Embed Size (px)
Citation preview

DIARRHEA
HOSSEIN S
ANEIAN
HOSSEIN S
ANEIAN
Ped. Ped.
Gastroenterologist
Gastroenterologist
ور شهری
ور شهری
13911391

DefinitionIn epidemiological studies diarrhoea is
defined as:
Passage of three or more loose or watery stools in a
24-hour period, a loose stool being one that would
take the shape of a container.
DefinitionIn Pediatrics, Diarrhoea is an increase in the:
Fluidity
Volume
Numberof stools relative to the usual habits of each individual.

Stool output > 10 g / kg / day, > 200ml per m² BSA/d , >150-200 gr per m² BSA/d.

Importance of Diarrhoea In under five children
Diarrhoea is a leading cause of:MortalityMorbiditySevere malnutrition

2.5 billion episodes/year2.5 billion episodes/year
3.6 episodes/baby/year3.6 episodes/baby/year
In children under 5 years of ageIn children under 5 years of age
In children under 5 years of ageIn children under 5 years of age
3.2 million deaths/ year3.2 million deaths/ year
5 million per year in 5 million per year in 19801980 to less to less than 2 million in than 2 million in 19991999
= مرگ ومیر 18اسها ل %کودکان
.دومین علت مرگ ومیر کودکان 1/5 میلیون مرگ در سال
روتا ویروس =527000(deaths=29%)
ETEC=300000-500000160000شیگال =

DIARRHOEA MALNUTRITION,
شناختی و تکاملی روانی اختالالت
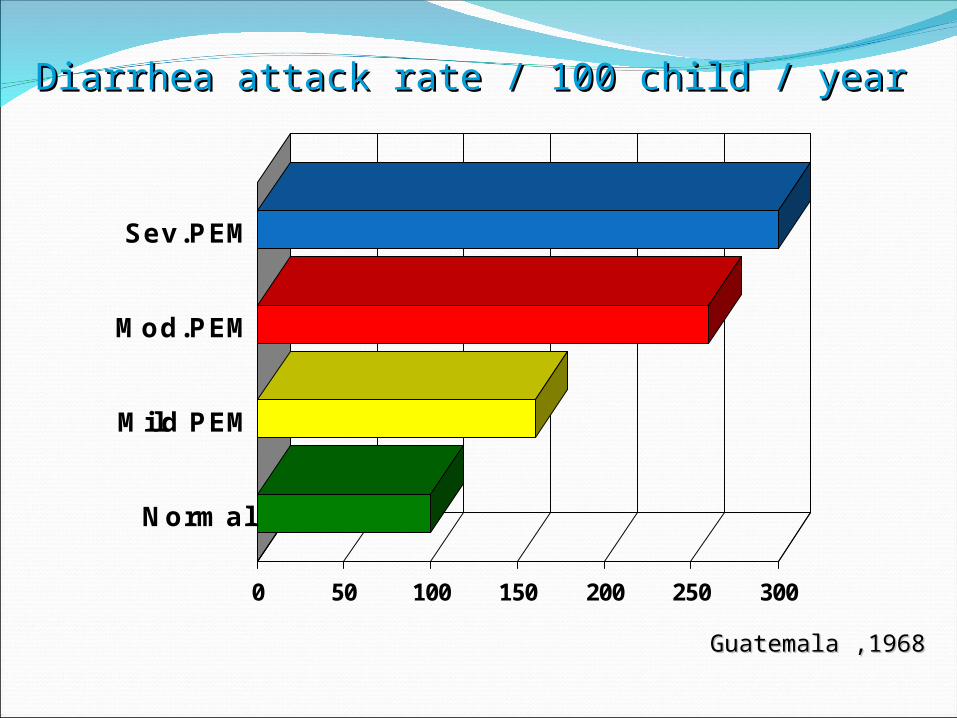
0 50 100 150 200 250 300
Normal
Mild PEM
Mod.PEM
Sev.PEM
Diarrhea attack rate / 100 child / yearDiarrhea attack rate / 100 child / year
Guatemala ,1968Guatemala ,1968

Acute Watery DiarrhoeaConstitutes 80% of cases of diarrhoea
Begins acutely, lasts less than 14 days (most episodes last less than 7 days),
Involves passage of frequent loose or watery stools without visible blood.
Vomiting may occur,Fever may be present
Main sequelae: Dehydration that can be fatalContributes to malnutrition

Dysentery (Bloody Diarrhoea)Constitutes 10% of cases of diarrhoea
Diarrhoea with visible red blood in the stools
Main sequelae:
Anorexia
Rapid weight loss
Damage to the intestinal mucosa

Persistent Diarrhoea
Constitutes 10% of cases of diarrhoea
Diarrhoea that begins acutely as watery
diarrhoea or as dysentery and lasts for 14 days
or more.
Should not be confused with chronic diarrhoea
which is recurrent or long-lasting diarrhoea
due to noninfectious causes.

