-
7/25/2019 Distal Radioulnar Joint Instability
1/12
Selected
The American Academy of Orthopaedic SurgeonsPrinted with
permission of the
American Academy of Orthopaedic Surgeons. This article,
as well as other lectures presented
at the Academys Annual Meeting,will be available in February
2007 inInstructional Course Lectures,
Volume 56. The completevolume can be ordered online
at www.aaos.org, or by calling 800-626-6726
(8 A. M .-5 P . M ., Central time).
J. LAWRENCE M ARSHEDITOR , VOL. 56
COMMITTEE
J. LAWRENCE M ARSHCHAIRMAN
FREDERICK M. AZA R PAU L J. DUWELIUSTERRY R. LIGHT
EX-O FFICIOD EMPSEY S . SPRINGFIELDDEPUTY EDITOR OF THE JOURNAL
OF BONE AND JOINT SURGERYFOR INSTRUCTIONAL COURSE LECTURES
JAMES D. H ECKMANEDITOR -IN -CHIEF,THE JOURNAL OF BONE AND JOINT
SURGERY
-
7/25/2019 Distal Radioulnar Joint Instability
2/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
Distal RadioulnarJoint Instability
BY R OBERT M. SZABO, MD, MPH
An Instructional Course Lecture, American Academy of Orthopaedic
Surgeons
The distal radioulnar joint is inherentlyunstable. Pathologic
instability can beacute or chronic; it can be dorsal, pal-mar, or
multidirectional; and it can re-sult primarily from soft-tissue
injuryor osseous malunion. Recognition ofthe type and cause of
instability is fun-damental in order to provide
effectivetreatment.
Anatomy of theDistal Radioulnar Joint
The distal radioulnar joint is a distal ar-ticulation in the
biarticulate rotationalarrangement of the forearm. This
articu-lation allows only one degree of motion:pronation and
supination. The sigmoidnotch of the radius is concave and isshallow
with a radius of curvature of15 mm. The ulnar head is
semicylin-drical and has an articulate convexityof 220 with a
radius of curvature of10 mm 1. The ulnar head is surroundedby an
ulnar carpal ligament complex.This consists of the ulnolunate and
ul-
notriquetral ligaments, which originatefrom the palmar
radioulnar ligamentnear the ulnar styloid process. Whenseen through
an arthroscope, these liga-ments appear to be continuous with
thetriangular fibrocartilage.
The triangular fibrocartilage is afibrocartilaginous disk
originating atthe junction of the lunate fossa and thesigmoid notch
and inserting at the baseof the ulnar styloid. Its central
portionis cartilaginous, and it is designed for
weight-bearing. It is also avascular. Theperipheral margins are
composed ofthick lamellar cartilage designed fortensile loading and
are called the dorsaland palmar radioulnar ligaments .
Theperipheral margins of the triangular fi-brocartilage are well
vascularized fromthe palmar and dorsal branches of theanterior
interosseous artery and fromthe ulnar artery. The ulnar styloid is
thecontinuation of the subcutaneous ridgeof the ulnar shaft, and it
stands as astrut on the end of the ulna to stabilizethe ulnar soft
tissues of the wrist. Thesheath of the extensor carpi ulnaris,
theulnocarpal ligaments, and the triangu-lar fibrocartilage help to
maintain thecongruency of the distal radioulnar joint with
attachments at the base of theulnar styloid; together, they are
knownas the triangular fibrocartilage complex 2-6 .
The radius of curvature of the ulnadoes not equal that of the
sigmoid notch.Full congruity of two articulating sur-faces is
therefore not possible. The shal-
low sigmoid cavity and the differencebetween the radii of
curvature of thesigmoid notch and the ulnar head causethe ulna to
translate volarly in supina-tion and dorsally in pronation. In
theextremes of forearm rotation,
-
7/25/2019 Distal Radioulnar Joint Instability
3/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
tations of forearm rotation was de-scribed by Kleinman and
Graham 17.
The triangular fibrocartilage, theulnar carpal ligaments, the
infratendi-
nous extensor retinaculum, the prona-tor quadratus, and the
interosseousmembrane provide additional key soft-tissue
constraints. The triangular fibro-cartilage attaches to the fovea
in theulna by way of the dorsal and palmarradioulnar ligaments. The
fibers thatinsert into the fovea are separated fromthose that
insert into the styloid by anareolar vascular tissue known as
theligamentum subcruentum 18. There is adebate in the literature
regarding theradioulnar ligaments. According toSchuind et al., in
pronation the dorsalradioulnar ligament tightens as the
ulnatranslates dorsally and in supination thepalmar radioulnar
ligament tightens asthe ulna translates palmarly 19 (Table I).In
contrast, Ekenstam showed that inpronation the palmar radioulnar
liga-ment becomes taut (although thedorsal capsule tightens) as the
ulnatranslates dorsally, and in supinationthe dorsal radioulnar
ligament tightens(although the palmar capsule becomestight) as the
ulna translates volarly 20.Ekenstam believed that stability
inpronation depends on the tension inthe volar radioulnar ligament
and com-pression between the contact areas ofthe dorsal aspect of
the sigmoid notchand the ulna, whereas stability in supi-nation
depends on the tension in thedorsal radioulnar ligament and the
tri-angular fibrocartilage articular disk aswell as compression
between the con-tact areas of the volar aspect of the sig-moid
notch and the ulna.
Adams and Holley measured strainon the surface of the triangular
fibrocar-
tilage articular disk and calculated the
strain at the dorsal and palmar marginsof the disk 21. In
supination, strain in-creased dorsally; in pronation,
strainincreased palmarly. In a biomechanical
study of eleven fresh cadavers, Ward etal. measured tension in
the dorsal andpalmar radioulnar ligaments, joint rota-tion, and
radial translation after sequen-tial excision of the disk,
interosseousmembrane, joint capsule, and radioulnarligaments 14.
This experiment confirmedthat the dorsal ligament tightens
duringpronation while the palmar ligament be-comes progressively
lax, whereas theconverse occurs during supination.
