Embed Size (px)
Citation preview
DILI Caused by Immune Checkpoint Modulators Used to Treat Cancer
Cyril Konto, MD
Clinical Lead, Executive Director
Early Oncology Development & Clinical Research
Disclosure
• Current employee and shareholder of Pfizer
2
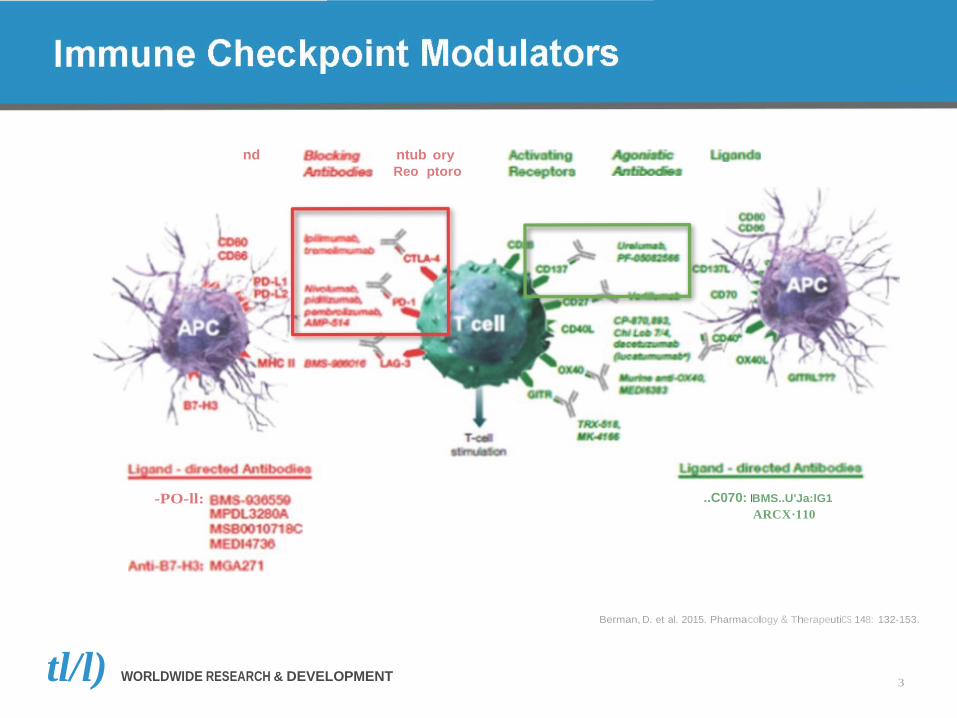
nd ntub ory Reo ptoro
-PO-ll: ..C070: IBMS..U'Ja:lG1 ARCX·110
Berman, D. et al. 2015. Pharmacology & TherapeutiCS 148: 132-153.
tl/l) WORLDWIDE RESEARCH & DEVELOPMENT 3

Immune Checkpoint Modulators in Advance Melanoma
so 40
:::
d
Thr NEW ENGLAND JOURNAL of MEDICINE
ORIGINAL ARTICLE
Nivolumab in Previously Untreated Melanoma without BRAF Mutation
Caroline Robert, M.D., Ph.D., Georgina V. Long, M.D., Ph.D., Benjamin Brady, M.D.,
Caroline Dutriaux, M.D., Michele Maio, M.D., Laurent Mortier, M.D., Jessica C. Hassel, M.D., Piotr Rutkowski, M.D., Ph.D., Catriona McNeil,M.D., Ph.D.,
Ewa Kalinka-Warzocha, M.D., Ph.D., Kerry J. Savage, M.D., Micaela M. Hernberg, M.D., Ph.D., Celeste Lebbe, M.D., Ph.D.,
Julie Charles, M.D., Ph.D., Catalin Mihalcioiu, M.D., Vanna Chiarion-Sileni, M.D., Cornelia Mauch, M.D., Ph.D., Francesco Cognetti, M.D.,Ana Arance, M.D., Ph.D.,
Henrik Schmidt, M.D., D.M.Sc., Dirk Schadendorf, M.D., Helen Gogas, M.D.,
Overall Survival
100
90
Hazard ratio for death, 0.42 (99.79% Cl, 0.25-0.73) P<0.001
Lotta Lundgren-Eriksson, M.D., Christine Horak, Ph.D., Brian Sharkey, Ph.D., ian M. Waxman, M.D., Victoria M4111.11111.D., and Paolo A. Ascierto, M.D. - 80
?ft. 70 bO
·s; 60 ·s;
llo.. ::::s
Cl) (I)
+-1 s:::: QJ "+I 30 cc.u.
20
10
0
Patients Who Died no.jtotal no.