WaterFood
Infected animal
Infected Person
بهداشت – فقرنامناسب

Etiology of Diarrhoea
Identification of the etiology of diarrhoea on
clinical grounds alone is not usually possible
except in epidemics or if there is history of
contact with a diagnosed case.
With the availability of modern laboratory
techniques, causative pathogens could be
identified in >75 % of cases of diarrhoea.

Etiology of DiarrhoeaThe majority of diarrhoeas occur as a result of
infection with a few pathogens which tend to recur again and again.
The most important causes of acute diarrhoea in developing countries are:
Rotavirus Enterotoxigenic Escherichia coli Shigella Campylobacter jejuni Cryptosporidium

Etiology of Acute Diarrhoea
0
2
4
6
8
10
12
14
16
18
20
Rotavirus E.E.Coli Shigella Camylobacter J. Cryptosporidium
Percent
15-25% 10-20%
5-15%10-15%
5-15%

Enteropathogens that are infectious ina small inoculum
(Shigella, enterohemorrhagic E. coli, Campylobacter
jejuni, noroviruses, rota virus, Giardia lamblia, Cryptosporidium parvum, Entamoeba histolytica)
can be transmitted by person-to-person contact,
others, such as cholera:Are generally a consequence of contamination of
food or water supply .

Food-borne outbreaks of bacterial diarrhea in the United States are most commonly due to:
Salmonella, E. coli, Clostridium botulinum,Clostridium perfringens, Staphylococcus aureus

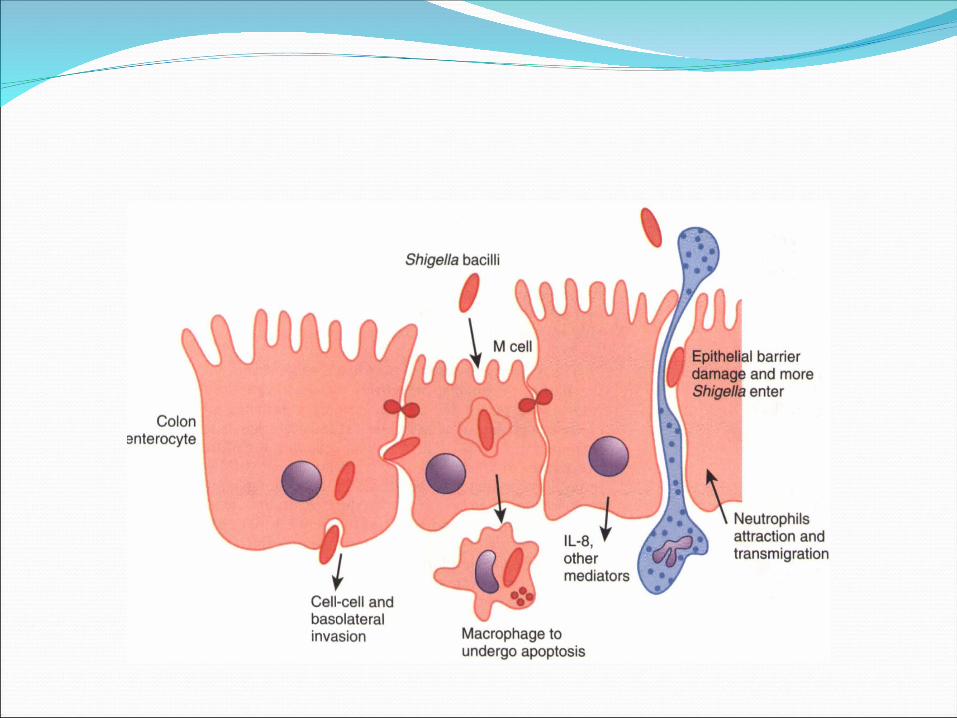
PATHOGENESIS OF INFECTIOUS DIARRHEA:
organisms have preformed toxins (S. aureus,
Bacillus cereus),?produce secretory toxin(cholera, E. coli,
Salmollella, Shigella)Adherence and/or translocation by bacteria. cytotoxic toxin (Shigella, S. aureus, Vibrio
parahemolyticus, C. difficile, E. coli, C. jejuni)invasiveMultiple

