Embed Size (px)
Citation preview

C
D
NSa
b
c
d
e
f
a
ARA
1
nppcsic
2
whoottfa
s(no
aA
0d
Leukemia Research 36 (2012) 521– 523
Contents lists available at SciVerse ScienceDirect
Leukemia Research
jo ur nal homep age: www.elsev ier .com/ locate / leukres
ase of the Month
ifferential diagnosis of paediatric bone pain: Acute lymphoblastic leukemia
icolien van der Havea,b, Shriram Vaidia Nathc,d, Colin Storye, Heather Tappb,e, C. Nicola f,arah Mooree, Rosemary Suttonf, Tamas Reveszb,d,e,∗
Radboud University, Nijmegen, The NetherlandsWomen’s and Children’s Hospital, Adelaide, AustraliaWomen’s and Children’s Research Institute, Adelaide, AustraliaDepartment of Haematology Oncology, University of Adelaide, Adelaide, AustraliaSA Pathology, Adelaide, AustraliaChildren’s Cancer Institute Australia, Lowy Cancer Research Centre, UNSW, Sydney, Australia
r t i c l e i n f o
rticle history:eceived 9 September 2011
vailable online 28 January 2012. Introduction
Acute lymphoblastic leukemia (ALL) is the commonest malig-ancy in childhood. While most patients with ALL present withallor or bleeding signs, some present with localized or diffuse boneains and these patients often have relatively normal full bloodounts (FBC) and a lower incidence of organomegaly [1,2]. It is pre-umed that the bone pain is caused by leukemic cells infiltrating thentramedullary bone marrow space [3]. This form of presentationan lead to delays in the diagnosis of ALL.
. Case report
In November 2005, an 11-year-old boy was admitted to hospitalith a history of left knee pain and limp of 3 months duration. Head headaches with recent onset of night sweats and a weight lossf 5 kg. On examination he had no pallor or lymphadenopathy, norganomegaly or rash. Plain X-ray revealed a subtle lucency withinhe left ilium. A bone scan showed multifocal increased uptake inhe left femur and patella with possible involvement of the leftemoral head and ischium. MRI investigations were indicative ofn infiltrative process in the pelvis and femora.
Results of the patient’s initial and subsequent investigations arehown in Table 1. Blood cultures were negative. A bone marrow
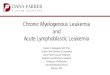
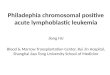
BM) aspirate and BM trephine collected from the iliac crest showedormal trilineage haematopoiesis (Fig. 1a). A working diagnosisf chronic relapsing multifocal osteomyelitis was reached, based∗ Corresponding author at: Department of Haematology Oncology, SA Pathologyt Women’s and Children’s Hospital, 72, King William’s Road, North Adelaide 5006,ustralia. Tel.: +61 8 8161 7327; fax: +61 8 8161 6567.
E-mail address: [email protected] (T. Revesz).
145-2126/$ – see front matter. Crown Copyright © 2012 Published by Elsevier Ltd. All rioi:10.1016/j.leukres.2012.01.001
on his clinical symptoms, radiological findings and a normal bonemarrow. He was treated with Piroxicam. A good response to thistherapy was observed with resolution of symptoms and weightgain.
Four months later he developed high fever, night sweats, chestpain and left ankle pain. A bone scan showed new lesions in the righttrapezoid bone and right acetabulum. Interestingly, the lesionsfrom November appeared to have resolved. Blood investigationswere unremarkable (Table 1). Again, his condition improved onPiroxicam.
He was discharged but within a fortnight developed lethargy,pallor, high fevers, drenching night sweats, a dry cough, epistaxisand bruising. He had lost 2 kg in weight. On examination he wasfebrile and pale with inguinal lymphadenopathy, hepatomegalyand splenomegaly (both 5 cm below costal margin). His blood countdemonstrated pancytopenia with 22% circulating blasts (Table 1).BM aspiration and trephine biopsy confirmed the diagnosis of BCPALL (Fig. 1b). Cytogenetic analysis of the leukaemic blasts showedthe chromosomal translocation t(1;19), confirmed by reverse tran-scriptase (RT)-PCR for the E2A-PBX1 fusion gene transcript. PCRbased tests to detect the common rearrangements in antigen recep-tor genes present in ALL were conducted as described previously [4]and revealed specific clonal sequences involving the immunoglob-ulin heavy chain IGH (Vh3-Dh3-Jh4) and T-cell receptor delta TRD(Vd2–Dd3) genes in the ALL diagnostic sample. The patient wastreated according to the BFM-based Australian and New ZealandChildren’s Haematology and Oncology Group Study 8 protocol. Hehad a good prednisolone response on day 8 and a BM aspirateafter 4 weeks of induction therapy showed both morphological
and cytogenetic remission. Minimal residual disease (MRD) mea-surements were carried out by real-time quantitative (RQ)-PCR onDNA isolated from bone marrow aspirates on days 33 and day 79of therapy as part of the stratification process [5]. The Taqmanghts reserved.