Nivolumab 50/210 Dacarbazine 96/208
0 3 6 9
Median Survival
mo (95% Cl)
Not reached 10.8 (9.3-12.1)
12 15 18
Months
WORLDWIDE RESEARCH & DEVELOPMENT 4
Robert, C et al. (CheckMate 066) 2015. N Engl J Med 372: 320-330
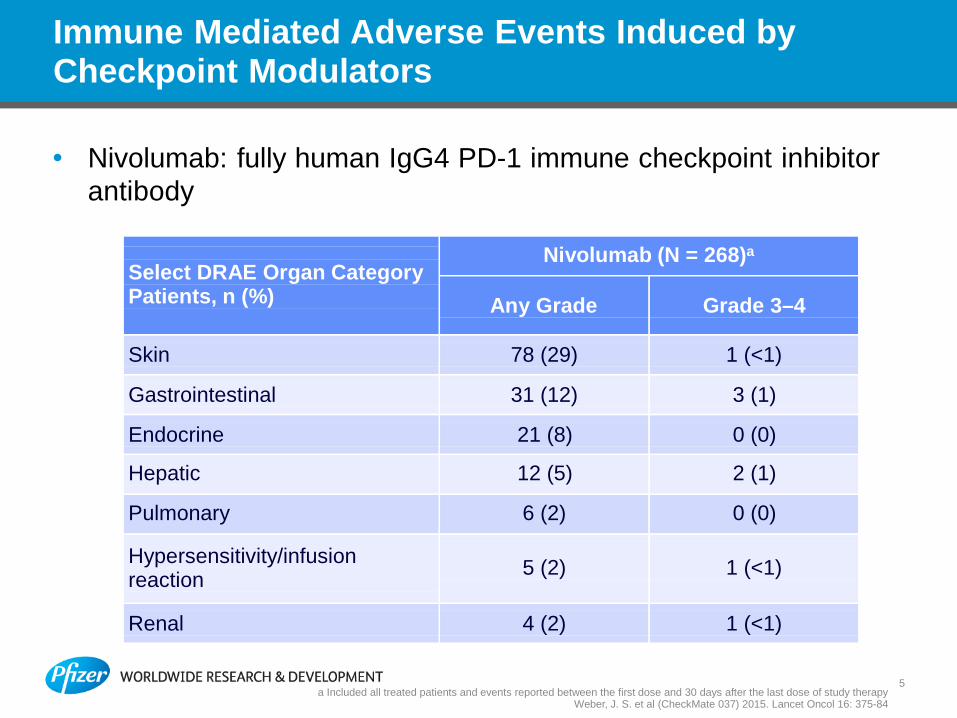
Immune Mediated Adverse Events Induced by Checkpoint Modulators
• Nivolumab: fully human IgG4 PD-1 immune checkpoint inhibitor antibody
Select DRAE Organ Category Patients, n (%)
Nivolumab (N = 268)a
Any Grade
Grade 3–4
Skin
78 (29)
1 (<1)
Gastrointestinal
31 (12)
3 (1)
Endocrine
21 (8)
0 (0)
Hepatic 12 (5) 2 (1)
Pulmonary 6 (2) 0 (0)
Hypersensitivity/infusion reaction
5 (2)
1 (<1)
Renal
4 (2)
1 (<1)
5 a Included all treated patients and events reported between the first dose and 30 days after the last dose of study therapy
Weber, J. S. et al (CheckMate 037) 2015. Lancet Oncol 16: 375-84
6
DILI due to Immune Checkpoint Modulators: Immune-Mediated Hepatitis
• Most frequently clinical diagnosis
– Few patients had liver biopsies (mainly with ipilimumab)
• Hepatitis defined by:
– LFT elevation after ruling out other etiologies
– Requiring corticosteroid therapy
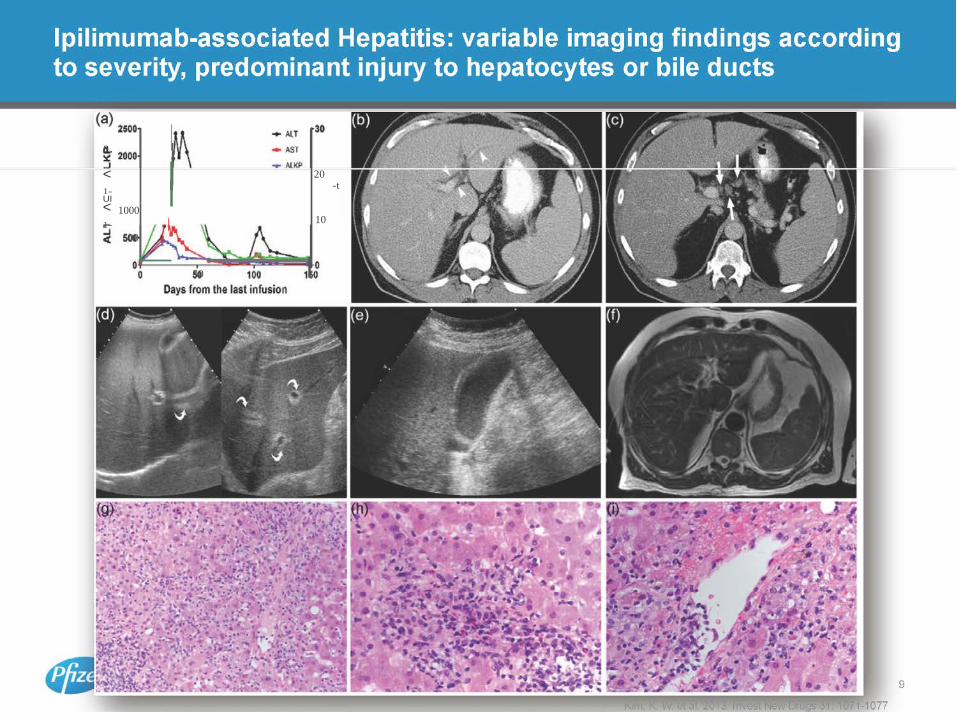
– Variable imaging findings according to clinical severity
– Mostly asymptomatic
– Rare clinical symptoms:
• General weakness, nausea/vomiting, dizziness
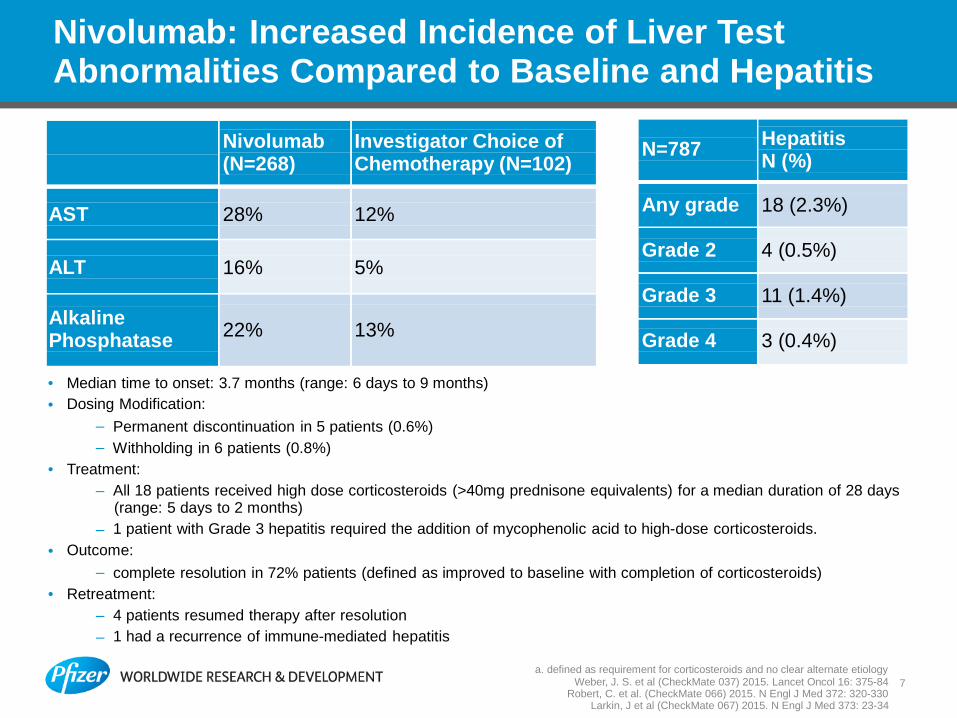
N=787
Hepatitis N (%)
Any grade
18 (2.3%)
Grade 2
4 (0.5%)
Grade 3
11 (1.4%)
Grade 4
3 (0.4%)
Nivolumab: Increased Incidence of Liver Test Abnormalities Compared to Baseline and Hepatitis
