Embed Size (px)
Citation preview

2008;139;305-315 J Am Dent Assoc
George Bogen, Jay S. Kim and Leif K. Bakland Aggregate: An Observational Study
Direct Pulp Capping With Mineral Trioxide
jada.ada.org ( this information is current as of July 20, 2010 ):The following resources related to this article are available online at
http://jada.ada.org/cgi/content/full/139/3/305found in the online version of this article at:
including high-resolution figures, can beUpdated information and services
http://jada.ada.org/cgi/collection/endodonticsEndodontics : subject collectionsThis article appears in the following
http://www.ada.org/prof/resources/pubs/jada/permissions.aspreproduce this article in whole or in part can be found at:
of this article or about permission toreprintsInformation about obtaining
© 2010 American Dental Association. The sponsor and its products are not endorsed by the ADA.
on July 20, 2010 jada.ada.org
Dow
nloaded from

Background. Pulp capping in carious teeth hasbeen considered unpredictable and therefore con-traindicated. A recently developed material, mineraltrioxide aggregate (MTA), resists bacterial leakage andmay provide protection for the pulp, allowing repairand continued pulp vitality in teeth when used in combi-nation with a sealed restoration.Methods. Forty patients aged 7 to 45 years accepted pulp-capping treat-ment when they received a diagnosis no more severe than reversible pulpitisafter undergoing cold testing and radiographic examination. The primaryauthor removed caries using a caries detector dye and sodium hypochloritesolution for hemostasis and placed MTA over the exposures and all sur-rounding dentin. The operator then restored the teeth provisionally withunbonded Clearfil Photocore (Kuraray Medical, Okayama, Japan). During asecond visit, the operator restored the teeth with bonded composite aftersensibility testing and confirmed MTA curing. At recall appointments,patients were evaluated for reparative dentin formation, pulpal calcification,continued normal root development and evidence of pathosis.Results. Over an observation period of nine years, the authors followed 49 of 53 teeth and found that 97.96 percent had favorable outcomes on thebasis of radiographic appearance, subjective symptoms and cold testing. Allteeth in younger patients (15/15) that initially had had open apexes showedcompleted root formation (apexogenesis). Conclusions. MTA can be a reliable pulp-capping material on direct car-ious exposures in permanent teeth when a two-visit treatment protocol isobserved.Practice Implications. Vital pulp therapy using MTA is a treatmentoption for teeth diagnosed with a condition no more severe than reversiblepulpitis.Key Words. Reversible pulpitis; direct pulp capping; mineral trioxideaggregate; sodium hypochlorite.JADA 2008;139(3):305-315.
Preservation and mainte-nance of pulpal vitality isone objective in endodon-tics. Historically, theplacement of a medica-
ment or material against a directpulpal exposure during caries exca-vation has been considered contro-versial, and instead conventionalendodontic therapy has been recom-mended.1-5 The reluctance to place adirect pulp cap on an exposure in acarious field is based on unpre-dictable outcomes using traditionalmaterials and treatment protocols.Moreover, when bacterial by-products induce pulpal inflamma-tion, compromise immune responsesand impede cellular differentiationand recruitment, normal pulpalrepair mechanisms may not func-tion properly. To date, researchershave been unable to identify a reli-able nonabsorbable bioactive pulp-capping material that consistentlystimulates cellular repair mecha-nisms, seals the dentin and pro-motes formation of a biologicallystable reparative dentin bridge.
Clinicians have used manymaterials and techniques for directpulp capping, including calciumhydroxide, hydrophilic resins, resin-modified glass ionomer cements, tri-calcium phosphates and, morerecently, mineral trioxide aggregate(MTA). Other innovative technicaladvances to halt the carious processand initiate the repair of potentially
A B S T R A C T
ARTICLE
4
Dr. Bogen maintains a private endodontic practice, 321 N. Larchmont Blvd., Suite 721, Los Angeles,Calif. 90004, e-mail “[email protected]”. Address reprint requests to Dr. Bogen.Dr. Kim is a professor of biostatistics, Loma Linda University, Calif.Dr. Bakland is a professor and the chairman, Department of Endodontics, Loma Linda University, Calif.
