-
REVIEW ARTICLE
Diaphyseal long bone nonunions — types, aetiology, economics,and
treatment recommendations
Markus Rupp1 & Christoph Biehl1 & Matthäus Budak1 &
Ulrich Thormann1 & Christian Heiss1 & Volker Alt1
Received: 8 May 2017 /Accepted: 12 December 2017# SICOT aisbl
2017
AbstractThe intention of the current article is to review the
epidemiology with related socioeconomic costs, pathophysiology,
andtreatment options for diaphyseal long bone delayed unions and
nonunions. Diaphyseal nonunions in the tibia and in the femurare
estimated to occur 4.6–8% after modern intramedullary nailing of
closed fractures with an even much higher risk in openfractures.
There is a high socioeconomic burden for long bone nonunions mainly
driven by indirect costs, such as productivitylosses due to long
treatment duration. The classic classification of Weber and Cech of
the 1970s is based on the underlyingbiological aspect of the
nonunion differentiating between Bvital^ (hypertrophic) and
Bavital^ (hypo−/atrophic) nonunions, andcan still be considered to
represent the basis for basic evaluation of nonunions. The Bdiamond
concept^ units biomechanical andbiological aspects and provides the
pre-requisites for successful bone healing in nonunions. For
humeral diaphyseal shaftnonunions, excellent results for
augmentation plating were reported. In atrophic humeral shaft
nonunions, compression platingwith stimulation of bone healing by
bone grafting or BMPs seem to be the best option. For femoral and
tibial diaphyseal shaftfractures, dynamization of the nail is an
atraumatic, effective, and cheap surgical possibility to achieve
bony consolidation,particularly in delayed nonunions before 24
weeks after initial surgery. In established hypertrophic nonunions
in the tibia andfemur, biomechanical stability should be addressed
by augmentation plating or exchange nailing. Hypotrophic or
atrophicnonunions require additional biological stimulation of bone
healing for augmentation plating.
Keywords Fracture . Nonunion . Nailing . Plating . Bone grafting
. Tibia . Femur . Humerus
Introduction
Historically, the definition of delayed union and nonunion
isrelated to healing time. If a fracture does not heal within
ausually adequate period of time, it is first considered as
de-layed union. Despite the slow and delayed fracture
healingprocess, union of the fracture is still possible without
surgicalintervention. For nonunions, bone healing without
surgicalintervention cannot be expected [1]. According to the
UnitedStates Food and Drug Administration (FDA), a nonunion
isestablished after a minimum of nine months after trauma withno
visible progressive signs of healing for three months [2].
Epidemiology and socioeconomic cost
Nonunion rates of all fractures are estimated between 1.9%and
10% [3, 4]. It has been hypothesized that 100,000 frac-tures go on
to nonunion each year in the United States [5]. Arecent study from
Scotland found 4895 nonunion cases treatedas inpatients between
2005 and 2010, averaging 979 per year,with an overall incidence of
18.94 per 100,000 population perannum [6].
Nonunion rates vary significantly due to different
anatomicregions, soft-tissue injury, and fracture fixation
principles usedfor surgical treatment. Regarding humeral shaft
fractures,which account for 0.5 to 3% of all fractures, nonunion
ratesare reported to be higher after locked intramedullary
nailing(up to 33%), compared to plate fixation, respectively [7,
8].Femoral shaft nonunions have been reported in about 8% inmodern
antegrade nailing of femoral shaft fractures [9, 10].For tibial
shaft fractures, an overall nonunion rate of 4.6%wasreported after
intramedullary nailing for closed and open tibialshaft fractures
[11]. Vallier et al. described a nonunion rate
* Volker [email protected]
1 Department of Trauma, Hand and Reconstructive
Surgery,University Hospital Giessen-Marburg GmbH, Campus
Giessen,Rudolf-Buchheim-Str. 7, 35385 Giessen, Germany
International
Orthopaedicshttps://doi.org/10.1007/s00264-017-3734-5
http://crossmark.crossref.org/dialog/?doi=10.1007/s00264-017-3734-5&domain=pdfmailto:[email protected]
-
after intramedullary nailing of 7.1% and 4.2% after plating
ofdistal tibia shaft fractures with all nonunions occurring
afteropen fractures [12]. Regarding the impact of soft tissue
inju-ries on nonunion rates of tibial shaft fractures, Sanders et
al.showed nonunion rates of 16% in Gustilo-Anderson type II,60% in
Gustilo-Anderson type IIIA, and 80% in Gustilo-Anderson type IIIB
fractures [13]. These findings were con-firmed by a review article
from Court-Brown with 1106 casesand nonunion rates of 0–6.4% for
Gustilo-Anderson type Iand II, and of 42.1–69.2% for
Gustilo-Anderson type IIIBopen tibial fractures [14].
For the analysis of the socioeconomic burden of non-unions,
direct costs of the treatment and indirect cost, suchas
productivity losses, have to be taken into account.Antonova et al.
described a median total care cost of US$25,556 for tibial shaft
nonunions compared to US$ 11,686for those with union of tibial
shaft fractures within 24 monthsafter fracture [15]. Khunda et al.
calculated £ 26,000/patientfor the direct costs of the treatment of
complex tibial nonunionwith the Taylor spatial frame in the United
Kingdom [16].Another study from the United Kingdom estimated
directtreatment costs between £ 7000 and £ 79,000 per case forthe
National Health Service (NHS) [6].
However, indirect costs are the key driver for overall costsin
fracture and nonunion patients. Hak et al. record indirectcosts to
be 67–79% in the Canadian and 82.8–93% in theEuropean health care
systems for the overall treatment costs[5].
Aetiology, classification and risk factors
Aetiology and risk factors
BThere is no difficulty, for example, in understanding that
thematerials effused for the consolidation of a fracture can
neverbe converted into a bony callus, if subjected to frequent
mo-tion and disturbance^ — this determination is still as
validtoday as it was when first published in the 5th edition
ofAstley Coopers , Churchill, London, in 1842 [17].
Biomechanicalreasons, such as instability at the fracture site and
shear stress,seem to be major risk factors for nonunion
development.Furthermore, biological reasons, such as poor blood
supplyand severe bone and soft tissue damage, are held
responsiblefor disturbance in fracture healing including infections
andlarge bone defects. Based on these findings, Weber andCech
developed their classification oriented on surgical treat-ment of
nonunions [1] (Fig.1a and b). At first, biological via-ble and
reactive nonunions are divided due to radiologicalcriteria:
hypertrophic nonunions, so called elephant foot non-unions, are
characterized by exuberant callus formation due toinadequate
biomechanical stability; in oligotrophic nonunions
immobilizing scaffolding due to fracture diastasis is not ableto
create consolidation by callus formation. Horse’s hoof non-unions
are characterized by less callus formation and can beregarded as a
milder form of elephant foot nonunions, whichnei ther produce
immovab le s tab i l i ty nor a l lowinterfragmentary mobility.
Secondly, non-viable nonunionsare regarded as biologically
non-reactive as they show nobiological activity on bone scans. This
is mainly attributableto inadequate vascular supply to the fracture
or nonunion site.In comminuted fractures, nonunions result from
absence offracture healing between non-viable bone fragments,
whereasthe main fragments are viable and not the primary reason
fornonunion development. Third, defect nonunions are charac-terized
by bone loss, mainly caused by the trauma itself or byinfection and
subsequent sequester formation. Fourthly, atro-phic nonunions are
the final stage of non-viable nonunionswith scar tissue in the
former fracture gaps, osteoporosis,and atrophy of the main
fragments close to the fracture site[1] (Fig. 2).
Hitherto, the Weber and Cech classification is the mostpopular
classification system for nonunions. However, scien-tific evidence
does not completely support the clinical andradiological findings
described by Weber and Cech as severalsimilarities were reported in
the histological analysis of atro-phic and hypertrophic nonunions.