Nivolumab (N=268)
Investigator Choice of Chemotherapy (N=102)
AST
28%
12% ALT
16%
5%
Alkaline Phosphatase
22%
13%
• Median time to onset: 3.7 months (range: 6 days to 9 months) • Dosing Modification:
– Permanent discontinuation in 5 patients (0.6%) – Withholding in 6 patients (0.8%)
• Treatment: – All 18 patients received high dose corticosteroids (>40mg prednisone equivalents) for a median duration of 28 days
(range: 5 days to 2 months) – 1 patient with Grade 3 hepatitis required the addition of mycophenolic acid to high-dose corticosteroids.
• Outcome: – complete resolution in 72% patients (defined as improved to baseline with completion of corticosteroids)
• Retreatment: – 4 patients resumed therapy after resolution – 1 had a recurrence of immune-mediated hepatitis
a. defined as requirement for corticosteroids and no clear alternate etiology
Weber, J. S. et al (CheckMate 037) 2015. Lancet Oncol 16: 375-84 7 Robert, C. et al. (CheckMate 066) 2015. N Engl J Med 372: 320-330
Larkin, J et al (CheckMate 067) 2015. N Engl J Med 373: 23-34
8
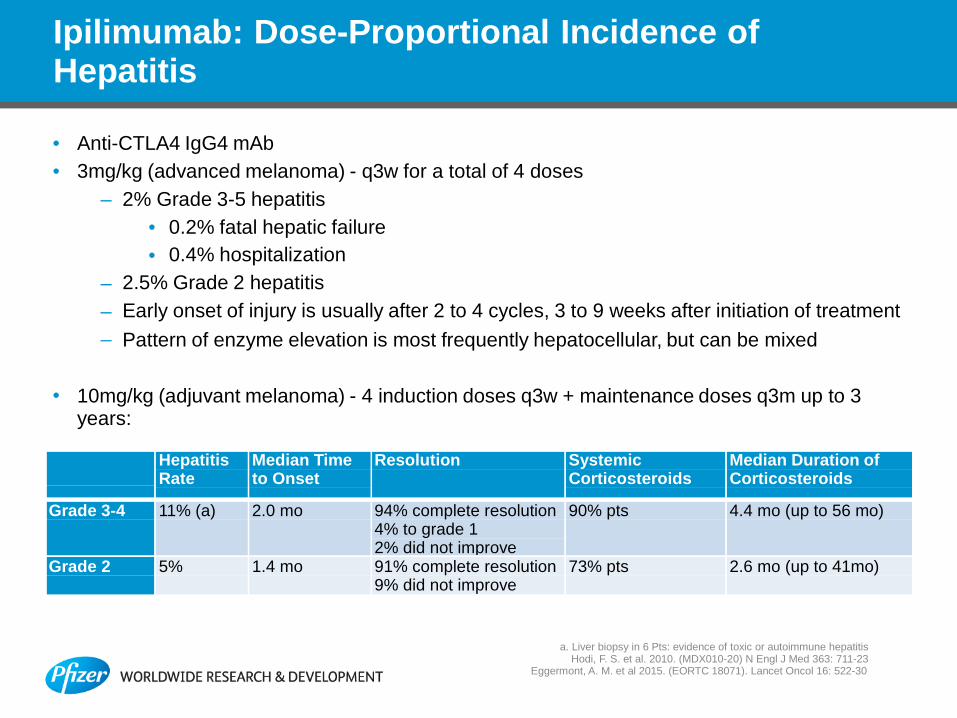
Ipilimumab: Dose-Proportional Incidence of Hepatitis
• Anti-CTLA4 IgG4 mAb • 3mg/kg (advanced melanoma) - q3w for a total of 4 doses
– 2% Grade 3-5 hepatitis • 0.2% fatal hepatic failure • 0.4% hospitalization
– 2.5% Grade 2 hepatitis – Early onset of injury is usually after 2 to 4 cycles, 3 to 9 weeks after initiation of treatment – Pattern of enzyme elevation is most frequently hepatocellular, but can be mixed
