-
Disease-Specific Treatment of Relapse after Allogeneic
Transplantation
-
Treatment of Relapse
Cellular ImmunotherapyWithdrawal of immune suppressionDLI ( +
chemotherapy)Second allogeneic SCTNon-Cellular therapiesSupportive
careConventional chemotherapy or radiationNovel cytotoxic
agentsBiological agentsImmunotherapy approaches
-
Treatment of RelapseCellular therapyWithdraw ISSecond BMT with
same or different donorDLIActivated DLIManipulated DLICD8 depleted,
CD4 enriched, antigen-specific.Dose titrated DLINK cellsModified T
cells (CARs)Other therapiesConventional chemotherapy or
radiationAntibodiesCD20, CD33, CD30, CTLA-4, etcBispecific
antibodiesBiological therapyLenalidomide, thalidomide, bortezomib,
azacytadine, decitabine, mTor inhibitors,others.Interferon, IL-2,
etcVaccinesOthers
-
Available data for treatment of relapseCML-CP: DLI restores
durable CR in 80% of pts with CP relapse.Dose, schedule, toxicity
well defined.Role of TKIs?AML, ALL, NHL, HL, CLL, MM, CML-AP/BCDLI
response rate, most effective approach, and long term
outcomes?Second SCT ?Other therapies ?
An embarrassing lack of data
-
Excuses (good ones)
Patients are heterogeneousAgeImpact of prior transplant
Myeloablative vs RICGVHD prophylaxis (TCD, alemtuzumab, sirolimus,
etc)Different graftsBM vs PBSCTCD, other manipulationDonor source
and availability (sibling/family, URD, UCB, matched or
mismatched)Different risks, timing to intervention, treatment
choice, etcClinical complications and co-morbidities after
allogeneic SCTMay not tolerate therapies wellActive GVHD? Acute or
chronic?Use of immune suppression
-
Excuses (good ones)
Disease-related issues are heterogeneousTiming of relapse: early
vs late relapse may be very differentHistology (particularly in
NHL)Disease burden and pace of progressionIn indolent diseases
residual disease may not require interventionInfluence of prior
therapies and likely drug resistanceSmall numbers of patients
studied with some diseases.No central database or sample repository
to assess interventions.Reticence for clinical trials in this
population (sponsors, cooperative group, FDA, investigators.Limits
access to new compounds
-
Excuses (good ones)
Lack of insurance coverage for clinical trials (and in some
cases standard DLI or other therapy)Bias for:Treatment
selectionDepends on patient, disease activity, donor availability,
prior therapiesPatient selectionAge, co-morbidity, past and present
transplant-related complications.Reporting of outcomes
-
Many issues are common to treatment of relapse of multiple
diseases
-
Cell Dose
Is there a dose:response relationship?In CML, low dose DLI (1 x
10^7/kg) with dose escalation may preserve GVL with limited GVHD.Is
this effective for other indolent relapses (NHL, HL, MM, CLL?)Not
useful for rapidly progressive acute leukemiaIs there a
dose:toxicity relationship?Minimal threshold for GVHD may vary by
donor source (haplo vs well matched)Sibling vs unrelated donorOften
dosed differently but not supported by comparative trials
-
Role of Chimerism
Does mixed or changing chimerism signify relapse?For CML, mixed
chimerism predicts relapse. Role for intervention depends on
timing, pace of change, and other factorsSignificance in other
diseases less clearMay depend on the cellular compartment evaluated
(T, NK, myeloid)Role of intervention for chimerism and influence on
outcome not well defined for most diseases.Treatment of mixed
chimerism with DLI may prevent relapse in some cases, but not
others.
-
Role for Second SCT
Available data is limited and should be reassessed in the modern
era.Conventional vs RIC conditioning? Influence of disease type and
extent of relapse?Same vs alternate donor?Influence of timing of
relapse?Manipulations to enhance GVT activity of second SCT?
-
Overcoming Limitations
NCI Sponsored Workshop on Relapse after Allogeneic SCT! The
first stepDefine critical issues relating to relapse
therapy.Multicenter and international collaborations to rapidly
test and analyze new therapies for relapse.
-
Disease-Specific Treatment of Relapse after Allogeneic
TransplantationFred FalkenburgJoseph AntinMarcos de LimaEli
EsteyJohn LevineJacob RoweAlan WayneDavid MaloneyKoen van
BesienKarl PeggsDavid PorterJose LeisNancy HardyNicolaus KrgerEdwin
Alyea
CMLAMLALLNHLMMCLLHL
-
Treatment of CML relapse after allogeneic SCT
Fred Falkenburg
Joseph Antin
-
Treatment of relapsed Chronic Phase CML with DLI after
Allogeneic Hematopoietic Stem Cell Transplantation (SCT)Complete
remissions in 80-90 % of casesRelatively low doses of DLI
requiredTime interval between treatment and response is dose and
disease state dependentInterferon may potentiate onset and
effectTarget recognition may determine balance between GVHD and
GVL
-
Hematopoiesis-associated minor histocompatibility antigens
(mHag) and GVL reactivityIn HLA-identical transplantation donor T
cells recognizing hematopoiesis-specific antigens on recipient
cells eliminate normal and malignant hematopoietic cells of
recipient originGVL-reactivity(Complete) donor chimerism
Hematopoiesis-specific mHag may be targets for GVL reactivity
with limited induction of GVHD
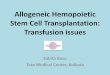
- BCR/ABL expression in bone marrow after
DLI0,000010,00010,0010,010,11SCT+12
SCT+28DLI+1.5+3+5+6+7+8+9+10+11+13+15+18+22+26weeks post
treatment
-
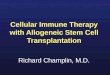
Kinetics of immune responses after DLIRZ
HA-2,-1, A2-HY tetramers DL (3)
Blad2
Blad3
HA-2,-1, A2-HY tetramers DL (2)
2.614.976615688214.9766156882SCT+12
3.715.113174061415.11317406147.5565870307
4.316.06295907668.0314795383DLI
