-
7/25/2019 Diuretic Dose Ckd
1/8
Diverse diuretics regimens differentially enhance
theantialbuminuric effect of reninangiotensin blockers
in patients with chronic kidney diseaseEnrique Morales1, Jara
Caro1, Eduardo Gutierrez1, Angel Sevillano1, Pilar Aun1, Cristina
Fernandez2 andManuel Praga1,3
1Department of Nephrology, University Hospital 12 de Octubre,
Madrid, Spain; 2Research and Clinical Epidemiology Unit, Department
of
Preventive Medicine, Hospital Clinic, San Carlos, Madrid, Spain
and 3Department of Medicine, Complutense University, Madrid,
Spain
The addition of spironolactone or hydrochlorothiazide
enhances the antialbuminuric effect of reninangiotensin
blockers. However, comparative studies on the effect of
different diuretics are lacking. We conducted a
prospectiverandomized crossover study to compare the effects of
spironolactone (25 mg/day), hydrochlorothiazide (50 mg/day)
without/with amiloride (5 mg/day) on top of enalapril
treatment in 21 patients with CKD stages 13 and a urinary
albumin-to-creatinine ratio (UACR) over 300 mg/g. Treatment
periods lasted 4 weeks. The UACR showed a significant
reduction with the diuretics: spironolactone, 34% or
hydrochlorothiazide without/with amiloride 42% or 56%,
respectively. Reduction of the UACR was significantly
greater
with hydrochlorothiazide without/with amiloride when
compared with spironolactone. The percentage of patients
who achieved UACR reductions greater than 30% and 50%
was greater with hydrochlorothiazide without/with amiloride
(81% and 57%, and 81% and 66%, respectively) when
compared with spironolactone alone (57% and 28%,
respectively). Glomerular filtration rate (GFR), blood
pressure,
and body weight decreased with the three diuretic regimens.
A significant correlation was found between the UACR
reduction and GFR and blood pressure changes. Thus, diverse
diuretic regimens differentially enhance albuminuria
reduction, an effect likely associated with the degree of
GFR
reduction.
Kidney International (2015) 88, 14341441;
doi:10.1038/ki.2015.249;
published online 26 August 2015
KEYWORDS: albuminuria; amiloride; diuretics;
hydrochlorothiazide; RAASblockade; spironolactone
The most important therapeutic strategies for slowing
theprogression of chronic kidney disease (CKD) and reducingthe
disproportionate cardiovascular risk of CKD patients are
controlling blood pressure (BP) and reducing albuminuria.1
7Reninangiotensinaldosterone system (RAAS)
blockers(angiotensin-converting enzyme inhibitors (ACEIs)
andangiotensin II receptor blockers (ARBs)) are the backboneof
these therapies due to their efficacy in controlling BP andtheir
known antialbuminuric effect. The favorable influenceof these drugs
on the progression of chronic diabetic andnondiabetic nephropathy
has been demonstrated in severalprospective controlled studies.39
This favorable influence hasa close relationship with the reduction
of albuminuria; themore intense the reduction in albuminuria the
greaterthe reduction in the risk of progression of CKD.4,7
However,
the antialbuminuric effect of RAAS blockers is mild ornegligible
in a substantial number of CKD patients. The so-called residual
albuminuria (i.e., the level of albuminuriathat persists after
reaching the maximum tolerated dosage ofRAAS blockers and proper BP
control) is considered one ofthe most significant factors in the
progression of kidneydamage.1013 Therefore, the search for new
alternatives thatenhance the antialbuminuric effect of ACEIs and
ARBs is ofparamount importance.
In recent years, several studies have demonstrated
theantialbuminuric potential of aldosterone receptor
antagonists(spironolactone (SR) and eplerenone).1421 Likewise,
observa-tional studies have suggested that this reduction in
albumi-
nuria, as occurs with ACEIs and ARBs, is associated with
asignificant reduction in the risk of progression of
CKD.18,2023
Nevertheless, prospective controlled studies have not
beenperformed with the duration necessary to demonstrate
therenoprotective effect of aldosterone antagonist
diuretics.Moreover, the combination of these diuretics with ACEIs
orARBs increases the risk of hyperkalemia, especially in
patientswith reduced glomerular filtration.18,20,21,23
Compared with the extensive experimental and clinicalresearch
performed on aldosterone antagonist diuretics, the
possible antialbuminuric effect of other diuretics has been
scarcely studied. However, several clinical studies have
shown
c l i n i c a l t r i a l
http://www.kidney-international.org
2015 International Society of Nephrology
Correspondence: Manuel Praga, Servicio de Nefrologa, Hospital 12
de
Octubre, Avenida Crdoba s/n., Madrid 28041, Spain.