JA D
A
CO
NT
I
NU
I N G E D UC
AT
IO
N
✷✷®
Direct pulp capping with mineral trioxideaggregateAn observational study
George Bogen, DDS; Jay S. Kim, PhD; Leif K. Bakland, DDS
R E S E A R C H
JADA, Vol. 139 http://jada.ada.org March 2008 305
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

damaged tissue include the use of lasers, ozonetechnology and bioactive agents that induce andstimulate pulpal defenses.6-8 Success rates withdirect pulp capping in a carious field have varieddepending on the technique and materials. Inhumans, success rates range from 30 to 85 per-cent in two- to 10-year retrospective studies.4,9-13
Recent advances in our understanding of pulpalphysiology, caries progression, inflammatorymediators and pulpal defense mechanisms havechanged the clinical approach to caries removaland protocols for direct pulp capping.14
Direct pulpal exposures can be a challengingproblem during excavation in a carious field. Adiagnosis of reversible pulpitis before treatmentis necessary for a successful outcome, but a definitive pulpal diagnosis often is difficult toestablish.9 In 1966, Fusayama and colleagues15
made significant advances in the field of cariesresearch and pulpal protection. They were thefirst to show that the upper layer of two distinc-tive carious layers could be stained selectivelyand that subsequent objective caries removalwould allow for pulpal preservation and repairwhen teeth were sealed with bonded resin-basedcomposites.16-18
In 1996, Matsuo and colleagues13 assessed fac-tors that affect the success of direct pulp capping.They placed direct pulp caps on teeth in a cariousfield using a caries detector, 10 percent sodiumhypochlorite (NaOCl) for hemostasis and fast-setcalcium hydroxide. The patient’s age, exposuresize, responses to percussion or thermal stimula-tion, and type of tooth and location had no reflec-tion on the success rate. When adequate hemo-stasis using 10 percent NaOCl could be attained,success rates increased. Thus, uncontrolled hem-orrhaging may be directly proportional to the con-centration of inflammatory mediators and thedegree of intrapulpal pressure, which may affectthe probability that hemostasis can be achieved.Nakanishi and colleagues19 reported evidence thatinflammatory mediators such as immunoglobulinG, immunoglobulin A, immunoglobulin M, elas-tase and prostaglandin E2 were present in higherquantities in clinically inflamed pulps.19
Calcium hydroxide—once considered thestandard for pulp-capping materials—provides anoption for reparative dentin formation, but long-term studies have shown results to be variableand somewhat unpredictable.9-12 The materialdoes not provide close adaptation to dentin, doesnot promote consistent odontoblast differentiation
and has been shown to be cytotoxic in cell cul-tures; the resultant reparative dentin formationcan be characterized by tunnel defects.20-22 Tunneldefects within dentin bridges may provide apathway for the penetration of microorganisms toactivate circulating immune cells, induce pulpalirritation and produce subsequent dystrophic cal-cification. Investigators using hydrophilic resinsand resin-modified glass ionomer cements asdirect pulp-capping agents have reportedpromising results in nonhuman primates23,24 buthave not determined predictable outcomes whenthese agents are used in humans.25-28 Researchersusing inventive modalities to test alternativepulp-capping agents also have been unsuccessfulin stimulating pulpal repair and healing in casesof direct carious exposures.29,30
MTA is a bioactive silicate cement that hasbeen shown to be an effective pulp-cappingmaterial in canine models and in nonhuman pri-mates.31-33 The material is successful because ofits small particle size, sealing ability, alkaline pHwhen set and slow release of calcium ions.34 Inves-tigators have reported that MTA induces pulpalcell proliferation,35,36 cytokine release,37 hardtissue formation22 and the synthesis of an inter-face with dentin that resembles hydroxyapatite incomposition.34 The material is nonabsorbable, setsin the presence of moisture, has a relatively highcompressive strength and has a sustained highalkaline pH.38 Recent studies examining partialpulpotomies or direct pulp capping using MTA inhumans have shown favorable short-termresults.39-43 There are no clinical studies that havecombined and evaluated the use of a cariesdetector dye, NaOCl hemostasis, direct MTA pulpcapping and bonded composite placement in atwo-visit protocol. The aim of our study was tomonitor the long-term success rate of surgicallyrepaired pulpal exposures in teeth with deep car-ious lesions using MTA and current adhesiontechnology.
METHODS AND MATERIALS
All patients in our study had been referred forendodontic treatment to a private office or theChildren’s Dental Health Clinic, Long Beach,Calif., and had completed periapical radiographs,
R E S E A R C H
306 JADA, Vol. 139 http://jada.ada.org March 2008
ABBREVIATION KEY. MTA: Mineral trioxide aggre-gate. NaOCL: Sodium hypochlorite. PDL: Periodontalligament.
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

periodontal probing, percussion testing andvitality assessment with cold testing. The pri-mary author (G.B.) selected 53 teeth for treat-ment over an eight-year period that included 51molars, one maxillary premolar and one maxil-lary incisor. All teeth exhibited initial deep cariesand no prior restorations. Both female and malepatients had variable health histories and symp-toms and ranged in age from 7 to 45 years. Allradiographs showed evidence of deep caries inclose proximity to the pulpal chamber with noevidence of thickened periodontal ligament(PDL), furcation radiolucencies, internal resorp-tion or periradicular pathosis. Clinically, all teethhad mobility and periodontal probings withinnormal range with no evidence of sinus tracts orswelling. No teeth treated in this study exhibitedpain on percussion. Fifteen younger patients hadradiographically evident immature apexes beforetreatment. We did not use control groups sincethe aim of the study was to monitor pulpal sur-vival time using one specific protocol, and weplanned to measure the outcomes against sur-vival periods from previous studies that used cal-cium hydroxide.9-13 We obtained written consentfrom all study participants or their legalguardians. The Loma Linda University Institu-tional Review Board (Loma Linda, Calif.)reviewed and accepted the protocol.
One operator (G.B.) completed all direct pulpcaps. After patients obtained profound local anes-thesia, the operator placed a dental dam andused an oral sealant to prevent saliva leakagewhere necessary. The operator used a cariesdetector dye and performed caries excavationunder ×3.5 to ×18.0 magnification using hand-pieces with high-speed diamond or carbide bursand no. 6-2 slow-speed carbide round burs. Hecontinued caries excavation even after pulpalexposures occurred and stopped the excavationwhen either little or no dye staining was evidentover the pulpal roof or axial wall.
The operator used either 5.25 percent or 6.00percent NaOCl as a direct solution or on a soakedcotton pellet to achieve hemostasis. He estab-lished hemorrhage control within one to 10 min-utes in all cases. The operator excluded onepatient from this study when hemorrhaging con-tinued beyond this time. After the operatorachieved hemostasis, he sprayed the exposuresite and dentin with water from a two-waysyringe and then air-dried the area. The dentalassistant mixed gray MTA or white MTA
according to the manufacturer’s instructions (Pro-Root MTA, Dentsply Tulsa Dental, Tulsa, Okla.)and the operator placed a 1.5- to 3.0-millimeterthick layer of the cement directly over the expo-sure site and surrounding dentin, leaving 1 to 2mm of dentin and enamel available circumferen-tially for the future bonded restoration. Afterplacing the MTA, the operator laid a flat, water-moistened cotton pellet directly over the materialand provisionally restored the tooth withunbonded Clearfil Photocore (Kuraray Medical,Okayama, Japan) that was photopolymerized for60 seconds.