The preponderance of biome-chanical evidence supports the
findingsreported by Schuind et al. 19, and the in-consistency
between their observationsand those presented by Ekenstam 20 canbe
resolved because, in pronation, thedorsal radioulnar ligament
tightens andtends to displace the ulna dorsally. Leftunconstrained,
this dynamic tensioningwould lead to subluxation and disloca-tion
of the joint. The palmar radioulnarligament checks that force and
keeps the joint reduced. If the interosseous mem-brane is disrupted
and the palmar radi-oulnar ligament is sectioned, the distalpart of
the ulna dislocates dorsally in pro-nation. If the interosseous
membrane isdisrupted and the dorsal radioulnar liga-ment is
sectioned, the distal part of theulna dislocates palmarly in
supination.
ClassificationDisorders of the distal radioulnar jointcan be
classified into four categories: (1)impaction, (2) incongruity, (3)
inflam-mation, and (4) instability. All of thesedisorders can
produce pain around thedistal radioulnar joint and should
beconsidered when a patient reports symp-
toms at the distal radioulnar joint. Ulnar
impaction is due to a positive ulnarvariance that causes the
distal part ofthe ulna to abut against the lunate, oftenleading to
thinning of the triangular fi-
brocartilage and eventually to a centraltear. Some surgeons also
refer to this asulnar abutment syndrome. Incongruityrefers to the
lack of a smooth interfacebetween the ulnar head and the
sigmoidnotch. Incongruity can be due to a post-traumatic condition
such as a distal ra-dial fracture into the sigmoid notch,or it can
be secondary to osteoarthritisor rheumatoid arthritis.
Inflammationaround the distal radioulnar joint isusually due to
extensor carpi ulnaristendinitis dorsally or flexor carpi ul-naris
tendinitis palmarly, and some-times these disorders can be of
acalcific variety.
Instability of the distal radioul-nar joint may be acute or
chronic andmay be related to osseous changes aftera fracture or to
soft-tissue injury. Soft-tissue injury of the triangular
fibrocarti-lage, dorsal radioulnar ligament, palmarradioulnar
ligament, interosseous mem-brane, joint capsule, or any
combina-tion of those structures is capable ofproducing instability
of the distal radi-oulnar joint. Fractures of the distal partof the
radius or distal part of the ulnaalter the biomechanics of the
distal ra-dioulnar joint 22. It is important to keepin mind that
instability can occur aloneor in conjunction with impaction,
in-congruity, or inflammation. Treatmentmust be directed at each
component ofthe disease complex.
Examination of theDistal Radioulnar JointTo examine the ulnar
styloid, oneshould follow the superficial border of
the ulnar shaft distally while the wrist is
TABLE I Effects of Pronation and Supination on the Dorsal and
Palmar Radioulnar Ligaments and Joint Capsule
Pronation Supination
Dorsal radioulnar ligament Tight as ulna displaces dorsally.
Dorsal capsuleimbrication stabilizes distal radioulnar joint,
pre-venting volar translation of radius
Lax
Palmar radioulnar ligament Lax Tight as ulna displaces palmarly.
Palmar capsuleimbrication stabilizes distal radioulnar
joint,preventing dorsal translation of radius
-
7/25/2019 Distal Radioulnar Joint Instability
4/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
in radial deviation. The ulnar styloidcan be found more volarly
than antici-pated. This maneuver should be donewith the wrist in a
pronated position.The distal radioulnar joint is the mostcomplex
structure to evaluate. Themost common pathological finding
isradioulnar incongruity secondary to amalunited distal radial
fracture withloss of the pronation-supination arc.With loss of the
volar tilt of the radius,the distal part of the ulna appears to
bemore prominent. With ulnar impac-tion, ulnar deviation and
extension arelimited and can be painful. The areasof pronation,
supination, and flexion-extension should be determined. To testfor
instability of the distal radioulnar
joint, the examiner should supinate thewrist while supporting
the hand, per-form a ballottement maneuver of thedistal part of the
ulna, and compare theaffected side with the normal side. Dur-ing
this maneuver, he or she should feelfor crepitus and ask the
patient if painoccurs. To check for instability of theextensor
carpi ulnaris tendon, the pa-tient should be asked to flex the
elbowand pronate and supinate the forearmwith the hand in slight
ulnar deviation
while the examiner looks for abnormalmotion of the extensor
carpi ulnaristendon. Peripheral tears of the triangu-lar
fibrocartilage complex can produceinstability of the distal
radioulnar jointwith the wrist in supination. With thepatients
forearm in supination, the ex-aminer should hold the distal part
ofthe ulna between the thumb and indexfinger and test for dorsal
and volar dis-placement of the distal part of the ulna.The
so-called press-test is a simple as-sessment. The patient is asked
to pushhimself or herself up from a seated posi-tion with use of
the affected wrist. Thistest creates an axial ulnar load and has
ahigh sensitivity for detecting a tear ofthe triangular
fibrocartilage complex 23.
Pain with this maneuver suggests thatthere is a lesion in the
triangular fibro-cartilage complex.
Radiographic TestsStandard radiographs of the distal partof the
ulna should be made with com-parison views of the unaffected side.
Theimages should include a true lateral ra-diograph made with the
forearm in neu-tral rotation. Any deviation of >10 froma true
lateral view will greatly reduce the
accuracy of the examination. Ulnar vari-ance should be measured
and comparedwith that on the contralateral side on ra-diographs
made with the forearm in neu-
tral rotation and the shoulder and elbowin 90 of flexion with
the x-ray beamdirected from posterior to anterior 24.Ulnar variance
changes by up to a milli-meter as the forearm moves from full
su-pination to full pronation; therefore, thisstandard position
should be used. Ulnarvariance is measured by drawing a trans-verse
line at the level of the lunate fossaand a second transverse line
at the levelof the ulnar head, and determining thedistance between
the two lines. On theposteroanterior radiograph, one shouldlook for
a fleck fracture demonstratingan avulsion of the triangular
fibrocarti-lage complex, an ulnar styloid nonunion,and joint
widening between the radiusand ulna (Fig. 1). Radiographic signs
ofinjury to the distal radioulnar joint in-clude a fracture at the
base of the ulnarstyloid, widening of the distal radioul-nar joint
space seen on the posteroante-rior radiograph, >20 of dorsal
radialangulation, and >5 mm of proximal dis-placement of the
distal part of the radius.
Computed tomography scanningis the technique of choice for
evaluat-ing congruity of the distal radioulnar joint, but the same
information can beobtained with magnetic resonance im-aging (Figs.
