Embed Size (px)
Citation preview
Diagnostic dilemmas in helminthology:what tools to use and when?Robert Bergquist1, Maria Vang Johansen2 and Jurg Utzinger3
1 Ingerod, 454 94 Brastad, Sweden2 DBL Centre for Health Research and Development, Faculty of Life Sciences, University of Copenhagen, Copenhagen,
Thorvaldsensvej 57, DK-1871 Frederiksberg C, Denmark3 Department of Public Health and Epidemiology, Swiss Tropical Institute, P.O. Box CH-4002 Basel, Switzerland
Opinion
Glossary
Accuracy: the percentage of correct results obtained by a test under evaluation
compared with the results of a reference or ‘gold standard’ test.
Community effectiveness: the ability of a particular intervention to alter the
natural history of a particular disease for the better, under actual conditions of
practice and use.
Cost-effectiveness: economic evaluation to assess what kind of results are
produced for the amount of money spent.
Efficacy: the ability of an intervention to produce the desired beneficial effect
under ideal circumstances (assessed by randomized controlled trials).
Elimination: reduction to zero of the incidence of a specific disease or infection
caused by a specific agent in a defined geographical area as a result of
deliberate efforts.
Eradication: permanent reduction to zero of the worldwide incidence of
infection caused by a specific agent as a result of deliberate efforts.
Precision: the degree to which repeated measurements or calculations show
the same or similar results.
Positive predictive value: the probability that a positive result accurately
indicates the presence of infection.
Sensitivity: the proportion of actual positives which are correctly identified as
such (i.e. the percentage of sick people who are identified as having the
condition).
Specificity: the proportion of negatives which are correctly identified (i.e. the
Available data regarding the distribution, prevalenceand severity of various diseases are based on the per-formance and operational characteristics of the diagnos-tic techniques applied; this is a fact that is particularlyapparent in the study of helminth infections. An import-ant lesson learnt from the efforts to rein in dracunculia-sis, lymphatic filariasis and schistosomiasis is that thediagnostic approach needs to be changed as furtherprogress is made towards control and ultimate elimin-ation of the disease. This insight prompted the opinionpiece presented here, which highlights diagnostic dilem-mas in helminthology related to the stage of controlachieved and sets out some research needs.
Choice of diagnostic assaysNew and ambitious goals have been set for the control ofinfectious diseases in the developingworld by governmentsand international donor agencies in collaboration with theWorld Health Organization (WHO). Considerable progresshas been made, but there is a tendency to emphasize drugtreatment and vaccines, so the importance of quality-assured diagnostic tests is often neglected [1]. However,the more successful a control programme becomes, themore crucial the need for an accurate assessment of theepidemiological situation becomes.
The helminthic diseases require diverse diagnosticapproaches. For example, although serology constitutesa valuable adjunct to the clinical diagnosis of echinococco-sis, trichinellosis and toxocariasis [2], the progressing localelimination (see Glossary) of various helminth infectionssuch as dracunculiasis [3], lymphatic filariasis [4,5] andschistosomiasis [4,6,7] highlights the need for adjustingthe diagnostic capability to the different stages of activecontrol.
The focus of this opinion article is on schistosomiasisand the main soil-transmitted helminthiases (ascariasis,hookworm disease and trichuriasis) because these diseasesare still widespread [8–10], although activities to controlthem have gained momentum owing to the World HealthAssembly resolution WHA54.19 of May 2001, which urgesmember states to treat at least 75% of school-aged childrenand other high-risk groups regularly with praziquantelagainst schistosomiasis and albendazole or mebendazoleagainst soil-transmitted helminthiases [11]. The food-borne trematodiases (e.g. clonorchiasis, fascioliasis,
Corresponding author: Bergquist, R. ([email protected]).
1471-4922/$ – see front matter � 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.pt.2009.01
opisthorchiasis and paragonimiasis) are also discussedbecause this group comprises serious yet truly neglectedtropical diseases, which, in addition to their veterinarysignificance, constitute an emerging public health threat inmany parts of the world [12–16].