Fibrous, cartilaginous andconnective tissue were found in varying
degree [18], whereasatrophic nonunions were histologically
characterized as acel-lular and oligocellular compared to more
cellular hypertrophicnonunions [18]. No difference in alkaline
phosphatase (ALP)activity in cell cultures, low levels of
osteocalcin in both tis-sues, but a different cell surface antigen
profile of nonunionstromal cells for mesenchymal stem cell (MSC)
relatedmarkers was found for atrophic (CD 105) and
hypertrophic(CD13, CD29, CD44, CD90, CD105, and CD166)
nonunions[18–20]. Using an animal model for atrophic nonunions,
Reedet al. could show that the vessel density reaches the same
levelas that of healing bone but at a later time-point [21].
Hofmannreported altered cell viability and down regulated gene
expres-sion patterns for canonical Wnt-, IGF-, TGF-β-, and
FGF-signaling pathways in osteoblasts of patients suffering
fromhypertrophic nonunion compared to bone tissue samples ofhealthy
individuals [22]. Being capable of degrading extracel-lular matrix
proteins, matrix metalloproteinases (MMPs) playan important role in
extracellular matrix remodeling in varioustissues of the organism.
In enchondral fracture repair, a pivotalrole of MMPs for osteoclast
independent cartilage callus deg-radation is described [23]. In
line with impaired enchondralbone healing due to delaying cartilage
callus removal byMMP inhibition, Fajardo et al. showed an up
regulation ofMMP-7 and MMP-12 as well as binding and degrading
ofbone morphogenetic protein (BMP)-2 by both MMPsin vitro [23, 24].
Levels of Dickkopf-1 protein, an antagonistof the Wnt signaling
pathway and consequent suppressor of
International Orthopaedics (SICOT)
-
fracture repair, were higher in atrophic nonunion stromal
cellscompared to bone marrow stromal cells [18]. Furthermore,
agenetic predisposition for nonunion development was eluci-dated by
identifying polymorphisms in blood and bone callussamples of
nonunion patients [25, 26].
Risk factors
Fracture personalities and patient variables are important
riskfactors for nonunion development. Claes et al. could show
theimpact of the fracture gap size for healing time and
nonuniondevelopment in a sheep model with a critical fracture gap
sizeof 2 mm in the tibia as well as in patients with tibia
shaftfractures treated with external fixation. Fracture gaps
largerthan 10 mm showed significantly decreased healing than
frac-ture gaps smaller than 3 mm [27, 28]. The authors
emphasized
the importance of fracture reduction and minimization of
frac-ture gaps for undisturbed fracture healing for the surgical
pro-cedure. Gaebler et al. showed a higher risk for delayed
unionand nonunion in tibia shaft fractures after
unreamedintramedullary nailing for fracture gaps larger than 3 mm
aswell (OR, CI 95%: delayed union: 11.8 (5.6–24.7), nonunion:4.1
(0.96–17.8)) [29]. Drosos et al. could confirm the higherrisk for
nonunion in fractures with gaps larger than 3 mm in aretrospective
analysis of tibia shaft fractures afterintramedullary nailing
(Hazard ratio 2.69, CI 95%, 1.68–4.31). [30]. The significance of
fracture gaps
-
The Bclassical^ technical question in intramedullary nailingof
long bone shaft fractures has been for decades: to ream ornot to
ream? Reamed nailing is supposed to provide betterbiomechanical
stability due to the use of thicker nails, whereasbenefits of
unreamed nailing are seen in the conservation ofthe endosteal blood
supply. Despite several meta-analyses,this question has not been
finally answered. The above men-tioned SPRINT trial showed that
reamed compared withunreamed nailing had a statistically decreased
risk for negativeoutcomes in closed fractures [11]. However, this
relationshipwas no longer significant when autodynamization
anddynamization were removed from the composite outcome.Therefore,
final evidence on the superiority of one of the tech-niques is yet
to be provided.
Furthermore, specific patient variables and comorbiditiesare
risk factors for nonunion development. Nonunion inci-dence is
higher in men (OR, 95% CI) (1.21; 1.16–1.25).Morbidities, such as
high body mass index (1.19; 1.12–1.25), smoking (1.20; 1.14–1.26),
diabetes mellitus type I(1.40; 1.21–1.61) and II (1.15; 1.07–1.24),
osteoarthritis andrheumatism (1.58; 1.38–1.82), osteoporosis (1.24;
1.14–1.34), vitamin D deficiency (1.14; 1.05–1.22), and renal
in-sufficiency (1.11; 1.04–1.17), seem to promote nonunion
de-velopment. Moreover, nonunions are found more frequent
inpatients taking anticoagulants (1.58; 1.51–1.66),
benzodiaze-pines (1.49; 1.36–1.62), insulin (1.21; 1.10–1.31),
antibiotics(1.17; 1.13–1.21), diuretics (1.13; 1.07–1.18), NSAID,
andopioids (1.84; 1.73–1.95) [32].
Treatment options
Asmentioned above, there are bothmechanical and
biologicalunderlying factors for the development of nonunions.
Basedon these observations, Giannoudis et al. introduced the
so-called Bdiamond concept^ for successful bone healing
empha-sizing the impact of the mechanical environment,
osteogeniccells, scaffolds, and growth factors [33].
These four different aspects are discussed in the
followingparagraphs with nail dynamization being a special property
forintramedullary nailing.
Nail dynamization
In the 1970s, intramedullary locking nails for fixation of
di-aphyseal bone fractures were established as the standard
tech-nique in orthopaedic trauma care [34].
After improved bone healing due to dynamization ofintramedullary
nails was reported in fracture and delayedunion animal models [35,
36], dynamization of intramedullarynails was subsequently
recommended as the standard proce-dure after intramedullary nailing
of long bone shaft fractures[37, 38]. The underlying principle of
dynamization is based on
an enhancement of the micromovement at the fracture
siteresulting in stimulation of healing [39].
The major risk for dynamization is a possible loss of reduc-tion
with successive leg length or rotation discrepancies, par-ticularly
in patients with highly comminuted fractures [40,41]. Therefore, it
should only be performed after regainingsufficient stability of the
fracture gap against possible loss ofreduction several weeks after
initial nailing.
Unstable atrophic nonunions were outlined as risk factorsfor
dynamization, whereas unstable hypertrophic nonunionsare regarded
as suitable for nail dynamization [42]. Open frac-tures correlate
with failure of dynamization and the callusdiameter seems to be a
predictive parameter for thedynamization procedure. A high callus
to diaphysis ratio, ascan be observed in hypertrophic delayed
unions and non-union, is considered a sign of high biological
healing poten-tial. If fracture healing is achieved by
dynamization, cost sav-ings of more than US$ 10,000 per case
compared to exchangenailing treatment were estimated [43].
If dynamization is taken into consideration, perfecttiming for
this intervention has not been determined, yet.Dynamization too
early, after one week of rigid fracturefixation, shows impaired
bone formation, while latedynamization, after three or four weeks,
improves fracturehealing in an external fixator animal model [44,
45].Vaughn et al. could not show any evidence between timeof
dynamization and success rates of dynamization in fem-oral and
tibial shaft fractures [43]. Regarding the technicalprocedure,
there seems to be some evidence that bone unionrates are
significantly higher in patients with delayed unionwhen
dynamization was carried out by preserving a screwin a dynamic
locking hole (93.3%) compared to those withall screws removed at
one end of the nail (58.3%) [46].Furthermore, the group treated
with all screws removedfor dynamization showed a higher bone union
rate for earlydynamization after ten to 24 weeks (83%) compared
topatients treated with late dynamization after 24 weeks(33%) (Fig.
2). Interestingly, no difference between earlierdynamization and
dynamization after 24 weeks was ob-served in the patients with a
preserved screw in the dynamiclocking hole. The working group of
Litrenta showed nodifference in time of failed or successful
dynamization inintramedullary nailing of aseptic tibial nonunion.
They re-ported a union rate of 83% for dynamization and showedthat
a gap defined as a minimum of 5 mm distraction in anarea of no
cortical contact was a statistically negative factorfor
dynamization [47].
As the humerus is a non-weight bearing bone, dynamizationof
nails in humeral diaphyseal shaft fractures is not a soundoption.
Experimental studies could show a relatively positiverelation
between compression and bone healing. For distrac-tion, as it
occurs rather than compression in the hanging upperextremities,
reports have been inconsistent [48].
