Embed Size (px)
Citation preview

Diagnostic Approach to theAcute Abdomen
Gilles Fecteau, DMV*, André Desrochers, DMV, MSc, David Francoz, DMV, MSc,Sylvain Nichols, DMV, MS
KEYWORDS
� Bovine � Abdomen � Colic � Pain � Ancillary tests
KEY POINTS
� Whether to cut or to wait is not an easy decision and remains a challenge for most foodanimal practitioners.
� Optimal management depends of multiple factors, some of which are under the directcontrol of the veterinarian, whereas others are totally independent.
� Complete physical examination and judicious use of ancillary tests remains the best ally.
� It is important to keep in mind that exploratory laparotomy is sometimes an economicaloption.
BACKGROUND INFORMATION
This description of the acute abdomen and the proposed diagnostic and therapeuticapproach are the result of clinical experience and interaction between cliniciansspecializing in surgery and in medicine. Although the authors realize that many con-cepts presented apply better in a teaching hospital, we think that many hints andtips remain relevant for the bovine practitioner confronted everyday with the fieldreality.One of the most challenging situations in bovine medicine, the acute abdomen may
evolve into a critical situation in which the client becomes nervous, especially if a valu-able animal is involved. In some species, the cost and risk associated with abdominalsurgery justifies completing the medical workup to avoid surgery if possible. In thebovine, the cost and risk associated to a standing laparotomy is such that, in manysituations, it seems more economical to perform a diagnostic exploratory laparotomyand institute the appropriate treatment instead of adding the cost of diagnostic testsand procedures before surgery. Is this a reasonable approach? Is it always withoutnegative consequences?
Disclosure: The authors have nothing to disclose.Clinical Sciences Department of Universite de Montreal, 3200 rue Sicotte, Saint-Hyacinthe,Quebec J2S 2M2, Canada* Corresponding author.E-mail address: [email protected]
Vet Clin Food Anim 34 (2018) 19–33https://doi.org/10.1016/j.cvfa.2017.10.001 vetfood.theclinics.com0749-0720/18/ª 2017 Elsevier Inc. All rights reserved.
Fecteau et al20
DEFINITION
The acute abdomen is a general term often used to characterize an animal presentedas an emergency, in a more or less severe critical state, and for which medical andpossibly surgical treatment will be necessary. The term is often used to describe casesin which some degree of uncertainty remains in regard to the diagnosis.
INTRODUCTION
The clinician should use a systematic approach based on adequate signalment andhistory, complete physical examination, and judicious choice of ancillary tests. Anexcellent knowledge of the bovine abdominal anatomy and a good understandingof the pathophysiology of abdominal pain are additional tools often useful in difficultcases. Good clinical judgment, critical analysis, and good client communication skillsare competencies that often make a difference in the outcome of a particular case.
ABDOMINAL PAIN IN RUMINANTS
Abdominal pain may be a consequence of excess distension of a hollow viscus,spasm of intestinal smooth muscle, stretching of the mesenteric supporting structure,intestinal ischemia, or chemical irritation of the visceral or parietal peritoneum.Abdominal pain may be classified into visceral pain (hollow viscus and solid organs)and parietal pain (parietal peritoneum, abdominal muscles, rib cage). Pain sensationfrom the parietal peritoneum travels through the peripheral spinal nerves and usuallylocalizes over the affected area. Because parietal pain is exacerbated by pressureand tension modification, the patient is reluctant to move and have a tonic reflexcontraction of the abdominal muscles. In most cases, no active clinical signs of colicare recognized. Some pain fiber endings are located in the submucosa and musclelayers of hollow viscus (intestines, bladder), and in the capsule of solid organs (kidney,liver). Consequently, distention, forceful contraction, or traction will produce pain.Capsule stretching will also create pain. Visceral pain is most often associated withactive manifestation of colic: kicking at the abdomen, treading with the rear feet, lyingdown or standing, and stretching out. Visceral pain is transmitted via sensory fibers inthe autonomic nerves and is often diffuse and difficult to localize.Differential diagnosis for colic in ruminants may be first categorized into abdominal
or extraabdominal origin. Extraabdominal causes include thoracic pain, laminitis, andmyopathy. Although not truly related to abdominal diseases, animals affected by thoseconditions can mimic clinical signs of colic. The abdominal causes can then be sub-categorized into digestive or nondigestive origin. The nondigestive causes include py-elonephritis and uterine torsion, whereas the classic abdominal digestive causesinclude abomasal volvulus, intussusception, and ileus.
RAPID EVALUATION OF THE PATIENT
Some patients need immediate medical assistance and the primary objective is to buytime to allow a better examination. Several abdominal emergencies are associatedwith either hypovolemic or septic shock. Hypovolemic shock is characterized byincreased heart rate, pale mucous membranes, slow capillary refill time, and dehydra-tion. Increased heart rate and dehydration are also observed in case of septic shock,but mucous membranes are hyperemic or bluish in color, and scleral vessels areengorged and dark. Intensive fluid therapy is the treatment of choice for both hypovo-lemic and septic shock.1 Consequently, an intravenous (IV) catheter should be placedand fluid therapy instituted immediately. IV administration of hypertonic saline

Diagnostic Approach to the Acute Abdomen 21
provides a rapid resuscitation in dehydrated or endotoxemic ruminants.2 A rate of 4 to5 mL/kg of hypertonic solution should be administered IV through the jugular vein over4 to 5 minutes. Animals should be provided with a supply of fresh water immediatelyafter the treatment or an IV infusion of an isotonic crystalloid solution should be insti-tuted. Cattle not observed to drink within 5 minutes should have 20 L of water pumpedinto the rumen.2 In the authors’ clinics, unless the animal is unable to stand or isshowing clinical signs of acute blood loss, hypertonic solutions are not used routinelyin cases of acute abdomen. Most patients would already have received nonsteroidalantiinflammatory drugs (NSAIDs) before presentation; however, if not previouslyadministered, they should be given to provide some degree of comfort and to allowthe complete evaluation of the animal.