E-mail:[email protected]
Received 5 April 2015; revised 20 June 2015; accepted 25 June
2015;
published online 26 August 2015
1434 Kidney International (2015) 88 , 14341441
http://dx.doi.org/10.1038/ki.2015.249http://www.kidney-international.org/mailto:[email protected]:[email protected]://www.kidney-international.org/http://dx.doi.org/10.1038/ki.2015.249
-
7/25/2019 Diuretic Dose Ckd
2/8
that hydrochlorothiazide (HCT), at dosages of 2550
mg/day,induces powerful albuminuria reductions in patients with
orwithout diabetes who have residual albuminuria despitemaximum
dosages of ACEIs or ARBs.2426 This antialbumi-nuric effect was
similar to that achieved with a low-sodiumdiet. The combination of
the two measures (HCT plus a low-sodium diet) achieved a very
significant reduction inalbuminuria, greater than that achieved by
each measure inisolation.24,26 Other studies have shown that
furosemide canalso boost the antialbuminuric effect of ACEIs and
ARBs.27,28
There is no clinical information available on
amilorideconcerning its possible antialbuminuric effect, but
experi-mental models have suggested a possible nephroprotectiverole
of this diuretic.29,30
To the best of our knowledge, there are no clinical studiesthat
have compared the antialbuminuric efficacy of varioustypes of
diuretics. This information would be extremelyimportant for the
design of renoprotective clinical strategies,given that the use of
various types of diuretics is standard
practice for controlling BP and volume overload in CKDpatients.
Aim of our study was to compare the antialbumi-nuric effect of SR,
HCT, and amiloride. However, amiloride isusually marketed in
combination with HCT in mostcountries, including ours. We therefore
designed a prospec-tive, randomized crossover study to compare the
antialbu-minuric effect of SR, HCT, and HCT+amiloride (A)
forpatients with CKD and a urinary albumin-to-creatinine
ratio(UACR) 4300 mg/g.
RESULTS
Of the 29 initially selected patients, 21 patients provided
their
informed consent and started the study. Three patients
wereexcluded for presenting UACR o300 mg/g, three patientswere
excluded because of lack of motivation to continue withthe study,
and two patients were excluded for other causes(Figure 1).
Table 1 reflects baseline clinical and biochemical
char-acteristics at the end of the run-in period for the
21randomized patients. Almost half of the patients had diabetesand
the other half had various glomerular conditions. In all,3 patients
had stage 1 CKD, 10 patients stage 2 CKD, and 8patients stage 3
CKD. During the study, there was very goodtreatment adherence to
the various types of diuretics in allpatients (490% of SR, HCT, and
HCT+A pills during the
three treatment periods). Two patients had to reduce
theenalapril dosage (20 mg/day) because of excessive BP controlin
the HCT+A group.
Main objective
As can be seen in Table 2, UACR showed a significantreduction
with the three types of diuretics: SR, 34% (95%confidence interval
(CI)= 21 to 47; P= 0.001); HCT, 42% (95% CI = 28 to 56; P= 0.001);
and HCT+A, 56% (95% CI = 44 to 67; P= 0.001). UACR reductionwas
significantly greater with HCT and HCT+A whencompared with SR.
Secondary objectives
The percentage of patients who achieved UACR reductions430 and
450% was also greater with HCT and HCT+A whencompared with SR,
although these differences did not reachstatistical significance
(Table 2). There was a 430% reductionin UACR in 12 patients (57%)
treated with SR and in 17patients (81%) treated with HCT or HCT+A.
The percentage ofpatients with 450% UACR reduction was greater in
theHCT+A group (14 patients (66%)) compared with the HCTgroup (12
patients (57%)) and SR group (6 patients (28%)).24-h proteinuria
and 24-h albuminuria also showed significantreductions with the
three types of diuretics, without significantbetween-group
differences (Table 2).
Tertiary objectives
Estimated glomerular filtration rate (eGFR) was reduced withthe
three types of diuretics, as shown in Table 3. Thisreduction was
statistically significant with HCT (8.5%(95% CI= 3.8 to 13.3; P=
0.002)) and with HCT+A(
12% (95% CI=
5.9 to
18.1; P= 0.001)), whereasit did not reach statistical
significance with SR (6% (95%CI= 0.9 to 11.9)). There were no
statistically significantbetween-group differences. As shown
inTable 3, BP (systolicBP, diastolic BP, and mean arterial
pressure) decreased withthe three types of diuretic treatment. This
decrease achievedstatistical significance with SR and with HCT+A.
Body weightalso decreased with the three types of diuretics (Table
3),reaching statistical significance with SR and HCT+A. Therewere
no significant between-group differences regarding BPand body
weight changes.
Other parameters
There were no significant changes in plasma sodium levelswith
any of the diuretics, whereas serum potassium levelsexperienced a
significant increase with SR and HCT+A(Table 4). Urinary excretions
of sodium and potassiumshowed no significant changes (Table 4).
Uric acid levelsincreased significantly with all study diuretics,
with nobetween-group differences (Table 4). As expected, renin
andaldosterone levels showed an increase with all types
ofdiuretics, which was significant in all cases except for
theincrease in aldosterone levels in patients treated with
HCT(Table 4). No significant between-group differences
were found.
Correlations and multivariate analysis
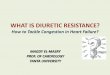
As shown in Figure 2, we found a significant correlationbetween
changes in UACR and eGFR when analyzing alltreatment periods (r=
0.50, P= 0.002) and in each of thethree types of diuretics
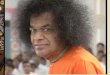
separately. Changes in UACR alsoshowed a significant correlation
with BP changes whenanalyzing all treatment periods (Figure 3),
although it did notreach statistical significance when the various
diuretics wereanalyzed separately. No significant correlation
between UACRand weight changes was found.
