblefor
voluntarymuscleactivity.
It is demonstrated the effectiveness of pelvic floor muscle training (PFMT) in
preventing both: urinary and fecal postpartum incontinence8.. However, there is no
evidenceoftheeffectofvaginalballssuchdysfunctions.
Therefore we must make three different intervention groups to integrate a
comparativestudyoftreatment.Currentlybeingcarriedoutasamethodofperineal
recovery after childbirth (PFMT) and vaginal areas as a new method to study. The
groupswouldbeasfollows:
• Group1(Control)=PFMTwouldperformtheexercisesexclusivelydesignedby
theteamofPhysiotherapyparticipatinginthestudy.
• Group 2 (Intervention a) = PFMT would perform exercises with the use of
vaginalspheres.
• Group3 (Intrervención-b) =wouldperform intensive treatment,designed for
physiotherapyequipmentvaginalareas.
4.OBJECTIVES:
4.1Mainobjective:
-Todeterminetheeffectivenessof3typesofmuscletrainingforrecoverypelvicfloor
postpartum and evaluate their effectiveness by perineometer, Test and Modified
OxfordICIQIncontinenceQuestionnaireSF.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
12
4.2 Specificobjectives:
- Evaluate theeffectivenessof three interventionson improving thesymptoms
of urinary incontinence in the target population (women in puerperal period
Sevilla)
- Assess the impact of improving the quality of life through King`s Health
Questionnaire(KHQ)initsSpanishversionvalidatedin2013.
- Assess the sexual satisfactionofwomenwhoparticipated in the intervention
throughthequestionnaire:FSFI(FemaleSexualFunctionIndex).
5.HYPOTHESIS:
Interventionbasedontheapplicationofthetraditionalmethod(PFMT)withtheuseof
vaginalballsincreasestheforceofperinealmusclesmeasuredbymodifiedtestOxford
and perineometer. Likewise, it decreased urine leakage in women with urinary
incontinencetreatmentversusexclusivetraditionalexercisespelvicfloor.
Similarlyinterventionbasedontheapplicationofthetraditionalmethodwiththeuse
of vaginal spheres improves quality of life and increases sexual satisfaction in the
puerperalperiodcomparedtotraditionaltreatment.
Therefore,womeninthepuerperalperiod,performpelvicfloorexercises(PFMT)with
vaginalspheres,havemorerapidandeffectiverecoveryoftheperinealstrength.
6.Methodology:
6.1typedesignandstudypopulation:
In order to determine the effectiveness of using vaginal areas for improving the
perinealstrengthofwomeninthepostpartumperiod,wehavedesignedarandomized
experimental clinical trial. We will take as a reference population all primiparous
womenwhogivebirthinthemetropolitanareaofSeville,inthecourseofayear.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
13
Theparticipationisvoluntaryandunpaidaskedallwomenthroughinformedconsent,
deliveredinthepuerperalvisit,themidwifeconsultationitself.
6.2EthicalAspects:
Datahavebeenobtained following theprovisionsof Law15/1999,ofDecember13,
Protectionof PersonalData. To ensure confidentiality of users, eachwas assigned a
protocolnumberwithoutstartinganypersonalinformationthatcanidentifythem,so
wehaveworkedwithanonymousdata.
Inallcases,anonymityandfreeparticipationofstudysubjectswillberespectedand,
followingthelegislationonbiomedicalresearch,amodelofinformedconsentmustbe
prepared for theparticipants in the study.Thecompletionof suchconsentwillbea
prerequisiteforparticipationintheproject.
In this model, you will be informed of the study objectives, the duration of their
participation, as well as the freedom to refuse participation, and they ensure data
confidentiality.
Thisresearcharisesfromapreviousstudy,whichwascertifiedtocomplywithethical
and scientificquality criteriaaccepted.Todo this,he issuedapermitand theEthics
Committee of the University Hospital Virgen de Valme Clinical Research, this being
favorabletoitsrealizationandattached(AnnexIII).
6.3CriteriaforInclusion/Exclusion:
Thecriteriathatwillbeusedtoincludeorexcludewomeninthestudyareasfollows:
6.3.1.Criteriousinclusion:
- Primiparouswomen.
- Womenwhoareinthepostpartumperiodbetween6weeks(quarantine)and6
monthsatthestartoftheintervention.
