Embed Size (px)
Citation preview

Clinical Imaging xxx (2013) xxx–xxx
Contents lists available at ScienceDirect
Clinical Imaging
j ourna l homepage: ht tp : / /www.c l in ica l imag ing.org
Diagnostic significance of periesophageal fat pad in ultrasonography for sliding hiatalhernias: sonographic fat pad sign
Emin Cakmakci a,⁎, Mehmet Tahtabasi a, Irfan Celebi a, Selma Cakmakci b, Aysel Bayram a, Safiye Tokgoz a,Mucahit Dogru a, Muzaffer Basak a
a Department of Radiology, Sisli Etfal Training and Research Hospital, Istanbul, Turkeyb Department of Pediatrics, Kaçkar Government Hospital, Rize, Turkey
a b s t r a c ta r t i c l e i n f o
⁎ Corresponding author. Department of Radiology, SisHospital, Etfal Sokak, 34360, Sisli, Istanbul, Turkey. Tel.:2123735014.
E-mail address: [email protected] (E. Cakmakc
0899-7071/$ – see front matter © 2013 Elsevier Inc. Alhttp://dx.doi.org/10.1016/j.clinimag.2013.09.009
Please cite this article as: Cakmakci E, et alsonographic fat pad sign, Clin Imaging (20
Article history:Received 13 April 2013Received in revised form 17 August 2013Accepted 26 September 2013Available online xxxx
Keywords:Sliding hiatal herniaDiagnosisUltrasonographyComputerized tomographyPeriesophageal fat pad
The aim of the present study was to investigate the diagnostic significance of visualization ofperiesophageal fat pad in ultrasonography or computed tomography for sliding hiatal hernias. Forty-sixcontrols and 21 esophageal hiatal hernia patients were compared in terms of sonographic and tomographicesophageal diameters. We suggest that absence of periesophageal fat pad sign in ultrasonography orcomputerized tomography is a noteworthy finding that calls for further investigation for the diagnosis ofsliding hiatal hernias.
© 2013 Elsevier Inc. All rights reserved.
1. Introduction
Hiatal hernia (HH) occurs due to the proximal displacement ofgastroesophageal junction and the stomach into the mediastinumthrough the esophageal hiatus. During the normal swallowingprocess, gastroesophageal junction and a small portion of the stomachis proximally displaced through the esophageal hiatus. However, HHmay exist if the phrenoesophageal ligament becomes loose due toaging or repetitive stress of swallowing. Clinically, HH is closelyassociated with reflux symptoms, esophagitis, Barrett's esophagus,and esophageal adenocarcinoma. Sliding HH (SHH) must also beconsidered in the differential diagnosis of cardiac and pulmonaryvascular diseases [1].
Diagnostic measures for SHH are barium swallow radiography,endoscopy, manometry, and computed tomography (CT). Endoscopyis a relatively invasive procedure, while barium contrast examinationand CT brings about the risk of radiation exposure. Transabdominalultrasonography (US) is actually a practical and safe method, but itsrole in the evaluation of gastroesophageal reflux and SHH is limited[2–4]. The pathophysiology of HHs is incompletely understood andvaries tremendously by the type of hernia (sliding and paraesopha-geal), size, age that it occurs, and others. US is able to define theabdominal esophagus in vivo, both in terms of its anatomy and as a
li Etfal Training and Research+90-5059436888; fax: +90-
i).
l rights reserved.
, Diagnostic significance of p13), http://dx.doi.org/10.101
functional structure. Accurate assessment of the sonographic canalrequires careful measurement under strictly defined clinical condi-tions. Using such criteria, ultrasound has a better sensitivity thanbarium studies in detecting small herniations [3,4].
The upper margin of the phrenic ampulla borders the tubularesophagus forming a muscular structure called “A” ring. This ringanatomically corresponds to the upper margin of the lower esophagealsphincter. The lower margin of the phrenic ampulla is bounded by thediaphragmatic indentation. Within the phrenic ampulla, anothermucosal ring (“B” ring) that corresponds to the squamocolumnarjunction or the union of the esophagus with the stomach can beidentified. In case theB ring is prominent (luminal diameter b13 mm), itis termed as Schatzki's ring [4,5]. Radiographically, HH is described as theseparation of B ring and the diaphragmatic indentation of N2 cm [1,4,5].
In this study, we discuss the diagnostic importance of visualizationof periesophageal fat pad under CT or US for HH. Apart from thewidening of esophageal diameter, we speculate that failure ofobservation of periesophageal fat pad in US or CT may aid in thediagnosis of HH.