HISTORY
Age, sex, breed, and production stage are important parameters to take into consid-eration when elaborating the differential diagnosis. For example, abomasal volvulusdevelops more frequently in dairy cows than in beef cattle.3,4 Similarly, uterine torsionsare essentially observed at the time of parturition or in the last trimester.5 Colic in awether or a buck goat should be considered a result of urolithiasis until proven other-wise. Nutrition program and management system are important parts of the history.Previous surgery, recent calving, and obstetric manipulations are important risk fac-tors for peritonitis. Recent estrus could be associated with hypocalcemia and resultsin paralytic ileus.6 Previous treatments, especially those that can modify clinical signsor the interpretation of laboratory results, should also be noted. Description of the clin-ical signs observed by the owner and the chronologic sequence of events are ofparticular interest. Fecal output, consistency, and appearance are relevantinformation.
PHYSICAL EXAMINATIONHemodynamic State
Assessment of cardiovascular status is essential and based on heart rate, mucousmembranes, capillary refill time, and dehydration. Determination of rectal temperature,pulse or heart rate, and respiratory rate (TPR) should always be performed firstbecause manipulations performed during the physical examination of an abdominalemergency can elicit pain, modifying the heart rate. The TPR and amount of painexhibited may also be used to monitor the evolution of the condition and the responseto the initiated treatment. Once vital parameters have been evaluated and the animalseems hemodynamically stable, a thorough physical examination of the body systemsshould be performed.
Profile, Auscultation
The abdominal profile should be observed from the rear and both sides to detect andcharacterize abdominal distention.7,8 An arched back may be observed in cases ofcranial abdominal pain or laminitis (sore feet). Examination of the thorax (pleuropneu-monia, rib fractures) and the musculoskeletal system (laminitis, myopathy) are impor-tant in eliminating diseases that mimic abdominal pain. Abdominal examination isperformed by auscultation, percussion, and succussion of the abdomen. The authorsthink that the rumen auscultation is of particular interest and should last at least 2 mi-nutes. The rumen contractions should be counted and characterized. Three completecontractions per 2 minutes are normal. Incomplete and frequent (>5 per 2 minutes) arenot normal. Complete absence of contraction for 2 minutes is also abnormal. The
Fecteau et al22
rumen auscultation should be repeated after the initial treatment is done to evaluatethe improvement. Pings are tympanic resonance caused by a gas-fluid interface ina distended organ and can be detected by simultaneous auscultation and percus-sion.7 Ping detection should be performed before rectal palpation because the pro-cedure may create an area of increased resonance on the right dorsal part of theabdomen. On the right side of the abdomen, many organsmay cause a ping. Location,pitch characteristics, and variability of the ping are essential to establish a differentialand precise diagnosis. On the left side, pings are principally associated with leftabomasal displacement, ruminal collapse, and pneumoperitoneum. Simultaneousauscultation and ballottement (succussion) of the abdomen may permit detection offluid trapped within the intestine or in a hollow viscus, such as the rumen orabomasum. The location of the fluid splashing sounds on auscultation-succussionmay help to confirm and differentiate among auscultation-percussion findings.
Pain Origin
Although the task may be challenging, localization of the origin of the pain should beattempted. Cattle with cranial abdominal pain associated with peritonitis are reluctantto move; they stand with elbows abducted and back arched. During examination,bruxism (grinding of the teeth) may be present. Pain can be elicited by pinchingover the withers or applying forceful movement with the knee or upward pressurewith a bar or pole over the xyphoid area or anterior abdomen. In response, the animalin pain may grunt or kick and be reluctant to dip the back.7 Sensitivity of this test maybe increased by simultaneous auscultation of the trachea. Tense abdominal muscles,secondary to parietal peritoneum inflammation, may also be detected during succus-sion. The visceral pain is often diffuse and virtually impossible to localize with certainty.
Transrectal Palpation
Per rectum abdominal palpation of cattle is helpful in the differential diagnosis of anacute abdomen. Cecal disorders are clearly diagnosed per rectal palpation. Moreover,cecal dilatation or volvulus can be differentiated by location of the apex. Multiple,dilated, turgid small intestine loops and a firm mass may be palpated in cases of intus-susception9,10 or hemorrhagic bowel syndrome (HBS).11 Uterine wall integrity may beevaluated. In cases of urolithiasis in bulls or steers, rectal palpation reveals a pulsatilepelvic urethra and a distended bladder. In cases of pyelonephritis, enlargement of 1 orboth ureters may be palpated. The left kidney may be painful, as well as enlarged.
Fecal Output and Appearance
Presence andmacroscopic appearance of feces can be evaluated during rectal exam-ination. A decreased volume of feces is principally associated with intestinal stasis orobstruction, which may occur secondary to mechanical obstruction (requiring surgicaltreatment) or to gastrointestinal ileus (requiring only medical treatment). However,feces may be present in the first few days after an intestinal obstruction.12 Macro-scopic appearance of feces is sometimes helpful in the differential diagnosis. HBSis associated with feces resembling raspberry jam. Dark feces (melena) are oftenassociated with abomasal ulcers. Fibrin and mucus without feces is more oftenseen in case of complete obstruction.
MEDICAL TREATMENT
If immediate surgery is not necessary, there is time to initiate a medical treatment thatwill first improve the general condition of the patient and sometimes will be sufficient to

Diagnostic Approach to the Acute Abdomen 23
obtain enough improvement and avoid surgery. If the animal is considered a potentialsurgical patient but not in immediate need of surgery, diagnostic procedures shouldbe considered and performed as medical therapy is administered. The goal of sup-portive therapy is to correct hemodynamic and metabolic imbalances, to controlpain, and to prevent or treat infection when suspected.
