Embed Size (px)
Citation preview

Ann. N.Y. Acad. Sci. ISSN 0077-8923
ANNALS OF THE NEW YORK ACADEMY OF SCIENCESIssue: The 12th OESO World Conference: Cancers of the Esophagus
Diet and esophageal disease
Sanford M. Dawsey,1 Renato B. Fagundes,2 Brian C. Jacobson,3 Laura A. Kresty,4
Susan R. Mallery,5 Shirley Paski,6 and Piet A. van den Brandt71Nutritional Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NationalInstitutes of Health, Bethesda, Maryland. 2Departamento de Clınica Medica. Universidade Federal de Santa Maria ePrograma de Pos Graduacao: Ciencias em Gastroenterologia, Universidade Federal do Rio Grande do Sul, Brasil. 3BostonUniversity Medical Center, Boston, Massachusetts. 4Department of Medicine, Division of Hematology & Oncology, MedicalCollege of Wisconsin, Milwaukee, Wisconsin. 5Division of Oral Maxillofacial Pathology & Radiology, College of Dentistry, OhioState University, Columbus, Ohio. 6University of Washington/VA Puget Sound, Seattle, Washington. 7Maastricht UniversityMedical Centre, Maastricht, Netherlands
Address for correspondence: [email protected]
The following, from the 12th OESO World Conference: Cancers of the Esophagus, includes commentaries onmacronutrients, dietary patterns, and risk of adenocarcinoma in Barrett’s esophagus; micronutrients, trace elements,and risk of Barrett’s esophagus and esophageal adenocarcinoma; the role of mate consumption in the development ofsquamous cell carcinoma; the relationship between energy excess and development of esophageal adenocarcinoma;and the nutritional management of the esophageal cancer patient.
Keywords: Barrett’s esophagus; macronutrients; micronutrients; mate; nutrition; esophageal adenocarcinoma; OESO
Concise summary
There are several difficulties encountered when cor-relating dietary factors with disease prevalence,including, in particular, confounding and study-design issues. Prospective cohort studies, whichmore adequately control for confounding as well asrecall bias, typically report either null or reducedassociations compared with case-control studies.Most of the existing literature on diet and Bar-rett’s carcinoma is based on case-control studiesin which minor to moderate inverse associationshave been reported with a diet low in fruits andvegetables, particularly green, leafy, and crucifer-ous vegetables, and a diet high in red and pro-cessed meats, with protective associations notedwith specific forms of vegetables, particularly green,leafy vegetables, and raw vegetables. Most studiesshow a strong inverse association between fiberand esophageal adenocarcinoma (EAC), and a re-cent meta-analysis on the association between meatintake and adenocarcinoma showed a relative riskfor the highest versus lowest intake categories forred and processed meat. Given the potential for
multiple interactions between specific macronu-trients, some investigators have turned instead topattern analyses, whereby types of diets are usedas the exposure variable. Overall, such studieshave found that a “healthy” diet is inversely asso-ciated with both Barrett’s esophagus (BE) and ade-nocarcinoma, whereas a “Western” style diet (highin meat consumption and low in fruits and vegeta-bles) appears to increase the risk.
Various meta-analyses illustrate the potential fordifferential information bias in retrospective case-control studies, possibly due to preclinical dis-ease symptoms that may affect dietary intake,particularly in upper gastrointestinal diseases. ForBE, significantly inverse associations were seen inmeta-analyses of risk and dietary vitamin C, vita-min E, and �-carotene in case-control studies, butno cohort data are available on these associations.For EAC, significant inverse associations were seenin meta-analyses of Barrett’s risk and dietary vitaminC, vitamin E, �-carotene, folate, and an antioxidantscore in case-control studies, but there was signif-icant heterogeneity among the case-control stud-ies. Cohort data show that there may be a positive
doi: 10.1111/nyas.12528
127Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Diet and esophageal disease Dawsey et al.
association with dietary vitamin E intake. No clearassociations have been found between serum or di-etary vitamin D, nor vitamin supplement use andrisk of BE or adenocarcinoma in case-control or co-hort studies. A significant inverse association withtoenail selenium was seen in women but not inmen. For esophageal squamous cell cancer, statis-tically significant inverse association was found forhigh versus low toenail selenium levels. Given thelikelihood of information bias in retrospective case-control studies, more evidence from prospectivecohort studies is clearly needed.
Heavy exposure to polycyclic aromatic hydrocar-bons (PAHs) can induce risk for esophageal squa-mous cell cancer and is demonstrated by high levelsof urine 1-hydroxypyrene glucuronide (1-OHPG),a stable metabolite that reflects recent exposureto mixed aromatic hydrocarbons. Some studiesreported histological findings, suggestive of PAHexposure in esophagectomy specimens. These find-ings were recently corroborated by a study that de-tected PAH metabolites in epithelial cells of theesophagus in Iran and demonstrated a dramaticdose–response association between the concentra-tion of these metabolites and squamous cell cancerrisk. In South America, the widespread consump-tion of mate, a traditional drink in that part of theworld, increases the risk of squamous cell cancer,and one probable mechanism for the carcinogenic-ity of mate is that it exposes consumers to high levelsof PAHs. Yerba mate leaves undergo several process-ing steps, the most crucial one being blanching anddrying the leaves over wood fires, which expose theleaves to abundant smoke. Recently, one Y. matebrand has been sold that advertises that the leavesare dried with steam heat. This processing withoutsmoke appears to yield a significantly lower expo-sure to aromatic hydrocarbons.