International Orthopaedics (SICOT)
-
In summary, being a quickly performed, cost saving minorsurgery,
dynamization can be recommended as first line sur-gical therapy.
Comminuted fractures and fracture gaps are riskfactors for
secondary loss of reduction after dynamization andmust definitely
be considered. Hitherto, the best timing fordynamization is not
clear, but dynamization of delayed unionis more promising than
dynamization of established femoraland tibial diaphyseal
nonunions.
Exchange nailing
The concept of reamed exchange nailing relies on the
im-provement of biomechanical stability by the use of a nail be-ing
at least one millimeter thicker in its diameter and on anBinternal
bone grafting^ by the reaming procedure with sub-sequent transport
of mesenchymal stem cells into the non-union site [49, 50].
Furthermore, longer nails with good filling of the
entireintramedullary canal and the use of more locking screws
alsocontribute to a biomechanical more stable construct [49].
Thelatest developments of implants transferred the angle
stablelocking concept in plate fixation to nails resulting in
angle-stable locking nails. Studies of the mechanical efficacy
ofthose systems are inconsistent. Mechanical stiffness seems
todepend more on the number of locking screws rather than onthe
angle-stable locking technique [51].
Regarding aseptic nonunion treatment, reamed exchangenailing in
aseptic tibial shafts can achieve high rates (97%) ofnonunion
healing [52]. In exchange nailing procedures, no sta-tistically
significant difference of time to union in statically-locked (7.3
months) versus dynamically-locked (7.9 months)exchange nails was
found. Furthermore, Abadie et al. figuredout that patients with
fibular osteotomy proceeded to union2.9 months faster than those
without fibular osteotomy, and thistrended toward significance (P =
0.067) [53]. Because the fib-ula has no statistically significant
impact on the stability ofdiaphyseal tibial fractures treated with
intramedullary nailing,it seems to be a feasible method to enable
earlier union (Fig. 3).
In femur shaft nonunions, a success rate of 86% healed
non-unions four months after revision surgery has been shown
[54].Hak et al. reported an overall success rate of 78.9% in
ex-changed reamed nailing of femur shaft nonunions, whereby
riskfactors such as smoking reduced the success rate to 66%
[55].According to Tsang et al., infection, bone gaps of more than5
mm, and an atrophic pattern of nonunion were
statisticallysignificant risk factors for failure of exchange
nailing in tibiashaft fracture. Only 11 out of 31 infected
nonunions (35.4%)healed after one exchange nail procedure [56]. In
humeral shaftnonunions, inconsistent results of exchange nailing
have beenreported. Lin et al. reported in 22 patients out of 23
(95.6%)bony union after revision exchange nailing. Nonunions
wereaddressed with open reduction, additional K-wire fixation,
andeither antegrade or retrograde nailing in 19 cases [57]. McKeeet
al. compared exchange nailing with open reduction, platefixation,
and autogenous bone grafting. Four out of ten (40%)exchange nail
procedures resulted in bony consolidation,whereas in nine out of
nine cases consolidation was achievedby plate fixation and
autologous bone graft application [58]. Aconsolidation rate of
46.1% (6/13) after exchange nailing forhumeral shaft nonunions is
described by Flinkkilä [59]. A re-cent review on union rates after
surgical treatment of humeralshaft nonunions showed the highest
healing rate of 98% inpatients who underwent plate fixation with
autologous bonegrafting (ABG) compared to plate fixation without
bonegrafting (95%). In contrast to plate fixation, union rates
werelower in revision surgery with intramedullary nailing: 88%
forintramedullary nailing with ABG (n = 164) and 66%
forintramedullary nailing without ABG (n = 78). External
fixationalso yielded a high healing rate of 98%, but was associated
withthe highest complication rate [8].
Bone grafts and bone morphogenetic proteins
In the case of atrophic nonviable nonunions, biological
issuessuch as poor vascular supply are considered to be the
mainreason of nonunion development. Besides improvement of the
a db cFig. 2 X-rays series of a delayed union treated with
dynamization of thenail after surgical treatment of an AO type 42
A1 fracture with closedreduction and internal fixation (CRIF) by
locked reamed intramedullarynailing a X-rays at 6 weeks after CRIF
with a locked reamed tibia nail,pain-adapted full load was allowed.
b X-rays 12 weeks after CRIF and
after full weight-bearing of 6 weekswith absence of fracture gap
bridging.Decision for dynamization was made and carried out after
12 weeks. cX-rays 4 weeks after dynamization with removal of both
proximal staticlocking bolts, d X-rays after 12 weeks after
dynamization with consoli-dation of the fracture
International Orthopaedics (SICOT)
-
mechanical stability, the purpose of the surgical therapy is
toaddress and to improve the biological environment accordingto the
Bdiamond concept^ [33].
Autogenous bone grafting provides all required properties
forbone formation: osteogenesis, osteoconduction andosteoinduction,
and is associated with low costs, absence ofdisease transmission or
rejection of the graft [60, 61]. Classicalharvest sites for
cancellous autogenous bone grafting are theiliac crest, proximal
tibia, distal tibia, and the distal radius.
General limitations of autogenous bone grafting are
limitedavailability and donor site morbidity, such as chronic
donorsite pain, wound complications, such as seroma or
infections,sensory loss, and scarring [62, 63].
For cortical bone grafts of the iliac crest, slower
revascu-larization, bone resorption, and transformation are
describeddue to a lower amount of available and biological active
cellsin the graft [64]. Vascularized bone graft techniques
wereestablished to overcome these limitations, with
freevascularized fibula bone grafts being the most frequently
usedtechnique [65].
The reamer-irrigator-aspirator (RIA) is an alternative meth-od
for the harvesting of autogenous cancellous bone graftmaterial from
the intramedullary canal of the femur by anintramedullary reaming
system and high union rates were re-ported for RIA bone grafts in
the treatment of nonunions [66].A recent study showed significantly
lower complications ratesin donor site morbidity compared to the
iliac crest [67].
Allograft is available in many forms: cancellous,
cortical,corticocancellous, osteochondral, and whole-bone
segments.Major drawback is its lack of osteogenic potential as all
cellsare removed during the production. Therefore, allografts
pri-marily serve as structural scaffold exhibiting
osteoconductivepotential [60, 68]. After cases of transmission of
blood bornediseases such as HIV were reported in the 1980s and
1990s,screening methods as well as new methods of processing
andpreparation of bone grafts were established. Between 1990and
2000more than 1,000,000 bone allografts were implantedwithout a
reported evidence of HIV or hepatitis transmissionin the US [69].
The risk of viral transmission associated withblood is reported for
hepatitis B as one in 63,000, for hepatitis
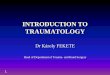
Fig. 3 X-rays series of anonunion treated with exchangenailing
11 months after surgicaltreatment of an AO type 42 C2fracture with
CRIF by lockedreamed intramedullary nailing. aNo bony consolidation
wasobserved 7 months after CRIF. bCoronal CTsections show the gap9
months after initial surgery,nonunion. c Postoperativecontrols
after exchange nailing ofthe tibia with a dynamically-locked tibial
nail and fibulaosteotomy 11 months after initialsurgery. d 6 weeks
postoperativecontrols after exchange nailingshow beginning bony
consolida-tion. e 3 months after revisionsurgery advanced
consolidationwas documented. f 6 months afterexchange nailing
X-rays showcomplete fracture consolidation
International Orthopaedics (SICOT)
-
C it is one in 100,000 and for HIV less than one in
1,000,000[70]. A further drawback of bone allograft implantation
islocal infection of the allograft. The main reason for infectionis
contamination of the graft. Contamination rates up to 10%and an
overall infection rate of implanted allograft bone be-tween 5 and
12.2% are reported [71, 72].
In 1965, M. Urist was the first to describe theosteoinductive
potential of demineralized bone matrix(DBM) and to discover the
underlying BMPs, which belongto the transforming growth factor-β
(TGF-β) protein super-family [73, 74].
