Embed Size (px)
DESCRIPTION
Diseases and Injuries of the Fetus and Newborn
Citation preview
DISEASES AND INJURIES OF THE FETUS AND NEWBORNOrpha Montillano-Corrado, MD
I. Diseases Common In The Preterm Fetus And NewbornII. Diseases Of The TermIII. Injuries Or The Fetus And Newborn
DISEASES COMMON IN THE PRETERM FETUS AND NEWBORN
RESPIRATORY DISTRESS SYNDROME (Hyaline membrane disease) can develop in term newborns with sepsis and meconium aspiration Clinical Findings:
Tachypnea Chest wall retractions Expiration with grunting and nasal flaring
Pathology If surfactant is inadequate, hyaline membranes form in the distal
bronchioles and alveoli, Low pressures cause collapse at end expiration
Respiratory insufficiency can be caused by sepsis, pneumonia, meconium aspiration, pneumothorax, heart failure malformations involving thoracic structures
Inadequate surfactant with subsequent lung collapse Unstable alveoli---low pressure cause collapse at end expiration Immaturity of the chest wall
Diagnosis Arterial blood gases Chest radiograph
Air bronchogram Ground glass appearance Lung opacity
Treatment Excess oxygen can damage the pulmonary epithelium and the retina1) CPAP(continuous positive airway pressure)
Prevents collapse of unstable alveoli and allows high inspired O2 concentration to be reduced
2) SURFACTANT-prevents development of HMD Antenatal corticosteroids and surfactant dec death rate
3) Correction of acidosis and antibiotics GLUCOCORTICOIDS
Prevents chronic lung disease but not recommended due to limited benefits and adverse neuropsychological effects.
Complications1) Bronchopulmonary dysplasia-persistent hyperoxia
Cases seen before 30 wks (Baraldi and Filippone, 2007)2) Pulmonary hypertension3) Retinopathy of prematurity (Retrolental Fibroplasia)
Prevention ANTENATAL CORTICOSTEROIDS
Decreases respiratory distress and Intraventricular hemorrhage in infants born between 24-34 wks.
INTRAVENTRICULAR HEMORRHAGE Also called IVH, is bleeding into the ventricles of the brain Prematurity is the greatest cause of intraventricular hemorrhage, and most
cases of IVH occur in babies less than 30 weeks gestation or under 1,500 grams (3 lbs 5 oz).
Four categoriesI. Subdural Hemorrhage
Result of trauma Minimal neurologic abnormalities
II. Subarachnoid III. Intracerebellar IV. Periventricular-Intraventricular
Hemorrhage results from either asphyxia or trauma PERIVENTRICULAR-INTRAVENTRICULAR
Bleeding extends to the ventricular system and brain parenchyma Hemorrhages develops within 72 hrs after birth and large lesions can
result to hydrocephalus and periventricular leukomalacia INTRAVENTRICULAR HEMORRAGE
In preterm neonate pathogenesis is multifactorial which includes1) Hypoxic-ischemic events2) Anatomical factors3) Coagulopathy