3.48.174093264224.52227979278.1740932642
451.182477899534.12165193334.121651933
2.91175.558166150582.0156860105109
3.42508.7071945285195.4836774957+6
1.21719.56161510221264.964866282159
0.7200.9371146732150.7028360049+8
1.1167.2984397998182.5073888725+9
1.7130.3675129752223.487165100393.1196521251
2.351.0524213679272.279580629168.0698951573
2.4109.6664688427255.8884272997+13
3.397.1655939146267.205383265172.8741954359
3.525.6160214813128.080107406638.424032222
2.784.6076957696105.759619712+22
2.9109.355989352327.3389973381136.6949866903
WBC x10E6/ml
CD8+/HA-2+ /ml
CD8+/HA-1+ /ml
CD8+/HY-A2+ /ml
weeks post treatment
CD8+/tetramer+ cells
WBC
data f-up roozeboom
datum8/27/9810/8/984/27/997/30/9912/14/9912/23/991/6/001/20/001/27/002/3/002/10/002/17/002/24/003/2/003/16/003/30/004/20/005/18/006/15/00
donorpat
SCT+12SCT+28DLI+1.5+3+5+6+7+8+9+10+11+13+15+18+22+26
Hbmmol/l7.76.76.67.77.17.36.76.455.66.565.95.8777.77
Trombox10E9/l6761681572943032702314014082942125210181163162156135
WBCx10E67.28.72.63.74.33.44.02.93.41.20.71.11.72.32.43.33.52.72.9
% lymfo%30322822101214192850975755382925262936
abs
lymfox10E3/ml216027847288144304085605519526006796279358746968259107831044
%
CD3+CD8+%23.099.4316.688.1616.0216.2423.0936.8526.0231.412016.4814.215.619.4725.1612.5824.0123.61
%
CD45+CD14-%93.9165.0781.0887.985.7781.0675.7974.2776.0395.3581.167.9471.2980.1274.1485.4589.3888.8890.16
abs #
CD3+CD8+x10E3/ml531403150768082171273326198167152186170183243128212273
%
HA-2+%000.010.020.020.010.030.430.770.870.120.110.070.030.060.040.020.040.04
CD8+/HA-2+0015151685111762509172020116713051110972685109
%
HA-1+%000.010.020.010.030.020.030.060.640.090.120.120.160.140.110.10.050.01
CD8+/HA-1+0015158253482195126515118322327225626712810627
% HY-A2+%0.010.010.010.010.020.040.030.050.040.030.030.05
CD8+/HY-A2+534088341095993687338137
chimerisme MNC
patient47080twm95
chimerisme Leuco
patient95
BCR/ABL VB8.00E-049.90E-013.40E-01negnegnegnd
BCR/ABL BM1.20E-037.90E-022.30E-01dub posdub posnegneg
morfologieCML+hypoplasieCML--ntb
CML--
HA-2,-1, A2-HY tetramers DL (3)
2.614.976615688214.9766156882SCT+12
3.715.113174061415.11317406147.5565870307
4.316.06295907668.0314795383DLI
3.48.174093264224.52227979278.1740932642
451.182477899534.12165193334.121651933
2.91175.558166150582.0156860105109
3.42508.7071945285195.4836774957+6
1.21719.56161510221264.964866282159
0.7200.9371146732150.7028360049+8
1.1167.2984397998182.5073888725+9
1.7130.3675129752223.487165100393.1196521251
2.351.0524213679272.279580629168.0698951573
2.4109.6664688427255.8884272997+13
3.397.1655939146267.205383265172.8741954359
3.525.6160214813128.080107406638.424032222
2.784.6076957696105.759619712+22
2.9109.355989352327.3389973381136.6949866903
WBC x10E6
CD8+/HA-2+
CD8+/HA-1+
CD8+/HY-A2+
weeks post treatment
CD8+/tetramer+ cells
WBC
Blad2
Blad3
HA-2,-1, A2-HY tetramers DL (2)
2.614.976615688214.9766156882
3.715.113174061415.1131740614
4.316.06295907668.0314795383
3.48.174093264224.5222797927
451.182477899534.121651933
2.91175.558166150582.0156860105
3.42508.7071945285195.4836774957
1.21719.56161510221264.9648662821
0.7200.9371146732150.7028360049
1.1167.2984397998182.5073888725
1.7130.3675129752223.4871651003
2.351.0524213679272.2795806291
2.4109.6664688427255.8884272997
3.397.1655939146267.2053832651
3.525.6160214813128.0801074066
2.784.6076957696105.759619712
2.9109.355989352327.3389973381
WBC x10E6
CD8+/HA-2+
CD8+/HA-1+
weeks post treatment
CD8+/tetramer+ cells/mL
WBC/mL
bcrabl PBGD ratio rozeboom
-3.096110013-2.919618754
-3.1116106997-1.5199135645
-0.0043648054-1.0233729087
+1.5+1.5
+3+3
-0.468521083-0.408272164
+6+6
+7+7
+8+8
-5.5-5.4
+10+10
+11+11
-5.5-5.4
+15+15
-5.5-5.4
-5.5-5.4
-5.5-5.4
BCR/ABL PB
BCR/ABL BM
weeks after DLI
bcr-abl/PBGD ratio
data f-up roozeboom
datum8/27/9810/8/984/27/997/30/9912/14/9912/23/991/6/001/20/001/27/002/3/002/10/002/17/002/24/003/2/003/16/003/30/004/20/005/18/006/15/00
donorpat
SCT+12SCT+28DLI+1.5+3+5+6+7+8+9+10+11+13+15+18+22+26
Hbmmol/l7.76.76.67.77.17.36.76.455.66.565.95.8777.77
Trombox10E9/l6761681572943032702314014082942125210181163162156135
WBCx10E67.28.72.63.74.33.44.02.93.41.20.71.11.72.32.43.33.52.72.9
% lymfo%30322822101214192850975755382925262936
abs
lymfox10E3/ml216027847288144304085605519526006796279358746968259107831044
%
CD3+CD8+%23.099.4316.688.1616.0216.2423.0936.8526.0231.412016.4814.215.619.4725.1612.5824.0123.61
%
CD45+CD14-%93.9165.0781.0887.985.7781.0675.7974.2776.0395.3581.167.9471.2980.1274.1485.4589.3888.8890.16
abs #
CD3+CD8+x10E3/ml531403150768082171273326198167152186170183243128212273
%
HA-2+%000.010.020.020.010.030.430.770.870.120.110.070.030.060.040.020.040.04
CD8+/HA-2+0015151685111762509172020116713051110972685109
%
HA-1+%000.010.020.010.030.020.030.060.640.090.120.120.160.140.110.10.050.01
CD8+/HA-1+0015158253482195126515118322327225626712810627
% HY-A2+%0.010.010.010.010.020.040.030.050.040.030.030.05
CD8+/HY-A2+534088341095993687338137
chimerisme MNC
patient47080twm95
chimerisme Leuco
patient95
BCR/ABL PB0.00080.0007720.990.34negnegnegnd
-3.096110013-3.1116106997-0.0043648054-0.468521083-5.5-5.5-5.5-5.5-5.5
BCR/ABL BM0.00120.02830.0790.23dub posdub posnegneg
-2.919618754-1.5199135645-1.0233729087-0.408272164-5.4-5.4-5.4-5.4-5.4
morfologieCML+hypoplasieCML--ntb
CML--
-
Treatment of relapsed Chronic Phase CML with DLI after
Allogeneic Hematopoietic Stem Cell Transplantation (SCT)Which
antigens need to be targeted to provoke a GVL response without
GVHDTargeting hematopoiesis restricted antigens results in specific
GVL?Are over-expressed self antigens targets of high avidity T cell
responses?