2. Materials and methods
This retrospective study had been performed in the radiologydepartment of a tertiary care center between May 2011 and May2012. Axial and sagittal CT images together with ultrasonographicviews had been obtained from 46 controls and 21 esophageal HHpatients. Patients below 18 or over 65 years and pregnant patientswere excluded from the study.Written informed consent allowing the
eriesophageal fat pad in ultrasonography for sliding hiatal hernias:6/j.clinimag.2013.09.009

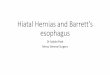
Fig. 1.Demonstration of periesophageal fat pad sign in (a) axial US view and (b) sagittalUS view in the same patient.
Fig. 2. (a) Axial contrast-enhanced CT scan demonstrating sonographic fat pad sign(hypodense area surrounded by blue arrows) and esophagus (blue star); (b) axialcontrast-enhanced CT scan demonstrating sonographic fat pad sign (hypodense areasurrounded by straight blue arrow) and esophagus with air images (oblique arrow).
2 E. Cakmakci et al. / Clinical Imaging xxx (2013) xxx–xxx
use of radiologic views for scientific purpose has been routinelyobtained previously from all patients examined in the radiologydepartment of our hospital. Control group consisted of patients whohad previously undergone CT examination and operated for varioustumours (breast Ca, Colon Ca, gastric Ca, etc.), and US was required forcertain periods. These patients have not undergone CT and/or USexaminations for this study.
Computerized tomography sections were visualized using ASiemens Somatom Definition (128 detector) device (Siemens Turkey,Istanbul, Turkey) (Fig. 1a,b). Computerized tomography was used inthe diagnosis of HH [6]. All of the comparative evaluations ofradiological images have been made by the same gastrointestinalsystem radiologist. CT images included in the study were obtained via(oral or intravenous) contrast-enhanced radiological examinationsAccordingly, since adequate doses of oral neutral or positive contrastmaterial were used and oral preparation of the patients wassatisfactorily performed, Z-line on gastroesophageal junction-borderzone on the junction between esophageal and gastricmucosa could beevaluated clearly. Three-dimensional reconstruction techniques fur-ther improve the quality of images.
Ultrasonographic assessment had been performed after a 6-hstarvation period with a Toshiba Applio XV device (Toshiba MedicalSystems®, Japan). Abdominal probe had been placed on the inferiorboundary of xiphoid process and directed cranially to havemidsagittal and midaxial views. The examination was performed bytracking linear echogenicity of diaphragm on midsaggital and
Please cite this article as: Cakmakci E, et al, Diagnostic significance of psonographic fat pad sign, Clin Imaging (2013), http://dx.doi.org/10.101
midaxial planes and orienting the probe cranially at an angle of30–60° (an average of 45°; angle of orientation may vary based onthe degree of abdominal obesity of the patient). On sagittal planewhere we saw longitudinal axis of aorta, immediately anterior to theaorta and on axial plane anterior or paramedian to the aorta, weobserved distal esophagus with intraluminal air echogenicities and ahypoechogenic wall, which continues with proximal part of thestomach. In patients with marked abdominal obesity or intensegaseous distension in the field of examination in whom we cannotvisualize esophageal hiatus, 1–2 min after one sip of water intake, wecan demonstrate this region during swallowing maneuver. Measure-ments were performed at the level of esophageal hiatus using the leftlobe of liver as the acoustic window. Esophageal diameter wasmeasured from the anterior to the posterior wall, while existence ofperiesophageal fat pad at the hiatal level was assessed during theradiological evaluation (Figs. 2a,b). In the sliding hernia group, USdemonstrated completely obliterated periesophageal echogeniccircular plane (sonographic fat pad sign) at the level of esophagealhiatus, and only echogenic air images secondary to gastric contentsare observed.
Both groups were compared in terms of age, gender, body massindex as well as sonographic and tomographic esophageal diameters.Existence of fat pad at the level of esophageal hiatal level was notedduring the radiological evaluation (Fig. 3a,b,c).
Approval of institutional review board was obtained for thepresent study.