• 10mg/kg (adjuvant melanoma) - 4 induction doses q3w + maintenance doses q3m up to 3 years:
Hepatitis
Rate Median Time to Onset
Resolution Systemic Corticosteroids
Median Duration of Corticosteroids
Grade 3-4 11% (a) 2.0 mo 94% complete resolution 4% to grade 1 2% did not improve
90% pts 4.4 mo (up to 56 mo)
Grade 2 5% 1.4 mo 91% complete resolution 9% did not improve
73% pts 2.6 mo (up to 41mo)
a. Liver biopsy in 6 Pts: evidence of toxic or autoimmune hepatitis Hodi, F. S. et al. 2010. (MDX010-20) N Engl J Med 363: 711-23
Eggermont, A. M. et al 2015. (EORTC 18071). Lancet Oncol 16: 522-30
30
a. .J < 20
-t 1- Ul < 1000 1- 10
< 500
50
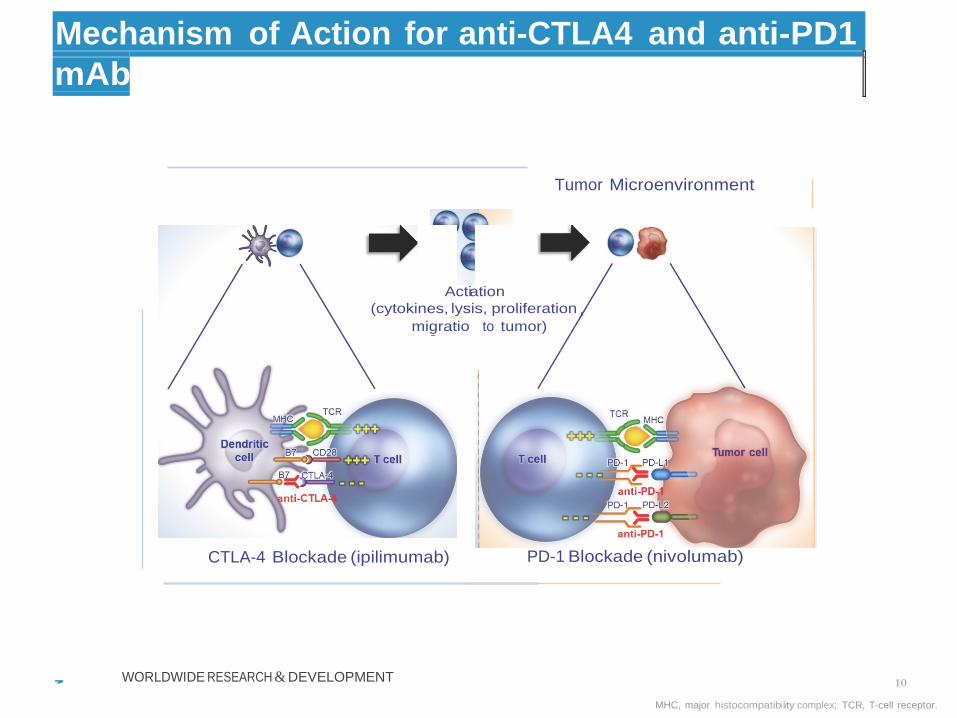
Mechanism of Action for anti-CTLA4 and anti-PD1 mAb
Tumor Microenvironment
Actiation (cytokines, lysis, proliferation
migratio to tumor)
CTLA-4 Blockade (ipilimumab) PD-1 Blockade (nivolumab) , WORLDWIDE RESEARCH & DEVELOPMENT 10
MHC, major histocompatibility complex; TCR, T-cell receptor.
208 192 178 108 105 98 88 80 76 74 63 50 31 24 9 210 195 181 142 134 123 112 106 105 96 88 79 42 36 13 202 183 166 82 72 59 44 39 35 31 26 22 12 8 3
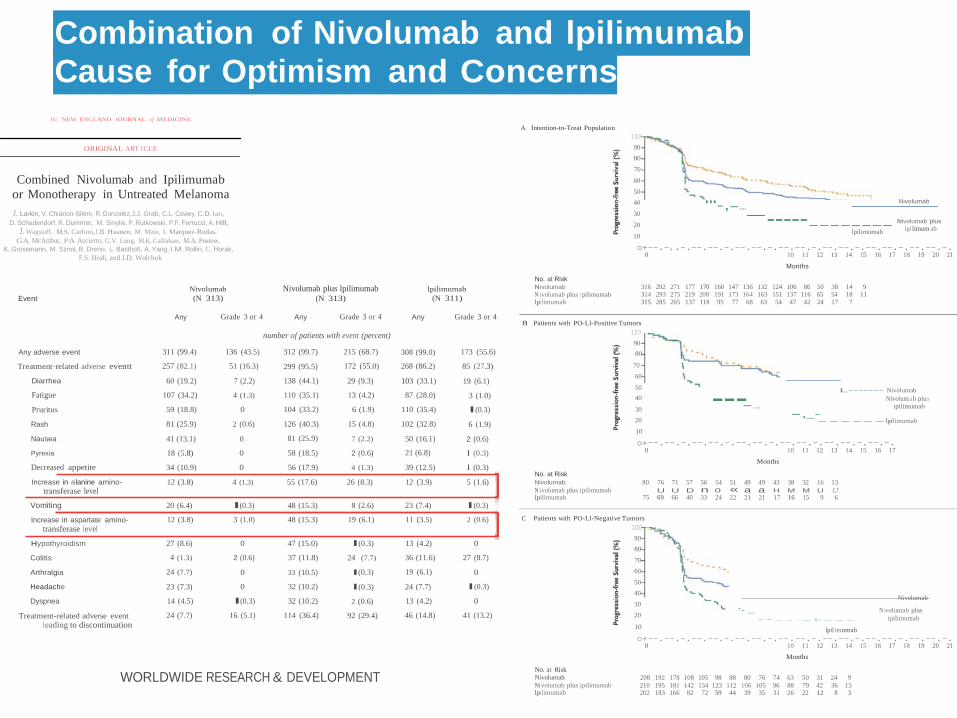
Combination of Nivolumab and lpilimumab Cause for Optimism and Concerns
Tht NEW ENGLAND JOURNAL of MEDICINE
ORIGINAL ART I CLE
Combined Nivolumab and Ipilimumab
or Monotherapy in Untreated Melanoma J. Larkin, V. Chiarion-Sileni, R. Gonzalez,J.J. Grab, C.L. Cowey, C.D. lao,
D. Schadendorf, R. Dummer, M. Smylie, P. Rutkowski, P.F. Ferrucci, A. Hill,
A Intention-to-Treat Population
100
90 80
70
60
50 40
30
20
'"-,-....
