Embed Size (px)
Citation preview

Disorganization of Inner Retina and Outer Retinal Morphology inDiabetic Macular Edema
Das, R., Spence, G., Hogg, R. E., Stevenson, M., & Chakravarthy, U. (2018). Disorganization of Inner Retinaand Outer Retinal Morphology in Diabetic Macular Edema. JAMA Ophthalmology, 1-7.https://doi.org/10.1001/jamaophthalmol.2017.6256
Published in:JAMA Ophthalmology
Document Version:Peer reviewed version
Queen's University Belfast - Research Portal:Link to publication record in Queen's University Belfast Research Portal
Publisher rights© 2018 American Medical Association. All rights reserved. This work is made available online in accordance with the publisher’s policies.Please refer to any applicable terms of use of the publisher.
General rightsCopyright for the publications made accessible via the Queen's University Belfast Research Portal is retained by the author(s) and / or othercopyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associatedwith these rights.
Take down policyThe Research Portal is Queen's institutional repository that provides access to Queen's research output. Every effort has been made toensure that content in the Research Portal does not infringe any person's rights, or applicable UK laws. If you discover content in theResearch Portal that you believe breaches copyright or violates any law, please contact [email protected].
Download date:03. Apr. 2022

1
Title- Disorganization of inner retina and outer retinal morphology in diabetic 1
macular edema 2
Authors 3
Radha Das FRCS, Queens University, Belfast 4
Email- [email protected] 5
Gareth Spence MB BCh, Belfast health and Social Care Trust 6
Email- [email protected] 7
Ruth E Hogg, PhD, Queens University, Belfast 8
Email- [email protected] 9
Michael Stevenson, PhD, Queens University, Belfast 10
Email- [email protected] 11
Usha Chakravathy, PhD, Queens University, Belfast 12
Email- [email protected] 13
14
Corresponding Author 15
Professor Usha Chakravarthy 16
Centre for Public health 17
Institute of Clinical Sciences A 18
Queen’s University of Belfast 19
Royal Victoria Hospital, Belfast BT12 6BA 20
Email – u.chakravarthy @qub.ac.uk 21
Phone- 028 9097 1654 22
23
Manuscript word count- 2993 24

2
Question: To characterize retinal morphology using spectral domain optical 25
coherence tomography in a large series of eyes with diabetic macular edema 26
(DME). 27
Findings: In this cross sectional observational case series that included one 28
hundred and two eyes from 80 individuals, disorganization of inner retinal layer 29
(DRIL) was strongly associated with the disruption of outer retinal layers. DRIL 30
was more frequently observed in eyes with increasing severity of diabetic 31
retinopathy and associated with poorer visual acuity. 32
Meaning: DRIL was associated with morphological changes in the outer retina 33
and worse levels of DR in eyes with DME. 34
Abstract 35
36
Importance: In diabetic macular edema (DME), identification of baseline markers 37
on spectral domain optical coherence tomography (SD-OCT) and their 38
relationship with severity of diabetic retinopathy (DR) might aid in the 39
management and in designing future trials. 40
Objective: To examine relationships between DR severity, retinal morphology on 41
SD-OCT and visual acuity (VA) in participants with DME. 42
Design: Cross sectional observational case series. 43
Setting: A single tertiary care referral center. 44

3
Participants: Demographics, VA, SD-OCT and color fundus photographs of 80 45
individuals with DME (102 eyes) seen between December 28th 2013 and 31st 46
April 2014 with data analysed between May and July 2016. 47
On SD-OCT we graded type and shape of DME, shape and presence of septae 48
within the intra retinal cystoid abnormalities, presence of hyper reflective dots and 49
foci, integrity of the external limiting membrane (ELM) and ellipsoid zone (EZ), 50
presence and extent of disorganization of inner retinal layer (DRIL), the status of 51
the vitreomacular interface and epiretinal membrane (ERM). We measured retinal 52
thickness at the fovea (RTF) and at the site of maximum pathology, choroidal 53
thickness (CT) at the fovea and 1000µ temporal and nasal to fovea. Color 54
photographs were graded to derive a DR severity stage. 55
Main Outcomes and Measures: SD-OCT features and thickness metrics. 56
Results: The mean age (SD) was 63 +/-11 and 37.5% were females. The odds of 57
having DRIL were greater in eyes with disrupted ELM (OR 4.4, 95% CI (1.6 to12), 58
P =. 003), disrupted EZ (OR 2.7, 95% CI (1 to 7.2), P = .03), presence of ERM 59
(OR 2.8, CI (1 to 7.4), P =. 03) and increase in RTF (OR 1.6, 95% CI (1.1 to 2.2), 60
P<. 001). DRIL was more likely to occur in eyes with proliferative DR (OR 7.3, 61
95% CI (1.7 to 31.4), P =. 007). Mean VA decreased by approximately 4.7 letters 62
for each 100-μm increase in the average global DRIL (95% CI (-7.9 to 1.4), P=. 63
006). 64
65
Conclusions and Relevance: DRIL was associated with disruption of outer 66
retina and increasing DR severity. Further studies are warranted to establish 67
DRIL as a non-invasive morphological marker in eyes with DME. 68