In 2001, the FDA approved recombinant human (rh)BMP-2
(dibotermin alfa, Inductos® Medtronic, Minneapolis, MN)for the
treatment of acute tibia fractures in adults, as an adjunctto
standard care using open fracture reduction andintramedullary
unreamed nail fixation and for single levellumbar interbody spine
fusion as a substitute for autogenousbone graft in adults. RhBMP-7
(eptotermin alfa, Osigraft®Olympus Biotech, Hopkinton, MA) was
approved by theFDA in 2002 for the treatment of tibia nonunion of
at leastnine months duration, secondary to trauma, in skeletally
ma-ture patients, in cases where previous treatment with
autografthas failed or use of autograft was unfeasible. The trial
ofFriedlaender et al. showed comparable clinical success
ratesbetween rhBMP-7 (81%) and autogenous bone graft (85%) asan
adjunct to intramedullary nailing in 124 tibial shaft non-unions
after an observation period of nine months. This trialhad a
non-inferiority study design to demonstrate safety andefficacy and
was not intended to show superiority of rhBMP-7over autogenous bone
grafting.
Currently, there is still a lack of sound randomized con-trolled
trials on the effects of BMPs compared to standard ofcare treatment
in nonunions, mainly attributable to the re-quired large sample
size with several hundreds of patientsand associated high costs for
such a clinical study.
However, the general concept of stimulation of bonehealing by
BMPs [75] was confirmed in several case reportsand case series for
nonunions of long bones of the upper [76,77] and lower extremity
[78, 79] with good success rates.
Recently, Olympus Biotech shut down its activities forrhBMP-7
and rhBMP-2 currently remains the only commer-cially available
BMP.
Cell therapy
The initial phase of bone healing is characterized by the
onsetof inflammation. MSCs, endothelial cells and immune
cellsmigrate toward the fractured bone region.
Osteoprogenitorcells, originating from the periosteum, the bone
marrow, andthe surrounding tissue react to the signals sent by
thehaematoma and migrate into the fracture area [80]. Hence, itis
not surprising that low levels of progenitor cells at nonunionsites
and in bonemarrow of nonunion patients [81] as well as a
systemic mesenchymal and osteogenic cell pool defect
wereobserved [82]. To improve the cellular environment in a
dis-turbed bone healing process, the application of bone marrowwas
proposed due to its osteogenic potential, which was firstobserved
by Gougeon in the nineteenth century [83]. Later,Friedenstein et
al. showed that new bone was formed byfibroblast-like bone marrow
cells in vitro after necrosis ofhematopoietic cells, which led to
the first isolation of MSCsin this context [84]. Furthermore, it
could be shown that thosecells are multipotent and can
differentiate to osteocytic,chondrocytic, and adipocytic lineages
[85]. Before isolatingMSCs from bonemarrow, several preclinical and
clinical stud-ies had confirmed the efficiency of bone marrow
implantationto induce bony regeneration [86, 87].
Bruder et al. were the first to demonstrate that MSCs iso-lated
from human bone marrow can regenerate bone in a largebone defect
[88]. Based on these findings, several clinicalstudies were
performed using MSCs in a single or combinedmanner with
osteoconductive or osteoinductive substances.Homma et al. described
the use of percutaneous autologousbone marrow cell grafting as an
efficient and safe treatment.Their one step technique includes the
aspiration of bone mar-row at the iliac crest and pooling of the
harvested cells inplastic bags containing cell culture medium and
anticoagulantsolution. After filtration to separate cellular
aggregates, theaspirate is percutaneously injected with a trocar at
the non-union gap and its respective bone ends under
fluoroscopy[89]. Bajada’s group showed union of a recalcitrant
tibial non-union with application of expanded bonemarrow stromal
cellsafter three weeks of tissue culture combined with a carrier
ofcalcium sulfate in pellet form [90]. Hernigou et al. found
acorrelation between the number and concentration of progen-itor
cells applied at the nonunion site and subsequent boneformation in
percutaneous autologous bone grafting [91].Quarto et al. described
a case series of patients with diaphysealbone defects treated by ex
vivo expanded osteoprogenitorcells placed on macroporous
hydroxyapatite scaffolds [92].Another approach was conducted by
Wittig et al. with theloading of MSCs on collagen microspheres (CM)
and theirincorporation into platelet-rich plasma (PRP) clots. This
com-bination ofMSCswas shown to induce new bone formation inlong
bone nonunions [93]. In total, promising results in non-union
treatment by local cell therapy are reported. However,there is
still a lack of evidence on the optimal cell harvesting,processing,
and application technique.
External fixation techniques for nonunions
External fixation for nonunion treatment offers high
stabilityand compression to the nonunion site to achieve bony
consol-idation. Furthermore, bone resection with or without
shorten-ing with subsequent bone segment transport or
lengtheningcan be performed. Drawbacks are foremost pin
loosening
International Orthopaedics (SICOT)
-
and pin infections and patient discomfort with long
treatmentduration [94]. Furthermore, regenerate related problems
suchas poor bone quality, delayed maturation, premature
consoli-dation, and docking site problems requiring revision
surgeryincluding bone grafting have been described [95].
Both monolateral and ring fixation systems have been
usedsuccessfully for the treatment of nonunions. High union ratesof
91.6% were reported by Harshwal et al. in 37 patientssuffering from
femoral or tibial nonunions treated with amonolateral external
fixator. Of these 37 patients, 32 weretreated by compression
osteosynthesis (monofocal), in six ofthem distraction osteogenesis
was carried out after initial com-pression of the nonunion site.
Five patients were treated by abifocal protocol with corticotomy
and bone transport due tobony defects larger than 3 cm in the tibia
and 5 cm in thefemur, respectively [96].
After failed exchange nailing in aseptic and oligotrophicfemoral
shaft nonunions, consolidation of the nonunion sitecan be achieved
using the Ilizarov fixator technique over the
indwelling nail with slow compression rates (0.25–0.5mmperday)
[97]. This has also been described in aseptic humeralshaft
nonunions for the combination of Ilizarov or monolateralexternal
fixators for compression in combination with anintramedullary
fixation device [98].
Resection of the nonunion site allows for a radical removalof
fibrous and scar tissue but can result in segmental defectslarger
than 5 cm that can be restored by corticotomy at theremaining
proximal or distal bone segment with daily gradualdistraction of
this bone segment through an external fixatorapparatus [99].
Traditionally, Ilizarov ring fixators were usedfor distraction
osteogenesis and bone transport but alsomonolateral techniques have
gained more and more interestdue to easier pin insertion and
uniplanar application [99].Modern circular fixators like the Taylor
spatial frame providenot only distraction options but also
correction of bone defor-mity in all planes [16].
In general, a daily distraction rate of 1 mm is recommendedand
provides sufficient osteogenic potential [100] but needs to
Fig. 4 Series of a femoral shaft nonunion after an AO type 32 B3
fracturefinally treated with augmentation plating. a Nonunion 7
months afterexchange nailing, autologous bone grafting, and rhBMP-2
application.
b Postoperative controls after augmentation plating with a
locking plate. cX-rays 6 weeks after augmentation plating. d
Consolidation 3 monthsafter augmentation plating
Table 1 Treatment recommendations for delayed unions and
humeral, femoral, and tibial diaphyseal nonunions without segmental
bone defects
Delayed union Hypertrophic nonunion Hypotrophic and atrophic
nonunion
Humeral shaft Augmentation plating after failednailing [109]
Compression plating with bone grafting [110]augmentation plating
after nailing [109]
Femoral shaft Nail dynamization [111] or earlyaugmentation
plating [104, 106]
Augmentation plating with or withoutbone grafting [104, 106]
§
Augmentation plating with biological stimulation bybone grafting
or biologics [104, 106, 112, 113] §
Tibial shaft Nail dynamization [47]or early exchange nailing
[52]
Reamed exchange nailing [52, 56] oraugmentation plating [107,
108]
Reamed exchange nailing or augmentation platingwith biological
stimulation by bone grafting or biologics
[52, 114]
§ Because of lower success rates for exchange nailing of femoral
shaft fractures compared to augmentation plating, exchange nailing
is regarded assecond line therapy
International Orthopaedics (SICOT)
-
be adapted to patients’ individual factors. Fixators should
beleft about 1.9 months for every 1 cm of bone defect to
reachadequate and stable bony consolidation [101]. To reduce
theduration of external fixation, the adjunct use of internal
fixa-tion devices has been described [102, 103].