-
Persistance of BCR/ABL despite repeated DLICML chronic phase,
allogeneic SCT from HLA identical brother
Hematological relapse: DLI 3x10E7 T cells/kg: hematological
remission, molecular persistence
Molecular persistence of disease despite escalating doses of
DLI:
Localized myeloid blast crise in epidural space: Systemic
chemotherapy Radiotherapy + DLI 1.5x10E8 T cells/kg,
-
Persistance of BCR/ABL despite repeated DLI isolation of CML
reactive CTL clones
-
Non-maturated immature CD34 CML cells
-
Maturated CML cells after culture with cytokines: myelocytes,
metamyelocytes, monocytes and granulocytes
-
Maturated CML cells incubated with T cell clones for 50
hoursHA-1no T-cellsC6-1
-
no T-cellsC6-1HA-1immature CML cells incubated with T cell
clones for 50 hours
-
ConclusionsCD8+ mHag specific CTL recognizing only maturation
associated antigens not present on CD34 positive stem or early
progenitor cells may result in persistence of disease
Should CML stem cells be targeted?
-
Cellular immunotherapy and TKIAre leukemic stem cells residing
after imatinib treatment susceptible targets for cellular
immunotherapeutic interventions?Should allo-SCT performed for
persistent CML be combined with continuous treatment with tyrosine
kinase inhibitors?
-
Quantitative flow cytometric analysis of phenotype and
proliferative status of CML precursor cells Isolation of CD34+ CML
precursor cells from PB or BM by MACS Cytokines: GM-CSF, G-CSF,
IL-3, SCF, EPO CFSE/PKH labeling of the target cell population Ab
labeling of specific cell populations (FITC, PE & APC)
Exclusion of death cells using propidium iodide Addition and
acquisition of a fixed amount of fluorescent
beads1032CFSECD34CFSEcounts
-
Specific kill of proliferating CML precursor cells by
ImatinibCFSECD346 dayscontrol100 mM imatinib
-
CFSE6 days pretreated48 hours CTL exposure (HLA-A2 restricted
mHag-specific CD8+ clone; E/T 3/1)control+ mHag spec.
CTLCross-resistance of Imatinib pre-treated CML precursor cells to
cell death induced by cytotoxic T cells100mM Imatinib
-
CFSECD346 days CTL exposure (HLA-A2 restricted mHag-specific
CD8+ clone; E/T 3/1)control+ mHag spec. CTLQuiescent CML precursor
cells are resistant to cell death induced by cytotoxic T cellsno
pre-treatment
-
ConclusionsQuiescent leukemic stem cells are protected from the
cytotoxic effect of tyrosine kinase inhibitors This population of
quiescent leukemic stem cells shows cross-resistance to cytotoxic T
cells involved in the GVL effect after allo-SCT, The
anti-proliferative effect of tyrosine kinase inhibitors on both the
leukemic cells and the T cells may potentially hamper the
potentially curative immune response after allo-SCTIf cellular
immunotherapy is combined with TKI, should treatment be
intermittent?
-
Treatment of relapsed CML after Allogeneic Hematopoietic Stem
Cell Transplantation (SCT)Identification of target cells and/or
antigens to be targetedSeparation of DLI into fractions (CD4 T
cells) Targeting minor histocompatiblity antigens or leukemia
associated antigens by adoptive transfer if purified T cells
Vaccination of patient with mHag, APC.Vaccination of donor with
mHagInterferon may potentiate onset and effectAre TKI useful, or
harmful?How to treat extramedullary relapses
-
Treatment of relapsed acute myelogenous leukemia after
allogeneic stem cell transplantationMarcos de Lima, MDM. D Anderson
Cancer Center
John Levine, MDUniversity of Michigan
Elihu Estey, MDFred Hutchinson Cancer Research Center
-
AML
Probability of relapse: 20% - 60% - definition of relapse is
key.
All results reflect (to a great extent) patient selection.
Major co-variates predicting relapse:- disease stage /
cytogenetics- preparative regimen intensity Ringdn et al. J Clin
Oncol; 27; 2009: 4570-4577 Trends affecting comparison with
historic data:- better prognostication for diploid patients (FLT3,
NPM)- treatment of older patients- use of reduced-intensity
regimens
Oran et al. Leukemia (2007) 21, 25402544. Eapen et al. BMT
2004;34:721-727
-
Donor Lymphocyte Infusions
Addition of chemotherapy improves response rate but not
long-term disease control.
GVHD in 10-60% of patients
Marrow aplasia in 5-20%.
TRM: 0-50%
Most series : adults, using mostly related donors.
Responses frequently do not translate into long-term survival,
due to GVHD, pancytopenia, infections, and disease relapse.
Donor availability and presence of GVHD are major
impediments.
-
Donor lymphocyte infusion alone Kolb H. Blood 1995;86:2041-2050
Loren A, Porter DL. Bone Marrow Transplantation (2008) 41,
483493.Porter DL et al. Blood 2000;95:1214-1221.
Investigatorn Outcomes Collins et al. 46
6/39 (15%) CR
Kolb et al. 195/17 (29%) CRShiobara et al. 21
8/21 (38%) Response7% DFS at 2 years
-
D L I and chemotherapy Porter DL. Leukemia
2003;17:1035-1037.Levine J. Bone Marrow Transplant 2008;42:201-205.
Choi S. Leukemia 2004;18:1789-1797.
Investigator (n) Outcomes Collins et al. 7 4/7 (57%) DFS
Kolb et al.
8
4/8 (50%) CR 2/4 (50%) DFS at 2 years
Choi et al.
16
10/16 (63%) CR 31% DFS at 2 years
Levine et al. 65 27/57 (47%) CR 19% DFS at 2 years
-
Schmid, C. et al. J Clin Oncol; 25:4938-4945 2007Donor
lymphocyte infusionEBMT analysis
399 patients with AML in first hematological relapse after
HSCT
DLI = n=171 versus no DLI (n = 228)
Median follow-up was 27 and 40 months
-
Schmid, C. et al. J Clin Oncol; 25:4938-4945 2007Fig 1.
Unadjusted survival of patients with first hematological relapse of
acute myeloid leukemia after allogeneic hematopoietic stem-cell
transplantation (HSCT)Multivariate analysis
1- age < 37 years (P = .008)
2- longer CR after HSCT (> 5 months; (P < .0001)
3- use of DLI (P = .04).