Food-based prevention capitalizes on the fact thatwhole foods are complex mixtures of bioactive phy-tochemicals that may act additively or synergisti-cally to inhibit multiple cancer signaling networks.Research supports that BE and EAC are inverselycorrelated with consumption of plant-based dietsrich in fruits, vegetables, fiber, and vitamins C, E,and �-carotene. Conversely, diets of animal-basedorigin generally increase risk for adenocarcinoma.Advances in molecular profiling coupled with in-tegration of environmental and host factors maybetter estimate risk for EAC and discern betweenprogressors and nonprogressors for future inter-vention trials. Profiling in patients may inform thetrue convergence zone (period between molecularintraepithelial neoplasia and cancer) from a molec-ular standpoint, permitting targeted interventionsin patients stratified by level of risk for cancerprogression. A pilot study conducted in patientswith Barrett’s metaplasia provided black raspberries(BRB) orally showed that oxidative stress levels werereduced, as measured by urinary 8-isoprostane lev-els. Preclinical studies with cranberry extracts tar-geting EAC are currently undertaken.
The etiology of malnutrition in esophageal canceris multifactorial, and multiple studies have shownan association between poor nutrition status andadverse outcomes. Nutrition care plans should bedeveloped starting from the diagnosis and stag-ing work through radiation and/or chemotherapy,surgery, and postesophagectomy. Several tools fornutrition assessment have been validated in oncol-ogy patients, and the decision to initiate nutritionsupport is based on nutritional assessment and theanticipated clinical course. Immunonutrition refersto immune-enhancing enteral formulas that containmixtures of arginine, ribonucleic acids, and essentialfatty acids.
1. Macronutrients, dietary patterns, andthe risk of Barrett’s esophagus andesophageal adenocarcinoma
Brian C. [email protected]
Nutritional epidemiologists have demonstratedstrong associations between numerous disease statesand dietary macronutrients (proteins, fats, and
carbohydrates, including fiber). There is now agrowing body of evidence suggesting associationsbetween macronutrients and both EAC and its pre-cursor lesion, BE. However, before discussing someof these potential associations, it is prudent to high-light some of the difficulties encountered whencorrelating dietary factors with disease prevalence,including, in particular, confounding and studydesign issues (i.e., case-control vs. cohort designs).
128 Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Dawsey et al. Diet and esophageal disease
For example, persons with symptoms of gastroe-sophageal reflux (GER) may alter their dietaryhabits to avoid symptoms, either because of theirown observations or owing to advice from careproviders or the media. If diet and GER are asso-ciated both with a disease such as EAC and witheach other, it becomes difficult to tease out the mag-nitude and direction of effect that a dietary compo-nent has on the disease. Body mass index, physicalactivity, and even pesticide use (as both a poten-tial carcinogen and as an agent used in agricul-ture) are just some of the other potential con-founders in any analysis of diet and esophagealdisease.
Study design and attendant confounding andbias are significant issues, as evidenced by the factthat case-control studies have often found associa-tions between diet and esophageal disease, whereasprospective cohort studies, which more adequatelycontrol for confounding as well as recall bias, typi-cally report either null or reduced associations com-pared with case-control studies.1 Further, becauseEAC is relatively uncommon, only three large co-hort studies have had a sufficient number of cases toevaluate diet as a risk factor thus far. Despite inclu-sion of over one million participants, the cumulativenumber of EAC cases in all three of these cohortscombined is still fewer than 1000.2–4 Analyses ofspecific dietary components can also be difficult be-cause macronutrients are strongly correlated withone another, an issue that suggests that evaluationof dietary patterns may be more informative thanstudies of individual macronutrients in understand-ing the role of diet in EAC.
Most of the existing literature on diet and BE orEAC is based on case-control studies in which minorto moderate inverse associations have been reportedwith a diet low in fruits and vegetables, particularlygreen, leafy, and cruciferous vegetables, and a diethigh in red and processed meats.1 Unfortunately, inboth the prospective National Institutes of Health(NIH)–AARP Diet and Health study and the Eu-ropean Prospective Study of Cancer and Nutrition(EPIC), there was no association between total fruitand vegetable consumption and EAC.2,5 There were,however, protective associations noted with specificforms of vegetables, particularly green, leafy vegeta-bles and raw vegetables. For example, in the NIH–AARP study, spinach was protective against EAC(hazard ratio 0.66; 95% CI 0.46–0.95) and there
were borderline protective associations for cabbageand broccoli. In the prospective Netherlands CohortStudy, raw vegetables and citrus fruits were protec-tive against EAC.4 However, in that study, protectionwas conferred more among smokers than nonsmok-ers, suggesting that fruits and vegetables may modifythe impact of smoking on EAC risk. Finally, whenconsidering dietary added sugars, the NIH–AARPstudy demonstrated an increased risk for EAC com-paring the highest to lowest quintiles (HR 1.62; 95%CI 1.07–2.45).6
Most, but not all, studies show a strong inverseassociation between fiber and EAC (odds ratio inthe 0.3–0.4 range for interquartile comparisons).Two studies looked specifically at fiber and risk ofBE, both showing inverse associations. In the FIN-BAR study, subjects consuming the greatest quan-tity of fiber had an odds ratio of 0.4 (95% CI0.25–0.8) compared with those in the lowest quar-tile for fiber intake. In a case-control study fromthe Kaiser Permanente group, there was protectionagainst BE by fruits and vegetables but not by grainsand legumes.1,7 This highlights an important point,in that Western diets often include fiber sources thatmay not be so healthy, such as white bread, crackers,sugared cereals, and pasta.