Nivolumab
------------- Nivolumab plus
J. Wagstaff, M.S. Carlino,J.B. Haanen, M. Maio, I. Marquez-Rodas, GA McArthur, PA Ascierto, G.V. Long, M.K. Callahan, M.A. Postow,
10 lpilimumab ipi limum ab
K. Grossmann, M. Sznol, B. Dreno, L. Bastholt, A. Yang, l.M. Rollin, C. Horak, o+--.-,.-.--.--.-.--.--.-.--.--.-.--.--.-.--.--.-.--.--.-. F.S. Hodi, and J.D. Wolchok 0
No. at Risk
10 11 12 13 14 15 16 17 18 19 20 21
Months
Event
Nivolumab (N 313)
Nivolumab plus lpilimumab (N 313)
lpilimumab (N 311)
Nivolumab N ivolumab plus i pilimumab lpil imumab
316 292 271 177 170 160 147 136 132 124 106 86 50 38 314 293 275 219 208 191 173 164 163 151 137 116 65 54 315 285 265 137 118 95 77 68 63 54 47 42 24 17
14 9 18 11 7
Any Grade 3 or 4
Any Grade 3 or 4
Any Grade 3 or 4
8 Patients with PO-Ll-Positive Tumors
number of patients with event (percent) 100
90 Any adverse event
Treatment·related adverse eventt
Diarrhea
Fatigue
Pruritus
311 (99.4)
257 (82.1)
60 (19.2)
107 (34.2)
59 (18.8)
136 (43.5)
51 (16.3)
7 (2.2)
4 (1.3)
0
312 (99.7)
299 (95.5)
138 (44.1)
110 (35.1)
104 (33.2)
215 (68.7)
172 (55.0)
29 (9.3)
13 (4.2)
6 (1.9)
308 (99.0)
268 (86.2)
103 (33.1)
87 (28.0)
110 (35.4)
173 (55.6) 80
85 (27.3) 70 60
19 (6.1) 50
3 (1.0) 40
l(0.3) 30
---- .... - ,_-
L------- Nivolumab
Nivolum a b plus ipilimumab
Rash 81 (25.9) 2 (0.6) 126 (40.3) 15 (4.8) 102 (32.8) 6 (1.9) 20 10
- - - - - - lpil imumab
Nausea 41 (13.1) 0 81 (25.9) 7 (2.2) 50 (16.1) 2 (0.6) o+--.--.-.--.--.-.--.--.-.--.--.-.--.--.-.--.-. Pyrexia
Decreased appetite
18 (5.8) 0
34 (10.9) 0
58 (18.5)
56 (17.9)
2 (0.6)
4 (1.3)
21 (6.8)
39 (12.5)
l (0.3)
l (0.3)
0
No. at Risk
Months
10 11 12 13 14 15 16 17
Increase in alanine amino- transferase level
12 (3.8) 4 (1.3) 55 (17.6) 26 (8.3) 12 (3.9) 5 (1.6) Nivolumab N ivolumab plus ipilimumab lpilimumab
80 76 71 57 56 54 51 49 49 43 38 32 16 13 U U D n 0 « a a H M M U U
75 69 66 40 33 24 22 21 21 17 16 15 9 6 Vomiting 20 (6.4) l(0.3) 48 (15.3) 8 (2.6) 23 (7.4) l(0.3)
Increase in aspartate amino- transferase level
Hypothyroidism
Colitis
Arthralgia
Headache
Dyspnea
Treatment-related adverse event l eading to discontinuation
12 (3.8)
27 (8.6)
4 (1.3)
24 (7.7)
23 (7.3)
14 (4.5)
24 (7.7)
3 (1.0)
0
2 (0.6)
0
0
l(0.3)
16 (5.1)
48 (15.3)
47 (15.0)
37 (11.8)
33 (10.5)
32 (10.2)
32 (10.2)
114 (36.4)
19 (6.1)
l(0.3)
24 (7.7)
l(0.3)
l(0.3)
2 (0.6)
92 (29.4)
11 (3.5)
13 (4.2)
36 (11.6)
19 (6.1)
24 (7.7)
13 (4.2)
46 (14.8)
2 (0.6)
0
27 (8.7)
0
l(0.3)
0
41 (13.2)
C Patients with PO-Ll-Negative Tumors 100
90 80
70 60
50 40
30 20
10
Nivolumab
'- _ N ivolumab plus - - ..._ ._ .... _ L- _ _ _ ipilimumab
lpil im umab o+--.--.-.--.--.-.--.--.-.--.--.-.--.--.-.--.--.-.--.--.-.