2-A and 2-B). There areseveral methods for evaluating sublux-ation
of the distal radioulnar joint, in-cluding the method described by
Minoet al.25,26, the congruency method 27, theepicenter method 27,
and the RUR (radi-oulnar ratio) method 28. Magnetic reso-nance
imaging is useful for identifyingtears of the triangular
fibrocartilage(Fig. 3), but its specificity and sensitiv-
ity vary 29
. It is necessary to use high-resolution magnetic resonance
imagingwith a dedicated wrist coil to obtain ac-curate scans 30-32.
Arthrography is still avaluable examination, and it is evenmore
useful when it is combined withmagnetic resonance imaging.
Arthros-copy is a sensitive method for evaluat-ing tears of the
triangular fibrocartilagecomplex and is considered the goldstandard
with which to compare theaccuracy of other examinations.
Fig. 1Posteroanterior radiograph showing a distal radioulnar
joint with chronic palmar instability in a fif-teen-year-old girl
who had sustained a fracture of the distal part of the radius two
years previ-ously. Note the large ulnar styloid nonunion fragment
and a fleck fracture representing the sitewhere the triangular
fibrocartilage complex avulsed from the fovea.
-
7/25/2019 Distal Radioulnar Joint Instability
5/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
Subluxation and DislocationBy convention, the ulna is
consideredto dislocate with respect to the radius,but it is the
radius that moves andtherefore is displaced. With dorsal
sub-luxation, the head of the ulna becomesprominent dorsally,
particularly in pro-nation, and may snap during wrist rota-tion.
This is usually associated with aweak and painful wrist. With
completedislocation, the ulnar head is locked inposition, most
commonly dorsally buton occasion palmarly. Supination is
re-stricted with either type of dislocationbecause the radius
cannot slip dorsallyover the ulnar head.
The mechanism of action for adorsal subluxation or dislocation
of theulna is extreme pronation and exten-sion with the coiled and
tightened ex-tensor carpi ulnaris and ulnar carpalligaments acting
as a sling to lift theulnar head through the dorsal capsule.
Weakening of the triangular fibrocarti-lage complex secondary to
its avulsion(or a fracture of the ulnar styloid) andattenuation of
the palmar radioulnarligament will allow the dislocation.Sheer
stress during this mechanismmay produce associated chondral
de-fects. The clinical appearance of a dor-sal dislocation of the
ulna is a tenderprominent dorsally displaced ulna anda forearm with
limited supination orlocked in pronation. Direct pressure
may reduce the dislocation, but the ul-nar head usually springs
back into adorsal position if the forearm remainspronated. There is
increased anteropos-terior translation of the distal radioul-nar
joint with passive motion. Routine
radiographs may be nondiagnostic. Aposteroanterior radiograph
can showthe ulna overlapping the distal part ofthe radius. The best
study with which tovisualize a subluxation or dislocation isa
computed tomography examination
Fig. 2-AT1-weighted magnetic resonance images of both wrists in
pronation made to compare the normal wrist (Fig. 2-A) with the
wrist that had a dorsal dis-tal ulnar subluxation (Fig. 2-B).
Fig. 2-B
Fig. 3T2-weighted magnetic resonance image showing a complex
peripheral tear (double arrows) andradial tear (single arrow) of
the triangular fibrocartilage complex.
-
7/25/2019 Distal Radioulnar Joint Instability
6/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
of both wrists performed in both pro-nation and supination
25,26,33-35.
Treatment of Acute DislocationsDorsal Subluxation and
DislocationAn acute dorsal dislocation can be re-duced with digital
pressure on the distalpart of the ulna and forceful supination.The
reduction should be maintainedfor six weeks. Some authors 36 have
ad-vocated full supination, whereas others 37 have recommended the
neutral posi-tion. Nonoperative methods of treat-ment should be
used only when thereis congruity of the distal radioulnar joint in
two planes. Open reduction
with repair of the triangular fibrocarti-lage complex should be
performed ifthe joint is locked and cannot be re-duced, or if it is
incongruous followingreduction. Open repair of the
triangularfibrocartilage complex is done with adorsal incision
through the fifth com-partment with the extensor digiti min-imi
reflected radially and the extensorcarpi ulnaris reflected ulnarly,
therebyexposing the triangular fibrocartilagecomplex and
visualizing the dorsal radi-
oulnar ligament. Nonabsorbable su-tures should be used to
reattach thetriangular fibrocartilage complex tothe ulnar styloid
38.
Ulnar styloid fractures have animportant effect on the stability
of thetriangular fibrocartilage complex. Thesefractures commonly
occur together withfractures of the distal part of the radiusand
can be a sign of instability of the tri-angular fibrocartilage
complex. Symp-tomatic nonunions of the styloid canoccur. Hauck et
al. classified these non-unions as type 1 when the distal
radio-ulnar joint is stable and as type 2 whenit is unstable 2.
Type-1 fractures occur
through the tip of the styloid, and whenthey become symptomatic
they are of-ten treated successfully with excision.Type-2 fractures
occur through the baseof the styloid, creating a much
largerfragment, and usually open reductionand internal fixation and
restoration ofthe integrity of the triangular fibrocarti-lage
complex is recommended even ifthere is a nonunion.
The distal part of the ulna can dis-locate or subluxate palmarly
as a result of
a fall on a supinated hand or from exer-tional lifting in
supination, with failureof the dorsal radioulnar ligament beingthe
critical event. Clinically, patientspresent with the forearm held
in a supi-nated position. Pronation is painful andrestricted 39.
The ulnar head is palpablevolarly, and ulnar dysesthesias may
de-velop from pressure on the ulnar nerve.Once again, a diagnosis
can be made onthe basis of good standard radiographs(Figs. 4-A and
4-B) and can be con-firmed by comparing computed tomog-raphy scans
of the affected and normalwrists. A fracture or erosion of the
pal-mar lip of the sigmoid notch may lead
to persistent instability. An acute pal-mar dislocation can be
reduced withdigital pressure on the distal part of theulna in a
dorsal direction combined withforceful pronation. The treatment
foran acute palmar dislocation is closedreduction with
immobilization for sixweeks in an above-the-elbow cast in aneutral
or slightly pronated position.Open treatment is reserved for
patientsfor whom closed reduction has failed.The approach is volar
with careful re-
Fig. 4-A
Standard posteroanterior (Fig. 4-A) and lateral (Fig. 4-B)
radiographs of the wrist, dem-onstrating palmar dislocation of the
ulna.