The operator instructed patients or their par-ents to call the office immediately if pain or dis-comfort occurred after treatment. Patients thenreturned to our office or the referring generaldentists’ offices for placement of the final restora-tion within five to 10 days. Two patients chosenot to return for continued treatment. Allpatients in the study were asymptomatic and hada normal response to cold testing before place-ment of the final restoration. After patientsagain obtained profound anesthesia, the operatorplaced a dental dam and removed the ClearfilPhotocore provisional restoration by using a car-bide bur in a high-speed handpiece. He thenassessed the MTA for hardness and removed theembedded cotton fibers with spoon excavators.Next, the operator placed Class I or II compositerestorations incrementally and bonded themusing a self-etching primer and resin withClearfil LB2 Bond and Clearfil AP-X Composite(Kuraray Medical). The referring general den-tists restored six teeth in five patients withbonded composites. Whenever possible, werecalled patients at six weeks, six months and ona yearly basis thereafter. Recall appointmentsconsisted of obtaining self-reports from patients,taking periapical radiographs and testing thepulp-capped teeth with a cold stimulus. Two of us(G.B. and L.K.B.) evaluated radiographs forreparative dentin formation, pulpal calcification,continued normal root development and theabsence of pathosis. We also evaluated the finalrestorations for marginal integrity. Threepatients had to attend recall appointments out ofstate, either at a private endodontic office or adental school facility.
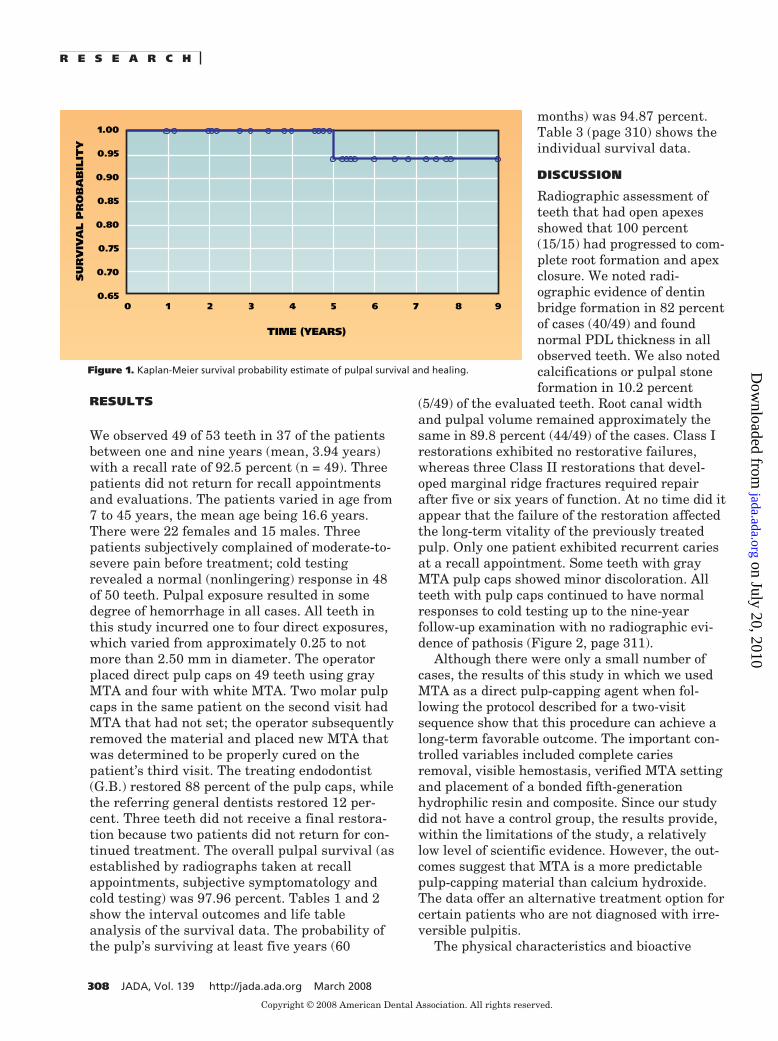
Statistical analysis. Figure 1 shows theresults of the study using the life table analysisand the Kaplan-Meier method to estimate theprobability of pulpal survival and healing.
R E S E A R C H
JADA, Vol. 139 http://jada.ada.org March 2008 307
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from
RESULTS
We observed 49 of 53 teeth in 37 of the patientsbetween one and nine years (mean, 3.94 years)with a recall rate of 92.5 percent (n = 49). Threepatients did not return for recall appointmentsand evaluations. The patients varied in age from7 to 45 years, the mean age being 16.6 years.There were 22 females and 15 males. Threepatients subjectively complained of moderate-to-severe pain before treatment; cold testingrevealed a normal (nonlingering) response in 48of 50 teeth. Pulpal exposure resulted in somedegree of hemorrhage in all cases. All teeth inthis study incurred one to four direct exposures,which varied from approximately 0.25 to notmore than 2.50 mm in diameter. The operatorplaced direct pulp caps on 49 teeth using grayMTA and four with white MTA. Two molar pulpcaps in the same patient on the second visit hadMTA that had not set; the operator subsequentlyremoved the material and placed new MTA thatwas determined to be properly cured on thepatient’s third visit. The treating endodontist(G.B.) restored 88 percent of the pulp caps, whilethe referring general dentists restored 12 per-cent. Three teeth did not receive a final restora-tion because two patients did not return for con-tinued treatment. The overall pulpal survival (asestablished by radiographs taken at recallappointments, subjective symptomatology andcold testing) was 97.96 percent. Tables 1 and 2show the interval outcomes and life tableanalysis of the survival data. The probability ofthe pulp’s surviving at least five years (60
months) was 94.87 percent.Table 3 (page 310) shows theindividual survival data.