E Moraleset al.: Antialbuminuric effect of diuretics c l i n i c
a l t r i a l
Kidney International (2015) 88 , 14341441 1435
-
7/25/2019 Diuretic Dose Ckd
3/8
Adverse effects
Tolerance to the three types of diuretics was good,
withouthypotension episodes. As shown inTable 4, serum
potassiumshowed a significant increase with SR and HCT+A,
althoughno episodes of severe hyperkalemia (serum potassium45.5
mEq/l) were observed. The number of patients showing
a serum potassium of 5 mEq/l or higher was 7 (33%) with SR,2
(9%) with HCT, and 9 (42%) with HCT+A. None of thepatients
discontinued the study during the follow-up. Allrandomized patients
completed the three treatment periods.
DISCUSSION
Our study is the first head-to-head comparison of the
antialbuminuric effect of three different types of diuretics
inpatients who had UACR4 300 mg/g despite maximal dosesof ACEI and
an acceptable control of BP. Our data show asignificant reduction
in albuminuria with the three types ofdiuretics used: SR, HCT, and
HCT+A. Regarding SR, ourstudy confirms its antialbuminuric
properties, which havebeen previously demonstrated in both
observational studiesand prospective controlled trials.1421 We
found a 34%(95% CI= 21 to 47) reduction in UACR baseline
valuesafter 4 weeks of treatment with 25 mg/day of SR. This dosehas
been the most commonly used in previous studies thatexamined the
antialbuminuric effect of SR.1421
But the most important and novel findings of our study
are that HCT, at doses of 50 mg/day, achieved a reductionin UACR
(42%; 95% CI= 28 to 56), which wassignificantly higher than that
obtained with SR, and that theUACR reduction was even more marked
when patients weretreated with the combination HCT+A (56%; 95% CI=
44to 67). Similarly, the percentage of patients who presentedUACR
reductions greater than 30 and 50% of baseline valueswas higher
with HCT or HCT+A as compared with SR(Table 2), although these
differences were not statisticallysignificant. It should be
stressed that the percentageof patients who reduced their UACR in
more than 50% ofbaseline values was 57% with HCT and 66% with
HCT+A.
41 Patients eligible and subsequentlyinvited for
participation
12 Declined participation
29 Enrolled in the run-in period
8 Excluded
3 Lack of motivation to adhere to study procedures
3 Albumin:creatinine excretion (mg/g)
-
7/25/2019 Diuretic Dose Ckd
4/8
Previous studies had demonstrated an antialbuminuriceffect of
HCT in chronic nephropathies.2426 Vogt et al.24
showed in a prospective, randomized, crossover study
conducted in non-diabetic patients with proteinuria
thatlosartan, at a dose of 100 mg/day, reduced proteinuria by30%.
The addition of a low-salt diet increased theanti-proteinuric
effect of losartan up to 55%, and that ofHCT (25 mg/day) up to 56%.
When a low-salt diet and HCTwere simultaneously added to losartan,
proteinuria reductionsreached 70% of baseline values. Another
crossover, prospec-tive, and randomized study showed that the
administration of50 mg/day of HCT for 6 weeks had the same effect
on residualalbuminuria of diabetic patients treated with maximal
ACEIdose than a low-sodium diet (42% reduction for bothmeasures),
whereas the simultaneous application of both
measures (low-sodium diet+50 mg/day of HCT) reducedalbuminuria
by 61%.26 Our study confirms the strongantialbuminuric effect of
HCT on top of maximal ACEI
doses and without changes in salt intake, and is the first
todemonstrate that the HCT-induced reduction in albuminuriais
greater than that caused by SR at doses of 25 mg/day andthat the
addition of amiloride to HCT increases furtheralbuminuria
reduction.
The exact mechanisms by which the anti-aldosteronediuretics (SR,
eplerenone) induce a significant reduction
ofproteinuria/albuminuria have not been clarified.1421
Experi-mental studies have shown that aldosterone infusions
causedirect damage to podocytes, which ultimately leads to
theappearance of proteinuria and glomerulosclerosis.31,32 SR
oreplerenone administration in these same experimental models
Table 2 |Effects of diuretics on albuminuria and proteinuria
Spironol actone Hydrochlorothiazide H ydrochl
orothiazide+amiloride
Baseline 4 Weeks Baseline 4 Weeks Baseline 4 weeks
UACR (mg/g) 810 (6011020) 742* (2411244) 1011 (8031218) 566*+
(205927) 1135 (9261344) 398*+ (212584)% UACR reduction 34 (2147) 42
(2856) 56 (4467)
Patients with 430% UACR reduction (%) 12 (57) 17 (81) 17
(81)
Patients with 450% UACR reduction (%) 6 (28) 12 (57) 14 (66)
24-H Albuminuria (mg) 1600 (10472152) 1125.2* (5001750) 1417
(8681965) 935* (2661603) 1882 (13252440) 577* (300855)
24-H Proteinuria (g) 1.7 (1.32.2) 1.5* (0.82.3) 1.7 (1.32.1)
1.3* (0.62) 2.4 (1.92.8) 0.9* (0.61.2)
Abbreviation: UACR, urinary albumin-to-creatinine ratio.
*Po0.05 for intragroup comparison; +Po0.05 for between-group
comparison.