4
Introduction 69
Diabetic retinopathy (DR) represents a spectrum of pathological changes that 70
occur in the microvasculature of the eye in patients with Diabetes Mellitus (DM). 71
Diabetic macular edema (DME) is a characteristic feature of DR and an important 72
cause of visual loss in people with DM 1. DME is an accumulation of fluid within 73
the macular tissue layers, which arises as a consequence of failure of the blood-74
retinal barrier (BRB). Typically DME causes blurring and distortion of vision, 75
which is reflected in a reduction in visual acuity (VA). The Wisconsin 76
Epidemiologic Study of Diabetic Retinopathy (WESDR) found that 20% of 77
patients with type 1 DM and 25% of those with type 2 DM will develop DME after 78
10 years of follow up 2. 79
Although DME is detectable as increases in macular thickness based on 80
biomicroscopic examination and through stereoscopic assessments of fundus 81
color images, the introduction of time domain optical coherence tomography 82
(OCT) enabled a more precise quantification of overall retinal thickness but this 83
measure was found to correlate only modestly with VA 3. The subsequent 84
availability of spectral domain OCT (SD-OCT) with superior resolution and 85
reproducibility has resulted in improved ability to differentiate early DME from 86
normality and also permits characterization of pathology on a retinal layer by 87
layer basis. Features such as hyper reflective foci can be localized to individual 88
retinal layers or as recently shown to be within the walls of microaneurysms 4. 89
Studies have been undertaken and have established correlations between VA 90
and certain features of retinal morphology such as the intactness of the ellipsoid 91
zone (EZ) and external limiting membrane (ELM) 5-7. A recent report from Sun et 92
al described an OCT feature termed disorganization of the retinal inner layers 93

5
(DRIL), improvement in which was predictive of better VA outcomes 8,9. Notably 94
DRIL was found to be associated with VA after resolution of center-involving DME 95
10. Although relationships between DRIL and VA have been explored, to date no 96
data exists on the relationships between DRIL and other OCT features of DME or 97
with severity of DR. The present study represents a systematic examination of 98
the relationships between DRIL and SD-OCT features of DME, severity of DR 99
and VA in a large series of eyes with DME. 100
101
Methods 102
This was a cross-sectional retrospective observational case series at a single 103
clinical center. The study adhered to the tenets of the Declaration of Helsinki and 104
full ethical approval from the local ethics committee (REC 105
reference14/NI/1025 ). Details of patients attending this clinic recorded in the 106
electronic medical records (EMR) were reviewed. 107
A standardized protocol using trained examiners is used to test and record VA, 108
which is measured on the Early Treatment Diabetic Retinopathy Study (ETDRS) 109
chart. Tomographic images were captured (Spectralis, Heidelberg Engineering, 110
Heidelberg, Germany) on both eyes at all visits and consists of a single horizontal 111
and vertical line scan through the fovea followed by a 6 x 6 mm macular raster 112
scan (37 raster lines spacing of 120μm, 20o *15o ). Color photographs (2 fields -113
macula centered and optic disc centered) were captured on a Visucam 500 (Carl 114
Zeiss Meditec, Oberkochen, Germany) after pupillary dilation. 115
The EMR was interrogated for patients with a diagnosis of DME who attended a 116
retina service between December 28th 2013 and 31st April 2014. The data 117

6
analysis was performed from May 2016 July 2016. 118
From the 94 unique cases we selected the records of 80 patients with a 119
confirmed diagnosis of DM type 1 or 2, with OCT features of DME, color fundus 120
photography and a VA record corresponding to the same visit. Exclusions were 121
diagnosis not DM, age < 18 years, OCT or fundus photographs not available. 122
We extracted information on age, sex, duration of DM, history of hypertension, 123
hyperlipidemia and cigarette smoking from the EMR for each case. 124
Image analysis 125
Grading was performed by two of the authors (R.D and G.S) after training by the 126
senior clinician (U.C.) who checked 20% of the grading outputs. Intergrader 127
variability was assessed by kappa statistics. The images were scrutinized on the 128
proprietary software provided by the manufacturer of the OCT acquisition system. 129
All of the B scans of the 6x6 macular raster were examined and we recorded the 130
type and shape of DME, shape of the intra retinal cystoid abnormalities and 131
septae if seen within the cystoid abnormalities, presence or absence of hyper 132
reflective dots and foci, and the status of the vitreomacular interface and 133
presence of an epiretinal membrane (ERM). We identified the foveal B scan 134
(defined as the scan passing through the maximal foveal depression) and 135
measured the horizontal extent of DRIL and disruption of the ELM and EZ. In the 136
dataset fewer than 10% of eyes were classified as not showing a foveal dip. In 137
these cases where the foveal scan was not clearly identifiable we used the scan, 138
which is offset by 5 degrees from the horizontal as the scan of choice. We also 139
measured the retinal thickness at the fovea (RTF) and at the site of maximum 140
pathology (maximum retinal thickness; MRT). We measured choroidal thickness 141