eriesophageal fat pad in ultrasonography for sliding hiatal hernias:6/j.clinimag.2013.09.009

Table 1Comparison of demographic, clinical, and radiological data of our series consisting ofive healthy cases with widened esophageal diameter (N2 cm)
Control group(n = 46)
HH group(n = 21)
Age 41.9 (18–75) 58.6 (34–88)
3E. Cakmakci et al. / Clinical Imaging xxx (2013) xxx–xxx
3. Results
The average ages for control group (20 females, 26 males) andhernia patients (10 females, 11 males) were 41.9 and 58.6,respectively. Body mass index in the control group was 19.75,whereas it was 28.5 in patients. Esophageal diameters measured via
Gender (female, male) 20, 26 10, 11Esophageal diameter (mm) at US 13.2 (6.6–35.3) 31.6 (22.5–46.5)Esophageal diameter (mm) at CT 13.1 (6.4–34.6) 31.6 (22.5–47.9)Body mass index 19.8 (18–23) 28.5 (24–36)
Fig. 3. (a) Axial section view obtained after swallowing. From inside out: echogenic airimages (the innermost region), mucosa (black ring), submucosa (gray area), muscularlayer (yellow ring), hyperechogenic completely circular fatty layer-sonographic fat padsign (green ring), diaphragmatic border of the esophageal hiatus (the outermost ring)(b) Sagittal section view obtained before swallowing or taking a sip of water: double-layered mucosa (black area: the innermost double layer), submucosa (gray area)muscular layer (yellow area); hyperechogenic complete circular fatty plane-sono-graphic fat pad sign (green ring), diaphragm (thick pink area), adventitial layer of theesophagus (dark red line); (c) Sagittal section view obtained 1–2 min after swallowingor taking a sip of water: echogenic air images (the innermost region), mucosa (blackring), submucosa (gray area), muscular layer (yellow ring), hyperechogenic completelycircular fatty layer-sonographic fat pad sign (green ring), and diaphragmatic border othe esophageal hiatus (the outermost ring).
Please cite this article as: Cakmakci E, et al, Diagnostic significance of periesophageal fat pad in ultrasonography for sliding hiatal hernias:sonographic fat pad sign, Clin Imaging (2013), http://dx.doi.org/10.1016/j.clinimag.2013.09.009
f
US and CT were 13.2 and 13.1 in the control group. In the other hand,esophageal diameters measured via US and CT were 31.6 and 31.5 inthe hernia group. In all healthy controls, periesophageal fat pad wasconsistently visualized under US or CT. In contrast, fat pad could notbe detected in patients complaining of HH. Demographic andradiological data are comparatively presented in Table 1.
4. Discussion
The diagnosis of HH can be made through radiographic, endo-scopic, and manometric assessment. Whereas large HHs can bedetected and diagnosed without difficulty using either of thesemethods, diagnosing small HHs (b2 cm) can be challenging with eachmodality having its limitations. While performing barium contraststudies of the upper gastrointestinal tract, a globular structure termed“phrenic ampulla” is seen above the diaphragm during swallows. Thisstructure has traditionally been considered to be a physiologic finding,but the study using simultaneous fluoroscopy and manometrydemonstrated that it corresponded to a small reducing HH [1–3].
In patients with a normal hiatal diameter, either a fat echogenicityin US or a fat density in CT scan was observed. However, in somepatients devoid of sliding hernia, hiatal diameter was found to beradiologically increased. These patients may be candidates foroccurrence of sliding hernia in the future. Increased hiatal diameterin some normal cases may be due to having meal just prior toradiological evaluation. Anyway, this finding reminds that thediagnostic reliability of increased esophageal diameter may bedoubtful for some SHH cases [7]. We suggest that fat pad sign mayhelp in confirmation of diagnosis especially in such patients.
In our series, cases without SHH displayed increased hiataldiameter in radiological images. We observed that there was a fatechogenicity (in ultrasonography) or fat density (in CT scans) inperioesophageal region at the level of esophageal hiatus. Wespeculate that the presence of fat pad in the perioesophageal areamay indicate the absence of SHH. Even though we are aware of thefact that our data to support this hypothesis are limited due to thesample size, this coincidental finding can be a useful and practicaldiagnostic clue if its reliability is confirmed by further studies.
In case periesophageal fat pad echogenicity within the esophagealhiatus is obliterated, inner and outer surfaces of esophagus must becontrolled both in axial and sagittal planes by repositioning theultrasound probe. Obliteration of periesophageal fat plan may occurnot only in SHH. In inflammatory pathologies, a symmetrical
.
;
f

4 E. Cakmakci et al. / Clinical Imaging xxx (2013) xxx–xxx
thickening of distal esophagus and gastroduodenal junction—that ismost obvious in the gastroduodenal segment—can be observed. Barretesophagus or mass lesions exist as asymmetrical thickening ofesophageal wall. Therefore, periesophageal fat pad will be obliteratedasymmetrically in axial USG views.
Since gastroesophageal junction is cranially elevated in SHH, distalesophagus disappears before entering the esophageal hiatus. Rugae orluminal air images consistent with stomach at the level of hiatus andcomplete obliteration of fat pad are seen in case of SHH. Inparaesophageal hernias, position of gastroesophageal junction willbe preserved, and gastric rugae extending superiorly from the hiatusor luminal air bubbles will be ready. In mixed hernias, US willdemonstrate the linear echogenicity of mucosal or submucosal layersending before entering the hiatus on one side with gastric luminal airbubbles [8–10].
