Embed Size (px)
Citation preview

3/22/2016
1
Undifferentiated Hypotension
Aparajita Sohoni MDAlameda Health System - Highland Hospital
April 7, 2016
Disclosures
• I have no relevant financial relationships to discloseI will not discuss any off-label use and/or investigational use in my presentation
• *Thanks to Arun Nagdev MD for use of slides/videos in preparation of this talk.
US Protocols for Shock

3/22/2016
2
RUSH
• Rapid Ultrasound for Shock and Hypotension
Outline
• What?
• Why?
• When?
• How?
• Cases
What is the RUSHexam?
• Rapid, systematic evaluation of:
- heart (pump)
- effective intravascular status (tank)
- arterial/venous circulation (pipes)
HIMAP
• Heart
• IVC
• Morison’s/FAST
• Aorta
• Pneumothorax

3/22/2016
3
Why do we do it?
• Assess etiology of shock
• Reversible causes of shock
• Guide resuscitation
Types of Shock
• Hypovolemic
• Cardiogenic
• Obstructive
• Distributive
When?
• Unexplained hypotension or shock
• Part of the primary resuscitation

3/22/2016
4
How to do the exam?
• Start with the heart and IVC
• Add components as clinically indicated
HIMAP
• Heart
• IVC
• Morison’s/FAST
• Aorta
• Pneumothorax
HIMAP++(pump, tank, pipes)
• Heart
• IVC
• Morison’s/FAST
• Aorta
• Pneumothorax
• Lungs for pulmonary edema
• Legs for DVT

3/22/2016
5
Heart
• Three questions:
- Pericardial effusion/tamponade?
- RV failure (massive PE)?
- Qualitative assessment of LV function?
Cardiac Views
• Parasternal long and Apical 4-chamber
• Small footprint probe (3-5MHz)
QuickTime™ and aH.264 decompressor
are needed to see this picture.
LVLVRVRV
Parasternal Long Axis View
LVLV
RVRV

3/22/2016
6
Pericardial effusion
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture. QuickTime™ and aVC Coding

3/22/2016
7
QuickTime™ and aVC Coding
QuickTime™ and aVC Coding
QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.
Pericardial vs. Pleural Fluid
• Descending thoracic aorta

3/22/2016
8
Pleural effusion
Descending Thoracic
Aorta Image source: https://sonospot.wordpress.com Image source: https://sonospot.wordpress.com
Pericardial effusion
Descending Thoracic
Aorta
QuickTime™ and aVC Coding
Pericardial Tamponade• Collapse of the RV during early diastole

3/22/2016
9
QuickTime™ and aVC Coding
Pericardial Tamponade
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aVC Coding
QuickTime™ and aH.264 decompressor
are needed to see this picture.

3/22/2016
10
Heart
• Three questions:
- Pericardial effusion/tamponade?
- RV failure (massive PE)?
- Qualitative assessment of LV function?
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.

3/22/2016
11
Heart
• Three questions:
- Pericardial effusion/tamponade?
- RV failure (massive PE)?
- Qualitative assessment of LV function?
QuickTime™ and aDV/DVCPRO - NTSC decompressor
are needed to see this picture.
QuickTime™ and aDV/DVCPRO - NTSC decompressor
are needed to see this picture.
Normal Low EF
Normal vs. Hypodynamic Left Ventricle
QuickTime™ and aDV - NTSC decompressor
are needed to see this picture.
Poor EF
QuickTime™ and aDV/DVCPRO - NTSC decompressor
are needed to see this picture.

3/22/2016
12
QuickTime™ and aDV/DVCPRO - NTSC decompressor
are needed to see this picture.
EPSS
• E-point to septal separation (EPSS)
• E wave: Early Filling Phase
- during diastole, initial wave of blood that enters the left ventricle from the left atrium (70-80%)
- A wave: “atrial kick”
- normal EPSS is less than 8-10mm
QuickTime™ and aH.264 decompressor
are needed to see this picture.
NormalAbnormal
QuickTime™ and aVC Coding