7
(CT) at the fovea and 1000µ temporal and nasal to fovea. The grading form is 142
shown in eTable 1 in the supplement. 143
We defined DRIL as the presence of a region on the B scan where the 144
boundaries between the ganglion cell–inner plexiform layer complex, inner 145
nuclear layer, and outer plexiform layer could not be separately identified. The 146
method used to determine the horizontal extent of DRIL in each of 7 B-scans was 147
identical that described by Sun et al in that we only measured the diameter upto a 148
maximum of 1000 μM. The B scans that were selected were the foveal scan and 149
the 3 immediately superior and inferior to the foveal scan. The measurements 150
from these 7 scans were summed to derive an average global DRIL measure for 151
each eye 8. 152
We graded the color photographs according to the ETDRS grading protocol 11 to 153
derive a DR severity stage. 154
Statistical analysis 155
We analyzed the data using SPSS version 22. We performed kappa statistics to 156
test the intergrader variability. We examined relationships between VA and age 157
and duration of diabetes using linear regression. We performed one-way 158
analysis of variance (ANOVA) for associations between VA with hypertension, 159
hyperlipidemia and smoking. We also used ANOVA to test relationships 160
between VA and the various categorical variables (retinal morphological features 161
observed on OCT and DR severity staging). . We used Pearson’s coefficient to 162
test for correlations between VA and OCT linear variables (diameter of DRIL, 163
disrupted ELM and EZ, height of RTF, MRT, and CT). With VA as the dependent 164
variable, those variables that reached significance in the preceding steps were 165

8
then tested using general linear regression modelling (GLM) after controlling for 166
RTF, which had been previously identified as a confounder factor by Sun et al 8. 167
As DRIL had been identified as a key determinant of VA outcome8,we performed 168
binary logistic regression to seek associations between presence or absence of 169
DRIL with SD OCT features and DR severity. We tested pairs of variables and we 170
did not create a multivariable model as the modest sample size could have lead 171
to invalidation of the independence of the observations on the variable of interest. 172
The interclass correlation of eyes with the same person was 0.08 and so we did 173
not deem it necessary to adjust for correlations between 2 eyes. We considered 174
P ≤. 05 as statistically significant in these analyses. 175
Results 176
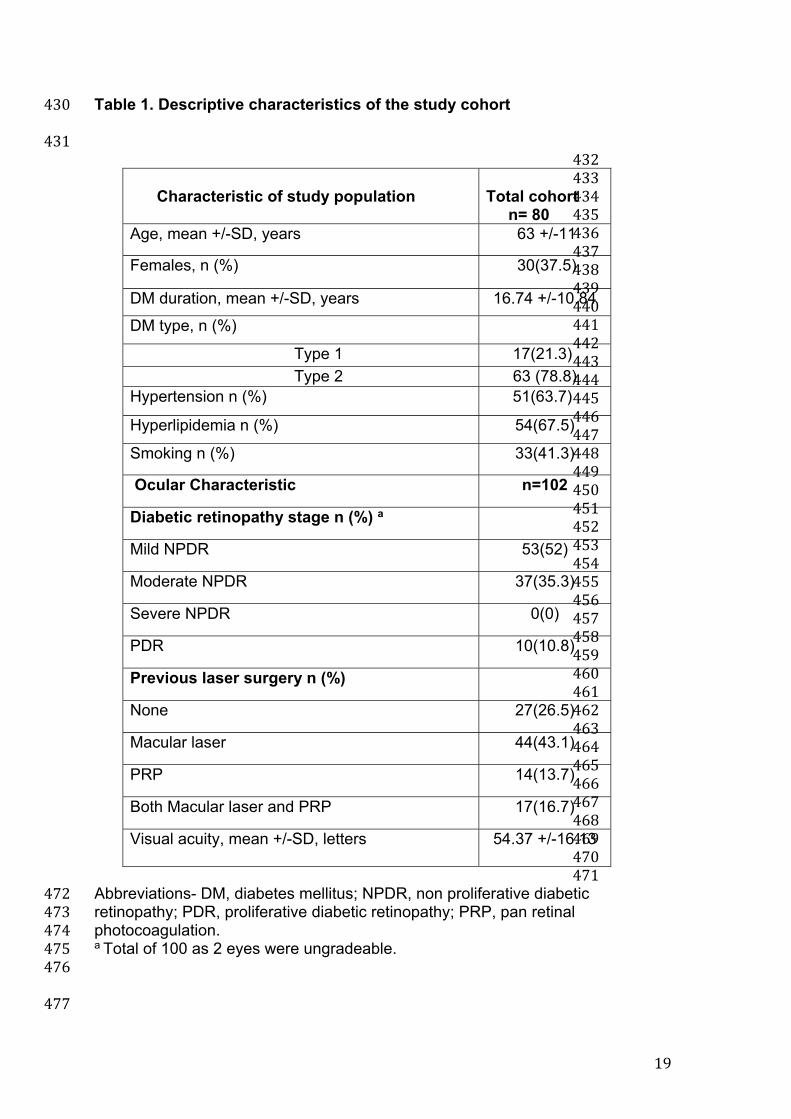
Descriptive characteristics of the study cohort are shown in Table 1. 177
One hundred and two eyes of 80 individuals were analysed. Due to poor quality 178
OCT images, one eye was not graded for OCT morphology and metrics. The 179
mean age was 63 (SD, 11) years, 30 (37.5%) were females, with the majority of 180
the sample having type 2 DM (Table 1). The frequency of the DR severity stages 181
in the 100 eyes (2 eyes were not graded due to poor quality colour images) is 182
shown in Table 1. Less than half of the included eyes had been previously treated 183
with macular laser and none had received an anti vascular endothelial growth 184
factor (VEGF) treatment. The intergrader variability was tested using kappa and 185
as large number of variables were graded, we provide the range of kappa values, 186
which was from 0.6 to 1. Linear regression of VA against age and duration of DM 187
showed no significant associations. ANOVA also confirmed the absence of 188
associations with key systemic features of hypertension, hyperlipidemia and 189