Table 3 |Effects of diuretics on renal function, blood pressure,
and weight
Spironolactone Hydrochlorothiazide
Hydrochlorothiazide+amiloride
Baseline 4 Weeks Baseline 4 Weeks Baseline 4 Weeks
Serum creatinine (mg/dl) 1.17 (0.4) 1.25 (0.4) 1.15 (0.3) 1.26
(0.4)* 1.21 (0.4) 1.35 (0.4)*eGFR ml/min per
1.73 m266 (26) 62 (26) 66 (25) 60 (24)* 64 (24) 55 (20)*
% eGFR reduction 6 (0.911.9) 8.5 (3.813.3) 12 (5.918.1)
SBP (mm Hg) 130 (18) 125 (20)* 129 (18) 124 (19) 128 (20) 121
(15)*DBP (mm Hg) 76 (13) 72 (10)* 75 (12) 71 (7) 74 (12) 70
(8)*
MAP (mm Hg) 87 (5) 85 (5)* 86 (3) 85 (4) 86 (4) 84 (4)*
% MAP reduction 2.1 (0.63.6) 1 (0.62.6) 2.7 (0.84.6)
Weight (kg) 89.1 (15.6) 88.1 (15.6)* 89.1 (16.2) 88.5 (15.2)
88.6 (15.3) 87.3 (15.1)*
% Weight reduction 1.2 (0.22.1) 0.4 (0.51.4) 1.3 (0.52.1)
Abbreviations: DBP, diastolic blood pressure; eGFR, estimated
glomerular filtration rate; MAP, mean arterial pressure; SBP,
systolic blood pressure.
*Po0.05 for intragroup comparisons.
Table 4 |Effects of diuretics on other biochemical
parameters
Spironolactone Hydrochlorothiazide
Hydrochlorothiazide+amiloride
Baseline 4 Weeks Baseline 4 Weeks Baseline 4 Weeks
Sodium (mEq/l) 141 (2.8) 140 (1.8) 140 (3.4) 140 (2.3) 141 (1.9)
140 (2.7)
Potassium (mEq/l) 4.7 (0.4) 5 (0.6)* 4.6 (0.4) 4.5 (0.4) 4.6
(0.5) 5 (0.6)*
Urinary sodium (mEq/24 h) 184 (152261) 227 (183271) 216 (175256)
240 (146333) 194 (160227) 208 (164253)
Urinary potassium (mEq/24 h) 73 (5987) 79 (6791) 77 (6788) 80
(56105) 80 (6694) 76 (6791)
Uric acid (mg/dl) 6.3 (1.4) 6.8 (1.8)* 6.5 (1.5) 7.3 (1.6)* 6.4
(1.5) 7.6 (1.7)*
Renin (pg/ml) 47 (2866) 82* (37126) 46 (2765) 106* (50163) 34
(1354) 168* (95241)Aldosterone (pg/ml) 150 (110198) 203* (162244)
166 (127205) 182 (142222) 119 (80158) 298* (198398)
*Po0.05 for intragroup comparisons.
Kidney International (2015) 88 , 14341441 1437
E Moraleset al.: Antialbuminuric effect of diuretics c l i n i c
a l t r i a l
-
7/25/2019 Diuretic Dose Ckd
5/8
largely prevents aldosterone detrimental effects.31,33
Relativeto amiloride, experimental studies have shown reductions
inproteinuria and a regression of glomerular lesions inhypertensive
rats29 and improvements in podocyte lesionsand glomerulosclerosis
in the 5/6 nephrectomy rat modeltreated with this drug, probably
mediated by an inhibition ofurokinase receptor.30 However, to our
knowledge, no clinicalstudies have previously evaluated the effect
of amiloride onpatients with proteinuria.
Regarding HCT, no specific mechanisms that may explainits
antialbuminuric effect have been elucidated. It has
beensuggested25,26 that HCT-induced antialbuminuric effect maybe
caused by volume depletion, thereby decreasing theintraglomerular
hypertension that typically accompaniesCKD. Although no concrete
data to support such hypothesishave been reported, the similar
antialbuminuric effect of HCTand salt-free diet, as well as the
synergistic effect of the twomeasures24,26 support this
possibility. If this hypothesis provesto be true, the same
mechanism (reduced glomerularintracapillary pressure secondary to
diuretic-induced volumedepletion) could be shared by any type of
diuretic, including
SR, eplerenone or amiloride, independently of
drug-specificantialbuminuric mechanisms. In favor of a possible
anti-albuminuric overall effect of diuretics, some studies
haveshown that furosemide also potentiates the
antialbuminuriceffect of RAAS blockade.27,28
Data from our study are also in agreement with a
possibleinfluence of volume depletion in the antialbuminuric effect
ofdiuretics. In line with previous studies,2426,34 we found
adecrease in BP, eGFR, and body weight with the three types
ofdiuretics, a decrease that reached statistical significance
withseveral of them (Table 3). As shown inFigures 2and3, bothBP and
eGFR decrease showed a statistically significantcorrelation with
the reduction in albuminuria. The differenteffects of SR, HCT, and
HCT+A on albuminuria coulddepend, therefore, on their potency to
reduce plasma volume.In addition, many studies have shown that both
BP loweringand weight loss induce significant albuminuria
reduction.35,36
However, it is unlikely that BP and eGFR lowering alone
canexplain the antialbuminuric effect of diuretics. Mean BP
reduction was 2.1%, 1%, and 2.7% with SR, HCT, andHCT+A,
respectively, and eGFR reduction was 6%, 8.5%, and12% in the same
periods, whereas UACR reduction achieved34%, 42%, and 56% of the
baseline values with SR, HCT, andHCT+A, respectively (Tables
2and3). BP, eGFR, and bodyweight decrease, as well as the
significant increase in uric acid,plasma renin, and plasma
aldosterone (Table 4), are likelyconsequences of the volume
depletion induced by diuretics.Studies are needed to accurately
analyze the relationshipbetween hemodynamic changes induced by
diuretics andtheir effect on albuminuria and glomerular
filtrationrate (GFR).