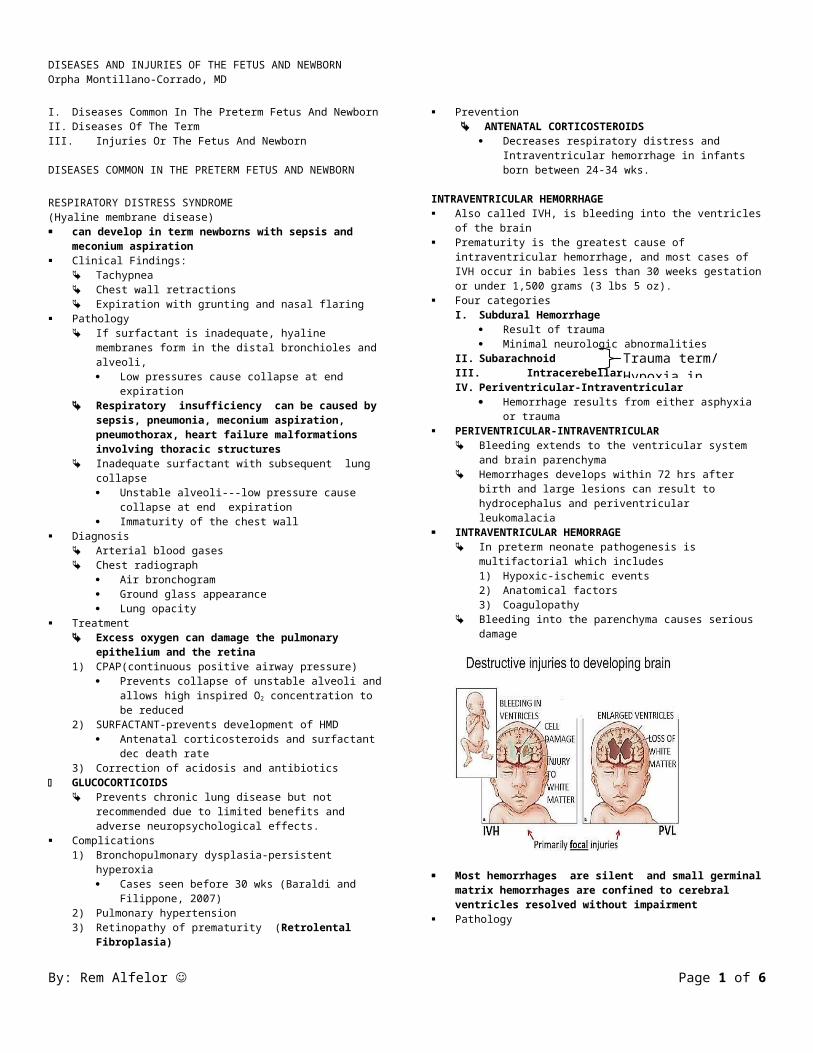
Bleeding into the parenchyma causes serious damage
Most hemorrhages are silent and small germinal matrix hemorrhages are confined to cerebral ventricles resolved without impairment
Pathology Damage to the germinal matrix capillary causing extravasation of bld into
the surrounding tissue. In preterm -fragile tissue due to:
1) Subependymal germinal matrix provides poor support2) Venous anatomy causes stasis and congestion3) Vascular autoregulation is impaired before 32 wks
Incidence Depends on the gestational age) Half of the neonates born before 34 wks will have some evidence of
hemorrhage (Hayden and associates 1985)
BRAIN DISORDERS 1) Neonatal Encephalopathy2) Cerebral Palsy Perinatal Asphyxia
Hypoxic-ischemic encephalopathy Characterized by clinical and laboratory evidence of acute or subacute
brain injury due to asphyxia. The primary causes of this condition are systemic hypoxemia and/or reduced cerebral blood flow
Diagnosis Guidelines from the American Academy of Pediatrics (AAP) and the
American College of Obstetrics and Gynecology (ACOG) for hypoxic-ischemic encephalopathy must be present for the designation of perinatal asphyxia severe enough to result in acute neurologic injury:
Profound metabolic or mixed acidemia (pH < 7) in an umbilical artery blood sample, if obtained
Persistence of an Apgar score of 0-3 for longer than 5 minutes Neonatal neurologic sequelae (eg, seizures, coma, hypotonia) Multiple
organ involvement (eg, kidney, lungs, liver, heart, intestines) Management
Following initial resuscitation and stabilization, treatment is largely supportive and should focus on the following1) Adequate ventilation2) Perfusion and blood pressure management -3) Careful fluid management4) Avoidance of hypoglycemia and hyperglycemia5) Hyperthermia management 6) Treatment of seizures
Hypothermia Therapy Extensive experimental data suggest that mild hypothermia (3-4°C
below baseline temperature) applied no later than 6 hours following injury is neuroprotective.
CEREBRAL PALSY Is an abnormality of motor function (as opposed to mental function) and postural
tone that are cerebral in origin acquired at an early age, even before birth. Signs and symptoms of cerebral palsy usually show in the first year of life.
The predominant symptoms and signs of cerebral palsy are related to motor difficulties ….such as developmental motor delay, gait disorders, poor fine and gross
motor coordination, swallowing disorders, or speech delay are all the result of the basic motor disorder
By: Rem Alfelor Page 1 of 4
Trauma term/Hypoxia in preterm
DISEASES AND INJURIES OF THE FETUS AND NEWBORNOrpha Montillano-Corrado, MD
This abnormality in the motor system is the result of brain lesions that are non-progressive.