9
smoking. (e Table 2). Therefore these variables were not included in any of the 190
subsequent analyses. 191
Associations between VA and retinal morphological features identified specific 192
variables that reached statistical significance on the ANOVA. These were, shape 193
of DME, presence of septae in intraretinal cystoid abnormalities, presence of 194
DRIL and disruption of ELM and EZ and DR severity stage. Other variables that 195
were tested [type and symmetry of intra retinal fluid, presence of cystoid 196
abnormalities and ERM] did not reach significance (eTable 3). Pearsons 197
correlation coefficients (e Table 4) showed significant correlations between VA 198
and horizontal extent of DRIL, ELM and EZ, RTF and MRT. 199
The results from GLM adjusted for RTF are shown in Table 2. Variables that lost 200
significance in the model were shape of DME and presence of septae in cystoid 201
abnormalities (Table 2) while all others remained significant. The parameter 202
estimates show that better VA is associated with absence of DRIL, intact ELM 203
and EZ and less severe stages of DR (Table 2). Presence of intact ELM is 204
associated with a 14 letter better mean VA (14 (95 % CI 7.9 to 19.8) P < 0.001) 205
compared to eyes with disrupted ELM. Similar differences in VA were also found 206
when the EZ was intact (10.5(4.7 to 16.4) P = 0.001) and when DRIL was absent 207
(9.8 (3 to 16.6) P < 0.001). 208
The parameter estimates indicate that for each 100-μm increase in the average 209
global DRIL, there is a decrease in the mean VA of approximately 4.6 letters 210
(Table 3). With each 100 μm increase in disruption of ELM and EZ, the mean VA 211
decreased by 0.4 letters. For each 100 μm of increase in RTF and MRT, VA 212
decreased by 2.4 and 0.04 letters respectively. After adjustment for RTF, all the 213
variables remained significant. The MRT variable showed a strong impact on VA 214

10
with each 100-μm increase in retinal thickness resulting in a decrease of 13.1 215
letters (-19.6 to -6.6, P <0.001). Figure 1A shows the presence of disrupted ELM 216
and EZ. 217
218
Relationship between DRIL and other OCT features of DME and DR 219
Binary logistic regression showed that the odds of having DRIL was greater in 220
eyes with disrupted ELM (odds ratio 4.4, 95% CI (1.6 to12), P=. 003) and 221
disrupted EZ (OR 2.7,1 to 7.2, P =. 03), presence of ERM (OR 2.8, 1 to 7.4, P =. 222
03) and increase in RTF (OR 1.6,1.1 to 2.2, P <. 001) (Table 4). DRIL was more 223
likely to occur in eyes with PDR (OR 7.3, 1.7 to 31.4, P = .007) (Table 4). Figure 224
1B is an example of DRIL in an eye with ERM. 225
Discussion 226
We systematically graded the tomographic images of the retina and sought 227
relationships between the presence and severity of a number of morphological 228
features of DME including DRIL a novel and recently described biomarker with 229
severity of DR and visual function. Results from this study suggest that centrally 230
located DRIL is correlated with VA in eyes with center-involved DME and was 231
strongly associated with the disruption of ELM and EZ layers and presence of 232
ERM. Worsening of VA was seen with increasing DR severity and may be related 233
to the presence of DRIL. The presence of central location of DRIL and the extent 234
of disruption were both associated with worse VA and these findings are similar 235
to previous studies, which found DRIL to be a predictive marker for VA outcomes 236
in eyes with resolved DME after treatment 8-10. A an important finding from our 237
analysis has been the elucidation of the relationship between the horizontal 238
extent of DRIL and VA and we have shown that for each 100 micron increase in 239