The choice of a diagnostic assay should be governed bythe objective of the activity. Indeed, the proper diagnosis ofan infection is paramount for all aspects of its preventionand control. Moreover, the evaluation of efficacy and com-munity effectiveness of interventions, verification of localdisease elimination and early detection of resurgencedepend strongly on the accuracy of diagnostic tools[17,18]. However, although the implementation of a com-plex diagnostic approach based on the highest possiblecombination of sensitivity and specificity can be defendedfrom a research point of view, even when it is time-con-suming and expensive, an approach that is useful in prac-tice is almost always a compromise between quality andquantity because the techniques needed for large-scaleapplication must be based on cost-effectiveness (i.e. timeand resources required per test), precision, simplicity androbustness. The dilemma represented by this need forcompromise is related to the nature of the infection andthe stage of control achieved.
The heart of the matter is the required continuousadaption of the diagnostic focus to the stage of control,
percentage of well people who are identified as not having the condition).
.004 Available online 9 March 2009 151

Figure 1. Schematic picture illuminating how falling endemicity levels influence control focus and diagnostic needs.
Opinion Trends in Parasitology Vol.25 No.4
taking into account the prevailing constraints in terms ofavailable resources. Figure 1 highlights this by showingthe various stages of a hypothetical helminth-control pro-gramme juxtaposed with the type of diagnostic tools thatmust be employed to reach the set goals.
From morbidity to post-transmissionIn 2002, Engels and colleagues [19] outlined the control ofschistosomiasis as a series of consecutive steps movingfrom morbidity control to elimination of infection as apublic health threat. This framework has been expandedto include the soil-transmitted helminthiases and the food-borne trematodiases. Underlying reasons for this are theconsiderable geographical overlap of these infections, thesimilar tools used for diagnosis at the onset of controlactivities (e.g. microscopy of stool samples) and the similarpublic health measures applied (e.g. large-scale adminis-tration of anthelminthic drugswhenmorbidity reduction isthe prime objective) [20,21]. Post-transmission control isnot depicted in Figure 1 because this stage is limited to asmall number of patients, but it should be realized that itwill require interventions for a prolonged period of time,particularly in the case of schistosomiasis and the food-borne trematodiases [22]. The idea to collate this infor-mation (Figure 2) is in line with the growing emphasis onintegrating the control of the so-called neglected tropicaldiseases [4,10,23–25]. Currently used techniques aredepicted in the arrow boxes in Figure 2; however, someof the entries are still tentative.
Diagnostic dilemmasMorbidity control – questionnaires and standard
diagnostic tests
When control of schistosomiasis was first attempted, era-dication was the stated goal – at least for some eminentscientists at the time [26]. However, the failure of thisapproach was not because of a diagnostic dilemma butdepended on the incongruence between objective and tools.The problem was circumvented by the advent of prazi-quantel, which permitted a change of tactics (i.e. substitut-
152
ing morbidity for transmission as the focus of control inhighly endemic areas) [27]. This strategy, which relies onmass administration of safe and efficacious drugs donatedor provided at low cost [4,7,10], is still recommended insettings where the proportion of those infected surpasses agiven threshold (e.g. >50% of school-aged childreninfected) [11]. With this diagnostic scenario, cost and sim-plicity are more important than sensitivity; this led to theutilization of community-based questionnaires, with theresults followed up by standard parasitological examin-ations of excreta (e.g. stool, urine and sputum). That theseresults are not fully reliable with respect to prevalence andgive even less information on the level of transmissionmust be weighed against the importance of rapidly identi-fying those most in need of treatment.
Interviewing schoolchildren about blood in the urinehas proved generally accurate and cost-effective for therapid identification of high-risk communities of urinaryschistosomiasis [28]. Although a similar approach, focusedon dietary habits (e.g. consumption of raw or undercookedfish), could be a quick way to identify populations at risk ofclonorchiasis [29], geographical and ethnographical differ-ences present an unforeseen dilemma. For example,whereas communities suffering from opisthorchiasis inThailand were able to perform self-diagnosis leading totreatment-seeking practices, this was not the case in Laos,where opisthorchiasis-specific symptoms were vague [30],leading to the conclusion that the questionnaire approachmust be locally assessed before large-scale implementa-tion. Thus, parasitological diagnostic tools are still neededfor assessing cure after treatment and, in the longer term,dependable disease surveillance.