(protein NSP4 acts as a viral enterotoxin)

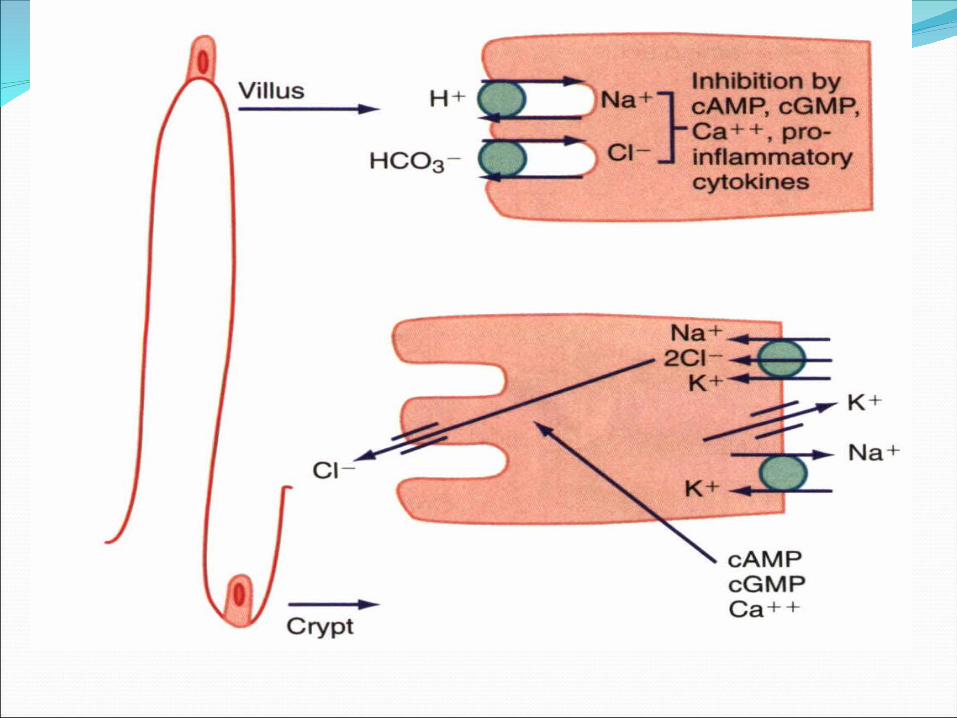
Rotavirus invades the absorptive enterocytes of villi but spares crypt cells.
The viruses replicates and infected enterocytes are destroyed

Rotavirus
Rotavirus inside enterocyte Rotavirus

1 21- Infected absorptive ente-
rocytes are killed causing patchy
epithelial cell destruc-tion and
villous shortening
2- Destroyed absorptive cells are
rapidly replaced by cells that
migrate from the crypts. So,
affected villi become temporarily
covered with immature non-
absorptive crypt-like secretory
cells having no brush border and
no brush border enzymes (e.g.
lactase)
1