11
DRIL there is a negative impact of around 6 letters which is more than one line on 240
the Early Treatment Diabetic Retinopathy Study (ETDRS) chart. It has been 241
hypothesized that disorganization of the inner retina occurs when bipolar axons 242
snap at a point when their elasticity limit has been exceeded due to edema 12. It 243
has also been suggested that DRIL represents loss of bipolar, amacrine or 244
horizontal cells within the inner retinal layers 8. Key findings from the present 245
analysis also include the highly significant relationships between presence of 246
DRIL and outer retinal changes. DRIL was strongly associated with the disruption 247
of ELM and EZ layers. In our study RTF was significantly increased in the 248
presence of DRIL and taken together suggest that the mechanisms that create 249
the conditions for inner retinal disorganization may also be responsible for 250
concurrent disruption of the outer retinal architecture. 251
We noted that these outer retinal changes were also associated with poor VA and 252
our findings are consistent with those from previous studies 5,7,13,14. . Breakdown 253
of the BRB in DME could create the conditions for damage to the ELM and EZ. 254
Unlike DRIL where mechanical forces have been considered in its pathogenesis, 255
it has been postulated that the disrupted ELM occurs as a consequence of 256
impaired retinal function 14. It is presently unknown if the EZ line seen on OCT 257
images truly corresponds to the histologic junction of the inner and outer 258
segments. An important consideration with the growing literature regarding the 259
EZ is how to objectively and consistently evaluate disruption. Maheshwary et al 5 260
concluded that not only is the status of Inner segment/Outer segment, disruption 261
important, but the percentage disruption is a predictor of visual acuity in a patient. 262
Spaide and Curcio speculated that this highly reflective band was located at the 263
ellipsoid in the inner segments, considering the correlation between the 264

12
microstructure on the SD-OCT images and the histologic findings 15. Our present 265
work not only reinforces the important clinical relevance of an intact EZ but also 266
suggests that the same pathogenic pathways that create conditions for DRIL may 267
also disrupt the outer retinal architecture. 268
Cystic changes that appear within the macula represent focal areas of coalesced 269
extra cellular fluid. These foci of fluid likely result from disturbed cellular function 270
of the Müller cells, which are thought to play an important role in acting as 271
metabolic pumps to keep the macula dehydrated 16,17. Based on the univariate 272
analysis undertaken in the present study we noted that VA was better in eyes 273
with septae within the cystoid abnormalities compared to those without and our 274
findings support those of previous investigators. 275
Many studies have shown that ERM is common in eyes with DME and similarly 276
we observed a high frequency of ERM in the present series. We systematically 277
graded for ERMs that are recognized on OCT as thin, hyperreflective bands 278
anterior to the retina or bright red bands in the pseudocolor representation on 279
OCT 18. Gandorfer et al showed that ERMs in DME consist of multilayered 280
membranes situated on a layer of native vitreous collagen, predominantly 281
coupled with fibroblasts and fibrous astrocytes 19. Removal of the ERM by 282
vitrectomy and membrane peel can result in resolution of the DME and 283
improvements in VA 19,20. To date no study has examined the associations 284
between ERM, DRIL and VA and our observations of a strong relationship 285
between these features suggest a common pathological process. Histological 286
studies are required to understand the pathogenetic mechanisms underpinning 287
these inner retinal morphological manifestations. 288

13
A prospective study investigated the correlation between the features of OCT 289
and the severity of retinopathy 21. This study found that the prevalence of DME 290
with serous retinal detachment and with vitreomacular traction was higher in eyes 291
with severe NPDR to PDR than in eyes with mild-to-moderate 21. It is also known 292
that increasing DR severity is associated with macular thickening 22. While the 293
present study also shows similar findings it is the first to report an association 294
between DRIL and increasing severity of DR. Our finding of worsening of VA with 295
increasing DR severity may be related to the presence of DRIL. 296
A biomarker that is of interest is the visibility of the cone outer receptor segments 297
(COST). It has been shown that there is reduced visibility of COST in patients 298
with DME. During grading we observed that COST lines could not be delineated 299
consistently therefore we did not grade for this biomarker. Our experience is 300
similar to that of Rii et al who found that these outer retinal layers could not be 301
segmented even in normal eyes scans 23. 302
The strengths of this study are the systematic grading of color and OCT images 303
and the homogenous sample of patients with DME naïve to treatment with anti 304
VEGF. An important limitation of the study is its cross-sectional design and 305
hence we are unable to predict the impact on function over time of the various 306
OCT markers that we identified. Also our study is retrospective and, the sample 307
size is modest. Furthermore the data were acquired as part of routine clinical care 308
and thus many patients had prior exposure to laser photocoagulation, which can 309
alter the appearance of the retinal layers. However we believe our findings do not 310
arise as a consequence of laser treatment since the foveal retina is avoided while 311
undertaking macular laser. 312
313