Faecal smears and Kato-Katz thick smears are widelyused direct methods for diagnosing intestinal schistoso-miasis, the common soil-transmitted helminthiases andmost food-borne trematode infections [31,32]. Although astrong bias towards false negatives would falsify the out-come, even a considerable proportion of false positiveswould not compromise the cost-effectiveness of thisapproach because the extra drug expense is marginal in
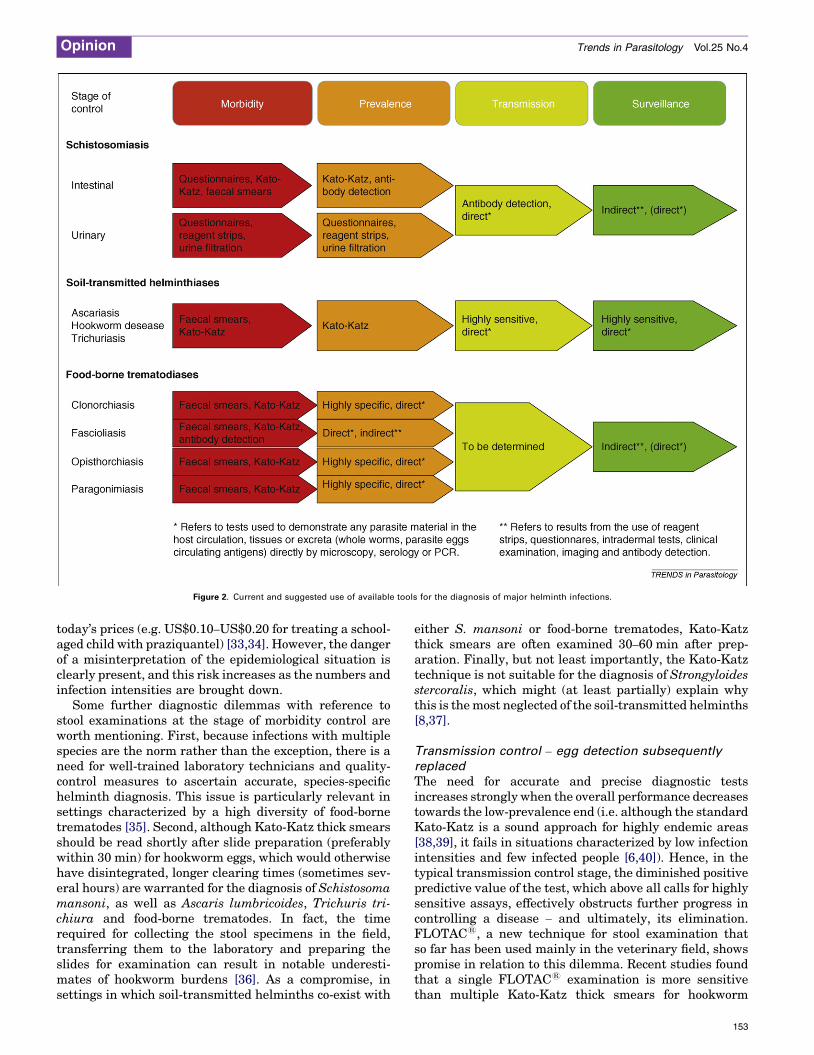
Figure 2. Current and suggested use of available tools for the diagnosis of major helminth infections.
Opinion Trends in Parasitology Vol.25 No.4
today’s prices (e.g. US$0.10–US$0.20 for treating a school-aged child with praziquantel) [33,34]. However, the dangerof a misinterpretation of the epidemiological situation isclearly present, and this risk increases as the numbers andinfection intensities are brought down.
Some further diagnostic dilemmas with reference tostool examinations at the stage of morbidity control areworth mentioning. First, because infections with multiplespecies are the norm rather than the exception, there is aneed for well-trained laboratory technicians and quality-control measures to ascertain accurate, species-specifichelminth diagnosis. This issue is particularly relevant insettings characterized by a high diversity of food-bornetrematodes [35]. Second, although Kato-Katz thick smearsshould be read shortly after slide preparation (preferablywithin 30 min) for hookworm eggs, which would otherwisehave disintegrated, longer clearing times (sometimes sev-eral hours) are warranted for the diagnosis of Schistosomamansoni, as well as Ascaris lumbricoides, Trichuris tri-chiura and food-borne trematodes. In fact, the timerequired for collecting the stool specimens in the field,transferring them to the laboratory and preparing theslides for examination can result in notable underesti-mates of hookworm burdens [36]. As a compromise, insettings in which soil-transmitted helminths co-exist with
either S. mansoni or food-borne trematodes, Kato-Katzthick smears are often examined 30–60 min after prep-aration. Finally, but not least importantly, the Kato-Katztechnique is not suitable for the diagnosis of Strongyloidesstercoralis, which might (at least partially) explain whythis is themost neglected of the soil-transmitted helminths[8,37].