3/22/2016
13

3/22/2016
14
Fractional Shortening
• Another way to estimate EF
• Correlates to overall LV contractility
• FS of 30-45% = normal LV contractility
• [EDD-ESD/EDD] x 100
Image source: https://sonospot.wordpress.com
Image source: https://sonospot.wordpress.com
QuickTime™ and aDV/DVCPRO - NTSC decompressor
are needed to see this picture.
QuickTime™ and aDV/DVCPRO - NTSC decompressor
are needed to see this picture.
Normal Low EF
Normal vs. Hypodynamic Left Ventricle

3/22/2016
15
Hyperdynamic LV
• LV walls change >90% between systole and diastole
• LV walls touch at end-systole
QuickTime™ and aH.264 decompressor
are needed to see this picture.
Heart
• Three questions:
✓Pericardial effusion/tamponade?
✓RV failure (massive PE)?
✓Qualitative assessment of LV function?
HIMAP
✓Heart
• IVC
• Morison’s/FAST
• Aorta
• Pneumothorax

3/22/2016
16
HIMAP
• Heart
• IVC
• Morison’s/FAST
• Aorta
• Pneumothorax
IVCIndicator toward chinAim towards thoracic
spine
RA
IVC
IVCImage the
IVC entering Right Atrium
QuickTime™ and aH.264 decompressor
are needed to see this picture.
IVCIVC

3/22/2016
17
• Assess for IVC fullness
• Assess for collapse with inspiration
- 2-3cm inferior to right atrial junction
• Note collapsibility
IVCGoals
QuickTime™ and aTIFF decompressor
are needed to see this picture.
QuickTime™ and aTIFF decompressor
are needed to see this picture.
cephalad caudad
diaphragm
RA border
cephalad caudad
diaphragm
RA border
IVCi IVCe
liver liver
Expiration
IVC
Inspiration
2-3 cm
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.
IVC & CVP

3/22/2016
18
IVC vs Aorta
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.
• Empties into heart ● Flows deep to heart
• Flows through liver ● Flows deep to liver
• Undulating Pulsation ● Bounding Pulsation
Pitfalls:
Can’t find the IVC?
• Use the internal jugular veins
• Note collapsibility during respiratory cycle
Image source: Seif et al. CCRP
HIMAP
✓Heart
✓IVC
• Morison’s/FAST
• Aorta
• Pneumothorax

3/22/2016
19
1. Hepatorenal -Morison’s*
2. Splenorenal*
3. Suprapubic
3
441 2
FAST Exam
*include thoracic views
Morison’s Pouch
QuickTime™ and aVC Coding
QuickTime™ and aVC Coding

3/22/2016
20
QuickTime™ and aVC Coding
Don’t forget the pleural space!
1. Hepatorenal -Morison’s*
2. Splenorenal*
3. Suprapubic
3
441 2
FAST Exam
*include thoracic views
Splenorenal Recess
Spleen
Kidney
Hyperechoic Diaphragm
Costophrenic recess
QuickTime™ and aVC Coding