Our study shows that both SR and HCT or HCT+Acombination are
powerful drugs to enhance the antialbumi-nuric effect of RAAS
blockade. Given the far-reachinginfluence of the amount of
albuminuria on the progressionof renal diseases,4,7,1013 reductions
in albuminuria by anytherapeutic measure are usually equated to a
renoprotectiveinfluence. However, we believe that the potential
renopro-tective effect of diuretics should be evaluated by means
ofprospective studies of sufficient duration to establish
renaloutcomes. Although diuretic tolerance was good in ourpatients
and reduced GFR reversible in all the cases, theefficacy and safety
of their long-term administration needs tobe demonstrated. Serum
potassium showed a significant
increase with SR and HCT+A, so using these medications forlonger
than 4 weeks may exacerbate the risk of serioushyperkalemia. On the
other hand, previous studies haveshown that an initial reduction of
GFR in patients treatedwith ARB or SR23,37 predicts a subsequent
long-termrenoprotective effect, probably reflecting a salutary
reversalof glomerular hyperfiltration.
As a large proportion of CKD patients are treated withdiuretics
for the treatment of hypertension, volume overload,or heart
failure, our data showing that thiazide diuretics andamiloride
portend an important antialbuminuric effect, evenhigher than that
of SR, are of considerable practical interest
0.40
0.20
0.00
0.20
0.40
0.60
0.80
1.00
0.40 0.20 0.00 0.20
r= 0.50, P= 0.001
r=0.62, P= 0.002 r=0.43, P=0.04 r= 0.44, P=0.04
%U
ACRchange
%U
ACRchange
% GFR change
HCT HCT+A SR
0.40
0.200.00
0.20
0.40
0.60
0.80
1.00
0.40
0.200.00
0.20
0.40
0.200.00
0.20
0.40
0.200.00
0.20
% GFR change
Figure 2 |Relationship between changes in glomerular
filtrationrate (GFR) and changes in urinary albumin-to-creatinine
ratio
(UACR).
1438 Kidney International (2015) 88 , 14341441
c l i n i c a l t r i a l E Moraleset al.: Antialbuminuric
effect of diuretics
-
7/25/2019 Diuretic Dose Ckd
6/8
for the design of therapeutic strategies for these patients.
Forexample, hyperkalemia is a serious potential risk in
patientstreated with ACEI, ARB, or antialdosterone
diuretics,particularly when kidney function is impaired.1421,38
Accord-ing to our data, HCT could be an attractive
therapeuticalternative, owing to its antialbuminuric and kaliuretic
effects,in patients with residual albuminuria in whom RAASblockade
optimization is hampered by hyperkalemia.Combining HCT and SR is
another interesting alternative in
patients prone to develop hyperkalemia.Our study has important
limitations. We analyzed short-
term effects of diuretics on intermediate end points, thus
noconclusions can be drawn about the sustainability of
theantialbuminuric effect or the possible long-term renoprotec-tive
effect of these drugs. As in our country there are onlydrugs with
amiloride in combination with HCT, we could notevaluate the
separate antialbuminuric effect of amiloride. Thesmall sample size
prevented from adjustment of additionalfactors that affect the
outcome. However, the prospective,randomized, and crossover design
of the study, whichincluded washout periods to more properly
analyze the
separate effects of each diuretic, reinforces the robustness
ofthe data.
In conclusion, the addition of SR, HCT, or HCT+A topatients with
UACR4 300 mg/day on top of maximum doseof ACEI, induces a
significant antialbuminuric effect,which was even higher with HCT
or HCT+A as comparedwith SR, likely associated with a more profound
reduction ofGFR in HCT or HCT+A groups. Further prospective
studiesare needed to evaluate the long-term renoprotectiveinfluence
of these albuminuria-lowering effects of diuretictreatment.
METHODS
This was an open, single-center, randomized crossover study
that
compared the antiproteinuric effect of three types of diuretics,
SR,
HCT, HCT+A in patients with CKD and a UACR 4300 mg/g
(EudraCT No: 2011-001929-24).
Patients
Candidates were identified at the Nephrology Division of
theHospital 12 de Octubre. The study protocol was approved by
the
Ethics Committee of Hospital 12 Octubre, and all study
patients
read and signed the informed consent document before starting
the
study. The included patients met the following criteria: male
or
female older than 18 years, chronic diabetic or nondiabetic
nephropathies, UACR 4300 mg/g, stable renal function during
the last 3 months, GFR 430 ml/min per 1.73 m2 and treatment
with ACEIs or ARBs in stable dosages during the last 3
months.