DISCUSSION
Radiographic assessment ofteeth that had open apexesshowed that 100 percent(15/15) had progressed to com-plete root formation and apexclosure. We noted radi-ographic evidence of dentinbridge formation in 82 percentof cases (40/49) and foundnormal PDL thickness in allobserved teeth. We also notedcalcifications or pulpal stoneformation in 10.2 percent
(5/49) of the evaluated teeth. Root canal widthand pulpal volume remained approximately thesame in 89.8 percent (44/49) of the cases. Class Irestorations exhibited no restorative failures,whereas three Class II restorations that devel-oped marginal ridge fractures required repairafter five or six years of function. At no time did itappear that the failure of the restoration affectedthe long-term vitality of the previously treatedpulp. Only one patient exhibited recurrent cariesat a recall appointment. Some teeth with grayMTA pulp caps showed minor discoloration. Allteeth with pulp caps continued to have normalresponses to cold testing up to the nine-yearfollow-up examination with no radiographic evi-dence of pathosis (Figure 2, page 311).
Although there were only a small number ofcases, the results of this study in which we usedMTA as a direct pulp-capping agent when fol-lowing the protocol described for a two-visitsequence show that this procedure can achieve along-term favorable outcome. The important con-trolled variables included complete cariesremoval, visible hemostasis, verified MTA settingand placement of a bonded fifth-generationhydrophilic resin and composite. Since our studydid not have a control group, the results provide,within the limitations of the study, a relativelylow level of scientific evidence. However, the out-comes suggest that MTA is a more predictablepulp-capping material than calcium hydroxide.The data offer an alternative treatment option forcertain patients who are not diagnosed with irre-versible pulpitis.
The physical characteristics and bioactive
R E S E A R C H
308 JADA, Vol. 139 http://jada.ada.org March 2008
1.00
0.95
0.90
0.85
0.80
0.75
0.70
0.650 1 2 3 4 5 6 7 8 9
TIME (YEARS)
SU
RV
IVA
L P
RO
BA
BIL
ITY
Figure 1. Kaplan-Meier survival probability estimate of pulpal survival and healing.
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

properties of MTA were acritical contributing factorto the success of thisstudy.34-38 The cement ishygroscopic, and its abilityto set is not affected by thepresence of blood or serumfluids.44 The high alka-linity of MTA, its calciumrelease and sustained pHof 12.5 most likely pre-vented any further micro-bial growth of residualmicroorganisms that wereleft after caries excavation.The high pH also extractsgrowth factors from adja-cent dentin that arethought to be responsiblefor promoting dentinalbridging.45 Furthermore,the release of calcium ionsby MTA generates a reac-tionary interfacial layer ofhydroxyapatite on its sur-face when it comes in con-tact with tissue fluids, andtheir presence also maycontribute to reparativedentin formation.34 Theclose physiochemical sealof dentin by MTA, deter-mined to be 0 micrometersin resin replica models,46
provides a more insolublebarrier against micro-leakage than does calcium hydroxide, which canshow gaps at the dentin interface of 7 to 15 µmwhen placed under composite restorations.47 Onceset, it is nonabsorbable, whereas set calciumhydroxide is unstable and can degrade and dis-solve under restorations, allowing potentialingress of microorganisms and subsequent bacte-rial contamination through tunnel defects in thedentin bridge. These events can induce continuedpulpal irritation, dystrophic calcification andpotential degenerative changes in the pulp.21,48
Traditionally, dentists place pulp-cappingagents over the exposure site and a small area ofsurrounding dentin. In our study, the operatorplaced MTA over the exposure site and the entirefloor or wall of the restoration preparation toallow a 1.5- to 3.0-mm thickness of the material.
If the exposure occurred on the axial wall in aClass II preparation, the operator placed MTA onthe base of the gingival-cavosurface to the mesialand distal restoration extensions in a 1.5- to 2.0-mm thickness (Figure 3, page 312). Afterapplying MTA, the operator trimmed and shapedthe material with spoon excavators to expose 1.0to 2.0 mm of peripheral dentin and enamel andthen used a small moist cotton pellet to clean it toensure an adequate surface area for bonding onthe second visit. The operator placed direct pulpcaps on only four teeth with white MTA since itwas not commercially available until late into thisstudy. We found no difference in short-term out-comes between the gray and the white MTA.