- NewbornbirthsTerm(from37weeks)
- CeaseLochia.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
14
- SufficientknowledgeoftheSpanishlanguage,bothwrittenandspoken.
- Acceptancetoparticipateinthestudythroughinformedconsent.
6.3.2Exclusioncriteria:
- Multiparouswomen
- Womenofflimitspostpartum(previousbirthto6monthsaftersurgery)
- Womenundergoingtreatmentoflowerurinarytract(ITUtreatment)
- Womenwhoarealreadyparticipatinginarecoveryprogrampelvicfloor.
- WomenwithtearIIIandIVgrade.
- Pregnant(orbecomepregnantapproachintheinterventionperiod)Women
- Starting point pelvic floormuscle balancewomen less than 2 points. (Where
retentionvaginalareasimpossible)
- Inabilitytoperformthenecessaryproceduresforintervention.
6.4Studyvariables:
Quantitativevariablestobetakenintoaccountforthestudy,all
numerictype,theyareasfollows:
- Maternalage(measuredinyears):DiscreteVariable/QuantitativeControl.
- Gestational age (measured in weeks): Variable Continuous / Quantitative
Control.
- Tearing Type: NT (No Tearing) / type I / type II / type III / type IV: Variable
quantitativecontinuous/Control.
- RNweight(measuredingrams):quantitativecontinuousvariable/Control
- ObjectiveForce1(TestOxfordDigitalScale0-5):DiscreteVariable/Dependent
quantitative.
- objective force 2 (perineometer 0 to 12): Continuous variable / Dependent
quantitative.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
15
Codingofqualitativevariablesstudiedwereasfollows:
- Type of delivery: eutocic 1; Forceps 2; Suction cup 3; Cesarean 4. Variable
Control
- Presentation:Cephalic1;2.Buttocks.VariableControl
- Analgesia:NA.1;Regional2;Local3.VariableControl
- Episiotomy:yes1;No2.VariableControl
- ICIQ-SF:NoIncontinence1;Smalllosses2;incontinence3.VariableControl
- Exercise conducted during the study: Control 1/2 and 3 Group Intervention
Group.Independentvariable
6.5Descriptionofthestudy:
The studywill be a Controlled and Randomized Clinical Trial, single-blind (Technical
opaque envelopes), with three parallel groups for intervention and subsequent
comparison:
Group1(Control):thisgroupwillperformpelvicfloorstandardizedexercises(PFMT),
designedby the physiotherapy team thatwill participate in the study, following the
guidelinesofcurrentclinicalpracticeanddeterminingadurationofatleast12weeks
tocarryouttheexercises.
Group 2 (Intervention-a): this group will perform pelvic floor exercises set by
physiotherapy equipment while using the vaginal balls. Its duration will also be 12
weeks.
Group3(Intervention-b):thisgroupwillusethevaginalballsintheiractivitiesofdaily
lifeduring12weeksoftheinterventionprogram,theintensityofthetimeofusingthe
balls will be determined by the physiotherapy team that participate in the study
program.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
16
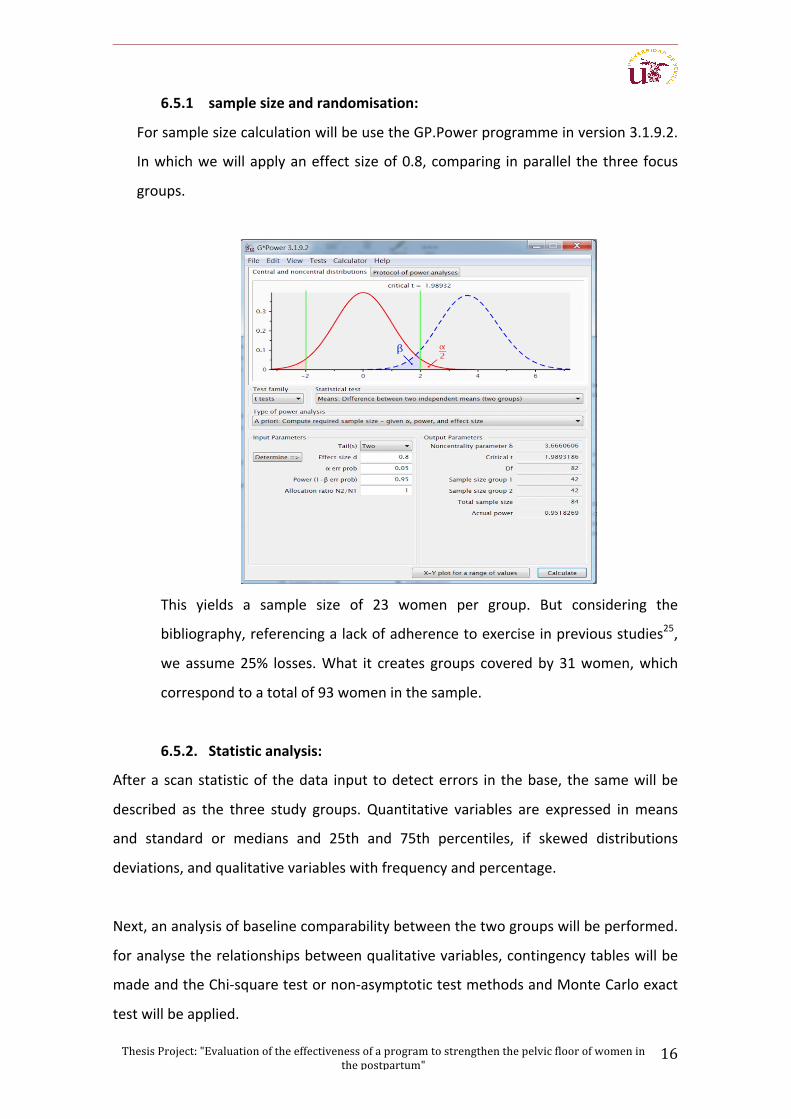