Transmission control – egg detection subsequently
replaced
The need for accurate and precise diagnostic testsincreases strongly when the overall performance decreasestowards the low-prevalence end (i.e. although the standardKato-Katz is a sound approach for highly endemic areas[38,39], it fails in situations characterized by low infectionintensities and few infected people [6,40]). Hence, in thetypical transmission control stage, the diminished positivepredictive value of the test, which above all calls for highlysensitive assays, effectively obstructs further progress incontrolling a disease – and ultimately, its elimination.FLOTAC1, a new technique for stool examination thatso far has been used mainly in the veterinary field, showspromise in relation to this dilemma. Recent studies foundthat a single FLOTAC1 examination is more sensitivethan multiple Kato-Katz thick smears for hookworm
153

Table 1. Characteristics in the diagnostic process at different stages of helminth-control programmesa
Characteristics Stage of helminth-control programme
Morbidity Prevalence Transmission Surveillance Elimination
Target � Human host � Human host � Human host � Human host � Human host
� Reservoir host � Reservoir host � Reservoir host
� Intermediate host � Intermediate host � Intermediate host
Diagnostic traits � Simplicity � Sensitivity � High sensitivity � High sensitivity � High sensitivity
� Low cost � Specificity � Specificity � Specificity � High specificity
Suggested approach � Questionnaire � Sensitive direct tests � Antigen detection � Antibody detection � PCR
� Microscopy � Labelled antibodyb � Antibody detection
Strengths and
limitations
� Good indicator of
general status
� Development of test
system not completed
� Antigen detection not
sufficiently sensitive
� Excellent sensitivity � Capable assays
� Neglects light
infections
� Intermediate host testing
complicated
� Crossreactions and
specificity problems
� Certified testing
� Specific titres diminish
only slowly
� System not yet
availableaUsing schistosomiasis as an example.bApplied to the intermediate host.
Opinion Trends in Parasitology Vol.25 No.4
diagnosis [41], as well as A. lumbricoides and T. trichiuradiagnosis [42]. In addition, multiple stool (or urine orsputum) examinations and the use of different methodssimultaneously should be considered [37,43–45].
Thus, once morbidity is under control, further progressdemands more sensitive techniques, and when the trans-mission and surveillance control stages have beenreached, cost might increase because control at theselevels must consider different kinds of host (e.g. schisto-somiasis; see Table 1) and requires even more sensitiveapproaches. At this stage, antibody detection is clearly thepreferential, primary approach for monitoring the humanpopulation [39]. Of note, in the Chinese national schisto-somiasis control programme, serology is routinely imple-mented, usually followed by stool examination ofseropositive individuals [6]. However, there are manychallenges to this course of action. First, antibody detec-tion is not quantitative. Second, it fails to distinguishbetween current and cured infections, although progresshas been made in remedying this issue [39]. Third, thehigh degree of crossreactivity with clonorchiasis and para-gonimiasis is a problem of particular importance in Chinaand the countries south of its border, where these food-borne trematode infections are highly endemic [12,13,15].In areas where antibody detection is challenged by a highlevel of crossreactivity, molecular tools should be contem-plated in spite of their higher cost and the requirement forspeciality laboratories. For example, in Brazil, PCRapplied to human faeces found a prevalence of 38.1% ina study of 194 individuals from an S.-mansoni-endemicarea, whereas triplicate Kato-Katz thick smears achievedonly 30.9% prevalence in the same samples [46]. PCRapproaches have also been successfully developed forseveral other helminths, including food-borne trematodes[47]. Fourth, integration of this type of serology intonational control programmes requires access to afford-able, high-quality reagents or kits, as well as successfulmethodological standardization and definition of assayperformance. These points might explain why only afew countries have adopted antibody detection as a keystrategy in helminth diagnosis. This notwithstanding, it islikely that antibody detection will gain in importance asfurther progress is made with controlling helminth infec-tions [39].
154
Post-transmission control – imaging techniques
Recent progress in the use of imaging techniques forhelminthic diseases [13,48,49] has shown that pathologyremains a problem long after the infection has been suc-cessfully treated. Based on experience from Japan, surgicaland other interventions might increasingly be needed onan individual basis in settings in which transmission oftrematode infections has been interrupted. This is cur-rently a totally neglected problem that needs to be bud-geted for as a final outlay when elimination is in sight.