Augmentation plating
The improvement of biomechanical stability in diaphyseallong
bone nonunions has directed attention to additional platefixation
use after failed intramedullary nailing. Mainly rota-tional
instability seems to be an important factor in the devel-opment of
nonunions, which can be addressed by augmenta-tion plating [104,
105]. Ueng et al. reported a case series on 17diaphyseal femoral
nonunions with augmentation plating plusadditional bone grafting
from the iliac crest without removalof the nail after failed
intramedullary nailing. In all 17 patients,nonunions healed at a
mean follow-up of seven months afteraugmentative plate fixation
without complications [104]. Asshown in Fig. 4, femoral shaft
nonunions can be addressedeffectively by augmentation plating. In
this complex case,healing of the nonunion was reached by
augmentation platingimprovingmechanical instability, which was the
result of a toosmall nail diameter and a remaining fracture gap
after initialimprovement worthy reduction of an AO type 32 B3
fracture.Meanwhile several studies confirmed the excellent result
ofaugmentation plating for femoral, tibial, and humeral
shaftfractures. In femur shaft nonunions, high success rates of100%
of augmentation plating with or without autologousbone grafting
were reported [106, 107]. For tibial shaft non-unions, augmentation
plating also shows a good result be-tween 84.6% [107] and 96.4%
[108]. For humeral shaft non-unions augmentation plating seems to
be an excellent thera-peutic approach, too. Gessmann et al.
reported a 97% successrate of anterior augmentation plating after
antegrade or retro-grade intramedullary nailing [109].
Conclusions and treatment recommendations
Surgical treatment of aseptic nonunions should still be
per-formed according to the Weber-Cech classification. It
remainschallenging for the patient and the surgeon, and is
associatedwith significant costs for the health care system.
For humeral diaphyseal shaft nonunions, excellent resultsfor
augmentation plating were reported. In atrophic humeralshaft
nonunions, compression plating with stimulation of bonehealing by
bone grafting or BMPs seems to be the best option(Table 1).
For femoral and tibial diaphyseal shaft fractures,dynamization
of the nail is an atraumatic, effective, and cheapsurgical
possibility to achieve bony consolidation, particularlyin delayed
nonunions before 24 weeks after initial surgery. In
established hypertrophic nonunions, biomechanical
stabilityshould be addressed by augmentation plating or
exchangenailing. Hypotrophic or atrophic nonunions additionally
requirebiological stimulation of bone healing for augmentation
plating.
For segmental bone defects, external fixation techniquesremain
the treatment of choice. Patient comfort and successrates can be
positively influenced by the additional use ofinternal fixation
devices.
References
1. Weber BG, Cech O (1973) Pseudarthrosen.
PathophysiologieBiomechanik Therapie Ergebnisse. Huber, Bern
2. Frolke JP, Patka P (2007) Definition and classification of
fracturenon-unions. Injury 38(Suppl 2):S19–S22
3. Einhorn TA (1995) Enhancement of fracture-healing. J Bone
JointSurg Am 77:940–956
4. Mills LA, Aitken SA, Simpson AHR (2017) The risk of non-union
per fracture: current myths and revised figures from a pop-ulation
of over 4 million adults. Acta Orthop 88:434-439.
https://doi.org/10.1080/17453674.2017.1321351
5. Hak DJ, Fitzpatrick D, Bishop JA, Marsh JL, Tilp S,
Schnettler R,Simpson H, Alt V (2014) Delayed union and nonunions:
epide-miology, clinical issues, and financial aspects. Injury
45(Suppl 2):S3–S7. https://doi.org/10.1016/j.injury.2014.04.002
6. Mills LA, Simpson AH (2013) The relative incidence of
fracturenon-union in the Scottish population (5.17 million): a
5-year epi-demiological study. BMJ Open.
https://doi.org/10.1136/bmjopen-2012-002276
7. Nandra R, Grover L, Porter K (2015) Fracture non-union
epide-miology and treatment. Trauma 18:3–11.
https://doi.org/10.1177/1460408615591625
8. Peters RM, Claessen FM, Doornberg JN, Kolovich GP, DiercksRL,
van den BekeromMP (2015) Union rate after operative treat-ment of
humeral shaft nonunion–a systematic review. Injury 46:2314–2324.
https://doi.org/10.1016/j.injury.2015.09.041
9. Giannoudis P, MacDonald D, Matthews S, Smith R, Furlong A,De
Boer P (2000) Nonunion of the femoral diaphysis. Bone Joint
J82:655–658
10. Canadian Orthopaedic Trauma S (2003) Nonunion
followingintramedullary nailing of the femur with and without
reaming.Results of a multicenter randomized clinical trial. J Bone
JointSurg Am Vol 85-A:2093–2096
11. Investigators SPERINPTF (2008) Randomized trial of reamed
andunreamed intramedullary nailing of tibial shaft fractures. J
BoneJoint Surg Am 90:2567
12. Vallier HA, Cureton BA, Patterson BM (2011) Randomized,
pro-spective comparison of plate versus intramedullary nail
fixationfor distal tibia shaft fractures. J Orthop Trauma
25:736–741.https://doi.org/10.1097/BOT.0b013e318213f709
13. Sanders R, Jersinovich I, Anglen J, DiPasquale T, Herscovici
D Jr(1994) The treatment of open tibial shaft fractures using
aninterlocked intramedullary nail without reaming. J OrthopTrauma
8:504–510
14. Court-Brown CM (2004) Reamed intramedullary tibial nailing:
anoverview and analysis of 1106 cases. J Orthop Trauma
18:96–101
15. Antonova E, Le TK, Burge R, Mershon J (2013) Tibia shaft
frac-tures: costly burden of nonunions. BMC Musculoskelet
Disord14:42
International Orthopaedics (SICOT)
https://doi.org/10.1080/17453674.2017.1321351https://doi.org/10.1080/17453674.2017.1321351https://doi.org/10.1016/j.injury.2014.04.002https://doi.org/10.1136/bmjopen-2012-002276https://doi.org/10.1136/bmjopen-2012-002276https://doi.org/10.1177/1460408615591625https://doi.org/10.1177/1460408615591625https://doi.org/10.1016/j.injury.2015.09.041https://doi.org/10.1097/BOT.0b013e318213f709
-
16. Khunda A, Al-Maiyah M, Eardley W, Montgomery R (2016)
Themanagement of tibial fracture non-union using the Taylor
spatialframe. J Orthop 13:360–363
17. Cooper A (1842) A treatise on dislocations and fractures of
thejoints. Churchill, London
18. Bajada S, Marshall MJ, Wright KT, Richardson JB, Johnson
WE(2009) Decreased osteogenesis, increased cell senescence and
el-evated Dickkopf-1 secretion in human fracture non union
stromalcells. Bone 45:726–735.