Fig. 4-B
-
7/25/2019 Distal Radioulnar Joint Instability
7/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
traction of the volar neurovascular bun-dle in an ulnar
direction.
Tears of the Triangular
Fibrocartilage ComplexTriangular fibrocartilage tears can
occurwithout causing instability of the distalradioulnar joint. The
most commontear occurs within the articular diskof the triangular
fibrocartilage, near itsattachment to the radius, and is not
as-sociated with instability of the distalradioulnar joint 40-44.
The tears them-selves, however, can be unstable andsymptomatic.
Despite the recognitionof specific types of triangular
fibrocar-tilage lesions45, the exact mechanismsof injury remain
uncertain. Adams etal., using a laboratory model to simu-late
distraction of the radius and ulnathrough the distal radioulnar
joint, pos-tulated that such a distraction force mayresult from a
violent axial load on theforearm 40. This model did not, how-ever,
produce the types of tears of thetriangular fibrocartilage complex
thatare seen clinically. Probably, a combi-nation of compression
across the wristtrapping the disk in the ulnocarpal jointwith
distraction or twisting of the distal
radioulnar joint then creates enoughshear forces to tear the
disk.
Symptomatic instability and tearsof the triangular
fibrocartilage complex
require surgical treatment. The periph-eral rim of the
triangular fibrocartilageis well vascularized and has good heal-ing
potential. Repair of these lesionswith a variety of techniques can
lead tohealing. Historically, open repair wasadvocated 38, but
currently most peri-pheral tears can be treated arthros-copically.
This arthroscopic approachrepairs only the superficial fibers ofthe
triangular fibrocartilage complexto the joint capsule and not the
deepportion that inserts onto the fovea.There is much less chance
that centraltears of the triangular fibrocartilagecomplex will heal
because they are inareas of hypovascularity or avascular-ity.
Arthroscopic dbridement of theselesions is recommended 46.
Chronic Distal RadioulnarJoint InstabilityDorsal, Palmar,
orBidirectional Instability Chronic distal radioulnar joint
instabil-ity is a painful and often disabling con-
dition. Functional bracing, which hasbeen tested in a cadaveric
model 47, canbe used for patients who do not wish tohave surgery,
but most patients prefer
surgical treatment. It is necessary tocheck the osseous anatomy
in patientswith chronic palmar dislocation. Manypatients have had a
fracture of the wristor forearm, sometimes many years be-fore
symptoms developed at the distalradioulnar joint. Bilateral
radiographsof the entire wrist and forearm, madein the same
position, should be com-pared. Osseous malalignment shouldbe
corrected. The status of the triangu-lar fibrocartilage complex is
evaluatedwith either magnetic resonance imagingor arthroscopy. If
the triangular fibro-cartilage complex is not repairable, atendon
reconstruction is needed andshould be tightened in supination
48,49.
Illustrative Case ReportAn eighteen-year-old,
right-hand-dominant man presented with painin the left wrist and
forearm that hadbeen increasing during the previoustwo years. He
had sustained a fractureof the distal third of the left radius
atthe age of twelve years and had been
Fig. 5-APosteroanterior (Fig. 5-A) and lateral (Fig. 5-B)
radiographs made three years after plate fixation of a fracture of
the distal part of the left radius in atwelve-year-old boy. Note
the apex volar angulation of the radius. The normal right side is
shown for comparison.
Fig. 5-B
-
7/25/2019 Distal Radioulnar Joint Instability
8/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
treated nonoperatively. One monthlater, he fell and sustained a
refractureof the radius as well as an ulnar styloidfracture. The
fracture of the radius wastreated with open reduction and inter-nal
fixation through a volar approach.It healed without complication,
and thepatient returned to full participation involleyball,
weight-lifting, soccer, andsnowboarding.
Three years later, he noticed swell-ing about the wrist and had
pain at thedistal part of the left ulna in association
with many activities. Volar angulationof the radius could be
seen on radio-graphs (Figs. 5-A and 5-B). The trian-gular
fibrocartilage complex appearednormal on the magnetic resonance
im-aging scan. The symptoms were attrib-uted to malunion of the
fracture andangular overgrowth of the radius result-ing in palmar
subluxation of the distalpart of the ulna and instability of the
dis-tal radioulnar joint. The hardware wasremoved, and a dome
osteotomy of the
left radius with iliac crest bone-graftingwas done. A
closing-wedge osteotomyof the radius was not performed becauseof
the potential that it could further de-stabilize the distal
radioulnar joint 50.Eight months after the surgery, the os-teotomy
site had healed and the patienthad regained the preoperative range
ofwrist motion. The distal radioulnar jointwas stable on
examination. He resumedall of his previous activities,
includingvolleyball and weight-lifting, withoutany symptoms in the
left upper extre-
mity, and he was discharged from ourclinic. He subsequently
joined the Ma-rine Corps and wrote to say that he hadremained
asymptomatic throughout allphysical endeavors involved in his
stren-uous active training 51.
Dorsal Subluxation andDislocations with FracturesGaleazzi
FracturesA Galeazzi fracture is a diaphyseal frac-ture of the
radius associated with a dis-
location of the radioulnar joint 52. AGaleazzi fracture has also
been calledthe fracture of necessity because non-operative
treatment so often yields apoor result. The radioulnar joint maybe
dislocated or subluxated, and it isalways affected (Figs. 6-A
through 6-D).Detection of the disorder of the distalradioulnar
joint in a patient with a ra-dial shaft fracture requires a high
levelof suspicion. Radiographs of the con-tralateral side may be
helpful. Rettigand Raskin found that twelve of twenty-
two fractures of the distal third of theradius (within 7.5 cm of
the midarticu-lar surface of the distal part of the radius)were
associated with intraoperative in-stability of the distal
radioulnar joint,whereas only one of eighteen fracturesin the
middle third of the radial shaft(>7.5 cm from the midarticular
surfaceof the distal part of the radius) was as-sociated with
intraoperative instabilityof the distal radioulnar joint 53.