14
In summary we have systematically studied both inner and outer retinal 314
morphology in DME and relationships both with VA and increasing severity of DR. 315
316
Conclusion 317
DRIL correlated with the integrity of outer retinal architecture and the presence of 318
ERM. The odds of having DRIL increased with DR severity. DRIL requires further 319
investigation in large clinical trials across multiple sites with prospective data 320
collection with adjustment for multiple potential confounders including VA and 321
other morphological features on OCT to be considered as a non-invasive marker. 322
323
Acknowledgement- 324
Dr Alyson Muldrew, senior grader, netWORC UK 325
Professor Usha Chakravarthy had full access to all the data in the study and 326
takes responsibility for the integrity of the data and the accuracy of the data 327
analysis. 328
329
330
331
332
333
334
335
336
337
338

15
References 339
1. Moss SE, Klein R, Klein BE. The 14-year incidence of visual loss in a diabetic population. 340
Ophthalmology. 1998;105(6):998-1003. doi: 10.1016/S0161-6420(98)96025-0. 341
2. Klein R, Klein BE, Moss SE, Cruickshanks KJ. The wisconsin epidemiologic study of diabetic 342
retinopathy. XV. the long-term incidence of macular edema. Ophthalmology. 1995;102(1):7-16. 343
3. Diabetic Retinopathy Clinical Research Network, Browning DJ, Glassman AR, et al. 344
Relationship between optical coherence tomography-measured central retinal thickness and visual 345
acuity in diabetic macular edema. Ophthalmology. 2007;114(3):525-536. doi: 346
10.1016/j.ophtha.2006.06.052. 347
4. Bolz M, Schmidt-Erfurth U, Deak G, et al. Optical coherence tomographic hyperreflective foci: 348
A morphologic sign of lipid extravasation in diabetic macular edema. Ophthalmology. 349
2009;116(5):914-920. doi: 10.1016/j.ophtha.2008.12.039; 10.1016/j.ophtha.2008.12.039. 350
5. Maheshwary AS, Oster SF, Yuson RM, Cheng L, Mojana F, Freeman WR. The association 351
between percent disruption of the photoreceptor inner segment-outer segment junction and visual 352
acuity in diabetic macular edema. Am J Ophthalmol. 2010;150(1):63-67.e1. doi: 353
10.1016/j.ajo.2010.01.039; 10.1016/j.ajo.2010.01.039. 354
6. Otani T, Yamaguchi Y, Kishi S. Correlation between visual acuity and foveal microstructural 355
changes in diabetic macular edema. Retina. 2010;30(5):774-780. doi: 356
10.1097/IAE.0b013e3181c2e0d6; 10.1097/IAE.0b013e3181c2e0d6. 357
7. Shin HJ, Lee SH, Chung H, Kim HC. Association between photoreceptor integrity and visual 358
outcome in diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2012;250(1):61-70. doi: 359
10.1007/s00417-011-1774-x; 10.1007/s00417-011-1774-x. 360

16
8. Sun JK, Lin MM, Lammer J, et al. Disorganization of the retinal inner layers as a predictor of 361
visual acuity in eyes with center-involved diabetic macular edema. JAMA Ophthalmol. 362
2014;132(11):1309-1316. doi: 10.1001/jamaophthalmol.2014.2350 [doi]. 363
9. Sun JK, Radwan SH, Soliman AZ, et al. Neural retinal disorganization as a robust marker of 364
visual acuity in current and resolved diabetic macular edema. Diabetes. 2015;64(7):2560-2570. 365
doi: 10.2337/db14-0782 [doi]. 366
10. Radwan SH, Soliman AZ, Tokarev J, Zhang L, van Kuijk FJ, Koozekanani DD. Association 367
of disorganization of retinal inner layers with vision after resolution of center-involved diabetic 368
macular edema. JAMA Ophthalmol. 2015;133(7):820-825. doi: 369
10.1001/jamaophthalmol.2015.0972 [doi]. 370
11. ETDRS report number 10. Grading diabetic retinopathy from stereoscopic color fundus 371
photographs--an extension of the modified airlie house classification. Early treatment diabetic 372
retinopathy study research group. Ophthalmology. 1991;98(5 Suppl):786-806. 373
12. Pelosini L, Hull CC, Boyce JF, McHugh D, Stanford MR, Marshall J. Optical coherence 374
tomography may be used to predict visual acuity in patients with macular edema. Invest 375
Ophthalmol Vis Sci. 2011;52(5):2741-2748. doi: 10.1167/iovs.09-4493 [doi]. 376
13. Forooghian F, Stetson PF, Meyer SA, et al. Relationship between photoreceptor outer segment 377
length and visual acuity in diabetic macular edema. Retina. 2010;30(1):63-70. doi: 378
10.1097/IAE.0b013e3181bd2c5a; 10.1097/IAE.0b013e3181bd2c5a. 379
14. Murakami T, Nishijima K, Sakamoto A, Ota M, Horii T, Yoshimura N. Association of 380
pathomorphology, photoreceptor status, and retinal thickness with visual acuity in diabetic 381
retinopathy. Am J Ophthalmol. 2011;151(2):310-317. doi: 10.1016/j.ajo.2010.08.022; 382
10.1016/j.ajo.2010.08.022. 383