https://doi.org/10.1016/j.bone.2009.06.015
19. Iwakura T, MiwaM, Sakai Y, Niikura T, Lee SY, Oe K,
HasegawaT, Kuroda R, Fujioka H, Doita M (2009) Human
hypertrophicnonunion tissue contains mesenchymal progenitor cells
withmultilineage capacity in vitro. J Orthop Res 27:208–215
20. Panteli M, Pountos I, Jones E, Giannoudis PV (2015)
Biologicaland molecular profile of fracture non-union tissue:
current in-sights. J Cell Mol Med 19:685–713
21. Reed A, Joyner C, Brownlow H, Simpson A (2002) Human
atro-phic fracture non-unions are not avascular. J Orthop Res
20:593–599
22. Hofmann A, Ritz U, HessmannM, Schmid C, Tresch A, Rompe
J,Meurer A, Rommens P (2008) Cell viability, osteoblast
differen-tiation, and gene expression are altered in human
osteoblasts fromhypertrophic fracture non-unions. Bone
42:894–906
23. McDonald MM, Morse A, Mikulec K, Peacock L, Baldock
PA,Kostenuik PJ, Little DG (2013) Matrix
metalloproteinase–drivenendochondral fracture union proceeds
independently of osteoclastactivity. J Bone Miner Res
28:1550–1560
24. Fajardo M, Liu C-J, Ilalov K, Egol KA (2010) Matrix
metallopro-teinases that associate with and cleave bone
morphogeneticprotein-2 in vitro are elevated in hypertrophic
fracture nonuniontissue. J Orthop Trauma 24:557–563
25. Zeckey C, Hildebrand F, Glaubitz LM, Jürgens S, Ludwig
T,Andruszkow H, Hüfner T, Krettek C, Stuhrmann M (2011)
Arepolymorphisms of molecules involved in bone healing correlatedto
aseptic femoral and tibial shaft non-unions? J Orthop Res
29:1724–1731
26. Xiong D-H, Liu X-G, Guo Y-F, Tan L-J, Wang L, Sha B-Y,
TangZ-H, Pan F, Yang T-L, Chen X-D (2009) Genome-wide associa-tion
and follow-up replication studies identified ADAMTS18 andTGFBR3 as
bone mass candidate genes in different ethnic groups.Am J Hum Genet
84:388–398
27. Claes L, Augat P, Suger G, Wilke HJ (1997) Influence of size
andstability of the osteotomy gap on the success of fracture
healing. JOrthop Res 15:577–584
28. Claes L, Grass R, Schmickal T, Kisse B, Eggers C, Gerngross
H,Mutschler W, Arand M, Wintermeyer T, Wentzensen A
(2002)Monitoring and healing analysis of 100 tibial shaft
fractures.Langenbeck's Arch Surg 387:146–152
29. Gaebler C, Berger U, Schandelmaier P, Greitbauer
M,Schauwecker HH, Applegate B, Zych G, Vecsei V (2001) Ratesand
odds ratios for complications in closed and open tibial frac-tures
treated with unreamed, small diameter tibial nails: a multi-center
analysis of 467 cases. J Orthop Trauma 15:415–423
30. Drosos G, Bishay M, Karnezis I, Alegakis A (2006) Factors
af-fecting fracture healing after intramedullary nailing of the
tibialdiaphysis for closed and grade I open fractures. Bone Joint J
88:227–231
31. Schemitsch EH, Bhandari M, Guyatt G, Sanders DW,Swiontkowski
M, Tornetta P, Walter SD, Zdero R, Goslings JC,Teague D, Jeray K,
McKee MD, Study to Prospectively EvaluateReamed Intramedullary
Nails in Patients with Tibial Fractures I(2012) Prognostic factors
for predicting outcomes afterintramedullary nailing of the tibia. J
Bone Joint Surg Am 94:1786-1793.
https://doi.org/10.2106/JBJS.J.01418
32. Zura R, Xiong Z, Einhorn T, Watson JT, Ostrum RF, Prayson
MJ,Della Rocca GJ, Mehta S, McKinley T, Wang Z, Steen RG
(2016)Epidemiology of fracture nonunion in 18 human bones. JAMASurg
151:e162775. https://doi.org/10.1001/jamasurg.2016.2775
33. Giannoudis PV, Einhorn TA,Marsh D (2007) Fracture healing:
thediamond concept. Injury 38:S3–S6
34. Klemm K, Schellmann W (1972) Dynamische und
statischeVerriegelung des Marknagels. Monatsschr Unfallheilkd
75:303
35. Egger EL, Gottsauner-Wolf F, Palmer J, Aro HT, Chao E
(1993)Effects of axial dynamization on bone healing. J Trauma
34:185–192
36. Claes L, Wilke H, Augat P, Rübenacker S, Margevicius K
(1995)Effect of dynamization on gap healing of diaphyseal
fracturesunder external fixation. Clin Biomech 10:227–234
37. Kempf I, Grosse A, Beck G (1985) Closed locked
intramedullarynailing. Its application to comminuted fractures of
the femur. JBone Joint Surg Am Vol 67:709–720
38. Foxworthy M, Pringle R (1995) Dynamization timing and its
ef-fect on bone healing when using the Orthofix dynamic
axialFixator. Injury 26:117–119
39. Glatt V, Evans CH, Tetsworth K (2016) A concert between
biol-ogy and biomechanics: the influence of the mechanical
environ-ment on bone healing. Front Physiol 7:678.
https://doi.org/10.3389/fphys.2016.00678
40. Pihlajamäki HK, Salminen ST, Böstman OM (2002) The
treat-ment of nonunions following intramedullary nailing of
femoralshaft fractures. J Orthop Trauma 16:394–402
41. Wu CC (1997) The effect of dynamization on slowing the
healingof femur shaft fractures after interlocking nailing. J
Trauma 43:263–267
42. Papakostidis C, Psyllakis I, Vardakas D, Grestas A,
GiannoudisPV (2011) Femoral-shaft fractures and nonunions treated
withintramedullary nails: the role of dynamisation. Injury
42:1353–1361
43. Vaughn J, Gotha H, Cohen E, Fantry AJ, Feller RJ, Van Meter
J,Hayda R, Born CT (2016) Nail Dynamization for delayed unionand
nonunion in femur and tibia fractures. Orthopedics 39:e1117–e1123.
https://doi.org/10.3928/01477447-20160819-01
44. Claes L, Blakytny R, Göckelmann M, Schoen M, Ignatius
A,Willie B (2009) Early dynamization by reduced fixation
stiffnessdoes not improve fracture healing in a rat femoral
osteotomymod-el. J Orthop Res 27:22–27
45. Claes L, Blakytny R, Besse J, Bausewein C, Ignatius A,
Willie B(2011) Late dynamization by reduced fixation stiffness
enhancesfracture healing in a rat femoral osteotomy model. J
OrthopTrauma 25:169–174
46. Huang KC, Tong KM, Lin YM, Loh el W, Hsu CE (2012)Evaluation
of methods and timing in nail dynamisation fortreating delayed
healing femoral shaft fractures. Injury 43:1747-1752.
https://doi.org/10.1016/j.injury.2012.06.024
47. Litrenta J, Tornetta P 3rd, Vallier H, Firoozabadi R,
Leighton R,Egol K, Kruppa C, Jones CB, Collinge C, Bhandari
M,Schemitsch E, Sanders D, Mullis B (2015) Dynamizations
andexchanges: success rates and indications. J Orthop Trauma
29:569–573. https://doi.org/10.1097/BOT.0000000000000311
48. Ghiasi MS, Chen J, Vaziri A, Rodriguez EK, Nazarian A
(2017)Bone fracture healing in mechanobiological modeling: a review
ofprinciples andmethods. Bone reports 6:87–100.
https://doi.org/10.1016/j.bonr.2017.03.002
49. Brinker MR, O'connor DP (2007) Exchange nailing of
ununitedfractures. The Journal of Bone & Joint Surgery
89:177–188
50. Wenisch S, Trinkaus K, Hild A, Hose D, Herde K, Heiss C,
KilianO, Alt V, Schnettler R (2005) Human reaming debris: a source
ofmultipotent stem cells. Bone 36:74–83
51. Hoffmann S, Gerber C, von Oldenburg G, Kessler M, Stephan
D,Augat P (2015) Effect of angular stability and other locking
International Orthopaedics (SICOT)
https://doi.org/10.1016/j.bone.2009.06.015https://doi.org/10.1016/j.bone.2009.06.015https://doi.org/10.2106/JBJS.J.01418https://doi.org/10.1001/jamasurg.2016.2775https://doi.org/10.3389/fphys.2016.00678https://doi.org/10.3389/fphys.2016.00678https://doi.org/10.3928/01477447-20160819-01https://doi.org/10.1016/j.injury.2012.06.024https://doi.org/10.1097/BOT.0000000000000311https://doi.org/10.1016/j.bonr.2017.03.002https://doi.org/10.1016/j.bonr.2017.03.002
-
parameters on the mechanical performance of intramedullarynails.