One-time brain injury, that will not occur again. Classified by the type of neurological dysfunction
1) Spastic Cerebral Palsy Strong association\ with mental retardation and seizure disorder-
20% Result from interruption of blood supply prior to delivery
2) Dyskinetic Cerebral Palsy According to the predominant symptoms dyskinetic CP may be
either Dystonic or Choreoathetotic includes ataxic cerebral palsy
Usually has genetic in origin3) Hypotonic Cerebral Palsy
Based on limb distribution involvement1) Quadriplegia2) Diplegia
Common in preterm and low birthweight- 30%3) Hemiplegia- 30%4) Monoplegia
Prenatal causes-70% Metabolic (severe hypoglycemia), TORCH, brain malformation or infracts,
toxins, genetic syndromes, rhesus incompatibility Natal causes-10% Postnatal causes- 20%
Meningitis, Traumatic Brain Injury, Toxins
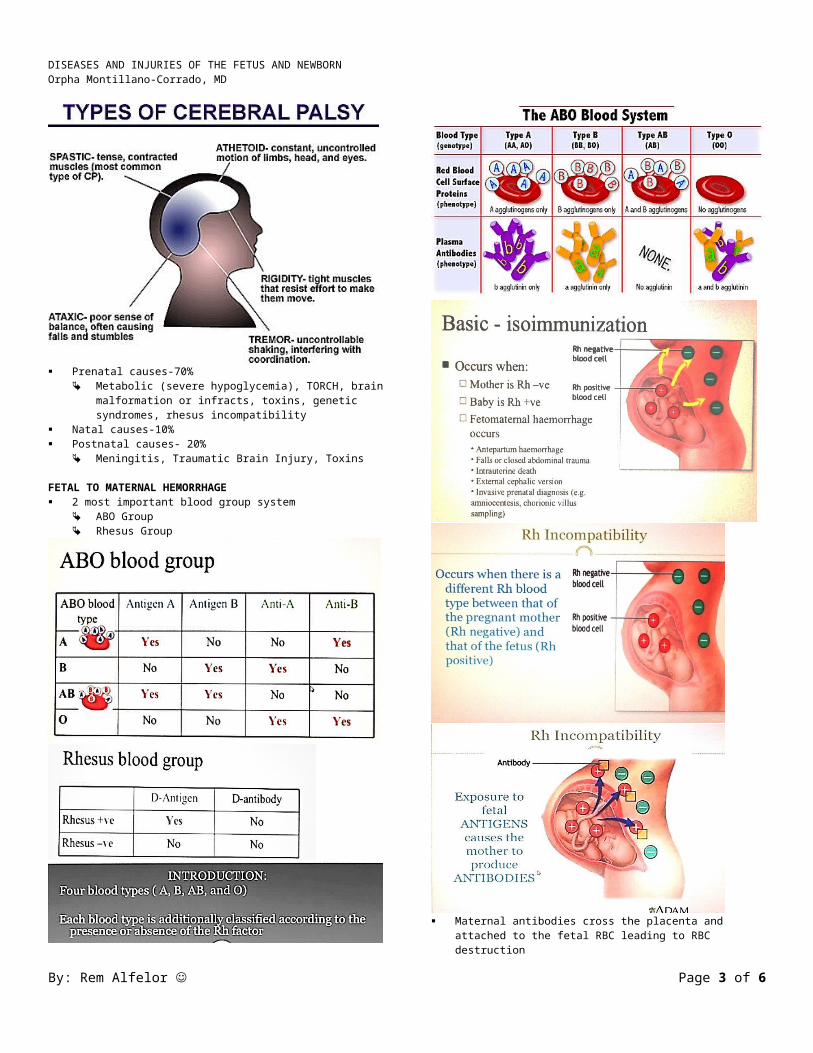
FETAL TO MATERNAL HEMORRHAGE 2 most important blood group system
ABO Group Rhesus Group
By: Rem Alfelor Page 2 of 4
DISEASES AND INJURIES OF THE FETUS AND NEWBORNOrpha Montillano-Corrado, MD
Maternal antibodies cross the placenta and attached to the fetal RBC leading to RBC destruction
Sequestration of macrophages in the fetal spleen (extravascular hemolysis) produces FETAL ANEMIA
If a mother has been sensitized before , there is a risk of the Rhesus + fetus developing hemolytic anemia and in severe cases HYDOPS FETALIS
HYDROPS FETALIS is an excess accumulation of fluid in the fetus Edema of fetus and placenta, ascites, pleural effusions and/or pericardial
effusions. Most cases of hydrops were caused by severe erythroblastosis fetalis secondary
to Rh isoimmunization
D-negative nonsensitized mother One dose of Anti-D immunoglobulin given at 28 wks Second dose given after delivery if the baby is D-positive.