Patients were excluded from the study if they had poorly
controlled
BP (systolic BP4160 mm Hg or diastolic BP4100 mm Hg),
a history of cardiovascular events (stroke, ischemic heart
disease)
in the past 6 months, or were on treatment with nonsteroidal
anti-
inflammatory drugs, corticosteroids, or other immunosuppres-
sants. The other exclusion criteria were a history of
renovasculardisease, obstructive uropathy, autoimmune disease,
cancer,
pregnancy or currently breastfeeding, and allergies or
intolerance
to HCT, SR, or amiloride.
The patients who met the inclusion/exclusion criteria in the
screening underwent a 3-month run-in period (Figure 1)
during
which the ACEIs or ARBs they were taking were replaced by
enalapril, the dosage of which was progressively increased until
the
maximum dosage of 40 mg/day was reached. This dosage
remained
fixed at that point and throughout all trial periods.
Randomization
All participants who by the end of the run-in period continued
to
meet the inclusion/exclusion criteria were randomly assigned to
oneof the three types of diuretic treatment, in a 1:1:1 ratio.
The
randomized assignment list was generated by a computer at
the
Clinical Research Unit of Hospital 12 de Octubre. All
participants
underwent the three types of diuretic treatment; the sequence
of
these treatments was established randomly, with cleansing
periods
between each of the three distinct treatments (Figure 1).
Procedures
Treatment periods with SR (25 mg/day), HCT (50 mg/day), and
HCT (50 mg/day)+A (5 mg/day) lasted 4 weeks each and were
separated by washout periods of the same length (Figure 2) to
avoid a
carry-over effect. The HCT dose was selected because amiloride
is
0.40
0.40
0.20
0.00
0.20
0.40
0.60
0.80
1.00
0.200.00
0.20
0.40
0.60
0.80
1.00
%U
ACRchange
%U
ACRchange
r= 0.33, P= 0.006
r= 0.27, P=0.22 r=0.30, P=0.17 r=0.41, P=0.06
% MAP change
% MAP change
HCT HCT+A SR
0.10
0.05
0.00
0.05
0.10
0.10
0.05
0.00
0.05
0.10
0.10
0.05
0.00
0.05
0.10
0.10 0.05 0.00 0.05 0.10
Figure 3 | Relationship between changes in mean arterial
pressure
(MAP) and changes in urinary albumin-to-creatinine ratio
(UACR).
Kidney International (2015) 88 , 14341441 1439
E Moraleset al.: Antialbuminuric effect of diuretics c l i n i c
a l t r i a l
-
7/25/2019 Diuretic Dose Ckd
7/8
marketed in combination with the same HCT dosage (50 mg).
Enalapril dosage was kept fixed (40 mg/day) throughout the
trial,
and the patients remaining standard medication was also
main-
tained without changes. The study drug was administered in
the
morning. At the start and end of each of the three different
treatments (SR, HCT, HCT+A), patients body weight, body mass
index, BP, and heart rate were measured. The blood tests
performed
at the start and end of each treatment period were as follows:
serumcreatinine, glucose, glycated hemoglobin (for patients with
diabetes),
sodium, potassium, calcium, chloride, total cholesterol,
high-density
lipoprotein-cholesterol, low-density lipoprotein-cholesterol
(calcu-
lated according to the Friedewald formula), triglycerides, uric
acid,
liver enzymes, plasma renin, and aldosterone. Patients were
instructed to collect 24-h urine during the day before
visit.
Albuminuria, proteinuria, sodium, potassium, urea, and
creatinine
were measured in this urine sample. A first morning urine
sample
was collected to determine UACR.
Body mass index was calculated as weight/height squared. BP
was
measured after 5 min of rest with the participant seated,
with
automatic equipment (OMRON, Lake Forest, IL), and the mean
of
three readings was recorded. Mean arterial pressure was
calculated as
the sum of one-third of the systolic BP and two-third of the
diastolic
BP. Plasma renin activity and aldosterone concentrations
were
measured by radioimmunoassay. The eGFR was measured using
the
MDRD-4 formula.
Objectives
The main study objective was the percentage change in the median
of
UACR between the baseline and final value of each treatment
period.
The secondary objectives were the proportion of patients who
achieved a 430 or 450% reduction in the UACR and the
percentage change in the median of the 24-h albuminuria and
proteinuria in the three different treatment periods. The
tertiary
objectives were the percentage change between the baseline
valuesand the end values of each treatment period for the
following
parameters: eGFR, systolic BP, diastolic BP, mean arterial
pressure,
and weight. The tolerance and adverse effects for each
treatment
period were recorded.
Statistical analysis
Normally distributed continuous variables are presented as
mean
standard deviation or median and interquartil range
(P25P75).
Variables were analyzed for a normal distribution with the
KolmogorovSmirnov test. Categorical variables are expressed
as
frequencies and percentages. CIs and all tests of
statistical
significance for treatment comparisons were evaluated at a
two-tailed significance level of 0.05.