Research needsIntensity of infection is a key determinant of morbidity, butthe relation between egg excretion in stool (or urine orsputum) and severity of disease is complex [11]. Attemptshave been made to classify helminth infection intensitiesbased on egg counts (Table 2); however, these classifi-cations are educated guesses at best, and new researchis warranted to put forth new or refined infection intensityclasses for the helminthiases covered here. Indeed, mor-bidity cannot be assessed without clinical examination andsound imaging techniques [13,48,49]. Nevertheless, thereis a possibility that laboratory testing could be a usefuladjunct. For example, a quantitative assay has been devel-oped for schistosomiasis-related bladder lesions that relieson the excretion of an eosinophilic cationic protein in theurine [50] and it might also be possible to use this approachfor faecal investigations [51].
Although stool examination provides an acceptablemeasure of the stage of infection in highly endemic areas,there was originally hope that antigen detection would dothe same at the other end of the control spectrum (i.e. inareas of very low endemicity). However, this has not beenvalidated because antigen-detection techniques are onlymarginally more sensitive than stool examination.Although serology and microscopy are complementary, itcannot be emphasized enough that the integration of ser-ological methods into national control programmesrequires the development of accurate, methodologicallystandardized and easily applicable assays for the detectionof both specific antibodies and antigens.
Although most countries are still far from eliminationwith respect to the helminthiases discussed here, it alreadymakes sense to consider what will be required before an

Table 2. Classification of infection intensities of different helminths according to egg countsa
Parasite investigated Unit of measure Infection intensity RefsLight Moderate Heavy
Schistosomes
Schistosoma mansoni EPG 1–99 100–399 �400 [11]
Schistosoma haematobium Eggs/10 ml urine 1–49 �50 �50 [11]
Soil-transmitted helminths
Ascaris lumbricoides EPG 1–4999 5000–49 999 �50 000 [11]
Hookworm EPG 1–1999 2000–3999 �4000 [11]
Trichuris trichiura EPG 1–999 1000–9999 �10 000 [11]
Food-borne trematodes
Clonorchis sinensis EPG TBD TBD TBD –
Fasciola hepatica EPG TBD TBD TBD –
Fasciola gigantica EPG TBD TBD TBD –
Opisthorchis viverrini EPG 1–999 1000–9999 �10 000 [52]
Paragonimus spp. EPG TBD TBD TBD –aOf note, for most food-borne trematodes, infection intensity thresholds are still lacking. Abbreviations: EPG, eggs per gram of stool; TBD, to be determined.
Opinion Trends in Parasitology Vol.25 No.4
infection in an area or entire country can be formallydeclared to be eliminated. Would it suffice to present acertain number of negative results, over a specified timeperiod, based on an absolutely specific and highly sensitiveassay (such as PCR), in conjunction with negative serol-ogy?
The issues discussed here are not the only ones that canintroduce failings as large-scale helminth control pro-grammes continue to advance, but the identification ofthe main diagnostic obstacles and dilemmas will facilitatethe finding of logical, straightforward ways to addressthem. The opinions expressed here are intended as anincitement to further enlargement of the scope of helminthdiagnosis in multi-country studies. Implementation ofstandardized protocols would lead to a more rigorousvalidation of the different diagnostic assays in use so thatthey can be utilized with better levels of confidence at thedifferent stages of control interventions.
AcknowledgementsWe wish to thank Lester Chitsulo for initiating an informal consultationat WHO to discuss some of the diagnostic dilemmas in helminthologyexpressed here. J.U. acknowledges financial support from the SwissNational Science Foundation (project no. PPOOB–102883; PPOOB–
119129).