In circumstances where diagnostic dilemma persists despite theseclues, repetitive axial and sagittal ultrasonographic examinationshould be performed after oral hydration of patients with at least500 ml of fluids. Subsequent to oral intake, luminal air and fluidechogenicities and symmetrical wall thickening of inflammatoryorigin will be observed. In contrast, benign or malignant mass lesionsor Barrett esophagus will appear as asymmetrical wall thickening orpolypoid lesions extending towards the lumen.
We speculate that detection of periesophageal fat pad is moreimportant than esophageal diameter in the diagnosis of SHH.Diameter can be affected by age, obesity, and body mass index.However, periesophageal fat pad seems not to be influenced bythese factors.
We observed that some controls had wide esophageal hiataldiameters despite the fact that they displayed no symptoms. We termthe hyperechogenic completely circular fat plane observed around theperiesophageal level in all healthy controls in our series as “fat padsign.” This sign is evident in both axial and sagittal views of real-timeUS. In SHH, this fat pad disappears completely, and acoustic shadowsensourcing from reverbation artefacts exist due to echogenous airimages. Asymmetrical disappearance of fat pad sign and peripheraldisplacement of esophageal luminal air occur in intraesophageal
Please cite this article as: Cakmakci E, et al, Diagnostic significance of psonographic fat pad sign, Clin Imaging (2013), http://dx.doi.org/10.101
malignancies. Therefore, we think that axial and sagittal US view notonly aids in diagnosis of SHH but also may provide clues for otheresophageal and paraesophageal pathologies.
The present study has two main limitations. First, this studyincludes the relatively small sample size. Secondly, neither controlsnor patients have had barium swallow to study absence/presence ofHH and type, size, and others.
In conclusion, absence of periesophageal fat pad sign in US orcomputerized tomography can be a valuable marker in the diagnosisof SHHs. We suggest that obliteration of periesophageal fat is anoteworthy finding that calls for further investigation for thediagnosis of SHH. Further clinical trials are essential to understandits actual diagnostic potential.
References
[1] Hyun JJ, Bak YT. Clinical significance of hiatal hernia. Gut Liver 2011;5:267–77.[2] Cakmakci E, Celebi I, Tahtabasi M, Tabakci ON, Ozkurt H, Basak M, Karpat Z.
Accuracy of ultrasonography in the diagnosis of sliding hiatal hernias. Acad Radiol2013;20:453–6.
[3] Kahrilas PJ, Kim HC, Pandolfino JE. Approaches to the diagnosis and grading ofhiatal hernia. Best Pract Res Clin Gastroenterol 2008;22:601.
[4] Barone M, Di Lernia P, Carbonara M, Ladisa R, Donno A, Amoruso A, Di Leo A,Francavilla A. Sliding gastric hiatal hernia diagnosis by transabdominal ultraso-nography: an easy, reliable and non-invasive procedure. Scand J Gastroenterol2006;41:851.
[5] Changchien CS, Hsu CC. Use of sonography in the evaluation of the gastroesoph-ageal junction. J Clin Ultrasound 1996;24:67–72.
[6] Noth I, Zangan SM, Soares RV, Forsythe A, Demchuk C, Takahashi SM, Patel SB,Strek ME, Krishnan JA, Patti MG, Macmahon H. Prevalence of hiatal hernia byblinded multidetector CT in patients with idiopathic pulmonary fibrosis. EurRespir J 2012;39:344–51.
[7] Eren S, Ciris F. Diaphragmatic hernia: diagnostic approaches with review of theliterature. Eur J Radiol 2005;54:448.
[8] Aliotta A, Rapaccini GL, Pompili M, Grattagliano A, Cedrone A, Trombino C, De LucaF, De Vitis I. Ultrasonographic signs of sliding gastric hiatal hernia and theirprospective evaluation. J Ultrasound Med 1995;14:457–61.
[9] Zhu SY, Liu RC, Chen LH, Luo F, Yang H, Feng X, Liao XH. Sonographicdemonstration of the normal thoracic esophagus. J Clin Ultrasound 2005;33:29–33.
[10] Esposito F, Lombardi R, Grasso AC, Dolezalova H, Sodano A, Tarantino L, Giorgio A.Transabdominal sonography of the normal gastroesophageal junction in children.J Clin Ultrasound 2001;29:326–31.
eriesophageal fat pad in ultrasonography for sliding hiatal hernias:6/j.clinimag.2013.09.009