Fluid Therapy
Crystalloid solutions (0.9% sodium chloride, Ringer solution) are indicated initially toreplenish fluid loss and improve the circulating blood volume. In the authors’ clinics,we often use a volume of 20 L of isotonic saline in adult cows (20 L IV in 60–90minutes)as an initial fluid therapy. It is not unusual for a critical adult cow to receive 60 L of IVfluid over 24 hours. Ideally, correction of electrolytes imbalance should be based onlaboratory results (measured in between 20 L of fluids). Most patients with acuteabdomen suffer from the metabolic alkalosis associated with hypochloremia and hy-pokalemia. Hypocalcemia is common in dairy cattle with gastrointestinal diseases.Calcium ions are of particular importance in gastrointestinal motility. In the authors’clinics, the IV solution used for the medical treatment of an acute abdomen is mostoften an isotonic saline (20 L of 0.9%) in which calcium borogluconate 23%(500 mL) is added. Response to fluid therapy helps make the diagnosis becauseimprovement with calcium-rich fluid provides insight in the likelihood of surgical prob-lem. If the patient continues to deteriorate while receiving rapid IV fluids, the medicalapproach may not be sufficient. Repeated TPR and brief gastrointestinal motilityassessment (rumen contractions, gut sounds, fecal output, and ultrasound assess-ment of motility) often indicate the benefit of medical therapy.
Pain Control
Pain is a primary cause of gastrointestinal hypomotility. Gastrointestinal pain in-creases sympathic tone, causing general inhibition of the gastrointestinal tract.13,14
Peritoneal inflammation or irritation and associated pain are initiatory factors of theileus in several species.13,15 Consequently, analgesic and antiinflammatory drugsare often considered in the management of the bovine acute abdomen. These drugsmust be used with the complete knowledge of their possible side-effects. NSAIDs mayinduce abomasal ulcers particularly in an anorexic patient. Analgesics may also alterclinical signs (pain, fever) used to decision-making. No single NSAID can be recom-mended based on scientific evidence for the management of abdominal emergenciesin cattle. The choice of NSAID becomes a matter of previous experience, comparativemedicine, legislation, and cost. In the authors’ experiences, both flunixin and ketopro-fen are adequate for the management of acute abdomen in cattle. In equine gastroin-testinal pain, a poor or short duration response to NSAIDs indicates the need forsurgery.14 This concept may or may not applied to cattle because their response topain is less predictable. Xylazine is reported to have significant effects on the gastro-intestinal tract in cattle, decreasing reticuloruminal and intestinal motility.16 Because ofthe hemodynamic changes associated with the administration of a2-agonists, thesedrugs must be used with caution in patients with arterial hypotension and/or shock.17
Antimicrobial Therapy
Bacterial translocation from the intestines may occur in cases of mechanical or func-tional ileus secondary to bacterial overgrowth, inflammation, and impairment of thefunctional barrier of the intestinal wall.15,18 The choice of antimicrobial is variablebut the IV route is always the first choice because most of these patients alreadyhave an IV catheter. The choice of antibiotic should also take into consideration legal
Fecteau et al24
aspects and the cost of the treatment. b-lactams, tetracyclines, and trimethoprim-sulfadoxine seem to be good choices. As a rule of thumb, trimethoprim-sulfadoxineis our first choice for enteric disease, whereas b-lactams are often used with peritonitisand presurgical antimicrobial therapy. Because a significant portion of these patientswill eventually need surgery, this could also justify initiating therapy. In cattle, there isno accepted recommendation for the duration of treatment. In human medicine, pro-longed broad-spectrum antibiotic therapy in case of surgical acute abdomen does notseem beneficial.19 Prevention of infective complications was not affected by prolong-ing the course of antibiotic treatment.19 In humanmedicine, the current recommendeddosage is a single prophylactic antibiotic administration when there is no or minimalevidence of contamination, and over 5 to 7 days when pus or contamination, eitherlocalized or diffuse, is present.19
Prokinetic Drugs
Motility-modifying agents may be used in the management of gastrointestinal disor-ders. In the bovine acute abdomen, it remains a difficult decision before establishinga final diagnosis because some patients suffer from a surgical condition. Prokineticscould aggravate the situation in these cases. In the authors’ clinics, we use prokineticdrugs only when a final diagnosis is made either by exploratory surgery or not.Steiner16 reviewed the different prokinetics that can be used in ruminant medicineand their clinical implication.
USEFUL DIAGNOSTIC PROCEDURES
Ancillary diagnostic tests mainly serve 3 purposes: assessment of the patient’s im-mediate requirements, attainment of an etiologic diagnosis and help determiningprognosis. The following procedures are the ones we find most useful in themanagement of the acute abdomen. They are described in a relative order ofimportance.
Blood Lactate Concentration
Blood lactate concentration is commonly used in the authors’ clinics to assess cardio-vascular state; to monitor the response to treatment; and, to some extent, provide anestimate of prognosis for survival. Our routine use includes an early measurement(before any treatment) and a follow-up measure after initial therapy (IV fluids, NSAIDs,or other). We found that an increase in blood lactate or very marginal reduction inblood lactate, despite aggressive therapy, indicates that surgery is needed or theprognosis is poor.
Blood Gas Analysis, Electrolytes, and Serum Biochemistry Profile
Most gastrointestinal impairment leads to sequestration of the high-chloride abomasalcontents into the upper gastrointestinal system. Some degree of systemic hypo-chloremic hypokalemic metabolic alkalosis eventually develops in most situations.The diagnostic value of this finding is limited because it does not bring precise infor-mation on the possible cause and has controversial value as a prognostic indicator.However, serial measurements allow the best monitoring of the evolution of a partic-
ular case. Serum calcium concentration is of great interest because it is commonly lowin anorexic periparturient dairy cattle. It is so important in gut motility that the authors’think we cannot ignore even a marginal diminution. The serum biochemistry profile willalso reveal any impairment in kidney or liver function, as well as liver damage (elevationof liver enzymes).