References1 Ridley, R.G. (2006) Diagnostics take centre stage.Nat. Rev.Microbiol. 4
(Suppl.), S12 Gottstein, B. and Piarroux, R. (2008) Current trends in tissue-affecting
helminths. Parasite 15, 291–2983 Ruiz-Tiben, E. and Hopkins, D.R. (2006) Dracunculiasis (Guinea worm
disease) eradication. Adv. Parasitol. 61, 275–3094 Lammie, P.J. et al. (2006) A blueprint for success: integration of
neglected tropical disease control programmes. Trends Parasitol. 22,313–321
5 Ottesen, E.A. (2006) Lymphatic filariasis: treatment, control andelimination. Adv. Parasitol. 61, 395–441
6 Zhu, Y.C. (2005) Immunodiagnosis and its role in schistosomiasiscontrol in China: a review. Acta Trop. 96, 130–136
7 Fenwick, A. et al. (2006) Implementation of human schistosomiasiscontrol: challenges and prospects. Adv. Parasitol. 61, 567–622
8 Bethony, J. et al. (2006) Soil-transmitted helminth infections:ascariasis, trichuriasis, and hookworm. Lancet 367, 1521–1532
9 Steinmann, P. et al. (2006) Schistosomiasis and water resourcesdevelopment: systematic review, meta-analysis, and estimates ofpeople at risk. Lancet Infect. Dis. 6, 411–425
10 Hotez, P.J. et al. (2008) Helminth infections: the great neglectedtropical diseases. J. Clin. Invest. 118, 1311–1321
11 WHO (2002) Prevention and control of schistosomiasis and soil-transmitted helminthiasis: report of a WHO expert committee.WHO Tech. Rep. Ser. No. 912
12 Keiser, J. and Utzinger, J. (2005) Emerging foodborne trematodiasis.Emerg. Infect. Dis. 11, 1507–1514
13 Lun, Z.R. et al. (2005) Clonorchiasis: a key foodborne zoonosis in China.Lancet Infect. Dis. 5, 31–41
14 McManus, D.P. and Dalton, J.P. (2006) Vaccines against the zoonotictrematodes Schistosoma japonicum, Fasciola hepatica and Fasciolagigantica. Parasitology 133 (Suppl.), S43–S61
15 Liu, Q. et al. (2008) Paragonimiasis: an important food-borne zoonosisin China. Trends Parasitol. 24, 318–323
16 Sripa, B. (2008) Concerted action is needed to tackle liver flukeinfections in Asia. PLoS Negl. Trop. Dis. 2, e232
17 The TDR Diagnostics Evaluation Expert Panel (2006) Evaluation ofdiagnostic tests for infectious diseases: general principles. Nat. Rev.Microbiol. 4 (Suppl.), S21–S31
18 Peeling, R.W. et al. (2006) A guide for diagnostic evaluations.Nat. Rev.Microbiol. 4 (Suppl.), S2–S6
19 Engels, D. et al. (2002) The global epidemiological situation ofschistosomiasis and new approaches to control and research. ActaTrop. 82, 139–146
20 Engels, D. and Savioli, L. (2006) Reconsidering the underestimatedburden caused by neglected tropical diseases. Trends Parasitol. 22,363–366
21 Brooker, S. and Utzinger, J. (2007) Integrated disease mapping in apolyparasitic world. Geospat. Health 1, 141–146
22 Giboda, M. and Bergquist, N.R. (2000) Post-transmissionschistosomiasis: a new agenda. Acta Trop. 77, 3–7
23 Brady, M.A. et al. (2006) Projected benefits from integrating NTDprograms in sub-Saharan Africa. Trends Parasitol. 22, 285–291
24 Fenwick, A. (2006) New initiatives against Africa’s worms. Trans. R.Soc. Trop. Med. Hyg. 100, 200–207
25 Kolaczinski, J.H. et al. (2007) Neglected tropical diseases in Uganda:the prospect and challenge of integrated control. Trends Parasitol. 23,485–493
26 Jordan, P. (2000) From Katayama to the Dakhla Oasis: the beginningof epidemiology and control of bilharzia. Acta Trop. 77, 9–40
27 WHO (1985) The control of schistosomiasis: report of a WHO expertcommittee. WHO Tech. Rep. Ser. No. 728
28 Lengeler, C. et al. (2002) Questionnaires for rapid screening ofschistosomiasis in sub-Saharan Africa. Bull. World Health Organ.80, 235–242
29 Dang, T.C. et al. (2008) Prevalence, intensity and risk factors forclonorchiasis and possible use of questionnaires to detectindividuals at risk in northern Vietnam. Trans. R. Soc. Trop. Med.Hyg. 102, 1263–1268