WORLDWIDE RESEARCH & DEVELOPMENT
0
No. at Risk Nivolumab Ni volumab plus ipilimumab lpil imumab
10 11 12 13 14 15 16 17 18 19 20 21
Months
12
Larkin, J et al (CheckMate 067) 2015. N Engl J Med 373: 23-34
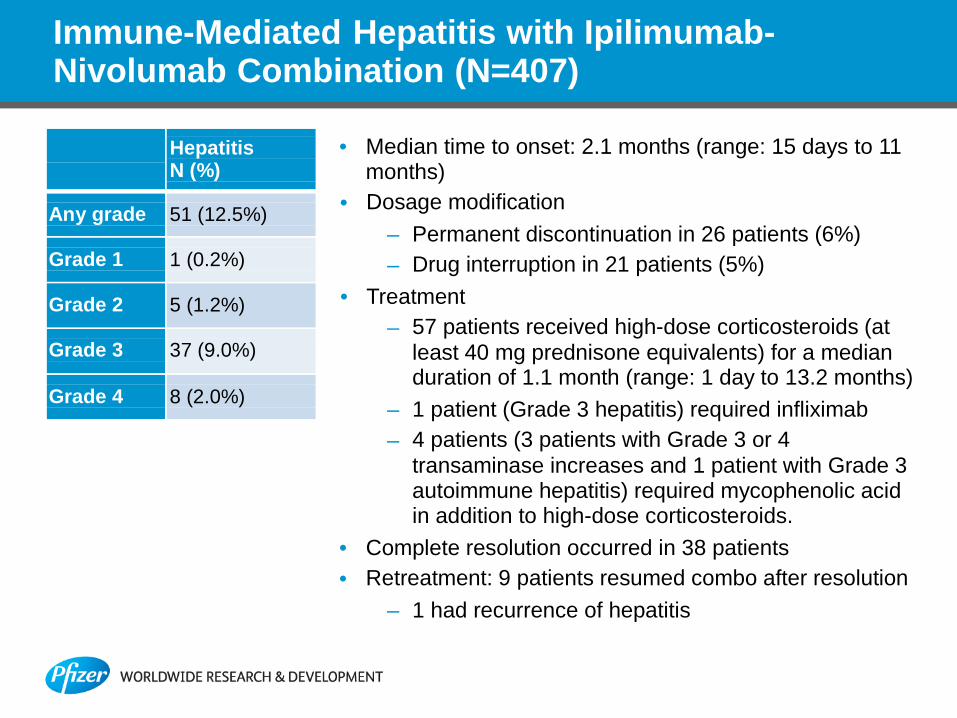
Hepatitis N (%)
Any grade
51 (12.5%)
Grade 1
1 (0.2%)
Grade 2
5 (1.2%)
Grade 3
37 (9.0%)
Grade 4
8 (2.0%)
Immune-Mediated Hepatitis with Ipilimumab- Nivolumab Combination (N=407)
• Median time to onset: 2.1 months (range: 15 days to 11 months)
• Dosage modification – Permanent discontinuation in 26 patients (6%) – Drug interruption in 21 patients (5%)
• Treatment – 57 patients received high-dose corticosteroids (at
least 40 mg prednisone equivalents) for a median duration of 1.1 month (range: 1 day to 13.2 months)
– 1 patient (Grade 3 hepatitis) required infliximab – 4 patients (3 patients with Grade 3 or 4
transaminase increases and 1 patient with Grade 3 autoimmune hepatitis) required mycophenolic acid in addition to high-dose corticosteroids.
• Complete resolution occurred in 38 patients • Retreatment: 9 patients resumed combo after resolution
– 1 had recurrence of hepatitis

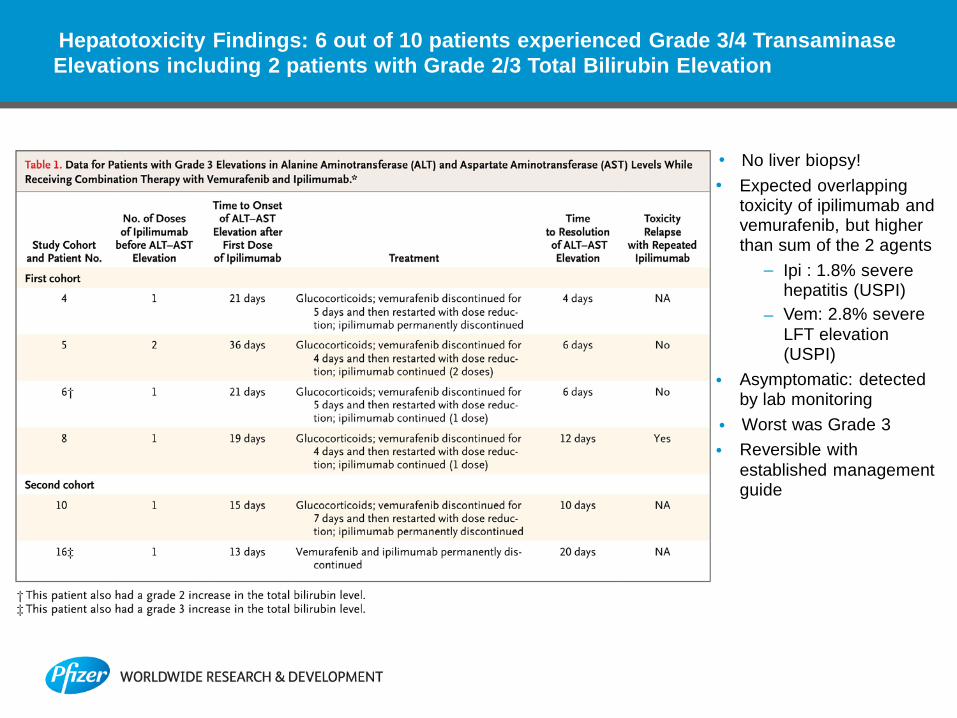
Combination of Ipilimumab and Vemurafenib Synergistic Liver Toxicity Resulting in Phase 1 Study Termination
Ipilimumab
Induction phase q3w x 4
Maintenance phase q3m
D1 D22 D43 Vemurafenib lead-
in phase
D64
D85 D162
D-27 Vemurafenib bid continuous dosing
• Phase 1 primary objective: MTD • Vemurafenib lead-in phase for 4 weeks prior to start ipilimumab • DLT observation period during the combo phase only • 3+3 patients treated in cohort 1 • 3+3 patients treated in cohort -1A
13
14
Ribas, A. et al. 2013. N Engl J Med 368: 1365-1366
Hepatotoxicity Findings: 6 out of 10 patients experienced Grade 3/4 Transaminase Elevations including 2 patients with Grade 2/3 Total Bilirubin Elevation
• No liver biopsy! • Expected overlapping
toxicity of ipilimumab and vemurafenib, but higher than sum of the 2 agents
– Ipi : 1.8% severe hepatitis (USPI)
– Vem: 2.8% severe LFT elevation (USPI)
• Asymptomatic: detected by lab monitoring
• Worst was Grade 3 • Reversible with