A recent meta-analysis examined the associationbetween meat intake and EAC, finding a summaryrelative risk for the highest versus lowest intake cat-egories of 1.31 (95% CI 1.05–1.64) for red meatand 1.41 (95% CI 1.09–1.83) for processed meat.8
Again, it is worth noting that significant associationswere seen with case-control studies included in themeta-analysis but not uniformly with the prospec-tive studies. In the NIH–AARP study, the associationbetween EAC and dietary fat was generally null oncefully adjusted for potential confounders, but theremay have been a protective effect against EAC bypolyunsaturated fat among subjects with a normalbody-mass index (BMI).3
Given the potential for multiple interactions be-tween specific macronutrients, some investigatorshave turned instead to pattern analyses, wherebytypes of diets (e.g., healthy, Western, and high salt)are used as the exposure variable. Overall, such stud-ies have found that a healthy diet (one high in fruitsand vegetables and low in red meat and saturatedfat) is inversely associated with both EAC and BE,whereas a Western-style diet (one high in meat con-sumption and low in fruits and vegetables) appears
129Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Diet and esophageal disease Dawsey et al.
to increase the risk of EAC and BE.9,10 Diets high indairy or salt were not associated with EAC.
It also bears noting that the timing between ex-posure to certain macronutrients and the onset ofBE or EAC remains unknown. In fact, since nearlyall cases of EAC arise within segments of BE, dietaryassociations may be linked primarily to an excessrisk of BE, with any excess risk of EAC being re-lated simply to having BE. In summary, dietary pat-tern analyses suggests that so-called “healthy” diets,those high in fruits and vegetables and low in redmeat and saturated fat, may be associated with alower risk of both BE and EAC. However, firm con-clusions are currently limited by the paucity of datafrom high-quality prospective cohort studies.
2. Micronutrients and the risk ofBarrett’s esophagus and esophagealadenocarcinoma
Piet A. van den [email protected]
This short commentary will review what is knownabout selected micronutrients and the risk of BE, therisk of EAC, and the progression from BE to EAC. Itis limited to the dietary vitamins and antioxidantsC, D, E, �-carotene, folate, supplemental vitaminintake, and the mineral selenium.
Relatively few epidemiological studies have beenspecifically conducted on EAC (instead of over-all esophageal cancer) or BE. Among these arepopulation-based or hospital-based case-controlstudies in the United States, Canada, Europe, andAustralia. Only three prospective cohort studieshave published some data on micronutrients andrisk of EAC: the NIH–AARP study (n = 492,000),with 382 EAC cases after 8 years of follow-up; theEPIC study (n = 520,000), with 65 EAC cases after6.5 years of follow-up; and the Netherlands CohortStudy (NLCS; n = 120,852), with 144 EAC casesafter 16.3 years of follow-up. The NLCS has alsoconducted follow-up on occurrence of BE, usingrecord linkage to a national pathology registry, andfound 433 BE cases (with intestinal metaplasia).
We performed various meta-analyses for BE andEAC based on the published data from these studies,using Stata. A first meta-analysis of fruit (as impor-tant sources of vitamins) and risk of BE showed astatistically significant RR of 0.74 (95% CI 0.55–0.99) for high versus low fruit intake among four
available case-control studies, with no significantheterogeneity. However, in the NLCS cohort, we re-cently found nonsignificant RRs of 1.12 in womenand 1.00 in men, indicating no protection by fruit.11
This illustrates the potential for differential infor-mation bias in retrospective case-control studies,possibly due to preclinical disease symptoms thatmay affect dietary intake, particularly in upper gas-trointestinal diseases.12
Keeping this caveat in mind, significant inverseassociations were seen in meta-analyses of BE riskand dietary vitamin C (high vs. low, RR = 0.66),vitamin E (RR = 0.54), and �-carotene (RR = 0.58)in case-control studies, but no cohort data are avail-able yet on these associations. A similar pattern wasobserved for the combination of these vitamins intoan antioxidant score from foods. A borderline statis-tically significant inverse association was seen withfolate in case-control studies.
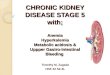
For EAC, significant inverse associations wereseen in meta-analyses of BE risk and dietary vita-min C (high vs. low, RR = 0.51), vitamin E (RR =0.65), �-carotene (RR = 0.56), folate (RR = 0.58),and an antioxidant score in case-control studies,but there was significant heterogeneity among thecase-control studies. However, cohort data showthat there may be a positive association with di-etary vitamin E intake: RR = 1.27 (95% CI, 0.94–1.72) for high versus low intake (Fig. 1).13 Noclear associations have been found between serumor dietary vitamin D and EAC risk. No signifi-cant associations were observed between vitaminsupplement use and risk of BE or EAC in case-control or cohort studies. In contrast, an inverseassociation was seen with (multi)vitamin supple-ment use and progression from BE to EAC in theSeattle BE cohort.14
Regarding selenium, observational studies haveused serum or toenail selenium levels as statusbiomarkers, because it is difficult to estimate dietaryselenium intake. Randomized controlled trials inChina have found a nonsignificantly reduced risk ofesophageal cancer, primarily esophageal squamouscell carcinoma (ESCC), in the supplemented group.The U.S. NPC trial also found a nonsignificantlyreduced risk of esophageal cancer after seleniumsupplementation,15 but numbers were very small. Inthe NLCS, we found no association between toenailselenium levels and risk of BE,16 similar to findingsfrom the FINBAR case-control study in Northern
130 Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Dawsey et al. Diet and esophageal disease
Figure 1. Vitamin E intake (high vs. low) and esophageal adenocarcinoma risk.