17
15. Spaide RF, Curcio CA. Anatomical correlates to the bands seen in the outer retina by optical 384
coherence tomography: Literature review and model. Retina. 2011;31(8):1609-1619. doi: 385
10.1097/IAE.0b013e3182247535 [doi]. 386
16. Rotsos TG, Moschos MM. Cystoid macular edema. Clin Ophthalmol. 2008;2(4):919-930. 387
17. Deak GG, Bolz M, Ritter M, et al. A systematic correlation between morphology and 388
functional alterations in diabetic macular edema. Invest Ophthalmol Vis Sci. 2010;51(12):6710-389
6714. doi: 10.1167/iovs.09-5064 [doi]. 390
18. Panozzo G, Parolini B, Gusson E, et al. Diabetic macular edema: An OCT-based 391
classification. Semin Ophthalmol. 2004;19(1-2):13-20. 392
19. Gandorfer A, Rohleder M, Grosselfinger S, Haritoglou C, Ulbig M, Kampik A. Epiretinal 393
pathology of diffuse diabetic macular edema associated with vitreomacular traction. Am J 394
Ophthalmol. 2005;139(4):638-652. doi: S0002-9394(04)01398-4 [pii]. 395
20. Sakimoto S, Saito Y, Nakata K, Sakamoto Y, Tatebayashi M. Surgical outcomes of epiretinal 396
membrane removal after successful pars plana vitrectomy for retinal diseases. Jpn J Ophthalmol. 397
2008;52(3):227-230. doi: 10.1007/s10384-008-0539-5 [doi]. 398
21. Alkuraya H, Kangave D, Abu El-Asrar AM. The correlation between optical coherence 399
tomographic features and severity of retinopathy, macular thickness and visual acuity in diabetic 400
macular edema. Int Ophthalmol. 2005;26(3):93-99. doi: 10.1007/s10792-006-9007-8 [doi]. 401
22. Browning DJ, Fraser CM, Clark S. The relationship of macular thickness to clinically graded 402
diabetic retinopathy severity in eyes without clinically detected diabetic macular edema. 403
Ophthalmology. 2008;115(3):533-539.e2. doi: S0161-6420(07)00749-X [pii]. 404

18
23. Rii T, Itoh Y, Inoue M, Hirakata A. Foveal cone outer segment tips line and disruption 405
artifacts in spectral-domain optical coherence tomographic images of normal eyes. Am J 406
Ophthalmol. 2012;153(3):524-529.e1. doi: 10.1016/j.ajo.2011.08.021 [doi]. 407
408
409
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
19
Table 1. Descriptive characteristics of the study cohort 430
431 432 433 434 435 436 437 438 439 440 441 442 443 444 445 446 447 448 449 450 451 452 453 454 455 456 457 458 459 460 461 462 463 464 465 466 467 468 469 470 471
Abbreviations- DM, diabetes mellitus; NPDR, non proliferative diabetic 472retinopathy; PDR, proliferative diabetic retinopathy; PRP, pan retinal 473photocoagulation. 474a Total of 100 as 2 eyes were ungradeable. 475 476
477
Characteristic of study population
Total cohort n= 80
Age, mean +/-SD, years 63 +/-11
Females, n (%) 30(37.5)
DM duration, mean +/-SD, years 16.74 +/-10.84
DM type, n (%)
Type 1 17(21.3)
Type 2 63 (78.8) Hypertension n (%) 51(63.7)
Hyperlipidemia n (%) 54(67.5)
Smoking n (%) 33(41.3)
Ocular Characteristic n=102
Diabetic retinopathy stage n (%) a
Mild NPDR 53(52)
Moderate NPDR 37(35.3)
Severe NPDR 0(0)
PDR 10(10.8)
Previous laser surgery n (%)
None 27(26.5)
Macular laser 44(43.1)
PRP 14(13.7)
Both Macular laser and PRP 17(16.7)
Visual acuity, mean +/-SD, letters
54.37 +/-16.13

20
Table 2. Associations between VA and retinal morphological features of DME 478and DR a 479Variable VA (letters)
mean +/-SD B (95%CI) P value
Shape of DME Dome 54.7 +/- 14.4 -1.7 (-9.1 to 5.5) .62 Fusiform 56.9 +/- 15.3 reference Septae in cystoid abnormalities
Yes 57.15 +/- 13.5 reference .19 No 49.95 +/-15.0 -4.7 (-11.9 to 2.4) DRIL Yes 46.1+/-14.9 reference No 58.1+/-13.5 9.8 (3.0 to 16.6) <.001 b ELM disrupted Yes 46.1+/-14.8 reference No 61.0+/-11.5 13.9(7.9 to 19.8) <.001 b EZ disrupted Yes 48.2+/-14.8 reference No 60.6+/-12.4 10.5(4.7 to 16.4) .001 b DR severity stage Mild NPDR 59.9+/-14.09 11.6 (2.0 to 21.1) .01 b Moderate NPDR 55.0+/-14.6 8.8(-1.0 to 18.7) .07 PDR 45.1+/-14.2 reference Abbreviations- VA, visual acuity; DME, diabetic macula edema; DRIL, 480disorganization of inner retinal layers; ELM, external limiting membrane; EZ, 481ellipsoid zone; DR, diabetic retinopathy; NPDR, non proliferative diabetic 482retinopathy; PDR, proliferative diabetic retinopathy. 483a Results are reported from General linear regression model adjusted for Retinal 484thickness at fovea. 485b P <.05. 486
487
488
489
490
491
492
493
494
495