-
Risk Factors for Survival Among Patients Receiving DLI for
Treatment of Hematological Relapse After HSCT for AML (n = 171)
Schmid, C. et al. J Clin Oncol; 25:4938-4945 2007
VariablePRelative Risk 95% CI
% blast at relapse (BM), > 35%.0060.560.38 to 0.85Female v
male.021.61.07 to 2.4Cytogenetics (favorable v other).0045.61.76 to
1.8remission versus no remission< .00015.82.5 to 13.7
-
Second transplant
-
6% of patients with recurrent leukemia receive a 2nd HSCT Eapen
et al. Bone Marrow Transplant 2004;34:721-727Second transplants
matched related donor CIBMTR analysis
AML125ALL 72CML 82
Age (years) 1040 (14)112056 (20)213064 (23)>30119 (43)
Same donor as 1st transplant238 85%
Follow-up of survivors, median93 mo.
-
Eapen et al. Bone Marrow Transplant 2004;34:721-727RIC was
associated with more relapses.Second transplants matched related
donor CIBMTR analysis
Overall mortality
Age at 2nd HSCT (years) 20961.00>201831.94 (1.422.64)62131.00
6523.47 (2.494.83)
-
Disease status at second transplant:
Refractory relapse 39%Untested relapse 56%CR 5% 847 patients
with AML, MDS, or myeloid blast crisis of CML received transplants
between May 1989 and November 2003 at MDACC.
346 patients relapsed (41%).
72 of 346 (21%) underwent a 2nd HSCT from the same or different
donor for AML. Disease burden may identify patients more likely to
benefit from secondallogeneic hematopoietic stem cell
transplantation to treat relapsed acute myelogenous leukemiaC
Hosing et al. BMT (2005) 36, 157162no circulating blasts / 5% bone
marrow blasts
-
Oran et al. Leukemia (2007) 21, 25402544.
-
Oran et al. Leukemia (2007) 21, 25402544;
-
Salvage chemotherapy
-
Chemotherapy
Response rates are a function of : - chemosensitivity -
remission duration - tempo (and disease bulk?) of relapse
No evidence that any particular regimen is superior to any
other.
FHCRC data (years 1977-1984)
95 patients relapsed - 55 received chemotherapyResponse rates:
CR rate with cytarabine (+/- adriamycin): 32% of 34 patients median
DFS of 9.7 months.
-
FHCRC data (years 1995-2004)
N=220
received chemotherapy +/- immunosuppression withdrawal
Time to relapse 2-year survival estimates
100 days 3% 100-200 days 9% > 200 days 19%
Mielcarek M et al. Biol Blood Marrow Transplant
2007;13:1160-1168.Mortimer J et al. J Clin Oncol 1989;7:50-57.
-
Novel agents
A variety of targeted agents are under investigation role
unclear in this setting.
sorafenib FLT3 positive patients Metzelder S et al. Blood
2009;113:6567-6571.
5-azacitidine. Jabbour et al. Cancer, 2009;115:1899-1905 Lubbert
et al. Bone Marrow Transplant 2009
-
Unanswered questions
Potentially answerable with a large database:
1- Better definition of subgroups more likely to benefit from
interventions (versus palliative care only).
2- DLI after alternative donor transplants.
3 Salvage therapy for children.
-
Unanswered questions
Potentially answerable with innovative, multicenter clinical
trials:
- how to incorporate newer drugs and/or cell therapy approaches
AND prove that they work.
-
Conclusions
Current therapies benefit a small minority of patients.
This is clearly a phase I scenario.
-
Key obstacles for development of large, randomized, prospective
clinical studies
Lack of large, multicenter prospective phase I and II studies to
define experimental arms in a randomized study. Lack of large
databases dealing specifically with relapse information.Lack of a
broad discussion and consensus that should ideally involve drug
companies and the FDA on the need to enroll patients in phase I, II
or III clinical trials for the treatment of AML relapsing after
allogeneic HSCT.
-
Proposed initiatives Creation of a sample repository.
Development (or improvement of current available databases) of
systems for detailed data collection in the relapse setting.
Multicenter approach!
Identification of target antigens, modification of DLI,
targeting antigens by adoptive transfer, vaccines etc
NK cells
Maintenance therapy : azacitidine, decitabine, sorafenib etc
-
Treatment of ALL that has relapsed after allogeneic
TransplantationAlan S Wayne and Jacob M. Rowe
-
Relapsed ALL Early diagnosis is probably crucial Conventional
and investigational therapies likely to be greater if intervention
is prior to florid relapse
-
INTRODUCTIONRelapsed ALL has a very poor prognosis In adults
only 7% survive 5 years
Relapse post allogeneic transplant, almost always
incurable0123450255075100PERCENT 7% N= 609 Fielding AK et al,
Blood, 2007
-
Relapsed ALL Post Allogeneic HSCT
While cures are rare, INDUCTION OF REMISSION
and / or PROLONGATION OF RESPONSE is an
important endpoint
-
ALL: Therapy at Relapse post Allo HSCTCURATIVE INTENT SUPPORTIVE
CARE ONLYMINORITY THERAPEUTIC INTENT MINORITY REMISSION
NON-MYELOABLATIVE INDUCTION MAINTENANCECONSOLIDATION /
MAINTENANCE
ALLO SCT
-
Graft versus Leukemia (GvL) in ALLFirst clinical description of
GvL in humans was in ALL !Weiden PL et al, NEJM 300: 1068,
1979DiseaseFreeSurvival(%)Syngeneicn=46YearsAllogeneic GVHD 0-I
n=117Allogeneic,GVHD II - IVn=79
-
Potent GvL in ALL in CR1 Goldstone AH, et al, Blood, 2008
-
Graft versus Leukemia (GvL) in ALL REDUCED-INTENSITY
CONDITIONING FOR HIGH-RISK ALLCIBMTR STUDY OF ALL IN CR1 OR CR2
RIC (n= 92) vs myeloablative (n= 1421)Median Age, yrs,45 28 p=
< .0001 OS @ 3 yrs, %38 43 p= .39 TRM @ 3 yrs, %32 33 p=
.86Marks, DI et al, ASH 2009
-
Graft versus Leukemia (GvL) in Relapsed ALLDonor Lymphocyte
Infusions (DLI)Rarely effective in florid relapseRapid
proliferative rate of ALL at relapseLow expression T cell
co-stimulatory molecules Porter DL et al, Blood, 2000CR following
matched sibling DLI in ALL only 10-20% in select patients Possibly
better outcome in unrelated DLI , but data based on very small
numbers.Probability (%)Weeks after complete
remissionCMLn=12ALLn=5AMLn=10Disease Free Survival, if CR after
unrelated DLI
-
Suggested Treatment of Relapsed ALL post TransplantUNFIT FOR
INTENSIVE THERAPY FIT FOR INTENSIVE THERAPY CONSERVATIVE CARE NO
RESPONSE BEST AVAILABLE REGIMEN TO ACHIEVE CR ORNON-MYELOABLATIVE
VERY GOOD (STABLE) PR (e.g., TKI) VCR + PREDNISONEMONOCLONAL
ANTIBODIESNO PRIOR GVHD PRIOR GVHD GRADE I DLI SECOND ALLOGENEIC