Ireland.17 For ESCC risk, we observed a statisticallysignificant inverse association in the NLCS with anRR of 0.37 (95% CI, 0.16–0.86) for high versus lowtoenail selenium levels.18 For EAC risk, a significantinverse association with toenail selenium was seenin women but not in men in the NLCS. In the Seat-tle BE progression cohort, no association was foundbetween serum selenium and progression from BEto EAC, but 82% were men.
The current evidence linking vitamins and min-erals and risk of EAC or BE is mostly or sometimesexclusively based on case-control studies, especiallyfor BE. Given the likelihood of information biasin retrospective case-control studies, more evidencefrom prospective cohort studies is clearly needed.It will also be informative if future analyses alsoevaluate associations within subgroups of smokingcategories, body mass index, sex, reflux, and otherrisk factors.
3. Polycyclic aromatic hydrocarbonexposure and esophageal cancer inSouth America: a new look to an oldrisk factor
Renato B. Fagundes and Sanford M. [email protected]
Esophageal cancer is the sixth most common causeof cancer death worldwide. Incidence and mortality
rates show striking variations across different ge-ographic regions, and in the high-risk regions,ESCC is by far the most common histologic typeof esophageal cancer.19
Tobacco smoking and heavy alcohol use are ma-jor risk factors for ESCC, but in high-risk popula-tions, many people do not smoke or drink alcohol.They may, however, be exposed to the same carcino-gens found in tobacco smoke, including PAHs, fromother sources. Studies conducted in Linxian, China,one of the highest risk areas for ESCC, have shownthat the inhabitants of this area are exposed to highlevels of carcinogenic PAHs, probably from the coalused for cooking and heating in unvented stoves.20
This heavy exposure to PAH is demonstrated byhigh levels of urine 1-OHPG, a stable PAH metabo-lite that reflects recent exposure to mixed PAHs.20 InGolestan, northeastern Iran, another area with veryhigh rates of ESCC, the population also has highurine 1-OHPG concentrations and little consump-tion of tobacco.21
Another study conducted in China showed his-tological findings suggestive of PAH exposure inesophagectomy specimens.22 This study was re-cently corroborated by a study that detected PAHmetabolites in epithelial cells of the esophagus inIran and demonstrated a dramatic dose–responseassociation between the concentration of thesemetabolites and ESCC risk.23
131Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Diet and esophageal disease Dawsey et al.
In South America, ESCC accounts for 90%or more of esophageal cancer cases, and a highgeographic variation in incidence also occurs. Thehigh-incidence area in South America encompassesSouthern Brazil, Uruguay, Paraguay, and NorthernArgentina. Previous research has shown that besidesalcohol abuse and cigarette smoking, the widespreadconsumption of mate, a traditional drink in thispart of the world, increases the risk of ESCC.24
Mate is a water infusion of the herb Y. mate (Ilexparaguayensis), and one probable mechanism for thecarcinogenicity of mate is that it exposes consumersto high levels of PAH. Three studies conducted in RioGrande do Sul, the most Southern Brazilian state,give support to this hypothesis. The first study iden-tified high levels of 1-OHPG in the urine of matedrinkers.24,25 The two subsequent studies showedthat most commercial Y. mate leaves contain largeamounts of PAH,26,27 and more than 50% of thebenzo[�]pyrene, a PAH classified by the Interna-tional Agency for Research on Cancer (IARC) as car-cinogenic to humans, is eluted in traditional hot orcold infusions of the Y. mate leaves.27 The commer-cial brands analyzed had a mean benzo[�]pyreneconcentration of 40 ng/g of leaves. If we assumethat an average of 50 g of leaves are used to makea typical gourd (a cuia) of mate, and 50% of thebenzo[�]pyrene in the leaves is eluted into the infu-sion, then drinking a gourd of mate in the traditionalway exposes the consumer to 50 g × 40 ng/g × 0.5elution = 1000 ng of benzo[�]pyrene, which equalsthe benzo[�]pyrene content of the smoke from 100cigarettes. Y. mate leaves undergo several processingsteps before they are ready for consumption, withthe most crucial steps being blanching and dryingthe leaves over wood fires, which exposes the leavesto abundant smoke. Nearly all of the PAH content ofY. mate is acquired during these blanching and dry-ing stages.28 Recently, one Y. mate brand has beensold that advertises that it is never exposed to smoke,because the leaves are dried with steam heat. Thisprocessing without smoke appears to yield a signif-icantly lower PAH exposure.26
In conclusion, drinking mate prepared from tra-ditionally processed Y. mate leaves exposes con-sumers to very high levels of PAH, which is proba-bly one reason for the observed association betweenmate drinking and ESCC risk. Changing the pro-cessing of Y. mate, such as drying the leaves withsteam heat rather than wood smoke, may lower
the PAH content of the commercial product. Asmate consumption is high in the South Ameri-can high-risk area for ESCC, reducing the PAHcontent of Y. mate could be beneficial to publichealth.
4. Considerations for utilizing afood-based preventive approach totarget esophageal adenocarcinoma
Laura A. Kresty and Susan R. [email protected]
Esophageal cancer is a significant health problem.Mortality statistics closely parallel incidence datareflecting the insidious nature of this disease: poorprognosis due to unsuccessful screening coupledwith late-stage diagnosis and ineffective treatmentoptions. Increasing rates of EAC and its recognizedprecursor, BE, have spurred interest in develop-ing improved preventive strategies to mitigate EACprogression. Food-based preventive approaches, de-fined as the use of food or food-derived bioactiveconstituents to reverse, suppress, delay, or preventcancer, are of particular interest given associationsbetween various dietary factors and EAC.