Openreduction with internal fixation of the
Fig. 6-BFigs. 6-A through 6-D A twenty-eight-year-old man was
seen with a Galeazzi-type fracturewith an entrapped extensor carpi
ulnaris tendon preventing reduction of the ulnar styloidthat is
attached to the triangular fibrocartilage complex. Note the
disrupted distal radioul-nar joint in addition to the fractures of
the radius and distal part of the ulna. Fig. 6-A Pos-teroanterior
radiograph showing the injury. Fig. 6-B Lateral radiograph showing
the injury.
Fig. 6-A
-
7/25/2019 Distal Radioulnar Joint Instability
9/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
radial fracture is the first stage of treat-ment of a Galeazzi
fracture. If the distalradioulnar joint is stable, early motioncan
be initiated. If it is unstable and re-ducible, the wrist should be
immobi-
lized in slight supination for four to sixweeks. If a sizable
ulnar styloid fractureis present, fixation may allow early
mo-bilization and should be considered. Ifthe distal radioulnar
joint is irreducible,open reduction of the joint is necessary;this
usually requires repair of the trian-gular fibrocartilage or
fixation of theulnar styloid fragment. Six weeks of im-mobilization
in slight supination is rec-ommended if the distal radioulnar
jointrequires surgical treatment. Rarely, the
extensor carpi ulnaris is interposedand prevents reduction; if
it is, it needsto be removed from the joint (Figs. 6-Cand 6-D)
54.
Essex-Lopresti InjuriesEssex-Lopresti injuries, which are
se-vere and disrupt the entire forearm 55,consist of a radial head
fracture withproximal migration of the radius. Themigration
indicates complete disrup-tion of the interosseous ligament andthe
triangular fibrocartilage complex.These injuries are usually caused
by afall on the outstretched hand with axialloading. The primary
stabilizer prevent-ing proximal migration of the radius is
the radial head, and the secondary sta-bilizers are the
interosseous ligamentand the triangular fibrocartilage. Diag-nosing
the wrist injury in this complex
is important. Treatment consists ofopen reduction and internal
fixation ofthe radial head if possible, with immo-bilization of the
forearm in supination.Pinning of the distal radioulnar joint isan
option, but if the pins break they canbe difficult to retrieve.
Comminuted ra-dial head fractures often are not repair-able and
require replacement, usuallywith a metallic prosthesis. Silicone
ra-dial head replacements have not per-formed well in this
situation becausethey fracture, causing particulate syno-vitis,
when they are placed under load.The operation is best done early as
de-layed treatment can lead to poorer re-sults. The options for
delayed surgeryinclude radial head replacement witha prosthesis or
allograft 56, or a Sauv-Kapandji procedure.
Multidirectional InstabilityThe axis of forearm motion
passesthrough the fovea of the distal part ofthe ulna. The deep
fibers of the distalradioulnar ligaments, the palmar radi-oulnar
ligament, the triangular fibro-cartilage, the ulnolunate ligament,
theulnotriquetral ligament, and the ulno-capitate ligament all
insert onto the fo-vea57. These ligamentous attachmentsare key to
the stability of the distal ra-dioulnar joint. The distal
radioulnar joint can be stabilized surgically in oneof three ways:
(1) a repair of the trian-gular fibrocartilage complex and
thedistal radioulnar ligaments, (2) anextrinsic soft-tissue
reconstruction ei-ther with a direct link (i.e., a
radioulnartether) or an indirect link (i.e., an ulnar
carpal sling tenodesis), or (3) a distalradioulnar ligament
reconstruction.
Procedures for Stabilizationof the Distal Radioulnar JointThe
first option for stabilizing the dis-tal radioulnar joint is to
repair the tri-angular fibrocartilage complex to thefovea, from
which it is usually found tobe ruptured. When repair is not
possi-ble, reconstruction is indicated. Thereare several procedures
for stabilization
Fig. 6-C
Fig. 6-C Posteroanterior radiograph made after initial fixation
of the radial and ulnarfractures. Note the widening of the distal
radioulnar joint. Fig. 6-D Lateral radiograph
made after initial fixation of the radial and ulnar fractures.
Note the dorsal displace-ment of the ulna. This problem occurred
because the initial surgeon did not recognizethe interposition of
the extensor carpi ulnaris tendon, which prevented the reductionof
the ulnar styloid/triangular fibrocartilage complex. Reoperation
was performed,and anatomical reduction and fixation was possible
after the extensor carpi ulnaristendon was repositioned
dorsally.
Fig. 6-D
-
7/25/2019 Distal Radioulnar Joint Instability
10/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
of the distal radioulnar joint, as describedby Hui and Linscheid
58, Tsai and Stil-well59, Breen and Jupiter 60, Fulkersonand Watson
61, and Ellison, Boyes, and
Bunnell1
, just to mention a few. Theabove are all indirect stabilization
pro-cedures through an ulnocarpal sling ortenodesis, or a direct
radioulnar tetherextrinsic to the joint (the techniquedescribed by
Fulkerson and Watson).Johnson described a dynamic muscletransfer
involving use of the pronatorquadratus 11. Other distal radioulnar
sta-bilization procedures involving recon-struction of the
radioulnar ligamentswere described by Scheker et al. 62, Sand-ers
and Hawkins 63, and Bowers 64. We arenot aware of any long-term
follow-upstudy of an adequate series of patientstreated with such
procedures. In a bio-mechanical cadaver model, reconstruc-tions of
the radioulnar ligaments werefound to be superior to radioulnar
teth-ering procedures although the resultsof capsular repair alone
most closelymatched the kinematics of an intactdistal radioulnar
joint 65.
I recommend the procedure de-scribed by Adams et al. to
reconstructthe ligamentous anatomy (Fig. 7) 48,49.Their indications
and criteria for ligamentreconstruction include unidirectional
orbidirectional chronic instability of thedistal radioulnar joint,
absence of sub-stantial arthritis, and a competent sig-moid notch
rim with no residual axialinstability of the forearm. Any
malunionshould be mild or corrected concur-rently. Adams and
Divelbiss cautionedthat, if the volar or dorsal lip of the sig-moid
notch is incompetent (shallow),ligament reconstruction may not
besufficient and an opening-wedge os-teotomy of the distal part of
the radius
may be required48
. The procedure isdone with use of a dorsal approachthrough the
fifth extensor compart-ment, which provides direct access tothe
distal radioulnar joint. Typical find-ings are a triangular
fibrocartilage com-plex that is torn from the ulna, a tornextensor
carpi ulnaris sheath, concomi-tant carpal ligament injuries, and
per-haps an ulnar styloid fracture. Adamsand Berger reported that,
of twenty pa-tients (twelve with bidirectional insta-
Fig. 8This patient underwent open reduction and in-
ternal fixation to treat a fracture of the distalpart of the
radius, but the dorsal subluxationof the ulna was never corrected.