Diagnostic Approach to the Acute Abdomen 25
Complete Blood Count
A white blood cell count rarely provides further information to establish the precisecause of the acute abdomen. In most cases, a minimal to moderate inflammatory pro-cess characterized by a neutrophilic leukocytosis is observed. Hematologic findingsmay also provide information about the severity of the associated sepsis and toxemia.Severe sepsis is associated with neutropenia, degenerative left shift, toxic changes ofneutrophil morphology, and lymphopenia. An inflammatory leukogram could also reflectchronic active inflammation, such as in peritonitis. Hematology is also an importantancillary test to monitor the response to treatment. Of particular interest is the relation-ship between plasma protein concentration and packed cell volume (PCV). Anincreased PCV combined with a normal to decreased plasma protein concentrationoften indicates an active secretion of protein-rich fluid into the peritoneal cavity. Shock,sepsis, and toxemia cause hemoconcentration and dehydration, and are associatedwith an increase of PCV and total solids. If a complete blood count is not available,PCV and total solids already provide some relevant information. Fibrinogen concentra-tion could add some insights in cases of chronic inflammation. Studies in cattle reportthat fibrinogen concentration may increase within 1 to 2 days after induction of inflam-matory conditions.20,21 Normal fibrinogen concentration, despite severe visceralinvolvement, should be observed only in peracute cases, within a few hours (eg, torsionof the root of the mesentery). Moderate to marked increased fibrinogen concentration isalso the signature of an active localized inflammatory condition, such as peritonitis.
Abdominocentesis and Peritoneal Fluid Evaluation
Abdominocentesis is a simple and practical procedure helpful to manage acuteabdomen. However, one should remember some bovine particularities. Absence ofperitoneal fluid does not rule out the possibility of peritonitis. Fluid can be evaluatedmacroscopically for color, volume, odor, and turbidity. A large volume of peritonealfluid is abnormal. Peritoneal fluid changes to cloudy yellow with peritonitis, whereasblood tinged with fibrin fluid is more often seen as bowel necrosis and extravasatedred blood cells occur. Normal bovine peritoneal fluid has a specific density lessthan 1.016. Protein content should be less than 3 g/dL, although some investigatorshave reported normal values up to 6.3 g/dL (the major part being albumin). Nucleatedcells count should be less than 10,000 cells per mL, with most macrophages. Lympho-cytes, eosinophils, and desquamated mesothelial cells may also be present. Neutro-phils are rare and more than 50% neutrophils indicate peritonitis. Periparturient cattlehave significantly more peritoneal fluid with a lower protein concentration. Whenmacroscopic examination is not diagnostic, cytologic examination of the peritonealfluid is useful. As an example, in some cases of lymphoma, abnormal lymphocytesmay be observed in the peritoneal fluid. Very little is known about the most commonbacteria isolated from acute or chronic peritonitis. However, because Trueperellapyogenes (Arcanobacterium pyogenes) is commonly isolated from abscesses in thebovine, one could assume that it may be of importance in chronic active peritonitis.Biochemical variables may be evaluated in peritoneal fluid. Lactate, glucose, alkalinephosphatase, and pH of the peritoneal fluid concentrations have been reported to beindicators of intestinal ischemia and peritonitis in horses.22
Medical Imaging: Ultrasound Examination, Laparoscopic Procedures, and CranialAbdominal Radiography
Ultrasound is used to image soft tissues of the abdominal cavity. The potential of thistool is enormous. The size and anatomic relationship of lesions may be delineated.

Fecteau et al26
Knowledge of the underlying anatomy is essential. Ultrasonography is a diagnostictool readily available in large animal medicine and surgery. To evaluate the abdomen,a 3.5 MHz curvilinear or linear probe is ideal. It allows the evaluation of the reticulum;the omasum; the abomasum; the small bowel, including the duodenum; the cecum;and spiral colon (Fig. 1). A 7.5 MHz transrectal probe can be used to diagnose abdom-inal effusion. However, in adult cattle, it is difficult to use the higher frequency probe toevaluate the gastrointestinal tract.During investigation of the acute abdomen, the ultrasound is used to identify the
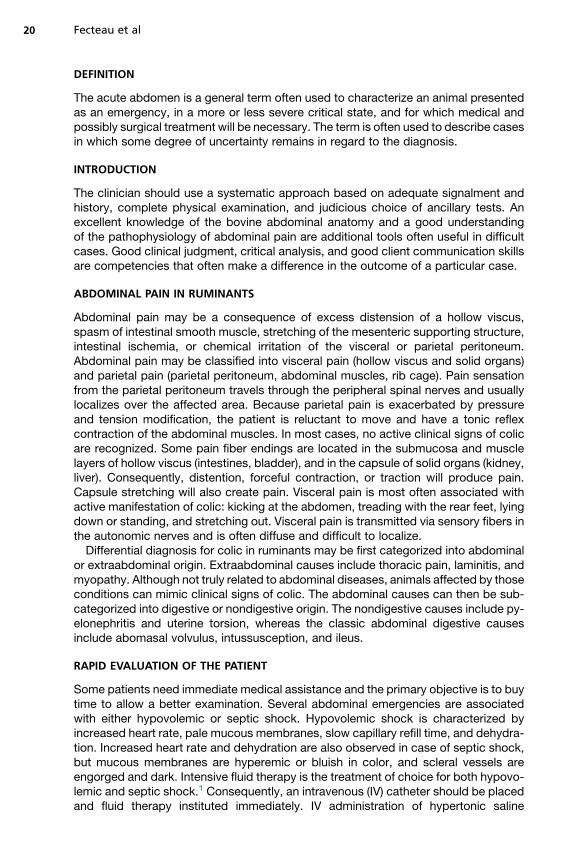
structure involved in the pathologic condition and to evaluate the presence of abdom-inal effusion (Fig. 2). Following an abdominocentesis, the effusion is characterized(lactate, red blood cells, leukocytes, and proteins) to diagnose the surgical abdomen.