Cancer-preventive interventions occur on acontinuum. Action-oriented, behaviorally focusedstrategies make up one end; food-based interven-tions, where foods or food-derived extracts areadministered in a nontraditional manner, outsidethe normal food matrix, reside in the middle; andtraditional medical model-focused interventionsutilizing single-agent pharmaceuticals on the otherend. Approaches have been expertly reviewed bypioneers in the field.29,30 Food-based preventioncapitalizes on the fact that whole foods are complexmixtures of bioactive phytochemicals that mayact additively or synergistically to inhibit multiplecancer-signaling networks. Additional positive as-pects associated with food-based prevention includelow toxicity, few adverse events, individual empow-erment, utilization of by-products (peels, seeds),cost effectiveness, renewability, sustainability, andpositive impact on local economies. Food-basedefforts also pose unique challenges. Foods arechemically complex and frequently incompletelyunderstood in terms of in vivo pharmacokinet-ics/pharmacodynamics; the metabolic fate of theparent compound and its metabolites is frequentlyunknown, raising challenges for establishing
132 Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Dawsey et al. Diet and esophageal disease
Figure 2. Progression to esophageal adenocarcinoma.
efficacious dosages, schedules of administration,and biomarkers of compliance. There is inher-ent variability in agriculture products due to soilcomposition, weather, plant species, ripeness, prod-uct processing, and stabilization. The burden ofproduct safety falls to the researcher, who must eval-uate potential contaminants (i.e., pesticides, molds,and heavy metals). Large-scale production andstandardization also pose challenges.29,30 Productpalatability, mode and matrix of delivery, and de-velopment of a placebo for randomized trials mustbe established. Lastly, there has been a regulatoryparadigm shift in recent years, resulting in investiga-tional new drug (IND) requirements for many food-and extract-based studies, particularly if any medi-cal claims are proposed. Interestingly, in a departurefrom its drug-focused structure, the U.S. Food andDrug Administration (FDA) recently approved itssecond botanical drug product, crofelemer, for themanagement of HIV-associated diarrhea.31
Research supports the view that BE and EACare inversely correlated with consumption ofplant-based diets rich in fruits, vegetables, fiber,and vitamins C, E, and �-carotene (reviewed inRef. 29). Conversely, diets of animal-based origingenerally increase EAC risk. Figure 2 outlinesadditional factors linked to increased EAC risk.However, there have been inconsistencies in theliterature with regard to dietary factors associatedwith BE and EAC development, raising questionsabout the strength of the associations and where to
focus preventive efforts to affect rising EAC rates.We postulate that differing results extend beyondobvious dietary complexity and methodologicalissues to include individual, tissue/cellular, andmolecular-level heterogeneity. Thus, food-based in-terventions targeting EAC must carefully select thefood-based product as well as the target population.Pohl et al.32 reports that specific dietary risk factorsare associated with different stages of esophagealdisease. Low fruit/vegetable consumption was notassociated with gastroesophageal reflux disease(GERD), but high consumption was protectiveagainst BE and EAC development,32 supportingthe view that the appropriateness of the interven-tion may differ based on individual risk factors,symptoms, and stage of pathologic progression.This illustrates population-specific considerationsto weigh in targeting EAC progression.
The concept of cancer prevention embraces theidea of targeting cancer early, optimally at a pre-malignant and reversible stage. This stems fromthe multistep carcinogenesis model characterizedby early genetic/epigenetic alterations accompaniedby phenotypic and histopathologic changes over along latency period. William et al.33 outlined thisphenomenon for a number of cancers, defining theperiod between molecular intraepithelial neoplasiaand cancer as the convergence zone, a zone of sub-clinical cancer providing an opportunity for tar-geted interventions.33 However, caution must beexercised in selecting the intervention population
133Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Diet and esophageal disease Dawsey et al.
Table 1. Nutrition assessment tools
Tool Characteristics Comments
Subjective global assessment
(SGA)
Weight loss, food intake, GI symptoms,
functional capacity + disease,
metabolic demand + focused
physical exam
Good sensitivity, predicts post-op
comp, LOS
Nutrition risk index (NRI) NRI = 1.519 (serum albumin; g/d) +41.7 current weight/usual weight
Good sensitivity, predicts post-op
comp, LOS
Malnutrition screening tool Weight, weight loss, appetite 100% sensitive, 81–92% specific versus
SGA
Nutrition risk screening BMI, weight loss, food intake + disease
severity
Validated in oncology patients
Note: LOS, length of stay.
when targeting EAC. The multistep and rather lin-ear cancer progression model of GERD–BE–EACis problematic, and in practice likely results ininterventions in heterogeneous low-risk popula-tions, not high-risk cancer progressors. Patient pop-ulation considerations, as elegantly summarized byReid et al.,34 include observations that 95% of EACcases arise in patients without a prior BE diagno-sis, 80% of EACs arise without a prior diagnosis ofGERD, 50% of EAC patients have no prior refluxsymptoms, and a large portion of BE patients areasymptomatic and not under surveillance. He con-cludes that endoscopic screening of GERD patientshas resulted in overdiagnosis of nonprogressing,non-life-threatening BE and underdiagnosis of pro-gressing BE/early EAC or life-threatening disease.There is hope that informed population stratifica-tion will increase intervention efficacy; however, thisis contingent on improved risk modeling. We mustmove beyond stratification based solely on patho-logic diagnoses and routine expression markers. Ad-vances in molecular profiling coupled with integra-tion of environmental and host factors may betterestimate risk for EAC and discern between progres-sors and nonprogressors for future intervention tri-als. Carter et al.35 recently reported that increasesin somatic copy-number alterations before cancerprogression and genome-wide doubling events thatcommonly follow aneuploidy are linked to EAC pro-gression. Thus, such profiling in BE or EAC pa-tients may inform the true convergence zone froma molecular standpoint, permitting targeted inter-ventions in patients stratified by level of risk for EACprogression.