522 N. van der Have et al. / Leukemia Research 36 (2012) 521– 523
Table 1Laboratory findings 5 months prior to and at the time of diagnosis.
Parameters (normal values) 1st presentation November2005
2nd presentationFebruary 2006
At diagnosis March 2006
Hb (115–155 g/L) 112 156 85Platelets (150–450 × 109/L 491 484 34WCC (5–11 × 109/L) 11.0 16.3 3.4Neutrophils (1.5–8 × 109/L) 6.0 10.1 0.4Lymphocytes (1.5–7 × 109/L) 2.7 4.2 1.6Blasts in blood (×109/L) 0 0 0.7CRP (<11) 22 14 79ESR (<15 mm/h) 38 13 91Peripheral blood film morphology Mild thrombocytosis Normal Blast cells with high
nuclear: cytoplasmaticratio. No Auer Rods
Bone marrow morphology Tri-lineagehaematopoiesis, noleukaemic blasts
Not performed 92% blasts with L1morphology, no Auer Rods
Flow-cytometry Not performed Not performed CD10, CD19, CD22, CD9,HLA-DR, CD45 positive
Cytogenetics and FISH Performed retrospectively:t(1;19) negative
Not performed t(1;19)
MRD Performed retrospectively:t <0.0
Not performed 100%
prsbsuws
Fs2
positive a
robes used for MRD analysis were specific for the IGH junctionalegion (JH1245) [6] and the second variable TRD segment (Vd2equence AGGTGACATTGATATTGCAAAGAACCTGGC) and in com-ination with primers for the specific rearrangement both gaveensitive MRD tests with a quantitative range of 10−4 [7]. MRD was
ndetectable for both time points for the two sensitive markers,hich together with clinical features resulted in his assessment astandard risk patient. He continued and completed the standard
ig. 1. (A). Bone marrow trephine November 2005 (H&E 40×) showing normal trilineaghowing normal maturation (C). Bone marrow trephine March 2006 (H&E 40×) showing006 (40×) showing a uniform population of small and medium-sized blasts with a high
1%
control arm of the protocol in March 2008. Since that time he hasbeen reviewed regularly in our outpatient clinic and remains incomplete remission.
In our review of this case, retrospective analyses of the BM slidesfrom the initial presentation were conducted to determine if sen-
sitive molecular tests could have been used to make an earlierdiagnosis. These BM slides collected 5 months before the ALL diag-nosis, failed to show the presence of the t(1;19) when tested usinge haematopoiesis and cellularity (B). Bone marrow aspirate November 2005 (10×) dense lymphoblastic infiltration of the marrow (D). Bone marrow aspirate Marchnucleocytoplasmic ratio (arrow pointing to typical small lymphoblast).

mia R
flml
3
bl[aTBrh
i[obmpprds
oocnstrimcaaotd
[
[
[
[
[
[
[
N. van der Have et al. / Leuke
uorescent in situ hybridization (FISH). In contrast, both of the MRDarkers were detected by RQ-PCR in the BM slide DNA, albeit at low
evels of less than 10−4 (<0.01%).
. Discussion
Our patient initially presented with severe bone pain and limput no organomegaly and a normal FBC. There are reports in the
iterature of such patients with the associated ‘delays’ in diagnosis1]. Due to the high suspicion of ALL at initial presentation, a BMspiration was performed but did not demonstrate any blast cells.he retrospective demonstration of low-level MRD in the originalM preparation raises the issue of ‘patchy’ changes in the BM. Earlyeports from the 1970s seem to support this but the phenomenonas never been extensively investigated.