TRANSPLANT +/- SECOND ALLOGENEIC TRANSPLANT* Consider clinical
trial**
-
Investigational ApproachesPH-POSITIVE PH-NEGATIVE NOVEL
CHEMOTHERAPY MONOCLONAL ANTIBODIESand TARGETED AGENTS +/-
CHEMOTHERAPY NOVEL TKIsUNCONJUGATED CONJUGATED
CD 20 GEMTUZUMAB OZOGAMICIN CD 22 (Anti CD33) CD 52 ANTI-CD22
IMMUNOTOXIN (CD 19)
Anti Flt3 (B-lineage) I131 -LABELLED ANTI- CD45 Bi-specific
DENILEUKIN DIFTITOX (IL-2)NELARABINE CLOFARABINE LIPOSOMAL
VINCRISTINEGAMMA SECRETASE INHIBITORS
-
55 kD recombinant single chain variable fragments
(scFv)Anti-CD19 Fv (HD37)Anti-CD3 Fv (L2K-07)Gly/Ser
linkerAnti-CD19 Bi-Specific T-Cell Engager (BiTE) MEDI-538, MT103,
BlinatumomabFv: variable fragment; VH: variable heavy-chain; VL:
variable light-chain; sc: single chain
-
Courtesy of Rupert Handgretinger, October 2009Clearance of
marrow blastsIncrease in CD8 T+ cellsCD19 BiTE for Relapse after
SCT Active against childhood ALLClearance of MRDCD19 BiTE
-
Future Directions - Cancer Vaccines I Attractive conceptually in
this patient population due to low toxicity Efficacy more likely in
states of minimal residual disease More data in AML, but similar
rationale may be applicable in ALL
-
Future Directions - Cancer Vaccines I I PEPTIDE VACCINES SOME
DATA IN AML USING WT1 PEPTIDE. MINIMAL
TOXICITYplateletsblastsBlasts, % Mailander V, Leukemia, 2004
MonthsPlatelets (/nl)VaccinationChemo-therapyWTI/PBGD
-
Future Directions - Cancer Vaccines III
PR1, a leukemia-associated antigen, studied for vaccination in
AML, with some success [HESLOP HE, STVENSON FK AND MOLLDDREM JJ,
HEMATOLOGY, ASH EDUCATION 2003] Dendritic cells and antigen
presenting cells utilized to improve the immune response to tumor
associated antigen in multiple myeloma [AVIGAN D ET AL, ASH 2008
AND 2009] Rationale applicable to other malignancies including
ALL
SUHOSKI MM , MOL THER, 2007
-
Disease-Specific Interventions for Relapse of non-Hodgkin
Lymphoma After Allogeneic Transplantation
David Maloney MD, PhDKoen van Besien, MD
-
NHL Relapse Following Allogeneic HCT: A Wide Range of Issues to
ConsiderMany different histologic subtypes of NHLindolent to
aggressive behaviorPatients often treated with Allogeneic HCT as
last resortafter failed high-dose therapy and autologous HCTwith
chemotherapy refractory diseaseTransplanted with a variety of
conditioning intensitiesmyeloablative, reduced intensity,
nonmyeloablativeT depleted or T replete graftsHLA matched or
mismatched, related, unrelated, cord blood or haploidentical stem
cell sources
-
Factors that Influence the Outcome of NHL Relapse post
Allogeneic HCTHistologyPresence or absence of GHVDT-replete vs
T-depleted graftsDisease status at HCT (chemorefractory vs
sensitive)Transplant conditioning intensityTiming of relapse (early
vs late)
-
Approach to the Treatment of NHLRelapse post Allogeneic HCTIn
the absence of GHVDWithdrawal of immunosuppression (IS)Donor
Lymphocyte Infusions (DLI)Monoclonal antibody therapyChemotherapy
+/- DLIRadiotherapy +/- DLIImmune stimulants (IL-2 etc)Second
allogeneic HCT
-
Specific Therapies: Withdrawal of ImmunosuppressionNo
prospective trialsSeveral reported successes
StudyCond for HCTnHistologyChem/XRTCR/PRResponsevan Besien
1997Ablative9DL (4)LBL(2)FL(2)PL (1)?33 CR2+-22+ moBishop
2008RIC13DL063 long CR42+-63+ mo
-
Specific Therapies: Donor Lymphocyte Infusions (DLI)An option in
the absence of GVHDMore commonly reported following T-depleted
HCTResponse often correlated with disease histology and pace of
progressionSome risk of subsequent GVHDA wide range of CD3 cell
doses used
-
Specific Therapies: Donor Lymphocyte Infusions (DLI)Usually
reported in context of larger transplant trials
StudyCond for HCTnHistologyChem/XRTCR/PRResponseRussell
2005T-dep (15)T-replete (2)17DL (5),MCL(4)FL(4),CLL (4)911PFS 3 y
52%OS 3 y 58%Bloor 2008T-dep (16)17CLL (3),MCL (3)FL (6),DL
(5)81310 in remission f/u 26 moBishop 2008RIC5DL (5)433 CR
74+-83+movan Besien 1997ablative3DL (2), PL (1)0Marks 2002T-dep15FL
(15)87 CR 16+-40+ moMandigers 2003T-dep7FL (5), SL (2)464 CR
43+-89+ mo
-
Specific Therapies: Chemotherapy +/- DLIAnecdotal reports of
chemotherapy +/- DLI generally within clinical trial
resultsOccasionally successfulSupport the concept of ongoing
graft-vs-tumor effects that may be capable of controlling minimal
residual diseaseNo clear choice of agentsConcern of ablating graft
appears low, but needs to be studied
-
Specific Therapies: Monoclonal Antibody TherapyFrequently
utilized for B cell NHLLow hematologic toxicityMay promote antigen
priming and graft-vs-tumor effectsTumor cell lines exposed to
rituximab were more effective at alloantigen presentation (Selenko
2002) Clinical trials from MD Anderson suggest improved outcome
following the addition of high-dose rituximab (FL and
CLL)Reasonable option for most patients
-
Specific Therapies: Other Immune Modulatory AgentsInterleukin-2
(Kiss 2003)CR in low grade NHL pt (flare GVHD)Interferon alpha
(Kawano 2004)CR in DLBCL with IFN + DLIThalidomide (Tueger 2006)1
pt with DLBCL and CRCTLA-4 blockade with ipilimumab (Bashey 2009)3
pts with HD or MCL had response
-
Impact of Early vs Late NHL Relapse Post Allogeneic HCTKenkre et
al, U Chicago8/23 durable remissions4 LGL, 1 MCL, 1 HL, 2 DLB6
Chemo, 2 DLI
-
Specific Interventions: Indolent NHL (FL)MD Anderson (Khouri
2008)Flu/Cy/Rituximab N=47All achieved CR, 2 relapses treated with
rituximab +/- DLI to CROS 85% at 5 yearsSeattle flu(2 Gy TBI) n=46
indolent (Rezvani 2008)Relapse rate indolent 14%, 2 treated with
IS/rituximab +/- DLIUK (alemtuzumab containing) n=41 (Morris
2004)Relapse at 3 years 44%6/10 responded to DLI leading to 65%
current PFS at 3 yearsUK (BEAM-alemtuzumab) n=44 (Ingram
2008)Relapse rate of 20%4/6 treated with DLI had CR
-
Specific Interventions: Indolent NHLGenerally very sensitive to
graft-vs-NHL effects with low relapse rate following T replete
HCTPrototype follicular NHLSensitive to IS withdrawalMonoclonal
antibody therapy (rituximab)DLIIn the absence of GVHD generally
start with above, then consider chemotherapy +/- aboveLong term
survival possible post relapse
-
Specific Interventions: Aggressive NHLSeattle flu(2Gy TBI)