21
Table 3- Correlations between VA and OCT derived linear variables a 496
Variable B (95%CI) P value
B (95%CI) P value ( adjusted for RTF)
RTF per 100 μm -2.4(-4 to -0.7), .005b MRT per 100 μm -0.04 (-.08 to-.01), .01 b -13.1(-19.6 to -6.6),
<.001 b Average global DRIL per 100 μm
-4.6(-8 to -1.3), .009 b -4.7 (-7.9 to -1.4), .006 b
ELM disruption at fovea per 100 μm
-0.4(-0.8 to -0.1), .01 b -0.5 (-0.9 to -0.1), .01 b
EZ disruption at fovea per 100 μm
-0.4(-0.7 to -0.1), .003 b -0.4(-0.7 to -0.1), .008 b
Abbreviations- VA, visual acuity; OCT, optical coherence tomography; RTF, retinal 497thickness at fovea; MRT, maximum retinal thickness; DRIL, disorganization of 498inner retinal layers; ELM, external limiting membrane; EZ, ellipsoid zone. 499a Results are reported from General linear regression model. 500b P<.05 501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517

22
Table 4- Relationship between DRIL with other retinal morphological 518features of DME and DR a 519 DRIL OR (95% CI) P value Variable n
Yes n
No n
Type of DME IRF only 17 55 IRF and SRF 6 23 0.8(.2 to 2.4) .7 Type of IRF Diffuse 4 17 reference Cystoid 5 21 1(0.2 to 4.3) .9 Mixed 14 40 1(0.2 to 4.3) .5 Cystoid abnormalities in inner retina
Yes 20 61 1.8(.4 to 7) .3
No 3 17 reference Septae in the cystoid abnormalities
Yes 13 46 0.6(.2-1.7) .3
No 7 15 reference IRF symmetry at fovea
Symmetrical 17 52 0.7(.2 to 2) .5
Asymmetrical 6 26 reference DME shape Dome 14 37 0.5(0.2 to1.4) .2 Fusiform 9 41 reference ERM Yes 11 19 2.8(1 to 7.4) .03b No 12 59 reference ELM disrupted
Yes 15 23 4.4(1.6 to12) .003 b
No 8 55 reference EZ disrupted Yes 14 28 2.7(1 to 7.2) .03 b No 9 50 reference RTF (linear variable)
NA NA 1.6(1.1 to 2.2)
<.001 b
DR severity scale
Mild NPDR 9 44 reference
Moderate NPDR
8 29 1.3(.4 to 3.8) .5
PDR 6 4 7.3(1.7 to 31.4)
.007 b
Abbreviations- DME, diabetic macular edema;DR, diabetic retinopathy; IRF, 520intraretinal fluid; SRF, subretinal fluid; ERM, epiretinal membrane;ELM, external 521limiting membrane; EZ, ellipsoid zone;RTF, retinal thickness at fovea; NPDR, non 522proliferative diabetic retinopathy; PDR, proliferative DR. 523a Results are reported form Binary logistic regression with DRIL presence as the 524dependent variable. 525b P <.05 526 527

23
528
Figure 1 A and B 529
530
531
532
A- SD-OCT image showing disrupted ELM and EZ in DME. The yellow line 533
denotes disruption of the ELM and EZ 534
B- SD-OCT image showing the presence of DRIL and ERM in DME. 535
Arrow depicts the ERM. The area of DRIL is denoted by a line where 536
the retinal boundaries cannot be identified. 537
538
539
540
541

24
542
543
544
545
546
547
548










![MEF2C Ablation in Endothelial Cells Reduces Retinal Vessel ... · MEF2C Ablation in Endothelial Cells Reduces Retinal ... (VO)] results in hypoxic retina, which secretes growth factors](https://img.dokumen.tips/doc/110x75/6074652eae791d1ccd15870e/mef2c-ablation-in-endothelial-cells-reduces-retinal-vessel-mef2c-ablation-in.jpg)














![Design of lensless retinal scanning display with ...sdl.sjtu.edu.cn/uploadfiles/2019/07/201907112312131213.pdf · coincides with the retina. Virtual retinal display (VRD) [23–25],](https://img.dokumen.tips/doc/110x75/5f87583e8044cd0abd514c26/design-of-lensless-retinal-scanning-display-with-sdlsjtueducnuploadfiles201907.jpg)