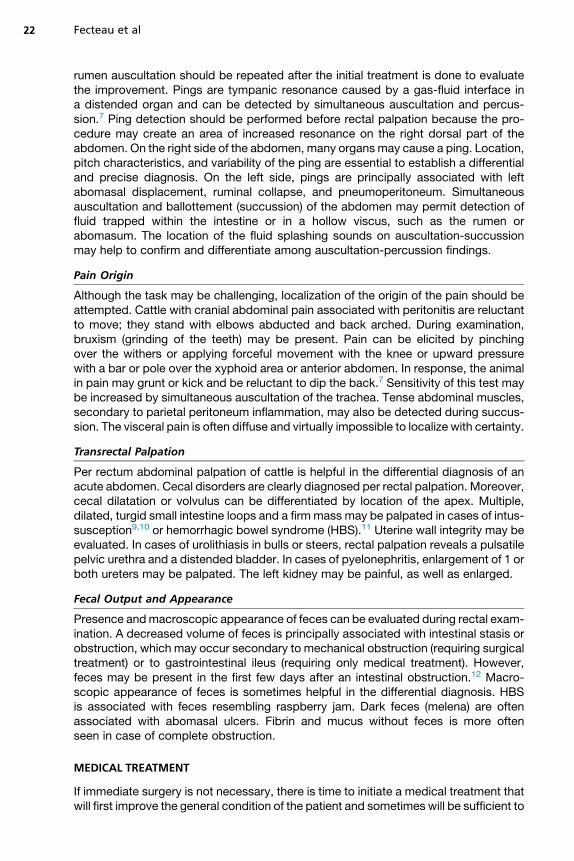
ReticulumThe reticulum is evaluated when reticuloperitonitis is suspected. The cranial abdomen(from left to right) is evaluated. The reticulum has a biphasic contraction.23 Abnormalcontraction or presence of abdominal effusion or even an organized abscess (Fig. 3)suggests hardware disease.24 A cranial abdominal radiograph would confirm the diag-nosis (Fig. 4).
OmasumPathologic complications of the omasum are uncommon. This structure is located onthe visceral surface of the liver. It is best seen by scanning the 6th to 11th intercostalspaces.25 Dilatation of this structure will be recognized ultrasonographically becausethe liver will be cranially displaced by a thick-walled structure. When filled with fluidfrom a proximal gastrointestinal obstruction, the leaves of the omasum becomeapparent (Fig. 5).26
AbomasumThe location of the abomasum can be followed by ultrasonography.27–29 It can beused to confirm a displacement30,31 or to detect a focal zone of peritonitis around achronically displaced abomasum. The distended abomasum is easily recognized byseeing mucosal folds floating in hyperechoic fluids (Fig. 6).Ultrasonography is an efficient tool for investigating vagal syndrome involving the
pylorus. A presumptive diagnosis of pyloric lymphoma (Fig. 7) can readily be
Fig. 1. Localization of abdominal structures evaluated ultrasonographically. (Adapted fromCD on the surgery of the abomasum in cattle Faculte de Medecine Veterinaire, Universite deMontreal 2002, with permission).
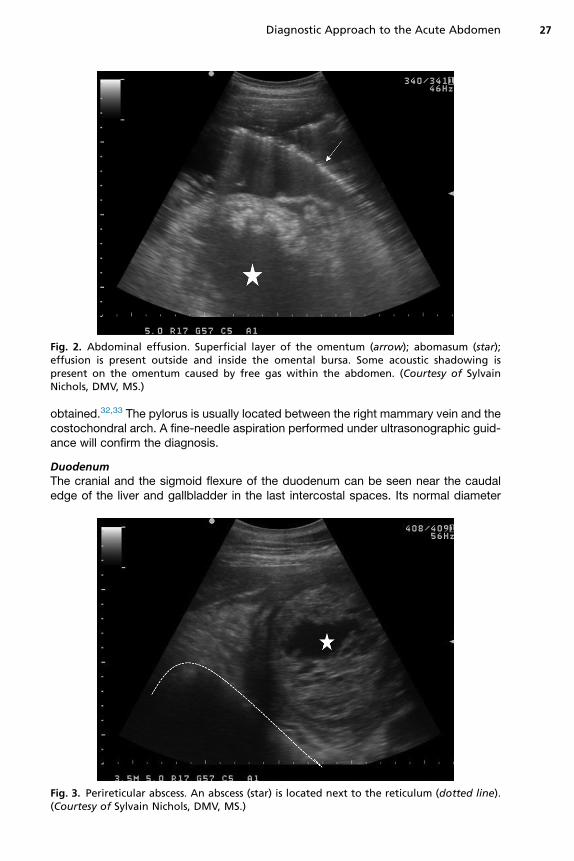
Fig. 2. Abdominal effusion. Superficial layer of the omentum (arrow); abomasum (star);effusion is present outside and inside the omental bursa. Some acoustic shadowing ispresent on the omentum caused by free gas within the abdomen. (Courtesy of SylvainNichols, DMV, MS.)
Diagnostic Approach to the Acute Abdomen 27
obtained.32,33 The pylorus is usually located between the right mammary vein and thecostochondral arch. A fine-needle aspiration performed under ultrasonographic guid-ance will confirm the diagnosis.