Biomed Tech (Berl) 60:157–164.
https://doi.org/10.1515/bmt-2014-0100
52. Hierholzer C, Friederichs J, Glowalla C, Woltmann A, Buhren
V,von Ruden C (2016) Reamed intramedullary exchange nailing inthe
operative treatment of aseptic tibial shaft nonunion. Int
Orthop.https://doi.org/10.1007/s00264-016-3317-x
53. Abadie B, Leas D, Cannada L, Malm P, Morwood M, Howes C,Zura
R, Healy K, Avery M, Schlatterer D (2016) Does screwconfiguration
or fibular Osteotomy decrease healing time in ex-change Tibial
nailing? J Orthop Trauma 30:622–626
54. Shroeder JE, Mosheiff R, Khoury A, Liebergall M, Weil
YA(2009) The outcome of closed, intramedullary exchange nailingwith
reamed insertion in the treatment of femoral shaft nonunions.J
Orthop Trauma 23:653–657
55. Hak DJ, Lee SS, Goulet JA (2000) Success of exchange
reamedintramedullary nailing for femoral shaft nonunion or
delayedunion. J Orthop Trauma 14:178–182
56. Tsang ST, Mills LA, Frantzias J, Baren JP, Keating JF,
SimpsonAH (2016) Exchange nailing for nonunion of diaphyseal
fracturesof the tibia: our results and an analysis of the risk
factors forfailure. Bone Joint J 98-B:534–541.
https://doi.org/10.1302/0301-620X.98B4.34870
57. Lin J, Chiang H, Hou S-M (2003) Open exchange locked
nailingin humeral nonunions after intramedullary nailing. Clin
OrthopRelat Res 411:260–268
58. McKeeMD,Miranda MA, Riemer BL, Blasier RB, Redmond BJ,Sims
SH, Waddell JP, Jupiter JB (1996) Management of humeralnonunion
after the failure of locking intramedullary nails. J OrthopTrauma
10:492–499
59. Flinkkilä T, Ristiniemi J, Hämäläinen M (2001) Nonunion
afterintramedullary nailing of humeral shaft fractures. J Trauma
AcuteCare Surg 50:540–544
60. Sen MK, Miclau T (2007) Autologous iliac crest bone
graft:should it still be the gold standard for treating nonunions?
Injury38(Suppl 1):S75–S80.
https://doi.org/10.1016/j.injury.2007.02.012
61. Megas P (2005) Classification of non-union. Injury 36(Suppl
4):S30–S37. https://doi.org/10.1016/j.injury.2005.10.008
62. Dekker TJ, White P, Adams SB (2016) Efficacy of a cellular
boneallograft for foot and ankle arthrodesis and revision
nonunionprocedures. Foot Ankle Int 1071100716674977
63. Dawson J, Kiner D,Warren Gardner I, Swafford R, Nowotarski
PJ(2014) The reamer–irrigator–aspirator as a device for
harvestingbone graft compared with iliac crest bone graft: union
rates andcomplications. J Orthop Trauma 28:584–590
64. Khan SN, Cammisa FP Jr, Sandhu HS, Diwan AD, Girardi FP,Lane
JM (2005) The biology of bone grafting. J Am AcadOrthopaed Surg
13:77–86
65. Griffin KS, Davis KM, McKinley TO, Anglen JO, Chu
T-MG,Boerckel JD, KacenaMA (2015) Evolution of bone grafting:
bonegrafts and tissue engineering strategies for vascularized bone
re-generation. Clin Rev Bone Mineral Metab 13:232–244
66. Cox G, Jones E, McGonagle D, Giannoudis PV (2011)
Reamer-irrigator-aspirator indications and clinical results: a
systematic re-view. Int Orthop 35:951–956
67. Calori G, ColomboM,Mazza E, Mazzola S,Malagoli E,Mineo
G(2014) Incidence of donor site morbidity following harvestingfrom
iliac crest or RIA graft. Injury 45:S116–S120
68. Emara KM, Diab RA, Emara AK (2015) Recent biological
trendsin management of fracture non-union. World J Orthoped
6:623
69. Tomford WW (2000) Bone allografts: past, present and
future.Cell Tissue Bank 1:105–109
70. Roberts TT, Rosenbaum AJ (2012) Bone grafts, bone
substitutesand orthobiologics: the bridge between basic science and
clinicaladvancements in fracture healing. Organ 8:114–124
71. Sutherland A, Raafat A, Yates P, Hutchison J (1997)
Infectionassociated with the use of allograft bone from the north
eastScotland bone Bank. J Hosp Infect 35:215–222
72. Liu J, Chao L, Su L, Wang J, Wang C (2002) Experience with
abone bank operation and allograft bone infection in recipients at
amedical centre in southern Taiwan. J Hosp Infect 50:293–297
73. Wozney JM, Rosen V, Celeste AJ,Mitsock LM,WhittersMJ,
KrizRW, Hewick RM, Wang EA (1988) Novel regulators of
boneformation: molecular clones and activities. Science
242:1528–1535
74. Urist MR (1965) Bone: formation by autoinduction. Science
150:893–899
75. Garrison KR, Shemilt I, Donell S, Ryder JJ, MugfordM, Harvey
I,Song F, Alt V (2010) Bone morphogenetic protein (BMP) forfracture
healing in adults. Cochrane Database Syst Rev 16:CD006950.
https://doi.org/10.1002/14651858.CD006950.pub2
76. Miska M, Findeisen S, Tanner M, Biglari B, Studier-Fischer
S,Grützner P, Schmidmaier G, Moghaddam A (2016) Treatment
ofnonunions in fractures of the humeral shaft according to the
dia-mond concept. Bone Joint J 98:81–87
77. Singh R, Bleibleh S, Kanakaris NK, Giannoudis PV (2016)
Upperlimb non-unions treated with BMP-7: efficacy and clinical
results.Injury 47:S33–S39
78. Pneumaticos SG, Panteli M, Triantafyllopoulos GK,
PapakostidisC, Giannoudis PV (2014) Management and outcome of
diaphy-seal aseptic non-unions of the lower limb: a systematic
review.The surgeon 12:166–175
79. Alt V, Meyer C, Litzlbauer HD, Schnettler R (2007) Treatment
ofa double nonunion of the femur by rhBMP-2. J Orthop Trauma
21:734–737
80. Schell H, Duda G, Peters A, Tsitsilonis S, Johnson K,
Schmidt-Bleek K (2017) The haematoma and its role in bone healing.
JExperiment Orthopaed 4:5
81. Seebach C, Henrich D, Tewksbury R, Wilhelm K, Marzi I
(2007)Number and proliferative capacity of human mesenchymal
stemcells are modulated positively in multiple trauma patients
andnegatively in atrophic nonunions. Calcif Tissue Int
80:294–300
82. MathieuM, Rigutto S, Ingels A, Spruyt D, Stricwant N,
KharroubiI, Albarani V, Jayankura M, Rasschaert J, Bastianelli E
(2013)Decreased pool of mesenchymal stem cells is associated with
al-tered chemokines serum levels in atrophic nonunion
fractures.Bone 53:391–398
83. Goujon E (1869) Recherches expérimentales sur les propriétés
dutissu osseux. JL Anat 6:399–412
84. Friedenstein AJ, Petrakova KV, Kurolesova AI, Frolova
GP(1968) HETEROTOPIC transplants of bone marrow.Transplantation
6:230–247
85. Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas
R,Mosca JD, Moorman MA, Simonetti DW, Craig S, Marshak DR(1999)
Multilineage potential of adult human mesenchymal stemcells.