(Rezvani 2008)DLBCL n=32, 41% disease progression1 DLI x 3 no
effect1 IS withdrawal- no effect1 second myeloablative HCT died
TRM1 successful IS withdrawal-rituximab-XRT (alive in CR 54+ mo)1
successful second RIC (same donor) (alive CR 34+ mo)1 response IS
withdrawal/ DLIUK flu-mel-alemtuzumab (Thomson 2009)DLBCL or
transformed (n=48)15/48 (33%) relapsed5/12 CR to DLI +/-
chemotherapy
-
Specific Interventions: Aggressive NHLFrench Registry (Sirvent
2009)DLBCL n=68Relapse at 4 years 41%20/26 relapses died of
disease5 in CR after chemo +/- XRT +/- DLIVancouver, BC (Doocey
2005)Myeloablative conditioning for DLBCL n=4413 progressed (32%)3
received DLI, all 13 died of diseaseNCI (Bishop 2008)N=15 with
aggressive NHL with relapse/ persistent disease post HCT6/11
treated with IS withdrawal or DLI responded3 / 4 treated with
Chemotherapy/ DLI responded6 remain in long term CR
-
Specific Interventions: Aggressive NHLGenerally a kinetic
problem post allogeneic HCTRequires disease control prior to
HCTEarly relapse difficult to manageLimited success withIS
withdrawal, DLI and antibody therapyLong term benefit
anecdotalAggressive chemotherapy +/- DLIXRT +/- DLIWorth
considering if disease is sensitive
-
Specific Interventions: Mantle-cell NHLMD AndersonMyeloablative
1/16 relapsed (Khouri 1999)RIC 3/18 relapsed (1/3 responded DLI)
(Khouri 2003)RIC n=35, (Tam 2009)6 year OS 53%, PFS 46% (3 pts
rituximab + DLI)Seattle (Maris 2004)Flu(2Gy TBI), n=33Relapse rate
9%, none after 6 monthsEBMT n=22 ( Robinson 2002)Progression at 2
years = 100%, ~50% overall group had T depletionUK (Morris,
2004)Alemtuzumab containing RIC (n=10 mcl)At 3 years 50% relapse
(1/2 responded to DLI)
-
Specific Interventions: Mantle-cell NHLSurprisingly sensitive to
allogeneic GVT activityLate relapses rare following T-replete
transplantsHigher relapse rate following T cell depletionRequiring
DLI or T cell add back Similar to indolent NHL for response to IS
withdrawalDLIchemotherapy +/- DLIRelapsing patients have chance of
long-term DFS with RX
-
Future: ConclusionsNHL often sensitive to GVT activityPost
transplant modulation is promisingDLIImmune modulatory
agentsAchieving a remission may allow re-establishment of GVT
effectsChemotherapy or other +/- DLIUltimately therapy should
invoke specific GVT immune responses without GVHD Registry studies
may be a first step toward prospective studies in specific
disease/risk categories.Prospective investigation of existing
strategies in favorable groupsRadically novel approaches in
unfavorable groups (i.e. aggressive histology/early relapse)
-
Salvage Options: Hodgkin Lymphoma
Dr Karl PeggsUniversity College LondonDr David PorterUniversity
of Pennsylvania Medical Center
-
Reduced toxicity transplantation = increased relapsing
population
Historically NRM prohibitiveRelatively few transplants
performedRelatively few patients lived long enough to
relapseExperience in salvaging relapsing patients limitedRIC/NST
increased allo-HSCT for HLrelapse is the commonest cause of
treatment failure44-81% at 2-3 years
-
Salvage chemotherapy
Most series demonstrate relapse risk higher in those with
refractory disease at transplantMost have received multiple lines
of salvage pre-transplant so limited options to explore agents to
which patients are naveNo published series appear prescriptive re
salvage; often the precise regimens used are not describedRegimens
including IVE, ESHAP, mini-BEAM, irradiation, gemcitibine have been
used in small numbers, often differing within series
-
Salvage chemotherapy
Response rates likely reflect disease-related features e.g.
chemosensitivity at transplant, time to relapse, tempo of relapseNo
evidence that any particular regimen islikely to affect a cure
superior to any otherAnecdotal reports suggest that occasional
patients achieve durable responsesMost relapses occur early - the
role of 2nd transplants has not been explored
-
Novel agents
Monoclonal antibodies (mAb) are of interest (might augment
DLI)anti-CD20: CD20+ nodular lymphocyte predominantrelatively few
of these cases are transplanted due to the rarity of NLP HL and
high cure rates with conventional
approachesanti-CD25:anti-CD30:both may be more effective if used as
vectors for delivery of radio-conjugates or cytotoxics (monomethyl
auristatin E)Immunostimulatory mAb:anti-CTLA-4, anti-PD1, anti-PDL1
(antagonistic)anti-4-1BB, anti-OX40 (agonistic)
-
Donor Lymphocyte Infusions
Overall response rates in the region 35-55% (30/71 = 42%) A
minority have durable responses (7/24 = 29%) Durable responses more
frequent following T cell depleted HSCT?
-
Donor Lymphocyte Infusions
n = 22 progression/relapse (7 post salvage) (17 UCLH, 5 RFH -10
previously reported)10 CR, 5 PR (20 evaluable, RR 75%) Response
associated with GvHD9/10 CR, 4/5 PR5 grade III-IV, 4 extensive
chronicCurrent status:6/10 maintain CR (median 4.8 yrs from DLI)3
died in CR (GvHD-related)1 progressed (2.3 yrs)2/5 PR progressed3
yr OS from relapse 62% and PFS 52% Peggs et al. ASH 2009;200
-
Unanswered questions
Largely overlap with those raised for other diseases:Nature of
the target antigensEBV antigens?Biomarkers of responsiveness:
histology, immune profilingRole of dose escalation, optimal
dosingRole of manipulated DLI e.g. CD8-depleted DLI, LMP-specific T
cells, ex-vivo activationPossible efficacy of genetically
re-targeted T cellsCAR or TCR gene therapies e.g. to CD30
-
Conclusions
Relapsed HL following allogeneic HSCT is increasingly commonTo
date there have been no reports of systematic evaluation of salvage
chemotherapyThere is no published evidence on the use of 2nd
transplantsIncreasing experience with DLI confirms graft versus HL,
though optimal strategies remain undefined
-
Proposed Initiatives
Many of the issues regarding DLI overlap with those in other
diseases and could be addressed across disease types.Dose,
schedule, manipulation, timing, MRD, significance of mixed
chimerismAn international collaborative network would facilitate
our ability to address disease-specific issuesRapid testing of new
interventions and early adoption of uniform treatment
strategies.