6.5.1 samplesizeandrandomisation:
ForsamplesizecalculationwillbeusetheGP.Powerprogrammeinversion3.1.9.2.
Inwhichwewillapplyaneffectsizeof0.8,comparing inparallel thethreefocus
groups.
This yields a sample size of 23 women per group. But considering the
bibliography,referencingalackofadherencetoexerciseinpreviousstudies25,
weassume25% losses.What it creates groups coveredby31women,which
correspondtoatotalof93womeninthesample.
6.5.2. Statisticanalysis:
Afterascanstatisticof thedata input todetecterrors in thebase, thesamewillbe
described as the three study groups. Quantitative variables are expressed inmeans
and standard or medians and 25th and 75th percentiles, if skewed distributions
deviations,andqualitativevariableswithfrequencyandpercentage.
Next,ananalysisofbaselinecomparabilitybetweenthetwogroupswillbeperformed.
foranalysetherelationshipsbetweenqualitativevariables,contingencytableswillbe
madeandtheChi-squaretestornon-asymptotictestmethodsandMonteCarloexact
testwillbeapplied.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
17
To see if there are differences in average of numerical variables between the two
groups, T-Student's testwill beused for independent samplesor Mann-Whitney-U
Testfornon-normaldistributions.Significantmeandifferenceswillbequantifiedwith
confidenceintervalsat95%and,ifnotnormal,thedifferencesbetweenmedianswith
confidenceintervalsHodges-Lehman95%.
Furthermore,tocontrastchangesinanumericalparametermeasuredatdifferenttime
points(possibleintra-interventionassessments)withineachgroup,theFriedmanTest
orthenonparametricWilcoxonTest isappliedinthecaseofonlytwomoments.The
change between two time points of a qualitative variable is analysed with the
McNemarTest.
The data analysis will be performed with the statistical program SPSS 23.0 for
Windows.
6.6Collectinginformation:
New in this thesis, we have included involvement with the Faculty of Computer
ScienceattheUniversityofSeville.
Participation is designing a mobile phone application (APP) to facilitate monitoring,
biofeedbackandadherencetotheexercisebypatients.4thyearstudentsofComputer
EngineeringdegreemaychoosethisprojectasFinalProjectduringtheyears2019and
2020.Theprojectisofferedwiththetitleanddescription:
"Toolformonitoringpatientsintherapeuticexerciseperiod."Description:
Theprojectistodevelopamobileapplicationthatwillsupportpatientswhileperformingtherapeuticexercisesindicated.Inaddition,theinformationcollectedbytheapplicationshouldbeavailabletohealthprofessionals,sothatyoucantrackthe
patientandtheanalysisandsubsequentoperationofthedataobtained.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
18
Therebywe facilitatemonitoringofpatients, include theuseofnew technologies in
the study, andwehaveprovidedautility applicationhealth, learningand improving
adherencetoexercise.