ABO INCOMPATIBILITY Common cause of hemolytic dse of the newborn 20% of fetus has abo maternal bld gp incompatibility
1) ABO dse frequently seen in first born2) Most species of anti-A and anti-B are Immunoglobulin (IgM) which does
not cross the placenta, does not reach fetal erythrocytes3) Milder than D-isoimmunization , rarely results in anemia4) Can affect future pregnancy but rarely becomes progressively more
severe Treatment
Phototherapy Exchanged transfusion with o negative blood
Diseases Of The Term Fetus And NeonateI. RESPIRATORY DISTRESS SYNDROME
II. MECONIUM ASIII. PIRATION SYNDROMEHEMORRHAGIC DISEASE OF THE NEWBORNIV. FETAL DEATH
RESPIRATORY DISTRESS SYNDROME in term infants Sepsis, group B strep, intrauterine acquired pneumonia, pulmonary hpf,
meconium aspiration and pulmonary hemorrhage
MECONIUM ASPIRATION Peripartum inhalation of meconium stained fluid –chemical pneumonitis,
mechanical airway obstruction, hypoxia
HEMORRHAGIC DISEASE of the newborn Spontaneous internal and external bleeding beginning anytime after birth
By: Rem Alfelor Page 3 of 4

DISEASES AND INJURIES OF THE FETUS AND NEWBORNOrpha Montillano-Corrado, MD
Results from abn low vit k dependent clotting factors (V,VII, IX, X ,prothrombin , protein C and S
Early Bleeding 48 hrs after birth Develops in infant not treated with vit k
Late Bleeding 2- 12 wks after birth to infants exclusively breastfeeding
(breast milk has low levels of vit k) Other causes:
Hemophilia, congenital syphilis, sepsis, thrombocytopenia erythroblastosis and intracranial hemorhage
Prophylaxis Vit k 1mg IM at delivery Active bleeing vit k is given IV Oral adminitration is not effective
INJURIES OF THE FETUS AND NEWBORNI. Head injuriesII. Nerve InjuriesIII. Skeletal and muscle injuriesIV. Congenital injuries
HEAD INJURY1) INTRACRANIAL INJURY
Spontaneous Subarachnoid/subdural bleeding is the most common type (doesn’t
result from a traumatic delivery) Traumatic Treatment:
Minimal handling Management of ICP Thermoregulation, o2 and ventilatory support Vit k for coagulation defect
CAPUT SUCCEDANEUM Effusion overlies the periosteum and consist of edema fluid
CEPHAL HEMATOMA Lies under the periosteum and consist of blood
NERVE INJURYI. SPINAL INJURY
Excessive traction during delivery, fracture or dislocation of the vertebrae Seen usually in forceps or breech delivery
II. BRACHIAL PLEXOPATHYIII. FACIAL PARALYSIS
BRACHIAL PLEXOPATHY1) ERB-DUCHENNE PARALYSIS
Damage to the upper plexus Injury to the 5-6th cervical root Absent Moro on the affected side Paralysis of the deltoid, infraspinous muscle
2) KLUMPKE’S PARALYSIS Damage of the lower plexus Injury to the 7th and 8th thoracic root Loss of sensory and motor function to the hand and wrist
FACIAL PARALYSIS Pressure on the facial nerve (7t h nerve) as it emerges from the stylomastoid
foramen 20% associated with forceps delivery
CONGENITAL INJURIES Amnionic band syndrome- strip of band form a focal ring around an extremity or
digit producing constriction to cause damage
SKELETAL AND MUSCLE INJURIES Clavicular Fracture-common
Incidence is 3-18/ 1000 live births Humeral Fracture- uncommon Femoral Fracture
Rare Associated with breech delivery
Skull Fracture 75% instrumental delivery When head is deep in the pelvis
Sternocleidomastoid Muscle- injured (breech delivery)
By: Rem Alfelor Page 4 of 4





