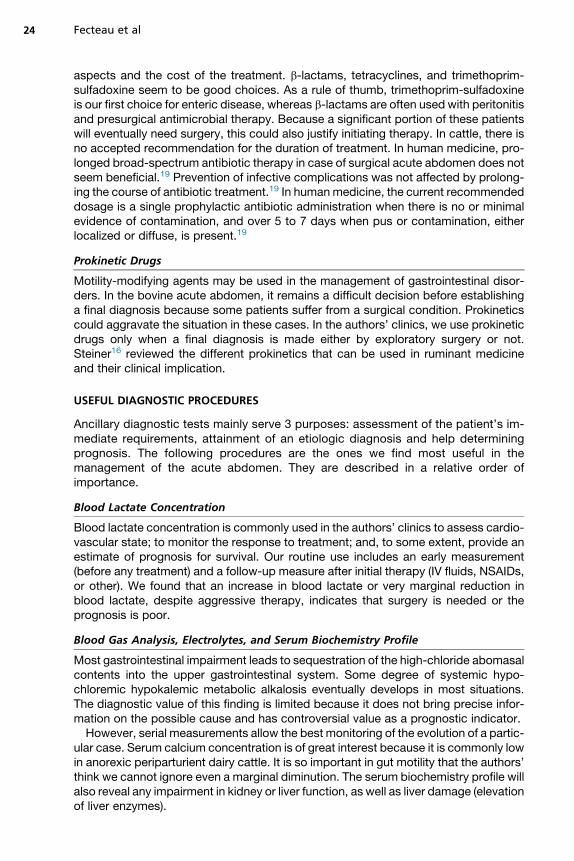
DuodenumThe cranial and the sigmoid flexure of the duodenum can be seen near the caudaledge of the liver and gallbladder in the last intercostal spaces. Its normal diameter
Fig. 3. Perireticular abscess. An abscess (star) is located next to the reticulum (dotted line).(Courtesy of Sylvain Nichols, DMV, MS.)

Fig. 4. Lateral radiograph of a cow with a perireticular abscess. A gas-fluid line is seen in themiddle of the reticulum. A magnet with multiple foreign bodies is seen at the bottom of thereticulum. (Courtesy of Sylvain Nichols, DMV, MS.)
Fecteau et al28
varies between 1.0 and 5.5 cm.34 They will be distended in cases of duodenal sigmoidflexure volvulus or proximal obstruction caused by a trichophytobezoar. Their diame-ters will then reach 10.0 cm.35 Peritonitis secondary to duodenal ulcers can also beseen in this area.
JejunumThe jejunum is usually confined in the caudal lower right flank within the supraomentalbursa. Normally, loops of jejunum of 2 to 4.5 cm in diameter are seen constantly mov-ing.34 Distended and hypomotile jejunum is frequently seen in cattle suffering fromfunctional and mechanical ileus.35 Presence of fluid surrounding the distended bowelsuggests peritonitis.Mechanical obstruction caused by a blood clot (HBS) or by an intussusception can
sometimes be located (Fig. 8).36
Fig. 5. Omasum of a cow suffering from an abomasal volvulus. The laminae (vertical whiteline) of the omasum are seen because of its abnormal fluid content. (Courtesy of SylvainNichols, DMV, MS.)

Fig. 6. Abomasum. Mucosal folds (arrows) can be seen floating in the normal hyperechoiccontent of the abomasum. (Courtesy of Sylvain Nichols, DMV, MS.)
Diagnostic Approach to the Acute Abdomen 29
Cecum and colonThe cecum and colon structures are usually filled with gas. Therefore, only their wallsare seen. The spiral colon has a typical undulated shape (garland). It is located in themiddle of the right paralumbar fossa just above the cecum.37 Normally, the cecum isseen as a crescent-shaped line of 5 to 18 cm in diameter traveling from cranial tocaudal. With cecal dilatation or volvulus, a large gas-filled and fluid-filled viscus (upto 25 cm), without any large mucosal folds (typical of a fluid-filled abomasum) isseen in the right paralumbar fossa.38
Fig. 7. Lymphomatous infiltration (dotted line) of the pylorus of an adult Holstein cowsuffering from vagal indigestion. (Courtesy of Sylvain Nichols, DMV, MS.)
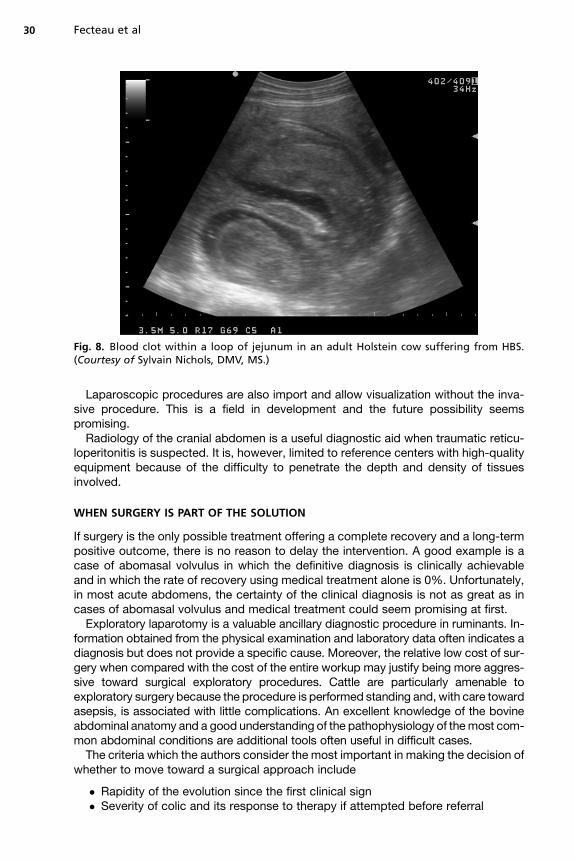
Fig. 8. Blood clot within a loop of jejunum in an adult Holstein cow suffering from HBS.(Courtesy of Sylvain Nichols, DMV, MS.)