Still, positive research supports that food-basedapproaches hold promise for cancer inhibition.Stoner comprehensively detailed a stepwise ap-proach for food-based inhibitor evaluations, span-ning preclinical to clinical evaluations of BRB inmultiple targets, including oral cavity, esophagus,and colon. We conducted a pilot study in pa-tients with BE metaplasia provided BRB orally for6 months at 32 or 45 g/day, and found that theberries were well tolerated, compliance was good,ellagic acid metabolites were elevated in sera, andoxidative stress levels were reduced, as measuredby urinary 8-isoprostane levels.36 Preclinical studieswith cranberry extracts targeting EAC are ongoingin our laboratory utilizing similar approaches. Ad-ditional food-based research is warranted for EACinhibition, particularly with regard to targeted de-livery and host interaction, as has been delineatedby Mallery et al. in the oral cavity.37
5. Nutritional considerations inesophageal cancer
Shirley [email protected]
Malnutrition is nearly universal in esophageal can-cer patients. Up to 85% of patients are malnourishedat diagnosis, and nutrition status worsens with ther-apy. Under-recognition, limited resources for nu-trition diagnosis and treatment, and inconsistentreferral of high-risk patients to nutrition experts arecommon.
The etiology of malnutrition in esophagealcancer is multifactorial. The tumor may cause
134 Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Dawsey et al. Diet and esophageal disease
Figure 3. Nutrition assessment and action plan.
mechanical obstruction or esophageal reflux.Chemotherapy and radiation therapy can result inmucositis, xerostomia, odynophagia, nausea, vomit-ing, and diarrhea. These gastrointestinal symptoms,as well as cancer cachexia, lead to reduced dietaryintake. Malnutrition may be perpetuated postop-eratively due to anastomotic stricture, esophagealdysmotility, poor gastric emptying, or dumpingsyndrome.
Multiple studies have shown an association be-tween poor nutrition status and adverse outcomes.Conversely, better nutrition status is associated withimproved therapy tolerance, therapy response, re-duced hospitalizations and length of stay, surgicalrespectability, and reduced operative complications.The goals of nutrition management are (1) to pre-vent or minimize nutritional deficiencies, (2) tominimize loss of lean body mass, (3) to minimizenutrition impact symptoms, and (4) to maximizequality of life. Weight loss due to gastrointestinalsymptoms and reduced dietary intake is generallyeasy to correct with nutrition support. Weight lossdue to cancer cachexia and inflammatory cytokinesis difficult to overcome, and the goal of nutritiontherapy and nutrition support in this setting is toreduce the loss of lean body mass.
Nutrition care plans should be developed start-ing from the diagnosis and staging work throughradiation and/or chemotherapy, surgery, and poste-sophagectomy. All patients should receive generaldietary advice. General advice should be providedby a healthcare professional with the time to counsel
the patient with respect to their dietary preferencesand can involve dietary therapy that addressesspecific gastrointestinal symptoms. Additionalcomponents of a nutrition care plan includenutrition assessment, indications for nutritionsupport, route for nutrition support, and specificformula considerations.
Assessment of nutrition status should be per-formed regularly using a validated tool. Manytools have been developed for this purpose.38–41
Several nutrition-assessment tools have been val-idated in oncology patients (Table 1). Patientswho screen as moderate-to-high nutritional riskshould be referred for a more detailed nutritionassessment.
The decision to initiate nutrition support is basedon nutritional assessment and the anticipated clin-ical course (Fig. 3). When providing nutrition sup-port, enteral is preferred over parenteral route. Oralsupplements may be provided orally or via an office-placed nasoenteric tube. Self-expanding metal stentsmay temporarily optimize oral nutrition, but shouldbe removed empirically following chemoradiationtherapy to reduce the risk of stent migration. Per-cutaneous jejunostomy can provide reliable en-teral access and is well tolerated, but placementis more challenging. Parenteral nutrition is appro-priate for providing reliable nutrition when enteralfeeding is not possible. Management of nutrition-related symptoms and provision of nutrition sup-port is ideally performed by a multidisciplinaryteam.42
135Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Diet and esophageal disease Dawsey et al.
Immunonutrition refers to immune-enhancingenteral formulas that contain mixtures of arginine,ribonucleic acids, and essential fatty acids (DHA,EPA). Immunonutrition appears to be the mosteffective in malnourished patients. Immunonutri-tion given 5–7 days preoperatively has been shownto reduce infectious complications and length ofstay.43 Malnourished patients may also benefit frompostoperative immunonutrition, and a single smalltrial found that immunonutrition before and dur-ing chemoradiation therapy improved performancestatus.44
Communication with the patient and his/herprimary care provider, dietitian, and gastroenterol-ogist is essential for reducing the risk of postoper-ative malnutrition. Maintaining adequate nutritionpostesophagectomy can be challenging. Develop-ment of anastomotic stricture, postvagotomy dys-motility, poor gastric emptying, or dumping syn-drome can result in reduced dietary intake andweight loss well beyond the immediate postoper-ative period.
In summary, all esophageal cancer patients areat risk for malnutrition. Regular nutrition screen-ing should be performed, and moderate- to high-risk patients should be referred to nutrition experts.A multidisciplinary team is best equipped to helppatients meet their nutritional goals. Immunonu-trition is a newer therapy that may be consideredin selected patients. A well-executed nutrition careplan and thoughtful use of nutrition support canimprove patient outcomes and quality of life.