The prognostic significance of bone pain or skeletal involvementn ALL may have changed with more intensive therapy over time2]. We retrospectively studied 119 children with ALL over a periodf 10 years and found no significant prognostic significance ofone pain at diagnosis (unpublished results). There is sparse infor-ation in the literature about the biology of leukemia with such
resentation. Maman et al. speculated that the leukemia in suchatients may have a greater propensity to remain in the bone mar-ow [3]. If steroids are started for these patients with the mistakeniagnosis of an autoimmune disorder, it can reduce the chance ofurvival [8].
This case illustrates the difficulty of diagnosing ALL in this subsetf patients. In our patient, the bone marrow did not show any obvi-us blasts on morphology at initial presentation (Fig. 1a). Hence,ytogenetic tests capable of detecting 1 leukemia cell among 102
ormal cells, were not performed. Even though FISH increases theensitivity up to 1 in 103 to 104, the t(1;19) was not detected onhe BM slide of the initial presentation even when performed ret-ospectively. Routine PCR for antigen receptor genes would also bensufficient to detect clonal rearrangements below 1 in 102 nor-
al cells. RQ-PCR MRD tests with sensitivity to detect 1 leukemiaell among 105 normal cells did show the presence of both IGHnd TRD specific rearrangements at very low levels (<1 × 10−4)
ssociated with his ALL. However, that analysis was dependentn the retrospective knowledge of the patient-specific MRD signa-ure which would not have been possible at the time of the initialiagnosis.[
esearch 36 (2012) 521– 523 523
This case challenges the view that sensitive molecular testing ofbone marrow samples for leukemic markers is useful in the diagno-sis of musculoskeletal manifestations. Differential diagnosis of ALLin these cases can be difficult probably due to patchy distributionand slow growth of the leukemia. These patients clearly requireregular clinical follow up with or without bone marrow aspiratesor trephines.
In our case the blood count became abnormal 5 months afterthe initial presentation and it was only then that we were able todiagnose ALL morphologically. He is currently in ongoing clinicaland morphological remission 6 years from initial diagnosis. The‘delay’ in diagnosis appears not to have impacted on his survival.
Acknowledgement
The authors declare no financial support or conflict of interest.Contributions. All authors contributed to either collecting and
analysing clinical data or to laboratory analyses. All authors con-tributed to the writing and revision of the manuscript.
References
1] Jonsson OG, Sartain P, Ducore JM, Buchanan GR. Bone pain as an initial symp-tom of childhood acute lymphoblastic leukemia: association with nearly normalhematologic indexes. J Pediatr 1990;117(2 Pt 1):233–7.
2] Revesz T, Kardos G, Kajtar P, Schuler D. The prognostic significance of bone andjoint manifestations in childhood leukemia. J Rheumatol 1985;12(3):647–8.
3] Maman E, Steinberg DM, Stark B, Izraeli S, Wientroub S. Acute lymphoblas-tic leukemia in children: correlation of musculoskeletal manifestations andimmunophenotypes. J Child Orthop 2007;1(1):63–8.
4] Sutton R, Venn NC, Tolisano J, Bahar AY, Giles JE, Ashton LJ, et al. Clinical sig-nificance of minimal residual disease at day 15 and at the end of therapy inchildhood acute lymphoblastic leukaemia. Br J Haematol 2009;146(3):292–9.
5] Flohr T, Schrauder A, Cazzaniga G, Panzer-Grumayer R, van der Velden V, Fis-cher S, et al. Minimal residual disease-directed risk stratification using real-timequantitative PCR analysis of immunoglobulin and T-cell receptor gene rear-rangements in the international multicenter trial AIEOP-BFM ALL 2000 forchildhood acute lymphoblastic leukemia. Leukemia 2008;22(4):771–82.
6] Sutton R, Bahar AY, Kwan E, Giles JE, Venn NC, Tran S, et al. Improving minimalresidual disease detection in precursor B-ALL based on immunoglobulin-kappaand heavy-chain gene rearrangements. Leukemia 2008;22(12):2265–7.
7] van der Velden VH, Cazzaniga G, Schrauder A, Hancock J, Bader P, Panzer-Grumayer ER, et al. Analysis of minimal residual disease by Ig/TCR gene
rearrangements: guidelines for interpretation of real-time quantitative PCR data.Leukemia 2007;21(4):604–11.8] Revesz T, Kardos G, Kajtar P, Schuler D. The adverse effect of prolonged pred-nisolone pretreatment in children with acute lymphoblastic leukemia. Cancer1985;55(8):1637–40.