7. Workplan:
- Searching:startsinJanuary2019andcontinuesthroughoutthestudy.
- APPdesigntrackingpatients:itsrealizationisofferedasafinaldegreeproject
attheFacultyofComputerEngineeringinApril2019.
- Start of Patient Recruitment: January 2019 to have the necessary sample for
thestudy.
- Data analysis: After completion of sample collection (estimated time approx
January2020)untilMarch2020
- Interpretationofresults:MarchandApril2020.
- Finalreport:July2020.
- Readingandproceduresthesisdefense:September2020.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
19
8. Bibliography:
1. R. O'Reilly, K. Peters, Jackson Beale B. & D. (2009)Women's experiences of
recovery from childbirth: focus on pelvic problems extend beyond the
puerperiumThat.JournalofClinicalNursing18(14),2013-2019.
2. KoelblH.,T. Igawa,S.Salvatore,LaterzaRM,A.Lowry,SievertKD&SultanA.
(2013)Pathophysiologyofurinaryincontinence,faecalincontinenceandpelvic
organ prolapse. In Incontinence, 5th edn (Abrams P., Cardozo L, Khoury S.&
WeinA.,eds),ICUDEAUnotplace,pp.263-359.
3. ThomDH&RortveitG.(2010)Prevalenceofpostpartumurinaryincontinence:
a systematic review. Acta ScandinavicaObstetetrica et Gynecologica 89 (12),
1511-1522.
4. Wai CY, McIntire DD, SD Atnip, Schaffer JI, Bloom SL & Leveno KJ (2011)
Urodynamic indices and pelvic organ prolapse quantification 3 months after
vaginal delivery in primiparous women. International Journal Urogynecology
PelvicFloorDysfunctionand22(10),1293-1298.
5. RetzkySS,RMRogersJr. incontinence inwomenUrinary.ClinSymp.1995;47
(3):2-32.
6. Herzog AR, Fultz NH. Prevalence and incidence of urinary incontinence in
Community-dwellingPopulations.JAmGeriatrSoc1990Mar;38(3):.273-81.
7. RortveitG,DaltveitAK,HannestadYS,HunskaarS.Vaginaldeliveryparameters
and urinary incontinence: the Norwegian EPINCONT study. Am J Obstet
Gynecol.2003;189(5):1268-74.
8. Hernandez Viñaspre Ruiz R, and Thomas C. Aznar "Urinary incontinence
unformed.Prevalenceandassociated factors"GoalsofNursing (2010):13.10,
66-72.
9. WilsonPD,RMHerbison,HerbisonGP.Obstetricpracticeandtheprevalenceof
urinary incontinence threemonthsafterdelivery.Br JObstetGynaecol 1996;
130(2):154-61.
10. MinaireP,SenglerJ,JacquetinB.Épidémiologiedel'incontinenceurinaire.Med
PhysRéadapAnna1995;38:1-8..
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
20
11. E Samuelsson, Victor A. Signs of genital prolapse in women sweadish
population20to59yearsoldofageandpossiblerelatedfactors.AnnJObstet
Gynecol.1999;180:299-305
12. Hernandez Viñaspre Ruiz R, Rubio Aranda E, Thomas C. Aznar urinary to 6
monthspostpartumincontinence.MedClin(Barc)2013;141(4):145-51.
13. Rotveit G, Kjersti A, Hannestad And Hunskaar S. Urinary incontinence after
vaginaldeliveryorcaesareansection.TheNewANDnglandJournalofMedicine
2003;348(10):900-7.
14. DincA,KizilkayaBejiN,YalcinO.Effectofpelvic floormuscleexercises inthe
treatment of urinary incontinence and the postpartum During Pregnancy
period.UroginecolIntJ.2009;20:1223-1231.
15. Dumoulin C, D Bourbonnais, Morin M, D Gravel, Lemieux MC. Predictors of
success for physiotherapy treatment in Women with persistent postpartum
stressurinaryincontinence.ArchPhysMedRehabil.2010;91:1059-1063.
16. Ewings P, Spencer S, H Marsh, M. O'Sullivan Obstetric risk factors and
preventativefoururinaryincontinencepelvicfloorexercises:Cohortstudyand
nestedrandomizedcontrolledtrial.JObstetGynaecol.2005;25:558-64.