All statistical comparisons of variables between treatment
groups
for the primary and secondary objectives with continuous
variables
were conducted using a linear mixed-effect model for
repeated
measures. In this model, baseline levels of percentage change in
the
median of proteinuria between the baseline and final value of
each
treatment period were considered as covariance, participants
as
random effects, and treatment group, sequence, and
treatment-
group-by-sequence (treatment by period interaction to test for
carry-
over effects) as fixed effects. Method used to fit such mixed
models is
that of expectationmaximization algorithm where the variance
components (intragroup and between group comparison) are
treated
as unobserved nuisance parameters in the joint likelihood.
All analyses were conducted in all randomized participants
who
were treated with at least one dose of the study drug.
Statistical
analyses were performed using SPSS/PC 17 (SPSS Inc. Chicago,
IL).
DISCLOSURE
The authors declare no conflict of interest.
ACKNOWLEDGMENTSThis study was supported by grants from
Ministerio de Sanidad yPoltica Social (Ministry of Health and
Social Policy; 1392-H-199),REDinREN (RD012/0021), FIS (Fondo de
Investigaciones Sanitarias)10/02668 and 13/02502 and Asociacin para
la Investigacin yTratamiento de la Enfermedad Renal (AITER,
Association for theResearch and Treatment of Kidney Disease). We
thank Rosa MaraVega Viaa for her cooperation throughout the
preparation andmanagement of the clinical trial.
REFERENCES1. El-Atat FA, Stas SN, McFarlane SIet al. The
relationship between
hyperinsulinemia, hypertension and progressive renal disease. J
Am SocNephrol2004; 15: 28162827.
2. Remuzzi G, Bertani T. Pathophysiology of progressive
nephropathies.
New Engl J Med1998; 339: 1448
1456.3. Holtkamp FA, de Zeeuw D, de Graeff PAet al. Albuminuria
and bloodpressure, independent targets for cardioprotective therapy
in patientswith diabetes and nephropathy: a post hoc analysis of
the combinedRENAAL and IDNT trials. Eur Heart J2011; 32:
14931499.
4. Eijkelkamp WB, Zhang Z, Remuzzi Get al. Albuminuria is a
target forrenoprotective therapy independent from blood pressure in
patients withtype 2 diabetic nephropathy: post hoc analysis from
the Reduction ofEndpoints in NIDDM with the Angiotensin II
Antagonist Losartan(RENAAL) trial. J Am Soc Nephrol2007; 18:
15401546.
5. Remuzzi G, Ruggenenti P, Perna Aet al; RENAAL Study Group.
Continuumof renoprotection with losartan at all stages of type 2
diabeticnephropathy: a post hoc analysis of the RENAAL trial
results. J Am SocNephrol2004; 15: 31173125.
6. de Zeeuw D, Remuzzi G, Parving HHet al. Albuminuria, a
therapeutictarget for cardiovascular protection in type 2 diabetic
patients withnephropathy.Circulation 2004; 110: 921927.
7. de Zeeuw D, Remuzzi G, Parving HHet al. Proteinuria, a target
forrenoprotection in patients with type 2 diabetic nephropathy:
lessonsfrom RENAAL. Kidney Int2004; 65: 23092320.
8. Parving HH, Lehnert H, Brchner-Mortensen Jet al. Irbesartan
in Patientswith Type 2 Diabetes and Microalbuminuria Study Group.
The effect ofirbersartan on the development of diabetic nephropathy
in patients withtype 2 diabetes. N Engl J Med2001; 345: 870878.
9. Kshirsagar AV, Joy MS, Hogan SLet al. Effect of ACE
inhibitors in diabeticand nondiabetic chronic renal disease: a
systematic overview ofrandomized placebo controlled trials.Am J
Kidney Dis 2000; 35: 695707.
10. Ruggenenti P, Perna A, Remuzzi G. Retarding progression of
chronic renaldisease: the neglected issue of residual proteinuria.
Kidney Int2003; 63:22542261.
11. Stevens LA, Greene T, Levey AS. Surrogate end points for
clinical trials ofkidney disease progression. Clin J Am Soc
Nephrol2006; 1: 874884.
12. Praga M, Morales E. Renal damage associated with
proteinuria.Kidney Int2002; 62: S42S46.
13. Jafar TH, Schmid CH, Landa Met al. Angiotensin-converting
enzymeinhibitors and progression of nondiabetic renal disease. A
meta-analysisof patient-level data. Ann Intern Med2001; 135:
7387.
14. Sato A, Hayashi K, Saruta T. Antiproteinuric effects of
mineralocorticoidreceptor blockade in patients with chronic renal
disease. Am JHypertension2005; 18: 4449.
15. Rachmani R, Slavachevsky I, Amit Met al. The effect of
spironolactone,cilazapril and their combination on albuminuria in
patients withhypertension and diabetic nephropathy is independent
of blood pressurereduction: a randomized controlled study.Diabet
Med2004;21: 471475.
16. Rossing K, Schjoedt KJ, Smidt UMet al. Beneficial effects of
addingspironolactone to recomendad antihypertensive treatment in
diabeticnephopathy: a randomized, double-masked, cross over study.
DiabetesCare2005; 28: 21062112.