Optical magnification and careful cariesremoval aided by a caries detector dye also were
R E S E A R C H
JADA, Vol. 139 http://jada.ada.org March 2008 309
TABLE 1
Interval failure/success rate of survival data.INTERVAL(YEARS)
NO. OFTEETH ATBEGINNING
OF INTERVAL
NO. OF TEETHFAILEDDURING
INTERVAL
NO. OFTEETH LOSTTO FOLLOW-
UP
INTERVALFAILURERATE (%)
INTERVALSUCCESSRATE (%)
0, 1
1, 2
2, 3
3, 4
4, 5
5, 6
6, 7
7, 8
8, 9
49
44
41
32
23
16
8
6
1
0
0
0
0
1
0
0
0
0
5
3
9
9
7
8
2
5
1
0
0
0
0
4.35
0
0
0
0
100
100
100
100
95.65
100
100
100
100
TABLE 2
Life table analysis of survival data.INTERVAL(YEARS)
NO. OF TEETHAT BEGINNINGOF INTERVAL
EFFECTIVESAMPLE SIZE
PROBABILITYOF FAILURE
PROBABILITYOF SURVIVING
(%)
INTERVALSUCCESSRATE (%)
0, 1
1, 2
2, 3
3, 4
4, 5
5, 6
6, 7
7, 8
8, 9
49
44
41
32
23
16
8
6
1
46.5
42.5
36.5
27.5
19.5
12
7
3.5
0.5
0
0
0
0
5.13
0
0
0
0
100
100
100
100
94.87
100
100
100
100
100
100
100
100
94.87
94.87
94.87
94.87
94.87
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

R E S E A R C H
TABLE 3
Distribution of 49 carious teeth with direct pulp caps with mineral trioxide aggregate.PATIENT TOOTH
NO.AGE
(YEARS)SEX DENTIN BRIDGE
FORMATIONPULP VITALITY SURVIVAL
TIME AT LAST RECALL
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
3
14
3019
314
19
2
30
30
19
30
30
15
1831
15
19
30
14
2
14
3141930
18
1930
19
1318
30
1314
2
15
31
3
1930
314
30
30
19
919
15
15
8
711
10
29
17
7
7
19
7
18
13
14
26
10
30
13
18
29
7
10
9
16
17
9
27
45
28
33
16
8
12
9
12
28
11
14
F
F
M
F
F
F
F
F
M
F
F
M
M
F
M
M
F
F
F
M
M
M
F
F
F
M
F
F
M
F
F
M
F
M
F
M
M
Undetermined
Yes
YesYes
YesYes
Undetermined
Yes
Yes
Yes
Yes
Yes
Undetermined
Yes
YesYes
Yes
Undetermined
Yes
Yes
Yes
Yes
YesYesYesYes
Yes
YesYes
Yes
YesUndetermined
Yes
UndeterminedYes
Undetermined
Yes
Yes
Yes
YesYes
YesYes
Yes
Undetermined
Yes
UndeterminedYes
Yes
7 years, 9 months
7 years, 6 months
7 years, 6 months2 years, 9 months
3 years, 10 months3 years, 10 months
7 years, 10 months
9 years
4 years, 7 months
4 years
2 years, 2 months
7 years, 3 months
6 years, 6 months
4 years, 9 months
2 years,1 month2 years, 1 month
3 years, 5 months
5 years (failure)
2 years
6 years, 10 months
4 years
5 years
5 years, 4 months5 years, 4 months5 years, 3 months5 years, 3 months
4 years, 5 months
6 years6 years
5 years, 5 months
4 years, 11 months4 years, 8 months
5 years, 6 months
3 years3 years
3 years, 5 months
2 years
3 years, 10 months
1 year
2 years, 2 months2 years, 2 months
1 year1 year
1 year
1 year
1 year, 2 months
4 years4 years
3 years
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

important components of this study. The studyoutcome shows that the human pulp has aninnate healing capacity that can be enhancedusing objective and conservative caries removal, abioactive pulp-capping material and a sealed res-toration. The high occurrence of pulpal repair andpulp-capping success appears to be more favor-
able in teeth of younger patients; success can beattributed to the presence of larger apicalforamina and greater vascularization of the pulp,in which active immune cell surveillance mayincrease chances for repair and intensify vitalpulpal maintenance.12 Pulpal survival decreaseswith age and cumulative restorative trauma.49,50
R E S E A R C H
JADA, Vol. 139 http://jada.ada.org March 2008 311
Figure 2. Radiographic and clinical sequence of mineral trioxide aggregate (MTA) direct pulp capping of a mandibular right molar in a 9-year-old female patient. A. Pretreatment radiograph showing intial deep caries and immature apices. B,C,D. Five-minute time of 5.25percent sodium hypochlorite hemostasis, on two 1.5- to 2.0-millimeter exposures (arrows). E. Radiograph of molar with MTA, water-moistened cotton pellet and unbonded Clearfil Photocore (Kuraray Medical, Okayama, Japan) provisional restoration after initial visit. F. Radiograph taken at the 5.5-year recall appointment showing permanent restoration and evidence of complete root formation. The tooth exhibited a normal response to cold testing.
A B
D
E F
C
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

We used NaOCl as a hemostatic agent in thisstudy on all pulpal exposures. Concentrationsvaried from 5.25 to 6.00 percent, since the concen-tration of commercially available solutionschanged during the study. Sodium hypochloritewas first advocated for pulpal hemostasis in thelate 1950s.51 The solution has several advanta-geous properties besides being an excellent hemo-static agent.51 Specifically, it can disinfect micro-bially contaminated dentinal chips and operativedebris, inhibit fibrin clot formation and disinfectthe adjacent perforated dentin interface. Al-though studies have shown that use of NaOCl atconcentrations higher than 0.025 percent is detri-mental to wound healing in human tissue when itis used as a fluid dressing for patients withburns,52 pulpal reactions appear to be remarkablyfavorable.53,54 No pulpal exposures in our studywere affected adversely by direct contact with5.25 to 6.00 percent NaOCl for periods of five to10 minutes.
In no case of successful pulp capping did radi-ographs show teeth with furcation pathosis. Allrecall examinations showed complete apexogen-esis of previously immature apexes (Figures 2Fand 4F), consistent with a case study by Pateland Cohenca.55 Apexogenesis may indicate thecontinued normal physiological activity of cemen-toblasts and odontoblasts in the absence of irri-tants. Apical closure allows for more predictableendodontic treatment if teeth require pulpectomyat a later stage.