established management guide
4-1BB and Urelumab • CD137 (4-1BB or TNFRSF9), TNF superfamily Type 1 membrane glycoprotein receptor
expressed on the surface of lymphoid organs and detected on activated T cells (CD4+ and CD8+), activated NK cells, NKT cells, Tregs, and others.
• Natural ligand: CD137L, a TNF superfamily Type II membrane glycoprotein – Expressed on activated T cells, macrophages, monocytes, DCs and B Cells – Enhance the ability of CD137+ DCs to potentiate T cell responsiveness to alloantigens – May augment T cell trafficking into tumors via CD137 expression on tumor-associated
endothelial cells • Urelumab (BMS-663513): First agonistic anti CD137 fully human IgG4 mAb non blocking
CD137L.
• Non-clin Toxicology: Administration of surrogate BMS-469492 at doses of 10 or 50 mg/kg twice weekly for 4 weeks to CD-1 mice resulted in skin and liver toxicity / Monkey studies showed good tolerability
• Hepatotoxicity, was the most frequent clinically important toxicity in clinic – Occurrence and severity increased from 1 mg/kg – 2 fatal cases of drug-related hepatotoxicity at 1 and 5 mg/kg q3w on study CA186006
responsible for clinical hold
• Most frequent grade 2+ laboratory abnormalities were increases in ALT (15%) and AST (12%), N=106
• Most recent clinical trials conducted at < 1 mg/kg q3w. • Anti-tumor activity as well as PD activity observed across a wide dose range (0.1 to 10mg/kg)
Li, S. Y. & Liu, Y. 2013. Clin Pharmacol 5: 47-53
Sanmamed, M. F. et al. 2015. Semin Oncol 42: 640-55 15 Ascierto, P. A. et al. 2010. Semin Oncol 37: 508-16
16
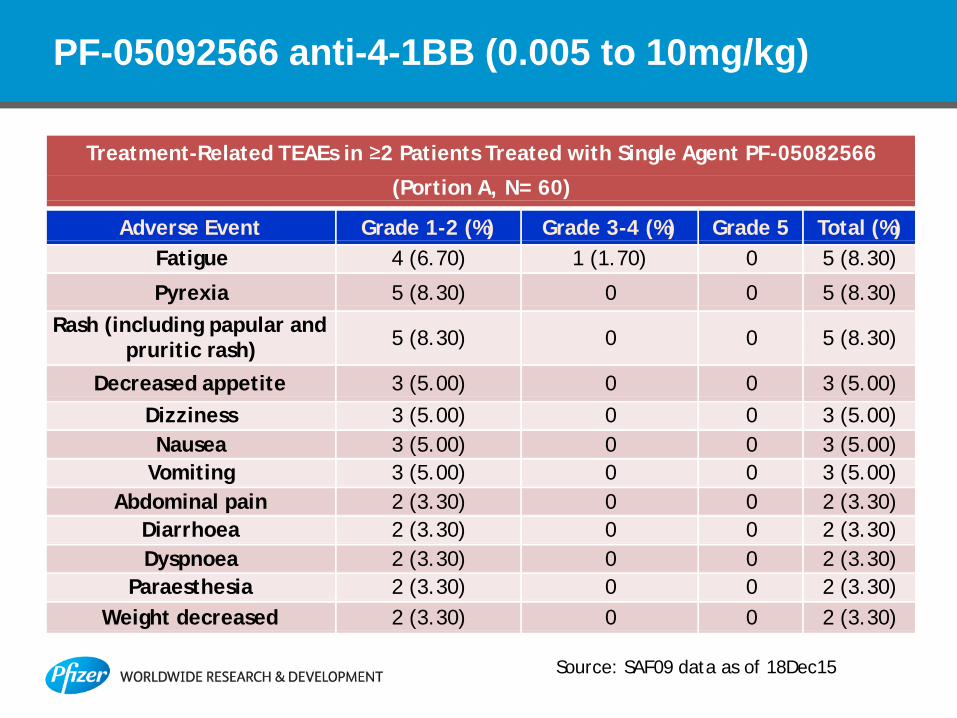
PF-05092566 anti-4-1BB (0.005 to 10mg/kg)
Treatment-Related TEAEs in ≥2 Patients Treated with Single Agent PF-05082566
(Portion A, N= 60)
Adverse Event Grade 1-2 (%) Grade 3-4 (%) Grade 5 Total (%) Fatigue 4 (6.70) 1 (1.70) 0 5 (8.30)
Pyrexia
5 (8.30)
0
0
5 (8.30) Rash (including papular and
pruritic rash)
5 (8.30)
0
0
5 (8.30)
Decreased appetite 3 (5.00) 0 0 3 (5.00) Dizziness 3 (5.00) 0 0 3 (5.00) Nausea 3 (5.00) 0 0 3 (5.00)
Vomiting 3 (5.00) 0 0 3 (5.00) Abdominal pain 2 (3.30) 0 0 2 (3.30)