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Kubo, A., D. Corely, C. Jensen & R. Kaur. 2010. Dietary fac-tors and the risks of esophageal adenocarcinoma and Bar-rett’s esophagus. Nutr. Res. Rev. 23: 230–246.
2. Jeurnink, S., F. Buchner, H. Bueno-de-Mesquita, et al. 2012.Variety in vegetable and fruit consumption and the risk ofgastric and esophageal cancer in the European ProspectiveInvestigation into Cancer and Nutrition. Int. J. Cancer 131:E963–E973.
3. O’Doherty, M., N. Freedman, A. Hollenbaeck, et al. 2011.Association of dietary fat intakes with risk of esophageal andgastric cancer in the NIH–AARP diet and health study. Int.J. Cancer 131: 1376–1387.
4. Steevens, J., L. Schouten, R. Goldbohm & P. van denBrandt. 2011. Vegetables and fruits consumption and risk of
esophageal and gastric cancer subtypes in the NetherlandsCohort Study. Int. J. Cancer 129: 2681–2693.
5. Freedman, N., Y. Park, A. Subar, et al. 2007. Fruit and veg-etable intake and esophageal cancer in a large prospectivecohort study. Int. J. Cancer 121: 2753–2760.
6. Tasevska, N., L. Jiao, A. Cross, et al. 2012. Sugars in diet andrisk of cancer in the NIH–AARP diet and health study. Int.J. Cancer 130: 159–169.
7. Kubo, A., T. Levin, G. Block, et al. 2008. Dietary antioxidants,fruits, and vegetables and the risk of Barrett’s esophagus. Am.J. Gastroenterol. 103: 1614–1623.
8. Huang, W., Y. Han, J. Xu, et al. 2013. Red and processedmeat intake and risk of esophageal adenocarcinoma: a meta-analysis of observational studies. Cancer Causes Control 24:193–201.
9. Chen, H., M.H. Ward, B.I. Graubard, et al. 2002. Dietarypatterns and adenocarcinoma of the esophagus and distalstomach. Am. J. Clin. Nutr.; 75: 137–144.
10. Kubo, A., G. Block, G. Rumore, et al. 2008. Dietary patternsand the risk of Barrett’s esophagus. Am. J. Epidemiol. 167:839–846.
11. Keszei, A.P., L.J. Schouten, A.L.C. Driessen, et al. 2014. Veg-etable, fruit and nitrate intake in relation to the risk ofBarrett’s esophagus in a large Dutch cohort. Br. J. Nutr. 111:1452–1456.
12. Botterweck, A.A., P.A. van den Brandt & R.A. Goldbohm.1998. A prospective cohort study on vegetable and fruit con-sumption and stomach cancer risk in The Netherlands. Am.J. Epidemiol. 148: 842–853.
13. Carman, S., F. Kamangar, N.D. Freedman, et al. 2009. Vita-min E intake and risk of esophageal and gastric cancers inthe NIH–AARP Diet and Health Study. Int. J. Cancer 125:165–170.
14. Dong, L.M., A.R. Kristal, U. Peters, et al. 2008. Dietary sup-plement use and risk of neoplastic progression in esophagealadenocarcinoma: a prospective study. Nutr. Cancer 60: 39–48.
15. Duffield-Lillico, A.J., M.E. Reid, B.W. Turnbull, et al. 2002.Baseline characteristics and the effect of selenium supple-mentation on cancer incidence in a randomized clinicaltrial: a summary report of the Nutritional Prevention ofCancer Trial. Cancer Epidemiol. Biomarkers Prev. 11: 630–639.
16. Steevens, J., L.J. Schouten, A.L. Driessen, et al. 2010. Toe-nail selenium status and the risk of Barrett’s esophagus: theNetherlands Cohort Study. Cancer Causes Control 21: 2259–2268.
17. O’Rorke, M.A., M.M. Cantwell, C.C. Abnet, et al. 2012. Toe-nail trace element status and risk of Barrett’s oesophagusand oesophageal adenocarcinoma: results from the FINBARstudy. Int. J. Cancer 131: 1882–1891.
18. Steevens, J., P.A. van den Brandt, R.A. Goldbohm & L.J.Schouten. 2010. Selenium status and the risk of esophagealand gastric cancer subtypes: the Netherlands cohort study.Gastroenterology 138: 1704–1713.
19. Ferlay, J., H.R. Shin, F. Bray, et al. 2010. Estimates of world-wide burden of cancer in 2008: GLOBOCAN 2008. Int. J.Cancer 127: 2893–2917.
20. Roth, M.J., Y.-L. Qiao, N. Rothman, et al. 2001. High urine1-hydroxypyrene glucuronide concentrations in Linxian,
136 Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.

Dawsey et al. Diet and esophageal disease
China, an area of high-risk for squamous oesophageal can-cer. Biomarkers 6: 381–386.
21. Kamangar, F., P.T. Strickland, A. Pourshams, et al. 2005.High exposure to polycyclic aromatic hydrocarbons maycontribute to high risk of esophageal cancer in northeasternIran. Anticancer Res. 25: 425–428.
22. Roth, M.J., W. Guo-Qing, K.J. Lewin, et al. 1998. Histopatho-logic changes seen in esophagectomy specimens from thehigh-risk region of Linxian, China: potential clues to an eti-ologic exposure? Hum. Pathol. 29: 1294–1298.
23. Abedi-Ardekani, B., F. Kamangar, S.M. Hewitt, et al. 2010.Polycyclic aromatic hydrocarbon exposure in oesophagealtissue and risk of oesophageal squamous cell carcinoma innorth-eastern Iran. Gut 59: 1178–1183.