17. Rotveit G, Kjersti A, Hannestad And Hunskaar S. Urinary incontinence after
vaginal delivery or caesarean section. The New England Journal ofMedicine
2003;348(10):900-7.
18. Oliveira Camargo F, Rodrigues Moura A, Martins R Arruda, Gracio Sartori
Ferreira M, Batista Castello Girão MJ, Aquino R. Castro Pelvic floor training
muscle in femalestressurinary incontinence:Betweengroupcomparisonand
training single treatment using PERFECT assesment scheme. Urigynecol Int J.
2009;20:1455-1462.
19. Hay-SmithEJ,BoK, LCBerghmans,HJHendriks,DeBieRA,vanWaalwijkvan
DoormES.Pelvicfloormuscletrainingforurinaryincontinenceinwomen.The
CochraneLibrary,Issue1,2001.CochraneDatabaseSystRev.2007
20. NietoBlancoE, J PerezCamacho,AlvarezDavilaV, LedoGarcíaMP,Moriano
BejarP,Perez LorenteM. Impactofurinary incontinenceonqualityof lifeof
womenaged40to65yearsinahealthareaofMadrid.ClinicalNursing.2004;
14:129-35.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
21
21. Schreiner L, TG Santos, Souza AB, CC Nygaard, Silva Filho IG. Electrical
stimulationforurinaryincontinenceinwomen:asystematicreview.IntBrazJ
Urol2013Jul-Aug.;39(4):454-64.
22. NygaardIE,HeitM.Stressurinaryincontinence.ObstetGynecol.2004Sep;104
(3):607-20.
23. Hannestad YS, Rortveit G, Sandvik H, Hunskar S. A community based
epidemiologicalsurveyoffemaleurinaryincontinence:theNorwegianEPICONT
study. Epidemiology of Incontinence in theCounty ofNord- Trondelag. J Clin
Epidemiol.2000Nov;53:1150-7.
24. R. Boyle, Hay-Smith EJ, Cody JD & Mørkved S. (2012) Pelvic floor muscle
training for prevention and treatment of urinary and faecal incontinence in
antenatal and postnatal women. Cochrane Database of Systematic Reviews
(10),CD007471.
25. OblasserC.,Christie J.&McCourtC. (2015)Vaginalconesorballspelvic floor
muscle to Improve performance and urinary continence in women post
partum:aquantitativesystematicreview.Midwifery31(11),1017-1025.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
22
9. ATTACHMENTS:
It isproposedtoparticipate inarandomizedscientificstudyentitled"Evaluationof the effectiveness of a program to strengthen thepelvic floorWOMEN INTHEPOSTPARTUM" which aims to repair the muscles of your pelvic floor muscleslocatedintheregionoftheperineuminvolvedactiveatthetimeofdeliverywiththeaimof increasing itspowerandelasticity in thepuerperalperiod.The studyaimstoassesstheextenttowhichthisstimulationofthepelvicflooriscapableofimproving the injuries of the musculature and indirectly its long-termconsequencessuchasgenitaldescents(bladder,vaginaanduterus), incontinenceorinvoluntaryleakageofurineandeventhedifficultiesvaginalintercourse.
Their participationwould, if accepted, perform a set of exercises pelvic floormuscle exercises and lower abdominal pressure previously will be taught bymidwives. The exercises would be held from 6 weeks postpartum (fulfilledquarantine)until6monthspostpartum.
If you choose to participate, you can withdraw at any time and withoutexplanation of the study. Moreover, the research team guarantees at all times,anonymityandconfidentialityoftheinformationisencryptedandwillbelimitedsolely to their age, parity, clinical data on the evolution of pregnancy, childbirthandpostpartum.
Your participation in this research study does not involve any risk to you oryourbaby,with the informationobtainedgreat interest in the future to increasethefieldofknowledgeandactiononwomen'shealthandqualityoflife.
Fieldworkwilltakeplaceinhealthcentresandatalltimesparticipantswillbecoordinated and supervised by professionals Obstetrics (midwives)whomay atanytime,consultanyaspectofthestudy.
HANDOUT FOR STUDY PARTICIPANTS:
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
23
INFORMED CONSENT STUDY: "Influence of an exercise program low abdominal pressure modified for
pregnancy to strengthen the pelvic floor muscles in pregnant women" I, Ms. _______________________________________________, of age, I stated:
- I have successfully been informed of the nature and purpose of the study, I
have described what is my participation and have notified me that no risk to
my health.