Science 284:143–147
86. Paley D, Young MC, Wiley AM, Fornasier VL, Jackson RW(1986)
Percutaneous bone marrow grafting of fractures and bonydefects an
experimental study in rabbits. Clin Orthop Relat Res208:300
87. Connolly JF, Guse R, Tiedeman J, Dehne R (1991)
Autologousmarrow injection as a substitute for operative grafting
of tibialnonunions. Clin Orthop Relat Res 266:259–270
88. Bruder SP, Kurth AA, Shea M, Hayes WC, Jaiswal N, Kadiyala
S(1998) Bone regeneration by implantation of purified,
culture-expanded human mesenchymal stem cells. J Orthop Res
16:155–162
89. Homma Y, Zimmermann G, Hernigou P (2013) Cellular
therapiesfor the treatment of non-union: the past, present and
future. Injury44:S46–S49
International Orthopaedics (SICOT)
https://doi.org/10.1515/bmt-2014-0100https://doi.org/10.1515/bmt-2014-0100https://doi.org/10.1007/s00264-016-3317-xhttps://doi.org/10.1302/0301-620X.98B4.34870https://doi.org/10.1302/0301-620X.98B4.34870https://doi.org/10.1016/j.injury.2007.02.012https://doi.org/10.1016/j.injury.2007.02.012https://doi.org/10.1016/j.injury.2005.10.008https://doi.org/10.1002/14651858.CD006950.pub2
-
90. Bajada S, Harrison P, Ashton B, Cassar-Pullicino V,
AshammakhiN, Richardson J (2007) Successful treatment of refractory
tibialnonunion using calcium sulphate and bone marrow stromal
cellimplantation. Bone Joint J 89:1382–1386
91. Hernigou P, Poignard A, Beaujean F, Rouard H
(2005)Percutaneous autologous bone-marrow grafting for
nonunions.Influence of the number and concentration of progenitor
cells. JBone Joint Surg Am vol 87:1430–1437.
https://doi.org/10.2106/JBJS.D.02215
92. Quarto R, Mastrogiacomo M, Cancedda R, Kutepov SM,Mukhachev
V, Lavroukov A, Kon E, Marcacci M (2001) Repairof large bone
defects with the use of autologous bone marrowstromal cells. N Engl
J Med 344:385–386
93. Wittig O, Romano E, Gonzalez C, Diaz-Solano D, Marquez
ME,Tovar P, Aoun R, Cardier JE (2016) A method of treatment
fornonunion after fractures using mesenchymal stromal cells
loadedon collagen microspheres and incorporated into platelet-rich
plas-ma clots. Int Orthop 40:1033–1038.
https://doi.org/10.1007/s00264-016-3130-6
94. Kazmers NH, Fragomen AT, Rozbruch SR (2016) Prevention ofpin
site infection in external fixation: a review of the
literature.Strategies Trauma Limb Reconstr 11:75–85
95. Kadhim M, Holmes L Jr, Gesheff MG, Conway JD (2017)Treatment
options for nonunion with segmental bone defects: sys-tematic
review and quantitative evidence synthesis. J OrthopTrauma
31:111–119. h t tps : / /do i .o rg /10
.1097/BOT.0000000000000700
96. Harshwal RK, Sankhala SS, Jalan D (2014) Management of
non-union of lower-extremity long bones using mono-lateral
externalfixator–report of 37 cases. Injury 45:560–567
97. Brinker MR, O'Connor DP (2003) Ilizarov compression over
anail for aseptic femoral nonunions that have failed
exchangenailing: a report of five cases. J Orthop Trauma
17:668–676
98. El-Rosasy MA (2012) Nonunited humerus shaft fractures
treatedby external fixator augmented by intramedullary rod. Indian
JOrthopaed 46:58
99. Ilizarov G, Lediaev V (1969) Replacement of defects of
longtubular bones by means of one of their fragments.
Vestnikkhirurgii imeni II Grekova 102:77
100. Ilizarov GA (1989) The tension-stress effect on the genesis
andgrowth of tissues: part II. The influence of the rate and
frequencyof distraction. Clin Orthopaed Relat Res 239:263–285
101. Green SA (1994) Skeletal defects a comparison of bone
graftingand bone transport for segmental skeletal defects. Clin
OrthopRelat Res 301:111–117
102. Oh CW, Apivatthakakul T, Oh JK, Kim JW, Lee HJ, Kyung
HS,Baek SG, Jung GH (2013) Bone transport with an external
fixatorand a locking plate for segmental tibial defects. The bone
& joint
journal 95-B:1667–1672.
https://doi.org/10.1302/0301-620X.95B12.31507
103. Kadhim M, Holmes L Jr, Gesheff MG, Conway JD
(2017)Treatment options for nonunion with segmental bone defects:
sys-tematic review and quantitative evidence synthesis. J
OrthopTrauma 31:111–119
104. Ueng SW, Chao E-K, Lee S-S, Shih C-H (1997)
Augmentativeplate fixation for the management of femoral nonunion
afterintramedullary nailing. J Trauma Acute Care Surg
43:640–644
105. Wang Z, Liu C, Liu C, Zhou Q, Liu J (2014) Effectiveness
ofexchange nailing and augmentation plating for femoral shaft
non-union after nailing. Int Orthop 38:2343–2347
106. Park J, Kim SG, Yoon HK, Yang KH (2010) The treatment
ofnonisthmal femoral shaft nonunions with im nail exchange
versusaugmentation plating. J Orthop Trauma 24:89–94
107. Birjandinejad A, Ebrahimzadeh MH, Ahmadzadeh-Chabock
H(2009) Augmentation plate fixation for the treatment of femoraland
tibial nonunion after intramedullary nailing. Orthopedics 32:409.
https://doi.org/10.3928/01477447-20090511-12
108. Ateschrang A, Albrecht D, Stockle U,Weise K, Stuby F,
Zieker D(2013) High success rate for augmentation compression
platingleaving the nail in situ for aseptic diaphyseal tibial
nonunions. JOrthop Trauma 27:145–149.
https://doi.org/10.1097/BOT.0b013e31825d01b2
109. Gessmann J, Königshausen M, Coulibaly MO, Schildhauer
TA,Seybold D (2016) Anterior augmentation plating of aseptic
hu-meral shaft nonunions after intramedullary nailing. Arch
OrthopTrauma Surg 136:631–638
110. Hierholzer C, Sama D, Toro JB, Peterson M, Helfet DL
(2006)Plate fixation of ununited humeral shaft fractures: effect of
type ofbone graft on healing. J Bone Joint Surg Am
88:1442–1447.https://doi.org/10.2106/JBJS.E.00332
111. Huang K-C, Tong K-M, Lin Y-M, Loh E-W, Hsu C-E
(2012)Evaluation of methods and timing in nail dynamisation for
treatingdelayed healing femoral shaft fractures. Injury
43:1747–1752
112. Lin CJ, Chiang CC, Wu PK, Chen CF, Huang CK, Su AW, ChenWM,
Liu CL, Chen TH (2012) Effectiveness of plate augmenta-tion for
femoral shaft nonunion after nailing. J Chin MedAssociation
75:396–401. https://doi.org/10.1016/j.jcma.2012.06.008
113. Choi Y, Kim K (2005) Plate augmentation leaving the nail in
situand bone grafting for non-union of femoral shaft fractures.
IntOrthop 29:287–290
114. Feldman DS, Shin SS, Madan S, Koval KJ (2003) Correction
oftibial malunion and nonunion with six-axis analysis
deformitycorrection using the Taylor spatial frame. J Orthop Trauma
17:549–554
International Orthopaedics (SICOT)
https://doi.org/10.2106/JBJS.D.02215https://doi.org/10.2106/JBJS.D.02215https://doi.org/10.1007/s00264-016-3130-6https://doi.org/10.1007/s00264-016-3130-6https://doi.org/10.1097/BOT.0000000000000700https://doi.org/10.1097/BOT.0000000000000700https://doi.org/10.1302/0301-620X.95B12.31507https://doi.org/10.1302/0301-620X.95B12.31507https://doi.org/10.3928/01477447-20090511-12https://doi.org/10.1097/BOT.0b013e31825d01b2https://doi.org/10.1097/BOT.0b013e31825d01b2https://doi.org/10.2106/JBJS.E.00332https://doi.org/10.1016/j.jcma.2012.06.008https://doi.org/10.1016/j.jcma.2012.06.008
-
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具
http://www.xuebalib.com/cloud/http://www.xuebalib.com/http://www.xuebalib.com/cloud/http://www.xuebalib.com/http://www.xuebalib.com/vip.htmlhttp://www.xuebalib.com/db.phphttp://www.xuebalib.com/zixun/2014-08-15/44.htmlhttp://www.xuebalib.com/
Diaphyseal long bone nonunions — types, aetiology, economics,
and treatment recommendationsAbstractIntroductionEpidemiology and
socioeconomic costAetiology, classification and risk
factorsAetiology and risk factorsRisk factors
Treatment optionsNail dynamizationExchange nailingBone grafts
and bone morphogenetic proteinsCell therapyExternal fixation
techniques for nonunionsAugmentation plating
Conclusions and treatment recommendationsReferences
学霸图书馆link:学霸图书馆