-
Treatment of Relapsed CLL after Allogeneic Stem Cell
Transplantation
Jose F. Leis, M.D., Ph.D.Mayo Clinic&Nancy M. Hardy, M.D.NCI
Experimental Transplantation and Immunology Branch
-
IntroductionRelapse remains a major cause of treatment failure
after allogeneic transplantation for CLLPFS rates 34-67% and
relapse rates 20-48% reportedRisk factors for relapse include bulky
disease, chemotherapy refractory disease at SCT, T-cell depletion,
donor selection, marrow involvement at SCT, increased number prior
therapies, etc.Both early and late relapses occurR/O donor derived
CLL in MRD SCTMonoclonal B lymphocytosis in13.5-18% of sibs
-
Survival of patients with fludarabine-refractory CLLKeating, M
et al. Leuk Lymphoma 2002; 43:17551762. MonthsProportion
surviving1.00.80.60.40.2001224364860728496(N = 147)
-
Donor Lymphocyte Infusions
Overall CR rate is 45% (33/73) Minority have durable
responses
-
Risk Factors for Failure of DLIsecondary graft-vs.-CLL
resistanceGCLLSG CLL3XUsed real-time PCR and/or flow-based MRD
monitoringIdentified 5 distinct patterns of MRD kineticsOne
pattern: GVL response but failed to reach complete MRD then
relapsed despite extensive cGVHDPossible mechanisms: clonal
evolution survival of clonogeneic cells at GVL sactuary sites
(LNs)developed tolerancepresence of tumor stem cell
Ritgen, Leukemia, 2008
-
Augmenting DLIDonor T-cells may not be appropriately activated
to induce GVL responseEx-vivo co-stimulation donor T-cells with
magnetic beads coated with OKT3 & anti-CD28Conventional DLI
--> escalating aDLI (1 x 106 to 1 x 108/kg in 5 dose levels) 12
days later18 patients: 8 CR (4/7 ALL, 2/4 AML, 1/1 CLL, 1/2 NHL)CLL
patient in CR at 6 years post aDLI7 aGVHD (5 grade I-II, 2 with
grade III)4 cGVHDPorter, Blood 2006
-
Augmenting DLIBi20 (FBTA05), trifunctional, bispecific antibody
targeting CD20 (NHL/CLL) and CD3 (T cells) and DLIMight direct
T-cell efficiently to tumor cell6 patients, 3 with p53-mutated CLL,
3 high-grade NHLCLL patients failed prior DLI,
alemtuzumab/rituximabAll 3 CLL patients showed transient clinical
responsesImproved B symptoms, LNs, splenomegaly, clearing of CLL
from blood with increasing doses Bi20Recurrence of disease within
weeks of cessation of Bi20Despite 1-4 doses DLI (106 to 108
CD3/kg)
Buhmann, BMT 2009
-
Chemotherapy ApproachesObstacles:33-90% reported to be
fludarabine-refractoryHigh-frequency of p53 mutations (up to
50%)Factors predict for failure to alkylating agents, purine
analogues, and rituximabLimited data available for salvage
chemotherapyUsually followed by DLISorror: 5 patients (Flu+rit,
CHOP, pentostatin, VCR/pred)- no durable responsesDelgado: 6
patients (2 CHOP, COP, CMOP=rit/alem, alemtuz+chl, flu/chl)1
patient alive in CR at 40+ months after CHOP and 2 DLI
-
Agents with activity against fludarabine-refractory, p53 mutated
CLLFlavopiridolCDK inhibitor45% response rate, 42% in p53 deleted,
72% in 11q deletedMajor toxicity: hyperacute tumor
lysisBendamustineBifunctional alkylating agent with purine-like
structureActive regardless of p53 or ZAP-70 statusORR >
50%AlemtuzumabORR 33%, equivalent for p53 deletedCytopenias and
infection risk, ? Effect on GVLByrd, Blood, 2007; Bergmann,
Haematologica, 2005
-
Agents with activity against fludarabine-refractory, p53 mutated
CLLHigh-dose methylprednisolone1 gram/m2/day x 5 days +
rituximabORR 78% including 5/9 p53-deleted with 1 cycleInfection in
1/3, Effect on GVL?OfatumumabHumanized anti-CD20 antibodyImpressive
activity in relapsed/refractory CLL (ORR 50%)Effects on acute and
chronic GVHD unknownLenalidomideImmunomodulatory effects: T-cell
activation via CD28, NK cytotoxicity, increased IL-2 expression30%
RR in 11q or 17p deletion CLL
Bowen, Leuk Lymph, 2007; Coiffier, Blood, 2008: Ferrajoli,
Blood, 2008
-
Conclusions
There is an absence of evidenced-based therapeutic options for
treatment of relapsed CLL after allogeneic transplantation Response
rates to standard salvage chemotherapy regimens has been
disappointingReports on the use of DLI are limited and response
rates have been highly variable (0% to 60% CCR) and questions
regarding the durability of response raisedMethods to augment DLI
and novel agents active against fludarabine-refractory CLL are
promising
-
Proposed Initiatives
Development of a national/international consortium to evaluated
the optimal use of DLI in treatment of relapsed CLLInitiation of
multi-center clinical trails to evaluate efficacy of promising
novel agents for treatment of relapsed CLL
-
Nicolaus Krger, Ted AlyeaDisease specific Treatment of Relapse
after Allogeneic Hematopoietic Cell Transplantation Multiple
MyelomaNCI Workshop 1/2-11.2009
-
Specific feature of allografting in Multiple MyelomaOnly about
50% will achieve complete remissionDespite CR, relapse rate is
higher than in other diseases and is about 50% at 5 yearsFor
patients without CR after allografting the progression-rate is even
higher (>80%)Extramedullary relapse seems to be increased after
allogeneic SCT
-
Donor lymphocyte infusion for relapse Studies for relapsed
patients: ORR: 40-67% and CR: 19-30%Acute GvHD II-IV: 52-56% and
cGvHD: 26-44%Strong correlation between response and occurrence of
GvHDNo clear correlation between CD3 cell dose and response
(Lokhorst et al 1997, Verdonck et al 1996, Salama 2000, Ayuk et
al., 2004, Tricot 1996, Bertz et al., 1997)After standard
conditioning
-
Donor lymphocyte infusion for relapseOverall response rate:38%:
PR: 19% and CR 19%Acute GvHD II-IV:38% and c GvHD: 42% (extensive