Diarrhoea 2 (3.30) 0 0 2 (3.30) Dyspnoea 2 (3.30) 0 0 2 (3.30)
Paraesthesia 2 (3.30) 0 0 2 (3.30) Weight decreased 2 (3.30) 0 0 2 (3.30)
Source: SAF09 data as of 18Dec15
17
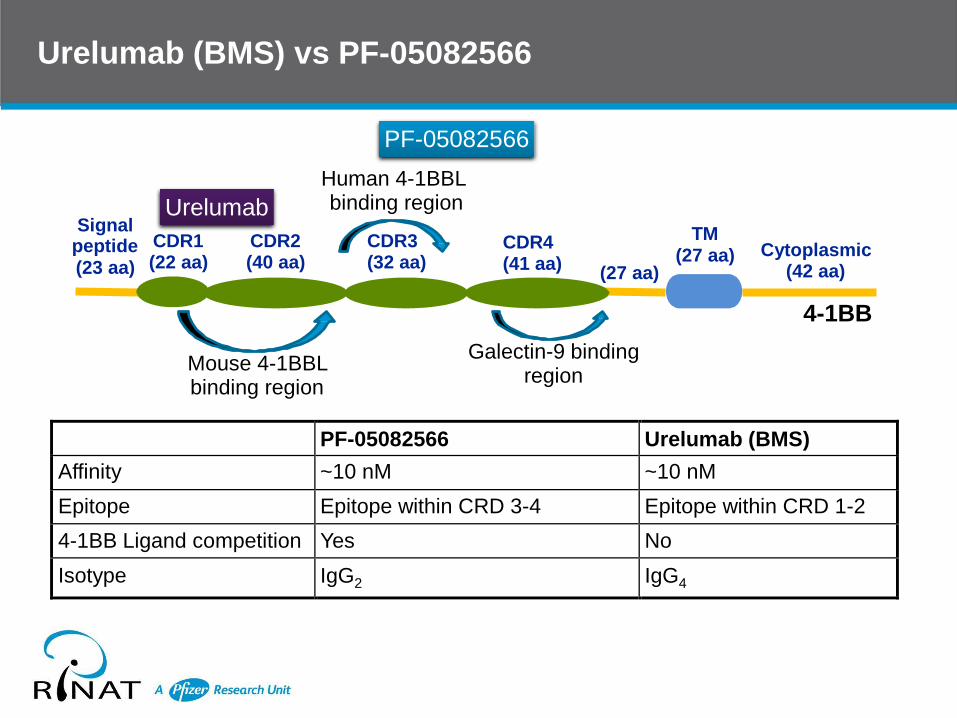
Urelumab (BMS) vs PF-05082566
Urelumab
PF-05082566
Human 4-1BBL binding region
Signal peptide
CDR1 (22 aa)
CDR2 (40 aa)
CDR3 (32 aa)
CDR4 (41 aa)
TM (27 aa) Cytoplasmic
(23 aa) (27 aa) (42 aa)
4-1BB
Mouse 4-1BBL binding region
Galectin-9 binding region
PF-05082566 Urelumab (BMS) Affinity ~10 nM ~10 nM Epitope Epitope within CRD 3-4 Epitope within CRD 1-2 4-1BB Ligand competition Yes No Isotype IgG2 IgG4

18
Key Elements of Safety Management for Liver Toxicity
• Monitor patients for abnormal liver tests prior to and periodically during treatment
• Rule out other etiologies rapidly
• Administer corticosteroids promptly at a dose of
– 0.5-1 mg/kg/day prednisone equivalents for moderate transaminase elevations, with or without concomitant elevation in total bilirubin
– 1-2 mg/kg/day prednisone equivalents for Grade 3-4 transaminase elevations, with or without concomitant elevation in total bilirubin
– Taper off over a minimum of 4 weeks
• Withhold therapy for moderate hepatitis
• Permanently discontinue for Grade 3-4 hepatitis
• In case of severe steroid-refractory hepatitis, use immunosuppressive agents (mycophenol acid)
– Anti-TNF Infliximab responsible for acute liver failure and hepatitis
19
Take Home Messages
• Benefit of immune checkpoint modulators outweighs the risks
• Mild-to-moderate serum aminotransferase elevations are common during anti-CTLA4 and anti-PD1 therapies
• Asymptomatic DILI, detected by frequent LFT monitoring
• Most frequently hepatocellular pattern of enzyme elevation, but can be mixed, particularly at the onset of injury
• Severe hepatitis in 2-10% of patients depending on checkpoint, dose and combination
• Early onset of injury (usually 3 to 15 weeks after initiation of treatment)
• Immune mediated hepatitis with focal or confluent necrosis and prominent lymphocytic infiltrates of activated T cells
• Corticosteroids are the main treatment, often successful





