Arthriticchanges developed in the distal radioulnar
joint, with pain and limitation of pronation-supination. This
problem was treated with aSauv-Kapandji procedure.
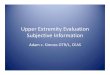
Fig. 7Dorsal and palmar ligament reconstruction, as described by
Adams and Divelbiss 48, for treat-ment of a chronically unstable
distal radioulnar joint. (Reprinted from: Adams BD, Divelbiss
BJ.Reconstruction of the posttraumatic unstable distal radioulnar
joint. Orthop Clin North Am.2001;32:353-63; with permission from
Elsevier.)
-
7/25/2019 Distal Radioulnar Joint Instability
11/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
bility and eight with unidirectionalinstability) followed for a
minimumof one year after the procedure, eigh-teen recovered
stability, with an 80%
recovery of supination, 84% recoveryof pronation, and 88%
recovery of gripstrength 49.
SalvageIf there is residual instability after adistal ulnar
resection, a flexor carpi ul-naris and extensor carpi ulnaris
tenode-sis, as described by Breen and Jupiter 60,66,can be
considered. Wolfe et al. reportedthat the distal part of the ulna
will re-main stable even after removal of morethan a third of it
67. This may be true af-ter a tumor resection, but it is not
areliable assumption after traumaticinjuries. Wide resections of
the distalpart of the ulna usually require someadditional form of
stabilization, andtenodesis of the flexor carpi ulnaris andextensor
carpi ulnaris tendons is rec-ommended. Implantation of a
metallicprosthesis to replace the distal part ofthe ulna can also
be considered as a sal-vage procedure for treatment of this
dif-ficult problem 68. The Sauv-Kapandjiprocedure is a useful
salvage techniquewhen there is instability of the distalpart of the
ulna and arthritic changes
(Fig. 8). The Sauv-Kapandji procedureinvolves fusion of the
distal radioulnar joint and creation of a pseudarthrosis ofthe ulna
just proximal to the arthrodesis
to allow forearm rotation69
. There canbe subluxation of the proximal ulnarstump, which can
be symptomatic, aftera Sauv-Kapandji procedure, and thiscan be
stabilized with either an extensorcarpi ulnaris tenodesis, as
described byMinami et al. 70, or a flexor carpi ulnaristenodesis,
as described by Lamey andFernandez 71.
OverviewAcute dislocations of the distal radioul-nar joint
should be reduced promptlyand treated with cast immobilization.If
the dislocation is irreducible, openreduction is warranted. The
first at-tempts to treat chronic instabilityshould be directed at
repairing the tri-angular fibrocartilage complex, butonly after
careful assessment for anyosseous malunions along the forearmaxis,
which must also be corrected. If itis not possible to repair the
triangularfibrocartilage complex, the osseous ar-chitecture is
normal, and no arthritis ispresent, a ligament reconstruction canbe
considered, but the competency ofthe sigmoid notch must be
evaluated
carefully. If there are arthritic changesat the distal
radioulnar joint, a Sauv-Kapandji procedure should be
performed,with stabilization of the proximal stump
with a slip of either the flexor carpi ul-naris or the extensor
carpi ulnaris.
Robert M. Szabo, MD, MPHDepartment of Orthopaedic Surgery,
Univer-sity of California, Davis, School of Medicine,4860 Y Street,
Sacramento, CA 95817. E-mailaddress: [email protected]
The author did not receive grants or outsidefunding in support
of his research for or prep-aration of this manuscript. He did not
receivepayments or other benefits or a commitmentor agreement to
provide such benefits from acommercial entity. No commercial entity
paidor directed, or agreed to pay or direct, any ben-efits to any
research fund, foundation, educa-tional institution, or other
charitable ornonprofit organization with which the authoris
affiliated or associated.
Printed with permission of the AmericanAcademy of Orthopaedic
Surgeons. This arti-cle, as well as other lectures presented at
theAcademys Annual Meeting, will be available inFebruary 2007 in
Instructional Course Lectures, Volume 56. The complete volume can
be or-dered online at www.aaos.org, or by calling800-626-6726 (8
A.M.-5 P.M., Central time).
References
1. Bowers WH. The distal radioulnar joint. In: GreenDP, editor.
Operative hand surgery. Volume 1. 3rd ed.New York: Churchill
Livingstone; 1993. p 973-1019.2. Hauck RM, Skahen J 3rd, Palmer AK.
Classifica-tion and treatment of ulnar styloid nonunion. J HandSurg
[Am]. 1996;21:418-22.3. Heiple KG, Freehafer AA, Vant Hof A.
Isolatedtraumatic dislocation of the distal end of the ulna
ordistal radio-ulnar joint. J Bone Joint Surg Am.1962;44:1387-94.4.
Linscheid RL. Biomechanics of the distal radioul-nar joint. Clin
Orthop Relat Res. 1992;275:46-55.
5. Palmer AK, Werner FW. The triangular fibrocarti-lage complex
of the wristanatomy and function.J Hand Surg [Am]. 1981;6:153-62.6.
Palmer AK, Linscheid RL, Fisk GR, Taleisnik J.Symposium: distal
ulnar injuries. Contemp Orthop.1983;7:81-118.7. Pirela-Cruz MA,
Goll SR, Klug M, Windler D.Stress computed tomography analysis of
the dis-tal radioulnar joint: a diagnostic tool for determin-ing
translational motion. J Hand Surg [Am]. 1991;16:75-82.8. Gofton WT,
Gordon KD, Dunning CE, Johnson JA,King GJ. Soft-tissue stabilizers
of the distal radioul-nar joint: an in vitro kinematic study. J
Hand Surg[Am]. 2004;29:423-31.
9. Kihara H, Short WH, Werner FW, Fortino MD,Palmer AK. The
stabilizing mechanism of the dis-tal radioulnar joint during
pronation and supina-tion. J Hand Surg [Am]. 1995;20:930-6.10.
Stuart PR. Pronator quadratus revisited. J HandSurg [Br].