Fecteau et al30
Laparoscopic procedures are also import and allow visualization without the inva-sive procedure. This is a field in development and the future possibility seemspromising.Radiology of the cranial abdomen is a useful diagnostic aid when traumatic reticu-
loperitonitis is suspected. It is, however, limited to reference centers with high-qualityequipment because of the difficulty to penetrate the depth and density of tissuesinvolved.
WHEN SURGERY IS PART OF THE SOLUTION
If surgery is the only possible treatment offering a complete recovery and a long-termpositive outcome, there is no reason to delay the intervention. A good example is acase of abomasal volvulus in which the definitive diagnosis is clinically achievableand in which the rate of recovery using medical treatment alone is 0%. Unfortunately,in most acute abdomens, the certainty of the clinical diagnosis is not as great as incases of abomasal volvulus and medical treatment could seem promising at first.Exploratory laparotomy is a valuable ancillary diagnostic procedure in ruminants. In-
formation obtained from the physical examination and laboratory data often indicates adiagnosis but does not provide a specific cause. Moreover, the relative low cost of sur-gery when compared with the cost of the entire workup may justify being more aggres-sive toward surgical exploratory procedures. Cattle are particularly amenable toexploratory surgery because the procedure is performed standing and, with care towardasepsis, is associated with little complications. An excellent knowledge of the bovineabdominal anatomy and a good understanding of the pathophysiology of themost com-mon abdominal conditions are additional tools often useful in difficult cases.The criteria which the authors consider the most important in making the decision of
whether to move toward a surgical approach include
� Rapidity of the evolution since the first clinical sign� Severity of colic and its response to therapy if attempted before referral
Diagnostic Approach to the Acute Abdomen 31
� The severity of the abdominal distention and the absence of fecal output� The heart rate and the rectal palpation findings� Blood lactate, particularly if blood lactate did not return toward normal after med-ical therapy
� Calcium measurements, particularly if low then justifying medical therapy first.
OTHER MEDICAL AND SUPPORTIVE TREATMENTS
Several other treatments may be used before or after surgery. Only a few aredescribed here.The use of purgatives (magnesium hydroxide, mineral oil, liquid paraffin) in cases of
suspected gastrointestinal obstruction or ileus in cattle has no therapeutic basis.12
Moreover, these treatments may exacerbate the condition. Because the intestinesare already filled with gas and fluid, purgatives only impose additional distention.Moreover, magnesium hydroxide may be responsible for detrimental effects, suchas metabolic alkalosis,39 sedation caused by hypermagnesemia,39 increased ruminalpH,40 and decreased ruminal microbial activity.40 The authors strongly discourage theuse of laxatives in bovine acute abdomen.No prokinetic drug is reported to directly increase ruminal motility. In cases of pro-
longed anorexia or acute indigestion, ruminal flora can be disturbed and reduced.Transfaunation may help to rapidly reconstitute the ruminal flora and hasten returnto normal function of the rumen and the digestive tract. The technique for and bene-ficial effects of transfaunation (reduction of ketonuria, increased feed intake, andhigher milk yield) have been reported in the postsurgical treatment of left abomasaldisplacement.41
The Kingman tube is routinely used in the authors’ clinics both before and after sur-gery. In fact, in several cases, as an adjunct to medical therapy, we believe that weoften avoid unnecessary surgery. The procedure is performed on a standing animal.The distension must be important and the ruminal contents should be fluid. When suc-cessful, the amount of rumen fluid evacuated is spectacular. The animal is immedi-ately relieved and time is bought for the medical therapy to become beneficial.
MONITORING
When a definitive diagnosis cannot be made, a close monitoring of the animal is indi-cated. Follow-up is also very important after surgery to ensure adequate responseand allow possible adjustment of treatment. We think that reevaluation every 4 to6 hours is adequate (vital parameters, rectal examination, presence and consistencyof feces, and pain combined to laboratory analyses). Deterioration or persistence ofclinical signs despite the initiation of supportive treatment is also an indication forsurgery.
SUMMARY
Whether to cut or to wait is not an easy decision and remains a challenge for most foodanimal practitioners. Optimal management depends of multiple factors, some of whichare under the direct control of the veterinarian, whereas others are totally independent.Complete physical examination and judicious use of ancillary tests remains the bestally. It is important to keep in mind that exploratory laparotomy is sometimes aneconomical option. However, it is also relevant to remember that it is not the only op-tion to get to the final diagnosis.

Fecteau et al32
REFERENCES
1. Walters PC. Approach to the acute abdomen. Clin Tech Small Anim Pract 2000;15(2):63–9.
2. Constable PD. Hypertonic saline. Vet Clin North Am Food Anim Pract 1999;15(3):559–85.
3. Constable PD, Miller GY, Hoffsis GF, et al. Risk factors for abomasal volvulus andleft abomasal displacement in cattle. Am J Vet Res 1992;53(7):1184–92.
4. Roussel AJ, Cohen ND, Hooper RN. Abomasal displacement and volvulus in beefcattle: 19 cases (1988-1998). J Am Vet Med Assoc 2000;216(5):730–3.
5. Pearson H. Intussusception in cattle. Vet Rec 1971;89(16):426–37.
6. Goff JP. Pathophysiology of calcium and phosphorus disorders. Vet Clin NorthAm Food Anim Pract 2000;16(2):319–37, vii.
7. Belknap EB, Navarre CB. Differentiation of gastrointestinal diseases in adult catt-let. Vet Clin North Am Food Anim Pract 2000;16(1):59–86.
8. Navarre CB, Belknap EB, Rowe SE. Differentiation of gastrointestinal diseases ofcalves. Vet Clin North Am Food Anim Pract 2000;16(1):37–57.
9. Constable PD, St Jean G, Hull BL, et al. Intussusception in cattle: 336 cases(1964-1993). J Am Vet Med Assoc 1997;210(4):531–6.