cGvHD: 10%)Response according GvHD:acute GvHD :no: 21% ORR yes: 67%
ORRchronic GvHD:no: 19% ORR yes: 63% ORRvan de Donk et al.,
2006After RIC
-
Survival after DLI according
resonse60801201,00,80,60,40,20,0Months1004020Proportion of
survivalCRPRLokhorst et al., 2004
-
Novel agents as salvage post allogeneic SCTRationalesBortezomib:
1. highly active against myeloma cells 2. in animal model: reduced
GvHD but retain Graft versus leukemia effect (Sun et al., PNAS
2004) and lead to a decreased T-helper 1 response among allreactive
T-lymphocytes (Blanco et al., Blood 2006) Lenalidomide and
Thalidomide:Activate T-cells and NK-cells which might augment the
graft versus myeloma effect (Lioznov et al., BMT 2009)Low dose
thalidomide more immunosuppressive properties
-
Immunomodulating agentsImmuno modulating agentsMothy,et al 2005;
Lioznov et al 2009; Minnema et al 2008
DosePat.PR-CRGvHDToxThali- domide50-600 mgn = 3129% - 0%n = 5,
grade I-IINeurotoxicityLenali- domide15-25 mgn = 2458% - 8%n = 3,
grade I-IIMyelosuppression (neuro-penia grade 3/4 =25%Lenali-
domide25 mgn = 1650%-31%n = 5, (n = 3, grade
III/IV)Myelosuppression, DVT n = 2
-
Proteasome InhibitorEl-Cheikh, 2008
DosePat.PR - CRGvHDToxBorte- zomib1-1.3 mg/m2 day 1, 4, 8 + 11n
= 3734% - 19%noneNeurotoxicity, grade 1-2: 85%
-
Donor lymphocyte infusion in combination with novel
agentsTreatment planThalidomide 100 mgDLI: 1 x 106 CD3+/kg (MUD)
or: 5 x 106 CD3+/kg (related)No response: escalating Thalidomide
(200 300 400 mg) And/or: further DLI14 daysKrger et al., Blood
2004
-
CR:6/1833%PR:4/1822%MR:2/1812%SD/NC:5/1828%PD:1/185%Low dose
thalidomide (100mg) and escalating DLIResponse rateMed. time to
response: 108 days (36 266)67% (ORR)
-
Thalidomide and DLIafter SCTNo. of patients181118acute GvHD
I-IV10 (55%)5 (46%)2 (11%)acute GvHD II-IV4 (22%)3 (27%)0chr.GvHD
lim4 (22%)4 (36%)7 (39%)chr.GvHD ext1 (6%)0 0after
Thal/DLIafterDLI
-
Treatment options for relapse
ORRCROverall survival1.Donor lymphocyte infusion (DLI)40 67 %19
-30 %med. 23-23.6 mo2.CD8-depleted donor-lymphocyte infusion71 %43
%2year: 55%3.Thalidomide29 83 %0 22 %3year: 25%4.Lenalidomide66 %8
23 %med. 19.9mo5.Bortezomib80 100 %29 30 %3year: 50%7.Thalidomide
plus DLI67 %22 %2year: 100%
-
Novel approaches and future researchManipulation to reduce GvHD
after DLI -CD8 depleted T-cells -CD4 enriched T-cells -Depleting
alloreactive T-cells -Alloreactive NK-cells -Tumor specific T-cells
(anti-idiotype, Cancer-tests antigen, HAG -Antibody mediated
cytotoxicity (BCMA) -Donor vaccination (e.g. idiotype)Enhance cell
mediated cytotoxicity -DLI in combination with novel agents
(thalidomide, Bortezomib, Lenalidomide)Investigate novel drug
combinations, e.g. Lenalidomide plus Bortezomib etc
-
Proposed Initiatives for the subcommitteeTreatment of Relapse
after allo SCTDose-finding studies for novel agents after
allogeneic SCT (Lenalidomide, bortezomib, hypomethylating agents)2.
Clinical trial investigating early (MRD based) vs late (clinical
based) therapeutic intervention (DLI and/or novel agents) to treat
relapse after allogeneic SCT3. Investigate novel agents in
combination with adoptive immunotherapy (T-cells or NK-cells) as
treatment for relapse after allogeneic SCT4. Investigate in a
prospective trial the value of a second allogeneic SCT in those
patient who relapsed to a RIC allograft
-
Future Directions and ProposalsBetter data collection and
reporting.Sample repository for relapse.Identify target cells
and/or antigens for GVT induction.Define prognostic factors and use
to develop and test appropriate strategiesClinicalBiomarkers for
response?
An embarrassing lack of data
-
Future Directions and ProposalsStudy novel agentsazacitidine,
decitabine, lenalidomide, bortezomib, sorafenib, etc..Combination
drug, antibody and/or cellular therapies.Vaccination strategies of
patient/donormHag, tumor-specific antigens, APCsModification of
DLITumor specific DLI through selection, genetic modification,
etc.ActivationSubset selection or depletion Readdress role of
second SCT, particularly after RIC SCT.
-
ObstaclesLack of comprehensive databases capturing relapse
information.Registry studies helpful first stepLack of large
multicenter prospective trials to define best therapies.Difficulty
setting up national and international collaborations.Difficulty
engaging sponsors, payors, regulators, physicians, patients in very
high risk, novel therapies.
-
Moving ForwardInternational multicenter network to rapidly and
definitively test and disseminate new treatment approaches for
relapse.Begin with the First International Workshop on the Biology,
Prevention and Treatment of Relapse after Allogeneic SCT.Maintain
interactions and momentum through workshops, meetings,
consortium-buildingDevelop trials and seek funding.Consider trial
design carefully for maximum and rapid impact. Multiple small
pilots vs randomized phase II or III?
-
Disease-Specific Treatment of Relapse after Allogeneic
TransplantationFred FalkenburgJoseph AntinMarcos de LimaEli
EsteyJohn LevineJacob RoweAlan WayneDavid MaloneyKoen van
BesienKarl PeggsDavid PorterJose LeisNancy HardyNicolaus KrgerEdwin
Alyea
An embarrassing lack of dataTapering immune suppression and
Cytokines : - response rate : anecdotes onlyTreatment should be
offered only for those relapsing longer than 1 yr??Authors
suggested that standard chemotherapy +/- DLI be used only in
patients who relapse 3-6 months after SCT, with other patients
being given clinical trials and palliative care absent such
trials
2*An embarrassing lack of data