Investigators21 have reported calcification ofthe pulpal chamber and canal lumen in conjunc-tion with calcium hydroxide pulp capping and thepresence of tunnel defects in the reparative
dentin bridge. In our study, 89.8 percent (44/49) ofpulp caps showed no significant evidence of cal-cific changes in either the pulp or canal spaceswhen a direct pulp cap had been placed withMTA. A total of 10.2 percent (5/49) cases showedsome form of calcification or pulpal stone forma-tion. Although we noted this posttreatment com-plication, we determined that all five of theseteeth tested within normal limits to a cold stim-ulus. Teeth with larger multiple pulpal exposures(≥ 2.0 mm) tended to exhibit more aggressivereparative dentin formation and calcification ofthe pulp and canal lumens. Continued radi-ographic evaluation of these five cases did notreveal decreased lumen size in canals nor pro-gressive pulpal calcification after 18 to 24 months(Figure 4A-4D).
We noted reparative dentin formation in mostpatients examined at the one-year recall appoint-ment. Dentin bridge thicknesses varied from 0.5to 1.5 mm at the recall appointment, althoughradiographic angulations may have preventedprecise recognition of bridging. In two teeth, theoperator inadvertently forced MTA into thepulpal chamber, yet the pulpal reaction and out-come were favorable (Figure 5, page 314). Thepresence of MTA at the interface of pulpal tissue,which may be affected initially by the cariesprocess, most likely stimulates the release ofgrowth factors necessary for pulpal cells torecruit and organize odontoblasts to lay downreparative dentin.56 Odontoblastlike cells havethe potential to produce reparative dentin orregenerate pulpal tissue when they differentiateinto odontoblasts during reparative dentinogen-esis.7 The injured pulpal tissue below the MTAinterface should exhibit tissue healing character-ized by angiogenesis and neovascularization, andcell proliferation of functional cuboidal cells inproximity to the damaged area.57 During dentinformation, these cells are characterized by syn-thesis and secretion of multiple noncollagenousproteins on an extracellullar collagen matrix thateventually mineralizes in the absence of bacterialmicroleakage.
In clinical practice, dentists are required tomake a diagnosis for patients at the initial exami-nation, but too often that diagnosis is basedexclusively on patient report and radiographicinterpretation. Sometimes clinicians initiateendodontic therapy without performing adequatepulpal testing in patients who have deep cariesand a favorable prognosis for pulpal repair. When
R E S E A R C H
312 JADA, Vol. 139 http://jada.ada.org March 2008
Figure 3. Posttreatment radiograph of mineral trioxide aggregate(MTA), moist cotton pellet and unbonded Clearfil Photocore(Kuraray Medical, Okayama, Japan) interim restoration placedagainst the axial wall of a maxillary left second premolar in a 17-year-old girl.
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

sensibility testing, radiographic evaluations andpatient self-reports indicate a normal pulp or adiagnosis no more severe than reversible pulpitis,then the clinician should consider vital pulptherapy to be a viable alternative to conventionalendodontic treatment.
CONCLUSION
The use of MTA, enhanced magnification, cariesremoval using a caries detector dye, NaOCl hemo-stasis/disinfection, and a fifth-generationhydrophilic resin and composite is part of a reli-
R E S E A R C H
JADA, Vol. 139 http://jada.ada.org March 2008 313
Figure 4. Treatment sequence of molar that was symptomatic on presentation in a 7-year-old boy. A. Pretreatment radiograph showingopen apexes and deep caries. B. Arrows showing two large 2.0- to 2.5-millimeter pulp exposures after caries excavation and hemostasis. C. Gray mineral trioxide aggregate placed over the entire pulpal roof. D. Radiograph after provisionalization. E. Molar after permanentrestoration placement. F. Radiograph taken at the four-year, nine-month recall appointment showing extensive reparative bridge formation(arrow). Cold stimulus testing revealed a normal pulpal response.
A
C
E
B
D
F
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

able two-visit pulp-capping protocol for direct car-ious exposures when the pulpal diagnosis is nomore severe than irreversible pulpitis. Cliniciansshould be aware that the treatment described wasperformed by one operator; we cannot claim thatevery clinician will obtain similar results. Carefulattention to diagnostic criteria and treatment pro-cedures, however, should result in many suc-cessful outcomes. ■
Disclosure: None of the authors reported any disclosures.
The authors thank Dr. Mahmoud Torabinejad, director, AdvancedEducation in Endodontics, Loma Linda University, Calif., and Dr.Nicholas Chandler, associate professor, Department of Oral Rehabilita-tion, School of Dentistry, University of Otago, Dunedin, New Zealand,for their support and mentorship.
1. Tronstad L, Mjör IA. Capping of the inflamed pulp. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1972;34(3):477-485.
2. Langeland K. Management of the inflamed pulp associated withdeep carious lesion. J Endod 1981;7(4):169-181.
3. Bergenholtz G. Advances since the paper by Zander and Glass
(1949) on the pursuit of healing methods for pulpal exposures: histor-ical perspectives. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2005;100(2 suppl):S102-S108.
4. Al-Hiyasat AS, Barrieshi-Nusair KM, Al-Omari MA. The radi-ographic outcomes of direct pulp-capping procedures performed bydental students: a retrospective study. JADA 2006;137(12):1699-1705.
5. Ward J. Vital pulp therapy in cariously exposed permanent teethand its limitations. Aust Endod J 2002;28(1):29-37.
6. Moritz A, Schoop U, Goharkhay K, Sperr W. The CO2 laser as anaid in direct pulp capping. J Endod 1998;24(4):248-51.
7. Goldberg M, Six N, Decup F, et al. Bioactive molecules and thefuture of pulp therapy. Am J Dent 2003;16(1):66-76.
8. Dähnhardt JE, Jaeggi T, Lussi A. Treating open carious lesions inanxious children with ozone: a prospective controlled clinical study. AmJ Dent 2006;19(5):267-70.