10. Pearson H. Uterine torsion in cattle: a review of 168 cases. Vet Rec 1971;89(23):597–603.
11. Dennison AC, VanMetre DC, Callan RJ, et al. Hemorrhagic bowel syndrome indairy cattle: 22 cases (1997-2000). J Am Vet Med Assoc 2002;221(5):686–9.
12. Pearson H, Pinsent PJ. Intestinal obstruction in cattle. Vet Rec 1977;101(9):162–6.
13. Bueno L, Fioramonti J, Delvaux M, et al. Mediators and pharmacology of visceralsensitivity: from basic to clinical investigations. Gastroenterology 1997;112(5):1714–43.
14. Malone E, Graham L. Management of gastrointestinal pain. Vet Clin North AmEquine Pract 2002;18(1):133–58.
15. Bauer AJ, Schwarz NT, Moore BA, et al. Ileus in critical illness: mechanisms andmanagement. Curr Opin Crit Care 2002;8(2):152–7.
16. Steiner A. Modifiers of gastrointestinal motility of cattle. Vet Clin North Am FoodAnim Pract 2003;19(3):647–60.
17. Gross ME. Tranquilizers, a2-adrenergic agonists and related agents. In:Adams HR, editor. Veterinary pharmacology and therapeutics. Ames (IA): IowaState University Press; 2001. p. 299–342.
18. Madl C, Druml W. Gastrointestinal disorders of the critically ill. Systemic conse-quences of ileus. Best Pract Res Clin Gastroenterol 2003;17(3):445–56.
19. Gleisner AL, Argenta R, Pimentel M, et al. Infective complications according toduration of antibiotic treatment in acute abdomen. Int J Infect Dis 2004;8(3):155–62.
20. Conner JG, Eckersall PD, Wiseman A, et al. Bovine acute phase responsefollowing turpentine injection. Res Vet Sci 1988;44(1):82–8.
21. Earley B, Crowe MA. Effects of ketoprofen alone or in combination with localanesthesia during the castration of bull calves on plasma cortisol, immunological,and inflammatory responses. J Anim Sci 2002;80(4):1044–52.
22. Saulez MN, Cebra CK, Tornquist SJ. The diagnostic and prognostic value of alka-line phosphatase activity in serum and peritoneal fluid from horses with acutecolic. J Vet Intern Med 2004;18(4):564–7.

Diagnostic Approach to the Acute Abdomen 33
23. Braun U, Rauch S. Ultrasonographic evaluation of reticular motility during rest,eating, rumination and stress in 30 healthy cows. Vet Rec 2008;163(19):571–4.
24. Braun U, Gotz M, Marmier O. Ultrasonographic findings in cows with traumaticreticuloperitonitis. Vet Rec 1993;133(17):416–22.
25. Braun U, Blessing S. Ultrasonographic examination of the omasum in 30 healthycows. Vet Rec 2006;159(24):812–5.
26. Braun U, Feller B, Hassig M, et al. Ultrasonographic examination of the omasum,liver, and small and large intestines in cows with right displacement of theabomasum and abomasal volvulus. Am J Vet Res 2008;69(6):777–84.
27. Braun U, Wild K, Guscetti F. Ultrasonographic examination of the abomasum of50 cows. Vet Rec 1997;140(4):93–8.
28. Van Winden SC, Brattinga CR, Muller KE, et al. Position of the abomasum in dairycows during the first six weeks after calving. Vet Rec 2002;151(15):446–9.
29. Wittek T, Constable P, Morin D. Ultrasonographic assessment of change inabomasal position during the last three months of gestation and first three monthsof lactation in Holstein-Friesian cows. J Am Vet Med Assoc 2005;227(9):1469–75.
30. Braun U, Feller B. Ultrasonographic findings in cows with right displacement ofthe abomasum and abomasal volvulus. Vet Rec 2008;162(10):311–5.
31. Braun U, Pusterla N, Schonmann M. Ultrasonographic findings in cows with leftdisplacement of the abomasum. Vet Rec 1997;141(13):331–5.
32. Braun U, Schnetzler C, Dettwiler M, et al. Ultrasonographic findings in a cow withabomasal lymphosarcoma: case report. BMC Vet Res 2011;7:20.
33. Buczinski S, Belanger AM, Francoz D. Ultrasonographic appearance of lympho-matous infiltration of the abomasum in cows with lymphoma. J Am Vet Med Assoc2011;238(8):1044–7.
34. Braun U, Marmier O. “Ultrasonographic examination of the small intestine ofcows. Vet Rec 1995;136(10):239–44.
35. Braun U, Marmier O, Pusterla N. Ultrasonographic examination of the small intes-tine of cows with ileus of the duodenum, jejunum or ileum. Vet Rec 1995;137(9):209–15.
36. Braun U, Forster E, Steininger K, et al. Ultrasonographic findings in 63 cows withhaemorrhagic bowel syndrome. Vet Rec 2010;166(3):79–81.
37. Braun U, Amrein E. Ultrasonographic examination of the caecum and the prox-imal and spiral ansa of the colon of cattle. Vet Rec 2001;149(2):45–8.
38. Braun U, Amrein E, Koller U, et al. Ultrasonographic findings in cows with dilata-tion, torsion and retroflexion of the caecum. Vet Rec 2002;150(3):75–9.
39. Kasari TR, Woodbury AH, Morcom-Kasari E. Adverse effect of orally administeredmagnesium hydroxide on serum magnesium concentration and systemic acid-base balance in adult cattle. J Am Vet Med Assoc 1990;196(5):735–42.
40. Smith GW, Correa MT. The effects of oral magnesium hydroxide administration onrumen fluid in cattle. J Vet Intern Med 2004;18(1):109–12.
41. Rager KD, George LW, House JK, et al. Evaluation of rumen transfaunation aftersurgical correction of left-sided displacement of the abomasum in cows. J Am VetMed Assoc 2004;225(6):915–20.