- I understood perfectly the explanations you have offered me and I consent to
participate in the study.
- That I have been informed of my right to withdraw this consent and leave my
participation at any time, at any time of this research, without having to justify
my will, without any loss as to my attention.
Today's date __________________
Date of birth:
Telephone 1: Phone 2:
Health center to which it belongs:
Hospital where she has given birth:
Signed: ___________________________
(Name, surname)
ID: ________________
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
24
UrinaryincontinencequestionnaireICIQ-SFICIQ(InternationalConsultationonIncontinenceQuestionnaire)isaself-administeredquestionnairethatidentifiespeoplewithurinaryincontinenceandtheimpactonqualityoflife.ICIQ-SF:totalscoresquestions1+2+3.IUdiagnosisisconsideredanythingabovezeroscore1.Howoftendoyouleakurine?(Checkonlyoneanswer).Never......................0Onceaweek...........12-3times/week.............2Onceaday................3Severaltimesaday.............4Continually................52. Give your opinion about the amount of urine you think that escapes, ie, theamountofurinethatusuallyloses(whetherornotwearingprotection).Markonlyoneanswer.nothingescapesme.........0Verylittle............2Amoderateamount........4Alotof..............63.Towhatextenttheseleaksurine,whichhasaffectedyourdailylife?12345678910Nothingmuch4.Whendidyouleakurine?Checkallthathappenstoyou.•Never.•Beforereachingtheservice.•Whencoughingorsneezing.•Whilehesleeps.•Whenperformingphysical/exerciseefforts.•Whenyoufinishurinatingandalreadydressed.•Noobviousreason.•continuously.
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
25
DICTAMEN ÚNICO EN LA COMUNIDAD AUTÓNOMA DE ANDALUCÍA
D/Dª: Jose Salas Turrents como secretario/a del CEI de los hospitales universitarios Vírgen Macarena-Virgen del Rocío
CERTIFICA
Que este Comité ha evaluado la propuesta de (No hay promotor/a asociado/a) para realizar el estudio de investigación titulado:
TÍTULO DEL ESTUDIO: Influencia de un programa de ejercicios de baja presión abdominal modificados parael embarazo para el fortalecimiento de la musculatura del suelo pélvico en la mujerembarazada
Protocolo, Versión: PDFHIP, Versión:CI, Versión: PDF
Y que considera que:
Se cumplen los requisitos necesarios de idoneidad del protocolo en relación con los objetivos del estudio y se ajusta a los principioséticos aplicables a este tipo de estudios.
La capacidad del/de la investigador/a y los medios disponibles son apropiados para llevar a cabo el estudio.
Están justificados los riesgos y molestias previsibles para los participantes.
Que los aspectos económicos involucrados en el proyecto, no interfieren con respecto a los postulados éticos.
Y que este Comité considera, que dicho estudio puede ser realizado en los Centros de la Comunidad Autónoma de Andalucíaque se relacionan, para lo cual corresponde a la Dirección del Centro correspondiente determinar si la capacidad y los mediosdisponibles son apropiados para llevar a cabo el estudio.
Lo que firmo en SEVILLA a 24/06/2015
D/Dª. Jose Salas Turrents, como Secretario/a del CEI de los hospitales universitarios Vírgen Macarena-Virgen del Rocío
Código Seguro De Verificación: 5f2df9c0b7d26dc4712fbfaa47cdef336441277d Fecha 24/06/2015Normativa Este documento incorpora firma electrónica reconocida de acuerdo a la Ley 59/2003, de 19 de diciembre, de firma electrónica.
Firmado Por Jose Salas TurrentsUrl De Verificación https://www.juntadeandalucia.es/salud/portaldeetica/xhtml/ayuda/verifica
rFirmaDocumento.iface/code/5f2df9c0b7d26dc4712fbfaa47cdef336441277dPágina 1/2
ThesisProject:"Evaluationoftheeffectivenessofaprogramtostrengthenthepelvicfloorofwomeninthepostpartum"
26



























![DOCTORAL THESIS [TESIS DOCTORAL] - UAM](https://img.dokumen.tips/doc/110x75/62162d5b17f9b23eb24b8a87/doctoral-thesis-tesis-doctoral-uam.jpg)