24. Sewram, V., S.E. De, P. Brennan & P. Boffetta. 2003. Mateconsumption and the risk of squamous cell esophageal can-cer in Uruguay. Cancer Epidemiol. Biomarkers Prev. 12: 508–513.
25. Fagundes, R.B., C.C. Abnet, P.T. Strickland, et al. 2006.Higher urine 1-hydroxy pyrene glucuronide (1-OHPG) isassociated with tobacco smoke exposure and drinking matein healthy subjects from Rio Grande do Sul, Brazil. BMCCancer 6: 139.
26. Golozar, A., R.B. Fagundes, A. Etemadi, et al. 2012. Signif-icant variation in the concentration of carcinogenic poly-cyclic aromatic hydrocarbons in yerba mate samples bybrand, batch, and processing method. Environ. Sci. Technol.46: 13488–13493.
27. Kamangar, F., M.M. Schantz, C.C. Abnet, et al. 2008. Highlevels of carcinogenic polycyclic aromatic hydrocarbons inmate drinks. Cancer Epidemiol. Biomarkers Prev. 17: 1262–1268.
28. Vieira, M.A., M. Maraschin, A.A. Rovaris, et al. 2010. Occur-rence of polycyclic aromatic hydrocarbons throughout theprocessing stages of erva-mate (Ilex paraguariensis). FoodAddit. Contam. Part A Chem. Anal. Control Expo. Risk Assess27: 776–782.
29. Fahey J.W., P. Talalay & T.W. Kensler. 2012. Notes from thefield: “green” chemoprevention and frugal medicine. CancerPrev. Res. 5: 179–188.
30. Stoner, G.D. 2009. Foodstuffs for preventing cancer: thepreclinical and clinical development of berries. Cancer Prev.Res. 2: 187–194.
31. Klein, R. & K. Struble U.S. Food and Drug Administration.Approval of Fulyzaq (crofelemer) to relieve symptoms ofdiarrhea in HIV/AIDS patients taking antiretroviral therapy.[2014, July 14]. Available: http://www.fda.gov/forconsum
ers/byaudience/forpatientadvocates/hivandaidsactivities/ucm333826.htm.
32. Pohl H., K. Wrobel, C. Bojarski, et al. 2013. Risk factorsin the development of esophageal adenocarcinoma. Am. J.Gastroenterol. 108: 200–207.
33. William, W.N. Jr., J.V. Heymach, E.S. Kim, et al. 2009. Molec-ular targets for cancer chemoprevention. Nat. Rev. Drug Dis-cov. 8: 213–225.
34. Reid, B.J., X. Li, P.C. Galipeau, et al. 2010. Barrett’s oe-sophagus and oesophageal adenocarcinoma: time for a newsynthesis. Nat. Reviews Cancer 10: 87–101.
35. Carter, S.L., K. Cibulskis, E. Helman, et al. 2012. Absolutequantification of somatic DNA alterations in human cancer.Nat. Biotechnol. 30: 413–421.
36. Kresty, L.A., W.L. Frankel, C.D. Hammond, et al. 2006.Transitioning from preclinical to clinical chemopreventiveassessments of lyophilized black raspberries: interim resultsshow berries modulate markers of oxidative stress in Bar-rett’s esophagus patients. Nutr. Cancer. 54: 148–156.
37. Mallery, S.R., D.B. Budendorf, M.P. Larsen, et al. 2011. Ef-fects of human oral mucosal tissue, saliva, and oral mi-croflora on intraoral metabolism and bioactivation of blackraspberry anthocyanins. Cancer Prev. Res. 4: 1209–1221.
38. Detsky, A.S. et al. 1987. Predicting nutrition associated com-plications for patients undergoing gastrointestinal surgery.JPEN J. Parenter. Enteral. Nutr. 11: 440–446.
39. Bauer, J. et al. 2002. Use of the scored Patient-GeneratedSubjective Global Assessment (PG-SGA) as a nutrition as-sessment tool in patients with cancer. Eur. J. Clin. Nutr. 56:779–785.
40. Ferguson, M. et al. 1999. Development of a valid and reliablemalnutrition screening tool for adult acute hospital patients.Nutrition 15: 458–464.
41. Kondrup, J. et al. 2003. Nutritional risk screening (NRS2002): a new method based on an analysis of controlledclinical trials. Clin. Nutr. 22: 321–336.
42. August, D.A. et al. 2009. A.S.P.E.N. clinical guidelines nu-trition support therapy during adult anticancer treatmentand in hematopoietic cell transplantation. JPEN J. Parenter.Enteral. Nutr. 33: 472–500.
43. Waitzberg, D.L. et al. 2006. Postsurgical infections are re-duced with specialized nutrition support. World J. Surg. 30:1592–1604.
44. Vasson, M.P. et al. 2014. Immunonutrition improves func-tional capacities in head and neck and esophageal cancer pa-tients undergoing radiochemotherapy: a randomized clini-cal trial. Clin. Nutr. 33: 204–210.
137Ann. N.Y. Acad. Sci. 1325 (2014) 127–137 C© 2014 New York Academy of Sciences.






![A rare cause of dysphagia due to esophageal intramural ......disease, GERD, and corrosive esophageal injury [4, 11– 14]. Abnormalities in esophageal motility, including, un-coordinated](https://img.dokumen.tips/doc/110x75/60b5b1e8c993b14a95327914/a-rare-cause-of-dysphagia-due-to-esophageal-intramural-disease-gerd-and.jpg)