3/22/2016
21
QuickTime™ and aVC Coding
Don’t forget the pleural space!
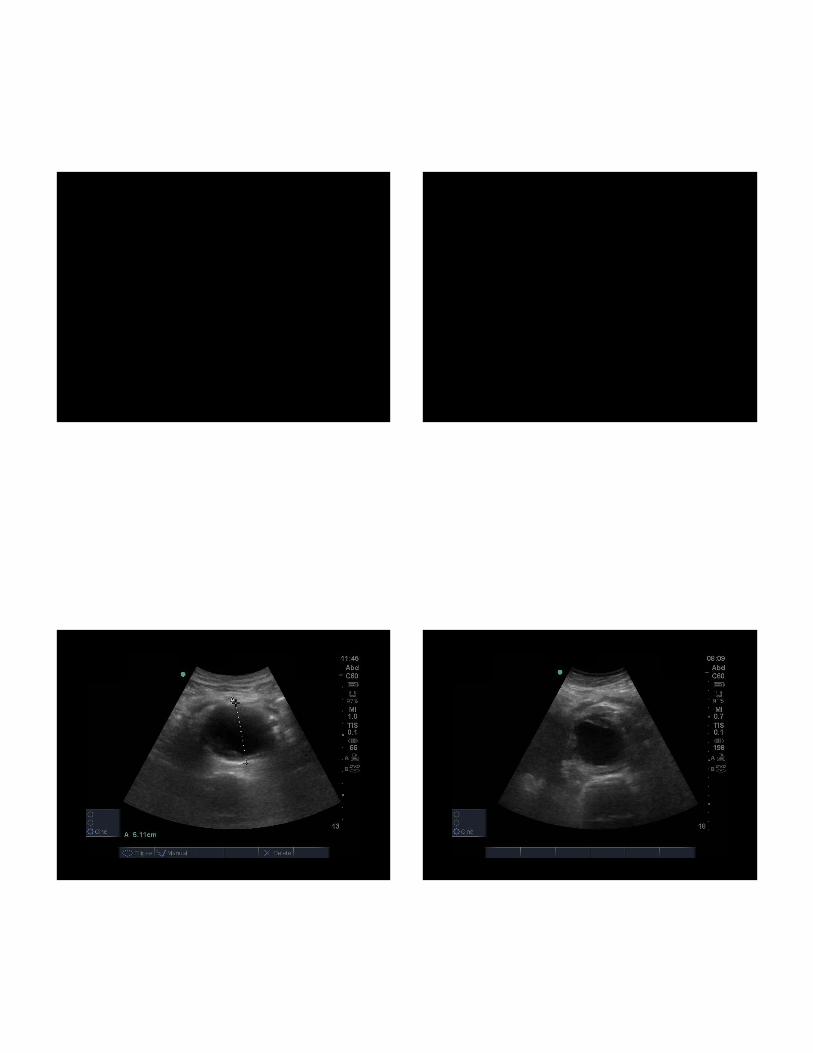
Suprapubic
Transverse Longitudinal
Pelvic View Transverse:
Male
Abnormal
Pelvic View Transverse: Female
Abnormal
Abnormal
Uterus

3/22/2016
22
Pelvic View Longitudinal:
Male
Abnormal
Pelvic View Longitudinal: Female
Abnormal
HIMAP
✓Heart
✓IVC
✓Morison’s/FAST
• Aorta
• Pneumothorax
Aorta
• 2 dimensions
• Image through the bifurcation
• Look for AAA or dissection
3/22/2016
23
QuickTime™ and aVC Coding
QuickTime™ and aVC Coding

3/22/2016
24
QuickTime™ and aVC Coding
QuickTime™ and aVC Coding

3/22/2016
25
HIMAP
✓Heart
✓IVC
✓Morison’s/FAST
✓Aorta
• Pneumothorax
Pneumothorax
• Linear transducer
• Indicator towards the head
• Anterior intercostal spaces
• Bilateral
QuickTime™ and aVC Coding
QuickTime™ and aVC Coding

3/22/2016
26
QuickTime™ and aVC Coding
Image source: Seif et al. CCRP
HIMAP
✓Heart
✓IVC
✓Morison’s/FAST
✓Aorta
✓Pneumothorax
HIMAP++(pump, tank, pipes)
• Heart
• IVC
• Morison’s/FAST
• Aorta
• Pneumothorax
• Lungs for pulmonary edema
• Legs for DVT

3/22/2016
27
Pulmonary Edema
QuickTime™ and aDV/DVCPRO - NTSC decompressor
are needed to see this picture.
Acute Interstitial Syndrome
Arise from the pleural line
Well-defined
B lines = interstitial syndrome
B lines = interstitial syndrome
Move with lung slidin
3 per rib space
Reach screen edge
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.
A Lines B Lines
Normal Lung
COPD
Asthma
Pulmonary Edema
Pneumonia
Interstitial Fibrosis
ARDS
Lung Contusion
QuickTime™ and aDV - NTSC decompressor
are needed to see this picture.
B lines = increased fluid in the interstitium

3/22/2016
28
QuickTime™ and aDV - NTSC decompressor
are needed to see this picture.QuickTime™ and a
H.264 decompressorare needed to see this picture.
A lines = Dry
B lines = WetB lines = Wet
QuickTime™ and aH.264 decompressor
are needed to see this picture.
A lines = DryA lines = Dry
QuickTime™ and aH.264 decompressor
are needed to see this picture.
HIMAP++(pump, tank, pipes)
• Heart
• IVC
• Morison’s/FAST
• Aorta
• Pneumothorax
• Lungs for pulmonary edema
• Legs for DVT