1996;21:714-22.11. Johnson RK. Stabilization of the distal ulna
bytransfer of the pronator quadratus origin. Clin Or-thop Relat
Res. 1992;275:130-2.12. Johnson RK, Shrewsbury MM. The
pronatorquadratus in motions and in stabilization of the ra-dius
and ulna at the distal radioulnar joint. J HandSurg [Am].
1976;1:205-9.13. Spinner M, Kaplan EB. Extensor carpi ulnaris.Its
relationship to stability of the distal radio-ulnar
joint. Clin Orthop Relat Res. 1970;68:124-9.14. Ward LD, Ambrose
CG, Masson MV, Levaro F. Therole of the distal radioulnar
ligaments, interosseousmembrane, and joint capsule in distal
radioulnar jointstability. J Hand Surg [Am]. 2000;25:341-51.15.
Watanabe H, Berger RA, An KN, Berglund LJ, Zo-bitz ME. Stability of
the distal radioulnar joint con-tributed by the joint capsule. J
Hand Surg [Am].2004;29:1114-20.16. Marangoz S, Leblebicioglu G.
Stability of the dis-tal radioulnar joint contributed by the joint
capsule. JHand Surg [Am]. 2005;30:868-9.
17. Kleinman WB, Graham TJ. The distal radioulnar joint capsule:
clinical anatomy and role in posttrau-matic limitation of forearm
rotation. J Hand Surg[Am]. 1998;23:588-99.18. Kauer JM. The
articular disc of the hand. ActaAnat (Basel). 1975;93:590-605.19.
Schuind F, An KN, Berglund L, Rey R, Cooney WP3rd, Linscheid RL,
Chao EY. The distal radioulnar lig-aments: a biomechanical study. J
Hand Surg [Am].1991;16:1106-14.20. Ekenstam F. Osseous anatomy and
articularrelationships about the distal ulna. Hand
Clin.1998;14:161-4.21. Adams BD, Holley KA. Strains in the
articular diskof the triangular fibrocartilage complex: a
biomechani-cal study. J Hand Surg [Am]. 1993;18:919-25.22. Kihara
H, Palmer AK, Werner FW, Short WH, For-tino MD. The effect of
dorsally angulated distal radiusfractures on distal radioulnar
joint congruency andforearm rotation. J Hand Surg [Am].
1996;21:40-7.23. Lester B, Halbrecht J, Levy IM, Gaudinez R.Press
test for office diagnosis of triangular fibro-cartilage complex
tears of the wrist. Ann Plast Surg.1995;35:41-5.24. Epner RA,
Bowers WH, Guilford WB. Ulna vari-ancethe effect of wrist
positioning and roentgenfilming technique. J Hand Surg [Am].
1982;7:298-305.
-
7/25/2019 Distal Radioulnar Joint Instability
12/12
T HE JOURNAL OF B ON E & JOINT SURGERY JBJS.OR GVOLUME 88-A
N UMBER 4 APRIL 2006
D ISTAL R ADIOULNAR J OINT I NSTABILITY
25. Mino DE, Palmer AK, Levinsohn EM. The role ofradiography and
computerized tomography in the di-agnosis of subluxation and
dislocation of the distalradioulnar joint. J Hand Surg [Am].
1983;8:23-31.26. Mino DE, Palmer AK, Levinsohn EM. Radiographyand
computerized tomography in the diagnosis of in-congruity of the
distal radio-ulnar joint. A prospectivestudy. J Bone Joint Surg Am.
1985;67:247-52.27. Wechsler RJ, Wehbe MA, Rifkin MD, Edeiken
J,Branch HM. Computed tomography diagnosis of distalradioulnar
subluxation. Skeletal Radiol. 1987;16:1-5.28. Lo IK, MacDermid JC,
Bennett JD, Bogoch E,King GJ. The radioulnar ratio: a new method of
quan-tifying distal radioulnar joint subluxation. J HandSurg [Am].
2001;26:236-43.29. Steinbach LS, Smith DK. MRI of the wrist.
ClinImaging. 2000;24:298-322.30. Potter HG, Asnis-Ernberg L,
Weiland AJ, Hotch-kiss RN, Peterson MG, McCormack RR Jr. The
utilityof high-resolution magnetic resonance imaging in
theevaluation of the triangular fibrocartilage complex ofthe wrist.
J Bone Joint Surg Am. 1997;79:1675-84.31. Kocharian A, Adkins MC,
Amrami KK, McGee KP,Rouleau PA, Wenger DE, Ehman RL, Felmlee
JP.Wrist: improved MR imaging with optimized transmit-receive coil
design. Radiology. 2002;223:870-6.32. Yoshioka H, Ueno T, Tanaka T,
Shindo M, Itai Y.High-resolution MR imaging of triangular
fibrocarti-lage complex (TFCC): comparison of microscopycoils and a
conventional small surface coil. SkeletalRadiol. 2003;32:575-81.33.
Burk DL Jr, Karasick D, Wechsler RJ. Imaging ofthe distal
radioulnar joint. Hand Clin. 1991;7:263-75.34. Cone RO, Szabo R,
Resnick D, Gelberman R, Ta-leisnik J, Gilula LA. Computed
tomography of the nor-mal radioulnar joints. Invest Radiol.
1983;18:541-5.35. King GJ, McMurtry RY, Rubenstein JD, OgstonNG.
Computerized tomography of the distal radioul-nar joint:
correlation with ligamentous pathology in acadaveric model. J Hand
Surg [Am]. 1986;11:711-7.36. Linscheid RL. Disorders of the distal
radioulnar
joint. In: Cooney WP, Dobyns JH, Linscheid RL, edi-tors. The
wrist: diagnosis and operative treatment.St. Louis: Mosby; 1998. p
829.37. Garcia-Elias M, Dobyns JH. Dorsal and palmardislocations of
the distal radioulnar joint. In: CooneyWP, Dobyns JH, Linscheid RL,
editors. The wrist: di-agnosis and operative treatment. St. Louis:
Mosby;1998. p 768.38. Hermansdorfer JD, Kleinman WB. Managementof
chronic peripheral tears of the triangular fibrocar-tilage complex.
J Hand Surg [Am]. 1991;16:340-6.39. Singletary EM. Volar
dislocation of the distal ra-dioulnar joint. Ann Emerg Med.