9. Hørsted P, Søndergaard B, Thylstrup A, El Attar K, Fejerskov O. Aretrospective study of direct pulp capping with calcium hydroxide com-pounds. Endod Dent Traumatol 1985;1(1):29-34.
10. Baume LJ, Holz J. Long term clinical assessment of direct pulpcapping. Int Dent J 1981;31(4):251-260.
11. Barthel CR, Rosenkranz B, Leuenberg A, Roulet JF. Pulp cappingof carious exposures: treatment outcome after 5 and 10 years—a retro-spective study. J Endod 2000;26(9):525-8.
12. Auschill TM, Arweiler NB, Hellwig E, Zamani-Alaei A, Sculean A.Success rate of direct pulp capping with calcium hydroxide [inGerman]. Schweiz Monatsschr Zahnmed 2003;113(9):946-952.
13. Matsuo T, Nakanishi T, Shimizu H, Ebisu S. A clinical study ofdirect pulp capping applied to carious-exposed pulps. J Endod
R E S E A R C H
314 JADA, Vol. 139 http://jada.ada.org March 2008
A
C D
B
Figure 5. Treatment of molar with deep axial wall caries in 29-year-old female exhibiting a normal pulpal response to cold testing. A. Radi-ograph showing deep caries with no evidence of periradicular or furcation pathosis. B. Two exposures 1.0- to 1.5-millimeters to distal axialwall after excavation using caries detector and 5.25 percent sodium hypochlorite hemostasis (arrows). C. Posttreatment radiograph showingprovisional restoration with mineral trioxide aggregate extending into the pulp chamber. D. Radiograph taken at the seven-year, 10-monthrecall appointment showing normal periodontal ligament and anatomical structures with no visual evidence of dentin bridge formation. Themolar responded within normal limits to cold testing.
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from

1996;22(10):551-556.14. Hahn CL, Liewehr FR. Relationships between caries bacteria,
host responses, and clinical signs and symptoms of pulpitis. J Endod2007;33(3):213-219.
15. Fusayama T, Okuse K, Hosoda H. Relationship between hard-ness, discoloration, and microbial invasion in carious dentin. J DentRes 1966;45(4):1033-1046.
16. Fusayama T, Kurosaki N. Structure and removal of cariousdentin. Int Dent J 1972;22(3):401-411.
17. Sato Y, Fusayama T. Removal of dentin guided by fuchsinstaining. J Dent Res 1976:55(4):678-683.
18. Fusayama T. A Simple Pain-Free Adhesive Restorative System byMinimal Reduction and Total Etching. St. Louis: IshiyakuEuroAmerica; 1993:6-72.
19. Nakanishi T, Matsuo T, Ebisu S. Quantitative analysis ofimmunoglobulins and inflammatory factors in human pulpal bloodfrom exposed pulps. J Endod 1995;21(3):131-136.
20. Schröder U. Effect of calcium hydroxide-containing pulp-cappingagents on pulp cell migration, proliferation, and differentiation. J DentRes 1985;64(special number):541-548.
21. Cox CF, Sübay RK, Ostro E, Suzuki S, Suzuki SH. Tunnel defectsin dentin bridges: their formation following direct pulp capping. OperDent 1996;21(1):4-11.
22. Andelin WE, Shabahang S, Wright K, Torabinejad M. Identifica-tion of hard tissue after experimental pulp capping using dentin sialo-protein (DSP) as a marker. J Endod 2003;29(10):646-650.
23. Tarmin B, Hafez AA, Cox CF. Pulpal response to a resin-modifiedglass-ionomer material on nonexposed and exposed monkey pulps.Quintessence Int 1998;29(8):535-542.
24. Cox CF, Hafez AA, Akimoto N, Otsuki M, Suzuki S, Tarim B. Bio-compatibility of primer, adhesive and resin composite systems on non-exposed and exposed pulps of non-human primate teeth. Am J Dent1998;11(special number):S55-S63.
25. Hebling J, Giro EM, Costa CA. Biocompatibility of an adhesivesystem applied to exposed human dental pulp. J Endod 1999;25(10):676-682.
26. do Nascimento AB, Fontana UF, Teixeira HM, Costa CA. Biocom-patibility of a resin-modified glass-ionomer cement applied as pulp cap-ping in human teeth. Am J Dent 2000;13(1):28-34.
27. Mjör IA. Pulp-dentin biology in restorative dentistry, part 7: theexposed pulp. Quintessence Int 2002;33(2):113-135.
28. Accorinte Mde L, Loguericio AD, Reis A, Muench A, de AraújoVC. Adverse effects of human pulps after direct pulp capping with dif-ferent components from a total-etch, three-step adhesive system. DentMater 2005;21(7):599-607.
29. Olsson H, Petersson K, Rohlin M. Formation of a hard tissue bar-rier after pulp capping in humans: a systematic review. Int Endod J2006;39(6);429-442.
30. Murray PE, Hafez AA, Smith AJ, Cox CF. Hierarchy of pulp cap-ping and repair activities responsible for dentin bridge formation. Am JDent 2002;15(4):236-243.
31. Camilleri J, Pitt Ford TR. Mineral trioxide aggregate: a review ofthe constituents and biological properties of the material. Int Endod J2006;39(10):747-754.