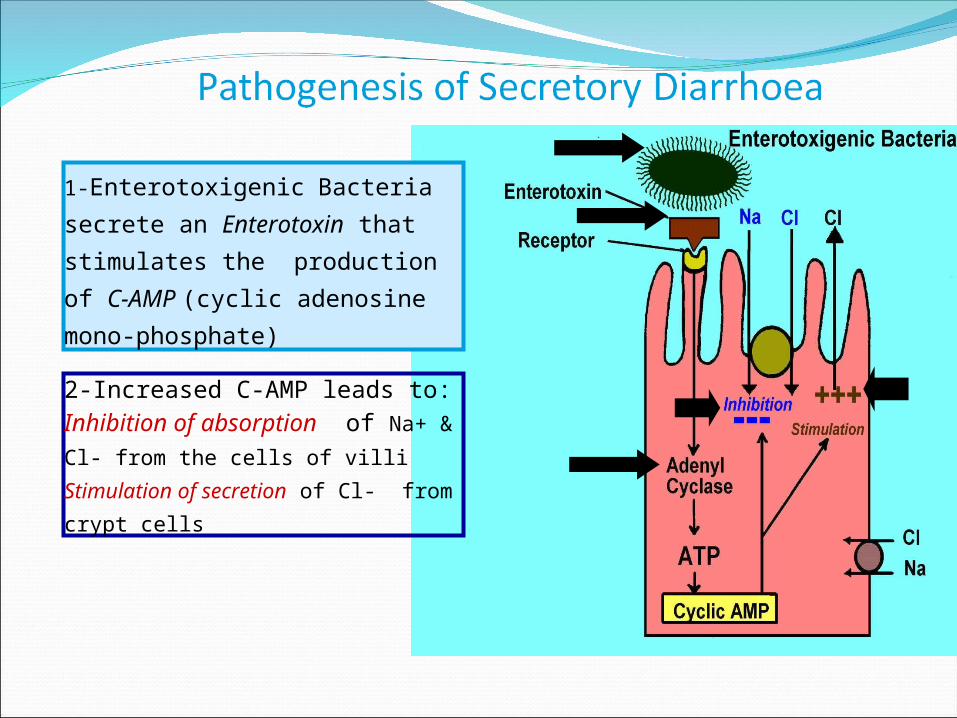
1-Enterotoxigenic Bacteria
secrete an Enterotoxin that
stimulates the production of C-
AMP (cyclic adenosine mono-
phosphate)
2-Increased C-AMP leads to:Inhibition of absorption of Na+
& Cl- from the cells of villi
Stimulation of secretion of Cl- from
crypt cells

Entero-Adherent E. Coli adherent to enterocyte of small intestine
(electron microscope X 20 000)


RISK FACTORS FOR GASTROENTERITIS:
1- environmental contamination and increased exposure to enteropathogens.
2-young age, 3-immunodeficiency,4- measles,5- malnutrition, 6- lack of exclusive or predominant breast-feeding. 7- nutritional deficiencies

Zink deficiency-21مرگ و میر ناشی از اسهال و پنومونی وماالریا را
%افزایش میدهد13
Vitamin A deficiency-24مرگ و میر ناشی از اسهال و سرخک وماالریا را
%افزایش میدهد20

clinical manifestationsSymptomatic, Asymptomatic C. jejuni Infections
clinical manifestations
There is considerable overlap in the symptomatology.
are related to the infecting pathogen and the dose or inoculum
development of complications (e.g., dehydration and electrolyte imbalance)

Usually the ingestion of preformed toxins (e.g., those of S. aureus) is associated with:
the rapid onset of nausea and vomiting within 6 hr, with possible fever, abdominal cramps, and diarrhea within 8-72 hr.

Watery diarrhea and abdominal cramps after an 8-16 hr incubation period are associated with enterotoxin-producing e. perfringens and B. cereus.

Abdominal cramps and watery diarrhea after a 16-48 hr incubation period can be associated with noroviruses, several enterotoxin-producing bacteria, Cryptosporidium, and Cyclospora and have also been a notable feature of influenza virus HINI infections.

Several organisms, including Salmonella, Shigella,
c. jejuni, Yersinia enterocolitica, enteroinvasive or hemorrhagic (Shigatoxin-producing) E. coli, and V.parahaemo/yticus, produce diarrhea that can contain blood as well as fecal leukocytes in association with abdominal cramps, tenesmus, and fever;

COMPLICATIONS:Most of the complications associated with
gastroententIs are related to delays in diagnosis and delays in the institution of appropriate therapy.
1-dehydration2- prolongation of the diarrheal episodes3-malnutrition 4- secondary infections5-In developing countries and HIV-infected
populations, associated bacteremias are well-recognized complications in malnourished children with diarrhea.
6-micronutrient deficiencies (iron, zinc).

Extra-intestinal complicationsSpecific pathogens are associated with extra
intestinal manifestations and complications
These are not pathognomonic of the infection,
nor do they always occur in close temporal association with the diarrheal episode


![Les lutins [Tarentelle]10 Ped f 'hrü/a He. Ped s/ ringendo Imp. du Denis. volando. E.I..D. O. Ped. Ped.t * Ped. *Ped.; * Grav. 8 r Ped. ppd. Ped Ped. Ped co Ped. Ped](https://img.dokumen.tips/doc/110x75/5e8dbeab73e27161bf098bf4/les-lutins-tarentelle-10-ped-f-hra-he-ped-s-ringendo-imp-du-denis-volando.jpg)