1994;23:881-3.40. Adams BD, Samani JE, Holley KA. Triangular
fi-brocartilage injury: a laboratory model. J Hand Surg
[Am]. 1996;21:189-93.
41. Adams BD. Partial excision of the triangular fi-brocartilage
complex articular disk: a biomechanicalstudy. J Hand Surg [Am].
1993;18:334-40.42. Chidgey LK, Dell PC, Bittar ES, Spanier
SS.Histologic anatomy of the triangular fibrocartilage.J Hand Surg
[Am]. 1991;16:1084-100.43. Osterman AL. Arthroscopic debridement of
tri-angular fibrocartilage complex tears.
Arthroscopy.1990;6:120-4.44. Reinus WR, Hardy DC, Totty WG, Gilula
LA.Arthrographic evaluation of the carpal triangularfibrocartilage
complex. J Hand Surg [Am]. 1987;12:495-503.45. Palmer AK.
Triangular fibrocartilage complexlesions: a classification. J Hand
Surg [Am]. 1989;14:594-606.46. Minami A, Ishikawa J, Suenaga N,
Kasashima T.Clinical results of treatment of triangular
fibrocarti-lage complex tears by ar throscopic debridement. JHand
Surg [Am]. 1996;21:406-11.47. Millard GM, Budoff JE, Paravic V,
Noble PC.Functional bracing for distal radioulnar joint
insta-bility. J Hand Surg [Am]. 2002;27:972-7.48. Adams BD,
Divelbiss BJ. Reconstruction of theposttraumatic unstable distal
radioulnar joint. Or-thop Clin North Am. 2001;32:353-63, x.49.
Adams BD, Berger RA. An anatomic reconstruc-tion of the distal
radioulnar ligaments for posttrau-matic distal radioulnar joint
instability. J Hand Surg[Am]. 2002;27:243-51.50. Nishiwaki M,
Nakamura T, Nakao Y, Nagura T,Toyama Y. Ulnar shortening effect on
distal radioul-nar joint stability: a biomechanical study. J
HandSurg [Am]. 2005;30:719-26.51. Williams AA, Szabo RM. Case
report: radialovergrowth and deformity after metaphyseal frac-ture
fixation in a child. Clin Orthop Relat Res.2005;435:258-62.52.
Galeazzi R. ber ein besonderes syndrom bei
verletzungen im bereich der unterarmknochen. ArchOrthop
Unfallchir. 1935;35:557-62.53. Rettig ME, Raskin KB. Galeazzi
fracture-dislocation: a new treatment-oriented classifica-tion. J
Hand Surg [Am]. 2001;26:228-35.54. Alexander AH, Lichtman DM.
Irreducibledistal radioulnar joint occurring in a
Galeazzifracturecase report. J Hand Surg [Am]. 1981;6:258-61.55.
Essex-Lopresti P. Fractures of the radial headwith distal
radio-ulnar dislocation; report of twocases. J Bone Joint Surg Br.
1951;33:244-7.56. Szabo RM, Hotchkiss RN, Slater RR Jr. The useof
frozen-allograft radial head replacement for treat-ment of
established symptomatic proximal transla-tion of the radius:
preliminary experience in fivecases. J Hand Surg [Am].
1997;22:269-78. Erra-
tum in: J Hand Surg [Am]. 1997;22:765.
57. Nakamura T, Takayama S, Horiuchi Y, Yabe Y.Origins and
insertions of the triangular fibrocarti-lage complex: a
histological study. J Hand Surg[Br]. 2001;26:446-54.58. Hui FC,
Linscheid RL. Ulnotriquetral augmenta-tion tenodesis: a
reconstructive procedure for dor-sal subluxation of the distal
radioulnar joint. J HandSurg [Am]. 1982;7:230-6.59. Tsai TM,
Stilwell JH. Repair of chronic sublux-ation of the distal
radioulnar joint (ulnar dorsal) us-ing flexor carpi ulnaris tendon.
J Hand Surg [Br].1984;9:289-94.60. Breen TF, Jupiter JB. Extensor
carpi ulnaris andflexor carpi ulnaris tenodesis of the unstable
distalulna. J Hand Surg [Am]. 1989;14:612-7.61. Fulkerson JP,
Watson HK. Congenital anteriorsubluxation of the distal ulna. A
case report. ClinOrthop Relat Res. 1978;131:179-82.62. Scheker LR,
Belliappa PP, Acosta R, German DS.Reconstruction of the dorsal
ligament of the trian-gular fibrocartilage complex. J Hand Surg
[Br].1994;19:310-8.63. Sanders RA, Hawkins B. Reconstructionof the
distal radioulnar joint for chronic volardislocation. A case
report. Orthopedics. 1989;12:1473-6.64. Bowers WH. Distal
radioulnar joint arthroplasty.Current concepts. Clin Orthop Relat
Res. 1992;275:104-9.65. Gofton WT, Gordon KD, Dunning CE,
JohnsonJA, King GJ. Comparison of distal radioulnar joint
re-constructions using an active joint motion simulator.J Hand Surg
[Am]. 2005;30:733-42.66. Breen TF, Jupiter J. Tenodesis of the
chroni-cally unstable distal ulna. Hand Clin. 1991;7:355-63.67.
Wolfe SW, Mih AD, Hotchkiss RN, Culp RW,Keifhaber TR, Nagle DJ.
Wide excision of the distalulna: a multicenter case study. J Hand
Surg [Am].1998;23:222-8.68. Masaoka S, Longsworth SH, Werner FW,
ShortWH, Green JK. Biomechanical analysis of two ul-nar head
prostheses. J Hand Surg [Am]. 2002;27:845-53.69. Sauv L, Kapandji
M. Nouvelle technique detraitement chirurgical des luxations
rcidivantesisoles de lextrmit infrieure du cubitus. J
Chir.1936;47:589-94.70. Minami A, Suzuki K, Suenaga N, Ishikawa
J.The Sauv-Kapandji procedure for osteoarthritisof the distal
radioulnar joint. J Hand Surg [Am].1995;20:602-8.71. Lamey DM,
Fernandez DL. Results of themodified Sauv-Kapandji procedure in the
treat-ment of chronic posttraumatic derangement ofthe distal
radioulnar joint. J Bone Joint Surg Am.1998;80:1758-69.