32. Ford TR, Torabinejad M, Abedi HR, Bakland LK, KariyawasamSP. Using mineral trioxide aggregate as a pulp-capping material.JADA 1996;127(10):1491-1494.
33. Junn DJ. Quantitative assessment of dentin bridge formation fol-lowing pulp-capping with mineral trioxide aggregate (master’s thesis).Loma Linda, Calif.: Loma Linda University; 2000.
34. Sarkar NK, Caicedo R, Ritwik P, Moiseyeva R, Kawashima I.Physiochemical basis of the biologic properties of mineral trioxideaggregate. J Endod 2005;31(2):97-100.
35. Moghaddame-Jafari S, Mantellini MG, Botero TM, McDonald NJ,Nör JE. Effect of ProRoot MTA on pulp cell apoptosis and proliferationin vitro. J Endod 2005;31(5):387-391.
36. Takita T, Hayashi M, Takeichi O, et al. Effect of mineral trioxide
aggregate on proliferation of cultured human dental pulp cells. IntEndod J 2006;39(5):415-422.
37. Koh ET, Pitt Ford TR, Torabinejad M, McDonald F. Mineral tri-oxide aggregate stimulates a biological response in human osteoblasts.J Biomed Mater Res 1997;37(3):432-439.
38. Torabinejad M, Hong CU, McDonald F, Pitt Ford TR. Physicaland chemical properties of a new root-end filling material. J. Endod1995;21(7):349-353.
39. Aeinehchi M, Eslami B, Ghanbariha M, Saffar AS. Mineral tri-oxide aggregate (MTA) and calcium hydroxide as pulp-capping agentsin human teeth: a preliminary report. Int Endod J 2003;36(3):225-231.
40. Witherspoon DE, Small JC, Harris GZ. Mineral trioxide aggre-gate pulpotomies: a case series outcomes assessment. JADA 2006;137(5):610-8.
41. Barrieshi-Nusair KM, Qudeimat MA. A prospective clinical studyof mineral trioxide aggregate for partial pulpotomy in cariouslyexposed permanent teeth. J Endod 2006;32(8):731-735.
42. Iwamoto CE, Adachi E, Pameijer CH, Barnes D, Romberg EE,Jefferies S. Clinical and histological evaluation of white ProRoot MTAin direct pulp capping. Am J Dent 2006;19(2):85-90.
43. Farsi N, Alamoudi N, Balto K, Al Mushayt A. Clinical assessmentof mineral trioxide aggregate (MTA) as direct pulp capping in youngpermanent teeth. J Clin Pediatr Dent 2006;31(2);72-76.
44. Torabinejad M, Higa RK, McKendry DJ, Pitt Ford TR. Dyeleakage of four root end filling materials: effects of blood contamina-tion. J Endod 1994;20(4):159-163.
45. Tomson PL, Grover LM, Lumley PJ, Sloan AJ, Smith AJ, CooperPR. Dissolution of bio-active dentine matrix components by mineral tri-oxide aggregate. J Dent 2007;35(8):636-642.
46. Torabinejad M, Smith PW, Kettering JD, Pitt Ford TR. Compara-tive investigation of marginal adaptation of mineral trioxide aggregateand other commonly used root-end filling materials. J Endod 1995;21(6):295-299.
47. Goracci G, Mori G. Scaning electron microscopic evaluation ofresin-dentin and calcium hydroxide-dentin interface with resin com-posite restorations. Quintessence Int 1996;27(2):129-135.
48. Cox CF, Keall CL, Keall HJ, Ostro E, Bergenholtz G. Biocompati-bility of surface-sealed dental materials against exposed pulps. JProsth Dent 1987;57(1):1-8.
49. Bernick S, Nedelman C. Effect of aging on the human pulp. JEndod 1975;1(3):88-94.
50. Abou-Rass M. The stressed pulp condition: an endodontic-restorative diagnostic concept. J Prosthet Dent 1982;48(3):264-267.
51. Hafez AA, Cox CF, Tarim B, Otsuki M, Akimoto N. An in vivoevaluation of hemorrhage control using sodium hypochlorite and directcapping with a one- or two-component adhesive system in exposed non-human primate pulps. Quintessence Int 2002;33(4):261-272.
52. Heggers JP, Sazy JA, Stenberg BD, et al. Bactericidal and wound-healing properties of sodium hypochlorite solutions: the 1991 LindbergAward. J Burn Care Rehabil 1991;12(5):420-424.
53. Garcia-Godoy F, Murray PE. Systemic evaluation of varioushaemostatic agents following local application prior to direct pulp cap-ping. Braz J Oral Sci 2005;4(14):791-797.
54. Demir T, Cehreli ZC. Clinical and radiographic evaluation ofadhesive pulp capping in primary molars following hemostasis with1.25% sodium hypochlorite: 2-year results. Am J Dent 2007;20(3):182-188.
55. Patel R, Cohenca N. Maturogenesis of a cariously exposed imma-ture permanent tooth using MTA for direct pulp capping: a case report.Dent Traumatol 2006;22(6):328-333.
56. Guven G, Cehreli ZC, Ural A, Serdar MA, Basak F. Effect of min-eral trioxide aggregate cements on transforming growth factor ‚1 andbone morphogenetic protein production by human fibroblasts in vitro. JEndod 2007;33(4):447-450.
57. Durand SH, Romeas A, Couble ML, et al. Expression of the TGF-beta/BMP inhibitor EVI1 in human dental pulp cells. Arch Oral Biol2007;52(8):712-719.
R E S E A R C H
JADA, Vol. 139 http://jada.ada.org March 2008 315
Copyright © 2008 American Dental Association. All rights reserved.
on July 20, 2010 jada.ada.org
Dow
nloaded from