30 Strandgaard, H. et al. (2008) Local perceptions and practices in regardto opisthorchiasis in two villages in Lao PDR. Southeast Asian J. Trop.Med. Public Health 39, 19–26
31 Katz, N. et al. (1972) A simple device for quantitative stool thick-smeartechnique in schistosomiasis mansoni. Rev. Inst. Med. Trop. Sao Paulo14, 397–400
155

Opinion Trends in Parasitology Vol.25 No.4
32 Rim, H.J. et al. (2003) Prevalence of intestinal parasite infections on anational scale among primary schoolchildren in Laos. Parasitol. Res.91, 267–272
33 Guyatt, H. (1998) Different approaches to modelling the cost-effectiveness of schistosomiasis control. Mem. Inst. Oswaldo Cruz 93(Suppl. 1), 75–84
34 Doenhoff, M.J. et al. (2008) Praziquantel: mechanisms of action,resistance and new derivatives for schistosomiasis. Curr. Opin.Infect. Dis. 21, 659–667
35 Trung Dung, D. et al. (2007) Fishborne zoonotic intestinal trematodes.Vietnam. Emerg. Infect. Dis. 13, 1828–1833
36 Dacombe, R.J. et al. (2007) Time delays between patient and laboratoryselectively affect accuracy of helminth diagnosis. Trans. R. Soc. Trop.Med. Hyg. 101, 140–145
37 Steinmann, P. et al. (2007) Occurrence of Strongyloides stercoralis inYunnan province, China, and comparison of diagnostic methods. PLoSNegl. Trop. Dis. 1, e75
38 Booth, M. et al. (2003) The influence of sampling effort and theperformance of the Kato-Katz technique in diagnosing Schistosomamansoni and hookworm co-infections in rural Cote d’Ivoire.Parasitology 127, 525–531
39 Doenhoff, M.J. et al. (2004) Specific and sensitive diagnosis ofschistosome infection: can it be done with antibodies? TrendsParasitol. 20, 35–39
40 Enk, M.J. et al. (2008) A combined strategy to improve the control ofSchistosomamansoni in areas of low prevalence in Brazil. Am. J. Trop.Med. Hyg. 78, 140–146
41 Utzinger, J. et al. (2008) FLOTAC: a new sensitive technique for thediagnosis of hookworm infections in humans. Trans. R. Soc. Trop. Med.Hyg. 102, 84–90
156
42 Knopp, S. et al. (2009) A single FLOTAC is more sensitive thantriplicate Kato-Katz for the diagnosis of low-intensity soil-transmitted helminth infections. Trans. R. Soc. Trop. Med. Hyg.103, 347–354
43 de Vlas, S.J. and Gryseels, B. (1992) Underestimation of Schistosomamansoni prevalences. Parasitol. Today 8, 274–277
44 Knopp, S. et al. (2008) Diagnosis of soil-transmitted helminths in theera of preventive chemotherapy: effect of multiple stool sampling anduse of different diagnostic techniques. PLoS Negl. Trop. Dis. 2, e331
45 Steinmann, P. et al. (2008) Extensive multiparasitism in a village ofYunnan province, People’s Republic of China, revealed by a suite ofdiagnostic methods. Am. J. Trop. Med. Hyg. 78, 760–769
46 Eberl, M. et al. (2002) A novel and sensitive method to monitorhelminth infections by faecal sampling. Acta Trop. 83, 183–187
47 Duenngai, K. et al. (2008) Improvement of PCR for detection ofOpisthorchis viverrini DNA in human stool samples. J. Clin.Microbiol. 46, 366–368
48 Khandelwal, N. et al. (2008) Biliary parasites: diagnostic andtherapeutic strategies. Curr. Treat. Options Gastroenterol. 11, 85–95
49 Lambertucci, J.R. et al. (2008) Imaging techniques in the evaluation ofmorbidity in schistosomiasis mansoni. Acta Trop. 108, 209–217
50 Leutscher, P.D.C. et al. (2000) Morbidity assessment in urinaryschistosomiasis infection through ultrasonography and measurement ofeosinophil cationic protein (ECP) in urine.Trop.Med. Int. Health 5, 88–93
51 Reimert, C.M. et al. (2008) Assessment of Schistosoma mansoniinduced intestinal inflammation by means of eosinophil cationicprotein, eosinophil protein X and myeloperoxidase before and aftertreatment with praziquantel. Acta Trop. 105, 253–259
52 Sadun, E.H. (1955) Studies on Opisthorchis viverrini in Thailand. Am.J. Hyg. 62, 81–115