17. Crysostomou A, Pedagogos E, MacGregor L et al. Double-blind,
placebocontrolled study on the effect of the aldosterone receptor
antagonistspironolactone in patients who have persistent
proteinuria and are on
1440 Kidney International (2015) 88 , 14341441
c l i n i c a l t r i a l E Moraleset al.: Antialbuminuric
effect of diuretics
-
7/25/2019 Diuretic Dose Ckd
8/8
long-term angiotensin-converting enzyme inhibitor therapy with
orwithout an angiotensin II receptor blocker. Clin J Am Soc
Nephrol2006; 1:256262.
18. Hirsch JS, Drexler Y, Bomback AS. Aldosterone blockade in
chronic kidneydisease.Semin Nephrol2014; 34: 307322.
19. Mehdi UF, Adams-Huet B, Raskin Pet al.Addition of
angiotensin receptorblockade or mineralocorticoid antagonism to
maximal angiotensin-converting enzyme inhibition in diabetic
nephropathy. J Am Soc Nephrol2009; 20: 26412650.
20. Bomback AS, Kshirsagar AV, Amamoo MAet al. Change in
proteinuriaafter adding aldosterone blockers to ACE inhibitors or
angiotensinreceptor blockers in CKD: a systematic review. Am J
Kidney Dis 2008; 51:199211.
21. Bolignano D, Palmer SC, Navaneethan SDet al. Aldosterone
antagonistsfor preventing the progression of chronic kidney
disease. CochraneDatabase Syst Rev2014; 4: CD007004.
22. Morales E, Huerta A, Gutierrez Eet al. The antiproteinuric
effect of theblockage of the renin-angiotensin-aldosterone system
(RAAS) in obesepatients. Which treatment option is the most
effective?. Nefrologia 2009;29: 421429.
23. Morales E, Millet VG, Rojas-Rivera J et al. Renoprotective
effectsof mineralocorticoid receptor blockers in patients with
proteinurickidney diseases. Nephrol Dial Transplant2013; 28
:405412.
24. Vogt L, Waanders F, Boomsma Fet al. Effects of dietary
sodium andhydrochlorothiazide on the antiproteinuric efficacy of
losartan. J Am Soc
Nephrol2008; 19: 999
1007.25. Buter H, Hemmelder MH, Navis Get al.The blunting of the
antiproteinuric
efficacy of ACE inhibition by high sodium intake can be
restoredby hydrochlorothiazide. Nephrol Dial Transplant1998;
13:16821685.
26. Kwakernaak AJ, Krikken JA, Binnenmars SHet al; Holland
NephrologyStudy (HONEST) Group. Effects of sodium restriction
andhydrochlorothiazide on RAAS blockade efficacy in diabetic
nephropathy:a randomised clinical trial. Lancet Diabetes
Endocrinol2014;2: 385395.
27. Esnault VL, Ekhlas A, Delcroix Cet al. Diuretic and enhanced
sodiumrestriction results in improved antiproteinuric response to
RASblocking agents. J Am Soc Nephrol2005; 16: 474481.
28. Esnault VL, Ekhlas A, Nguyen JMet al. Diuretic uptitration
with half dosecombined ACEI+ARB better decreases proteinuria than
combinedACEI+ARB uptitration. Nephrol Dial Transplant2010; 25:
22182224.
29. Sepehrdad R, Chander PN, Oruene Aet al. Amiloride reduces
stroke andrenal injury in stroke-prone hypertensive rats. Am J
Hypertens 2003; 16:312318.
30. Zhang B, Xie S, Shi Wet al. Amiloride off-target effect
inhibits podocyteurokinase receptor expression and reduces
proteinuria. Nephrol DialTransplant2012; 27: 17461755.
31. Nagase M, Yoshida S, Shibata Set al.Enhanced aldosterone
signaling in theearly nephropathy of rats with metabolic syndrome:
possible contributionof fat-derived factors. J Am Soc Nephrol2006;
17: 34383446.
32. Nagase M, Fujita T. Aldosterone and glomerular podocyte
injury.Clin ExpNephrol2008; 12: 233242.
33. Rocha R, Chander PN, Khanna Ket al.Mineralocorticoid
blockade reducesvascular injury in stroke-prone hypertensive rats.
Hypertension 1998; 31:451458.
34. Heeg JE, de Jong PE, van der Hem GKet al. Efficacy and
variability of theantiproteinuric effect of ACE inhibition by
lisinopril. Kidney Int1989; 36:272279.
35. Holtkamp FA, de Zeeuw D, de Graeff PAet al. Albuminuria and
bloodpressure, independent targets for cardioprotective therapy in
patientswith diabetes and nephropathy: a post hoc analysis of the
combined
RENAAL and IDNT trials. Eur Heart J. 2011; 32: 1493
1499.36. Morales E, Valero MA, Len Met al. Beneficial effects of
weight loss in
overweight patients with chronic proteinuric nephropathies. Am J
KidneyDis 2003; 41: 319327.
37. Holtkamp FA, de Zeeuw D, Thomas MCet al. An acute fall in
estimatedglomerular filtration rate during treatment with losartan
predicts a slowerdecrease in long-term renal function. Kidney
Int2011; 80: 282287.
38. Juurlink DN, Mamdani MM, Lee DS et al. Rates of hyperkalemia
afterpublication of the Randomized Aldactone Evaluation Study. N
Engl J Med2004; 351: 543551.
Kidney International (2015) 88 , 14341441 1441
E Moraleset al.: Antialbuminuric effect of diuretics c l i n i c
a l t r i a l