3/22/2016
29
QuickTime™ and aDV - NTSC decompressor
are needed to see this picture.
QuickTime™ and aVC Coding

3/22/2016
30
Overwhelmed?
• Don’t have to do everything on everyone
• Start with heart and IVC on everyone
Outline
• What?
• Why?
• When?
• How?
• Cases
Case 1
32 y/o Dev. Delayed maleCode 3 by EMS
SVT and respiratory distress
Phonating
Decreased BS on Left base
Extreme TachyIrregular rhythm
Pulses weak
No Edema
HR 242 BP 90/palp RR 34 SaO2 90%

3/22/2016
31
ED Course
• Pacer pads placed.
• Adenosine drawn up.
• Ultrasound machine to the bedside.
Bedside Echo, Apical
QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.

3/22/2016
32
Echo findings:
• Pericardial effusion: Huge
• Cardiac Function: Hyperdynamic LV
RV collapse
• Central Venous: HighPressure
= Impending Tamponade
Case 2
83 y/o MCHF, LVEF 20%
Febrile, HypotensiveAltered
BP 88/50 HR 110 R 18 O2 96% T 101.3
Phonating, Mumbling
Bibasilar RalesNml chest rise
TachyReg rhythm
Pulses weak
2+ Pitting Edema

3/22/2016
33
QuickTime™ and aH.264 decompressor
are needed to see this picture.
Parasternal Long Axis
QuickTime™ and aH.264 decompressor
are needed to see this picture.
Parasternal Short Axis
QuickTime™ and aH.264 decompressor
are needed to see this picture.
Apical 4 Chamber

3/22/2016
34
QuickTime™ and aH.264 decompressor
are needed to see this picture.
IVC
Echo findings:
• Pericardial effusion: No
• Cardiac Function: Depressed LV Fxn
• Central Venous: Low/NormalPressure
= Give me fluids
Case 3
46 y/o F with no PMHPalpitations and Dyspnea
BP 80/40 HR 152 R 32 O2 90% T 98.4
Speaking Full Sentences
CTA BKussmaul
Respirations
TachyReg rhythm
Pulses Normal
No Edema

3/22/2016
35
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.
Parasternal Long Axis
RV - Large &Hypokinetic
LV - Small &Hyperkinetic
Normal
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.
Parasternal Short Axis
“D”-ShapedLeft Ventricle
D
RV - Large &Hypokinetic
LV - Small &Hyperkinetic
(Septal Wall Flattening)
Normal
QuickTime™ and aH.264 decompressor
are needed to see this picture.
RV - Large &Hypokinetic
LV - Small &Hyperkinetic
RVD:LVD >1(normal<1)
QuickTime™ and aH.264 decompressor
are needed to see this picture.
Apical 4 ChamberNormal

3/22/2016
36
QuickTime™ and aH.264 decompressor
are needed to see this picture.
IVC
IVC= Plethoric(Full, Stiff)
Echo findings:
•Pericardial effusion: No
•Cardiac Function: Hyperdynamic LVRV Dysfunction
• (RV dilation, Pulm HTN)
•Central Venous: HighPressure=High Suspicion for Submassive Pulmonary
Embolism
Conclusions
• Valuable tool for evaluation of critically ill hypotensive patients
• Become comfortable with heart and IVC views; add on more as you go

3/22/2016
37
Where can I learn more?
• Weingart S, et al. The RUSH Exam: Rapid Ultrasound for Shock and Hypotension (http://emcrit.org/rush-exam/)
• Seif D, Pereira P, Mailhot T, et al. Bedside ultrasound in resuscitation and the rapid ultrasound in shock protocol. Crit Care Research & Practice. August 2012.
• Sonospot.wordpress.com (cases & review)
Questions?





















![Intradialytic hypotension [투석 중 저혈압]](https://img.dokumen.tips/doc/110x75/558406e7d8b42a6a148b4edc/intradialytic-hypotension--5584b8e435e7e.jpg)







